
Abstract
Aim
This study investigated differences in cognitive function between former rugby and non-contact-sport players, and assessed the association between concussion history and cognitive function.
Methods
Overall, 366 former players (mean ± standard deviation [SD] age 43.3 ± 8.2 years) were recruited from October 2012 to April 2014. Engagement in sport, general health, sports injuries and concussion history, and demographic information were obtained from an online self-report questionnaire. Cognitive functioning was assessed using the online CNS Vital Signs neuropsychological test battery. Cohen’s d effect size statistics were calculated for comparisons across player groups, concussion groups (one or more self-reported concussions versus no concussions) and between those groups with CNS Vital Signs age-matched norms (US norms). Individual differences within groups were represented as SDs.
Results
The elite-rugby group (n = 103) performed worse on tests of complex attention, processing speed, executive functioning, and cognitive flexibility than the non-contact-sport group (n = 65), and worse than the community-rugby group (n = 193) on complex attention. The community-rugby group performed worse than the non-contact group on executive functioning and cognitive flexibility. Compared with US norms, all three former player groups performed worse on verbal memory and reaction time; rugby groups performed worse on processing speed, cognitive flexibility and executive functioning; and the community-rugby group performed worse on composite memory. The community-rugby group and non-contact-sport group performed slightly better than US norms on complex attention, as did the elite-rugby group for motor speed. All three player groups had greater individual differences than US norms on composite memory, verbal memory and reaction time. The elite-rugby group had greater individual differences on processing speed and complex attention, and the community-rugby group had greater individual differences on psychomotor speed and motor speed. The average number of concussions recalled per player was greater for elite rugby and community rugby than non-contact sport. Former players who recalled one or more concussions (elite rugby, 85 %; community rugby, 77 %; non-contact sport, 23 %) had worse scores on cognitive flexibility, executive functioning, and complex attention than players who did not recall experiencing a concussion.
Conclusions
Past participation in rugby or a history of concussion were associated with small to moderate neurocognitive deficits (as indicated by worse CNS Vital Signs scores) in athletes post retirement from competitive sport.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The former elite rugby union player group had deficits in cognitive functioning relative to the non-contact-sport player group, as indicated by complex attention, cognitive flexibility, processing speed and executive functioning scores using the CNS Vital Signs test. The former community-rugby group performed worse than non-contact-sports players on cognitive flexibility and executive functioning tests. |
Community and elite former rugby union players reported a substantially higher number of concussions than non-contact-sport players. |
The player group who had experienced one or more concussions had deficits in cognitive flexibility, complex attention, and executive function relative to the player group with no history of concussion. |
Past participation in rugby or a history of concussion were associated with small to moderate neurocognitive deficits (as indicated by worse CNS Vital Signs scores) in athletes post retirement from competitive sport. |
1 Background
Rugby union is a field-based contact sport with over 7.7 million participants spanning 129 countries. Several variants of rugby exist, with the most commonly played form consisting of two teams of 15 players trying to score more points than the opposition within two continuous 40 min halves of a match. An additional eight athletes are available as replacements, giving a total of 23 players per team. Rugby involves physically challenging activities, including sprinting, kicking, passing, and tackling.
Concussion is a subset of traumatic brain injury that occurs when impact forces to the head or body result in transient changes in neurocognitive functions of the brain. Concussion can occur when playing/training for rugby as a result of impacts associated with falls, collisions, tackles, rucks, or scrums. Concussion symptoms typically include headache, dizziness, confusion and nausea [1].
Rugby has a high incidence of concussion [2]. Reports from the Rugby Football Union in England indicate that concussion is now the most common injury experienced by professional players, accounting for 12.5 % of all injuries [3]. In a study [4] of traumatic brain injuries across sports in New Zealand, rugby (union and league combined) was the sport linked to the greatest number of brain injuries. A variety of factors affect reported concussion rates, including lack of standardized criteria for recording concussions for injury surveillance purposes [5, 6] and a lack of disclosure of injuries to medical staff by players [7–9].
Concussive head impacts create a cascade of pathological metabolic changes that may result in a transient decline in cognitive function, and may potentiate long-term cognitive deficits similar to those associated with the aging process [10]. Studies across a range of sports have highlighted the negative short-term [11] and cumulative neurocognitive [12] effects of head trauma in sport. However, the possible association between concussion and negative long-term neuropsychological effects in former adult rugby players had not been studied at the start of this study.
This RugbyHealth substudy investigated cognitive functioning of former elite rugby, community rugby and non-contact-sport players using the CNS Vital Signs (CNS-VS) test battery. It also explored the effect of concussion history on neurocognition.
2 Methods
2.1 Study Design and Setting
This was a cross-sectional study of elite and community rugby players and a non-contact-sport comparison group. To protect the identity of athletes, the study was completed anonymously online. Participants gave informed consent after reading a participant information sheet about the project.
2.2 Study Participants
Participants were 366 former New Zealand athletes drawn from three groups: elite rugby (n = 103), community rugby (n = 198), and non-contact-sport retirees (cricket and field hockey players; n = 65). They were a self-selected cohort from the larger RugbyHealth project [13] of 485 participants investigating the health of retired rugby and non-contact-sport athletes who volunteered to participate in assessment of their neurocognition. Participants in the larger study were recruited from October 2012 to April 2014 using media reports, word of mouth, flyers, and social media. Elite rugby players were required to have played at international or national level, while the community-level group played at club or regional level. Non-contact-sport players may have played at any competitive level. All participants were required to be male, aged 23–72 years and retired from competitive play. Elite players are what would now be termed professional players; however, when many of the older participants in the study played at the international or national level of rugby, it was still amateur rugby, given that players were not paid to play.
2.3 Procedures
Information on engagement in sport, sport-related injury and concussion history, and demographic information was elicited from an online self-report rugby general health questionnaire developed for the study, which took approximately 40 min to complete. This paper provides data relating to concussions, alcohol use and current physical health.
A history of concussion was determined by asking participants several questions about their experiences of concussion. For example, they were asked how many times they had sustained a concussion while playing or training for rugby/hockey/cricket, had been evaluated by a doctor or other health professional for concussion, had lost consciousness (been ‘knocked out’) or sustained other symptoms of concussion, or had never reported their concussion to medical staff. Concussion was defined as being a blow to the head followed by a variety of symptoms (loss of consciousness, headache, dizziness, loss of balance, blurred vision, ‘seeing stars’, feeling in a fog or slowed down, memory problems, poor concentration, nausea, or throwing up).
Players were asked to rate their current physical health as very poor, poor, average, good, or excellent. Alcohol use was assessed using the Alcohol Use Disorders Identification Test (AUDIT) [14], and hazardous drinking was defined as a score higher than 7 on the AUDIT.
A web link was sent to participants to complete the online neuropsychological test. Online self-report data were linked with the neuropsychological test scores by a unique study registration number.
2.4 Neuropsychological Assessment
Cognitive functioning was assessed using the CNS-VS neuropsychological online test (CNS-VS; CNS Vital Signs LLC, Morrisville, NC, USA) [15]. The CNS-VS test battery includes seven tests assessing functioning across different cognitive domains, including verbal, visual and composite memory, psychomotor and information processing speed, reaction time, executive functioning, motor speed, cognitive flexibility, simple and complex attention. Explanations of the domains are provided in the CNS-VS ‘Brief Interpretation Guide’ (see http://www.cnsvitalsigns.com). For example, complex attention is the “ability to track and respond to information over lengthy periods of time and/or perform mental tasks requiring vigilance quickly and accurately”. Complex attention is important for self-regulation and behavioural control, e.g. holding information in the head while performing mental arithmetic. Executive function is “how well a subject recognizes rules, categories, and manages or navigates rapid decision making”. Executive function ability is needed to “sequence tasks and manage multiple tasks simultaneously as well as tracking and responding to a set of instructions”. Processing speed is the ability to understand and process new information quickly. The ability is important for fitness to drive, occupation tasks, and possible danger/risk signs. Cognitive flexibility is the ability to switch attention between tasks, e.g. focusing on writing an email then answering a phone call.
The CNS-VS grades severity of impairment based on an age-matched normative comparison database [16], given normal aging affects performance on all CNS-VS tests. Age-standardised domain scores (standardised to a mean of 100, with a standard deviation [SD] of 15) were calculated from the American age-matched normative data provided by the CNS-VS test developers (US norms). The database of 1650 healthy subjects without head injury, past neurological or psychiatric disorders, or learning disabilities had a mean age of 48.7 ± 11.1 for the 631 subjects aged 30–69 years. Higher standardised scores reflect higher levels of cognitive functioning. A threshold score of >110 indicates high function and high capacity, 90–110 represents normal function and normal capacity, 80–90 represents slight deficit and slight impairment, 70–79 represents possible moderate deficit and impairment, and <70 represents likely deficit and impairment [16]. An evaluation of the sensitivity and specificity of the CNS-VS test with identification of the score thresholds that best discriminate healthy people (normal) from people with mild cognitive impairment and patients with mild dementia has been conducted [17]; however, information about misclassification rates at the threshold scores does not appear to have been published. We therefore reported mean and SD values for the groups and plotted them to indicate the equivalent effect sizes for deviations from the US norms 100 standardisation point. The SDs indicate individual differences.
To explore the potential association of concussion history on cognitive functioning, data from all three former player groups were combined (due to the low number of rugby union players experiencing no concussions) and then separated into those who had experienced one or more concussions during their playing history and those who had not experienced any concussions.
2.5 Statistical Analyses
Data were analysed using SAS/STAT version 9.4 (SAS Institute, Inc., Cary, NC, USA) and customized Microsoft Excel spreadsheets (Microsoft Corporation, Redmond, WA, USA). Cohen’s d effect size statistics were calculated for comparisons across player groups (elite rugby, community rugby, non-contact sport), and concussion groups (one or more self-reported concussions versus no recalled concussions). Comparisons with both player and concussion groups were also made to the American age-matched normative data provided by the CNS-VS test developers (US norms). Effect sizes of 0.20 and above were considered as showing a difference worthy of consideration. The following descriptors were used for sizes of effects: trivial, <0.19; small, 0.20–0.59; moderate, 0.60–1.19; and large >1.20 [18].
No significant correlations were observed between former players’ demographic characteristics (e.g. age, education level, ethnicity, alcohol use) or sport played/level with the neuropsychological variables, therefore these factors were not used as covariates in analyses.
3 Results
3.1 Former-Player Demographics
Of the 485 former players enrolled in the RugbyHealth project, 366 (75 %) completed the CNS-VS test. The age range of former players was 29–72 years (mean ± SD age 43.3 ± 8.2 years; 103 elite rugby, 41.3 ± 7.5; 198 community rugby, 44.9 ± 8.4; 65 non-contact sport, 42.1 ± 7.7). Retirement from competitive sport ranged from a few months to 50+ years.
Characteristics of the former-player group (Table 1) were similar, except there were fewer non-European participants in the non-contact-sport players group. Participants in the two rugby groups sustained substantially more concussions per player than the non-contact-sport group (Table 1). Whereas 84.5 % of elite players reported having had at least one concussion, the rate among the community players was 77 %, and 23.1 % among non-contact players.
3.2 Sport Group Differences for Cognitive Function
Table 2 shows CNS-VS scores for each cognitive domain, with effect size comparisons between the New Zealand sport groups and the US norms. Positive effect sizes indicate that the sample group performed, on average, better than the US norms, while those with a negative sign indicate worse performance.
The elite-rugby group performed worse on tests of complex attention (effect size −0.67, 95 % confidence interval [CI] −1.07 to −0.26), processing speed (−0.51, −0.89 to −0.12), executive functioning (−0.41, −0.80 to −0.02), and cognitive flexibility (−0.37, −0.74 to 0.00) than the non-contact-sport group, and worse than the community-rugby group on complex attention (−0.38, −0.71 to −0.05). The community-rugby group performed worse than the non-contact group on executive functioning (−0.51, −0.89 to −0.12) and cognitive flexibility (−0.39, −0.69 to −0.08).
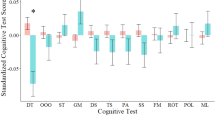
All three former-player groups performed worse than the US norms on verbal memory (elite rugby: −0.36, −0.60 to −0.12; community rugby: −0.54, −0.72 to −0.36; non-contact sport: −0.39, −0.69 to −0.08) and reaction time (elite rugby: −0.50, −0.69 to −0.30; community rugby: −0.61, −0.78 to −0.45; non-contact sport: −0.73, −0.98 to −0.48) (Fig. 1). Additionally, rugby groups performed worse on processing speed (elite rugby: −0.51, −0.75 to −0.26; community rugby: −0.32, −0.48 to −0.17), cognitive flexibility (elite rugby: −0.26, −0.47 to −0.05; community rugby: −0.27, −0.41 to −0.13) and executive functioning (elite rugby: −0.24, −0.45 to −0.03; community rugby: −0.23, −0.37 to −0.10) than the US norms. The community-rugby group performed worse than the US norms on composite memory (−0.31, −0.48 to −0.14), while the community-rugby group and the non-contact-sport group performed slightly better than the US norms on complex attention (community rugby: 0.22, 0.08–0.35; non-contact sport: 0.40, 0.20–0.60), as did the elite-rugby group in relation to motor speed (0.38, 0.19–0.57).

CNS-VS scores for each RugbyHealth player group compared with the US normative sample and each other, using Hopkins’ scale of effect sizes. The US norms mean score for each standardised variable was 100, with an SD of 15. The SD error bars for the means are bold for non-contact sport, dashed with half top for community rugby, and solid with full top for elite rugby. CNS-VS CNS Vital Signs test, SD standard deviation
All three player groups had greater individual differences than US norms on composite memory, verbal memory and reaction time. The elite-rugby group also had greater individual differences on processing speed and complex attention, and the community-rugby group had greater individual differences on psychomotor speed and motor speed.
3.3 Concussion History Group Differences for Cognitive Function
The average number of concussions recalled per player was 3.5 ± 2.0 for elite rugby, 2.9 ± 2.2 for community rugby and 0.4 ± 0.8 for non-contact sport. Regardless of sport, former players who recalled one or more concussions (elite rugby, 85 %; community rugby, 77 %; non-contact, 23 %) had worse scores on cognitive flexibility (effect size −0.35, 95 % CI −0.62 to −0.08), executive functioning (−0.27, −0.54 to −0.01) and complex attention (−0.28, −0.55 to −0.02) than former players who did not recall experiencing a concussion (Table 3).
Compared with the US norms, reaction times were moderately worse for both the ‘no concussion’ group (−0.63, −0.84 to −0.42) and the ‘one or more concussions’ group (−0.62, −0.77 to −0.48) (Fig. 2). Verbal memory deficits were also slightly worse for both the no concussion group (−0.48, −0.75 to −0. 20) and the one or more concussions group (−0.47, −0.64 to −0.31) compared with the US norms. The one or more concussions group had slightly worse deficits in processing speed (−0.38, −0.52 to −0.23), composite memory (−0.28, −0.43 to −0.12), cognitive flexibility (−0.28, −0.42 to −0.15) and executive functioning (−0.23, −0.36 to −0.09) compared with the US norms, while the no concussion group had slightly better performance than the US norms on motor speed (0.38, 0.18–0.57), complex attention (0.31, 0.15–0.48), visual memory (0.21, 0.00–0.42) and psychomotor speed (0.20, 0.00–0.40).

CNS-VS scores for the no concussion group and the one or more concussions group compared with the US normative sample and each other, using Hopkins’ scale of effect sizes. The US norms mean score for each standardised variable was 100, with an SD of 15. The SD error bars for the means are bold for no concussions, dashed for one or more concussions. CNS-VS CNS Vital Signs test, SD standard deviation
4 Discussion
The acute and long-term effects of concussive and subconcussive head impacts on brain health have gained attention over recent years [19–22]. Traumatic brain injury may predispose individuals to early-onset dementia and cognitive impairment, substance use disorders [23], depression [24, 25], neurodegenerative disease [26], and decreased psychomotor function [27, 28]. There is evidence of associations between head trauma and disturbed motor control [29], such as slowness of movement, incoordination, and impaired motor learning, although no direct causal links have been established to date [30]. A study examining relationships among concussion history, current symptoms and cognitive functioning (using the CNS-VS battery) among currently active soldiers found those with more previous concussions reported a greater number of current symptoms; however, no significant differences in cognitive function were observed between groups [31].
Disturbances to processing speed, memory and executive function are evident after mild traumatic brain injury, and can persist for prolonged periods after the initial injury [32, 33]. Recurrent concussions are suspected of promoting the development of long-term neurological disorders [8, 34]. Long-term brain electrophysiological changes in athletes with a history of multiple concussions [35–38] have been reported. Brain function decline in healthy retired athletes 3 decades post-concussion [37], assessed using neuropsychological and motor indices, has provided evidence for chronicity of cognitive and motor system changes consecutive to sports concussion [39].
Injuries have been reported at all levels of rugby, and there is preliminary evidence of long-term cognitive vulnerability in association with school-level participation in rugby [40]. A study of 27 South African rugby players, using a different battery of neuropsychological tests than in our study, showed that rugby players had consistently worse visuomotor processing speed than 18 age-matched, non-contact-sports participants [41]. This is consistent with our finding that rugby players performed worse than non-contact-sports people on some measures of neurocognitive function. The South African rugby players did not progress as well academically as the comparison group [40].
Our study provided a snapshot of the current neuropsychological health of former rugby players at elite or community level, and a comparison group of former non-contact-sport (cricket and hockey) players. The results provide evidence about clear small-to-moderate deficits in neurocognitive functioning for former rugby players and former athletes who had sustained concussion. The pattern of CNS-VS scores by group across the domains varied. There were two measures (cognitive flexibility and executive functioning) where both the elite and community rugby athletes were worse than the non-contact controls (i.e. 2 of 11 measures). In addition, compared with the non-contact controls, there were deficits for the elite-rugby group in complex attention and processing speed, and for the community-rugby group in executive functioning and cognitive flexibility (i.e. each group had 4 of 11 measures showing deficits). The test on which all the groups performed worst was reaction time, with trivial differences across the groups. We found the reaction time scores surprising as we did not expect our participants to perform worse on that measure than the aged-matched US norms. We do not have an explanation for why the reaction time scores were so poor.
Gualtieri and Johnson [17] indicated that tests which best discriminated between healthy people and people with mild cognitive impairment were memory, processing speed, and cognitive flexibility. We found an association between concussion history and some measures of cognitive functioning, notably cognitive flexibility, executive functioning, and complex attention. Given the substantially greater number of concussions in the rugby groups, these results reinforce the concern that rugby concussion injuries may have a long-term impact on neuropsychological health. The findings are of importance given the long periods of time (several decades in some instances) between playing rugby and sustaining concussion and time of cognitive assessment. Our results support those of De Beaumont et al. [37] who also reported brain function decline in healthy retired athletes who sustained their last sports concussion in early adulthood. In a cross-sectional study, former professional North American football players who sustained recurrent mild traumatic brain injury also showed cumulative effects and late-life cognitive impairment, suggesting increased neurological vulnerability to head impacts [25, 42].
The question ‘how well did our players perform on the tests?’ is only interpretable with reference to how people normally perform on the tests. Although there was a moderate difference in complex attention between the elite-rugby group and the non-contact group, the mean score for the elite players on complex attention was 99, which was near the US standardised average of 100. The moderate difference between the New Zealand groups is due to the non-contact-sports people performing better than the US standardised average, with a mean score of 106. With the exceptions of verbal memory and reaction time, the performance of former non-contact players on neurocognitive function variables was either close to normal levels or slightly higher than average when compared with the US sample of age-matched norms [16]. The performance of rugby players was slightly lower (small to moderate effect sizes) than the US norms on 5 of 11 measures (cognitive flexibility, processing speed, executive functioning, reaction time and verbal memory) and an additional measure for community players (composite memory). The elite players performed slightly better than the US norms on motor speed, as did the community players on complex attention. A normative non-athlete group from New Zealand was not available for comparison. While we have no a priori reason to expect substantial differences in test battery scores between Americans and New Zealanders, we do not know whether standardising the scores of sports people from New Zealand against the US norms affects the validity of results. The CNS-VS test is not specific to athletes [15].
It must be noted that there was greater variability in the scores of the elite-rugby group on some of the domains than would be expected by comparison with the normative data, even though their scores were not greatly different from the norms overall. For example, the elite-rugby group’s poor performance on processing speed also showed higher variability than the US norms, which implies that while most people performed as might be expected on the test, there was a higher-than-normal frequency of people in the tail of the distribution. To establish whether people who appeared to be performing poorly are actually impaired would require clinical evaluation, most likely conducted longitudinally.
The majority of rugby players in our study began playing senior rugby in 1980–1990. Most elite rugby players finished playing at an elite level between 1990 and 2000, and most community players finished playing between 2000 and 2010. The nature of rugby has changed over time (the modern game has larger, faster, stronger players, experiencing greater impact forces), as has awareness of medical issues (such as concussion) and availability of side-line medical assessment and better treatment of players’ injuries. Therefore, the nature of long-term health effects from rugby may change over time.
4.1 Strengths and Limitations of the Study
This was the first study to describe the long-term neurophysiological characteristics of former elite rugby, community rugby and non-contact-sport athletes in New Zealand. The inclusion of both elite/professional-level and community-level players increases the applicability of the findings to a wide range of retired rugby players. The study had a large proportion (50.5 %) of retired All Blacks (New Zealand national rugby team) in the elite rugby sample, which approximated 10 % of the living former All Blacks. Our analysis of the demographic characteristics indicated the groups were similar (except had higher income levels) to the general population, as determined by the 2006–2013 New Zealand census surveys [43].
Recruitment fell short for both the elite-rugby and non-contact-sport groups, reducing the statistical power to detect differences among groups; therefore, the results need to be interpreted accordingly. Like all studies involving recruitment of volunteers, the study was subject to non-response bias.
Data on concussion history were obtained from self-report, thus recall bias is a potential issue. Self-reported concussion does not necessarily align with medically diagnosed concussion [44]; however, self-reporting of prior concussion has been shown to be a reliable ordinal measure and may reflect some head injuries that were not previously reported [45, 46]. We did not assess the time since the last concussion, nor did we assess concussions that were not related to sport.
The CNS-VS test is not a specific diagnostic tool; however, computer-based tests of cognition can help to identify impairment [47, 48] and allow screening to be conducted in a cost-effective, standardised and time efficient manner across a large population [15]. Discriminant validity of the CNS-VS test is supported by studies of patients with mild cognitive impairment and dementia, post-concussion syndrome and severe traumatic brain injury, and depression (treated and untreated) [15], and it has been shown to be a reliable, valid test battery for cognitive functioning [15]. However, the test does have some limitations. According to the developers of the test, the CNS-VS computer-based test “… is not a substitute for formal neuropsychological testing, it is not diagnostic, and it will have only a limited role in the medical setting, absent the active participation of consulting neuropsychologists”. However, the CNS-VS test was the most suitable tool available for the type of study we conducted. As the test was self-administered in the home or work environment, contextual factors that were not controlled may have affected performance, although this is likely to be equivalent among the three groups. Education and special skills may affect CNS-VS test performance [16]; however, our retired-player groups had similar levels of education therefore we do not believe education level influenced the results.
The cross-sectional nature of the study limits the ability to infer causality between rugby/non-contact-sport participation, concussion and cognitive functioning in later life. For example, we cannot eliminate the possibility that the retired player groups may have differed in neurocognition prior to participation in sport.
4.2 Further Research Questions and Injury Control Opportunities
This study suggests a number of areas for further research. Notably, what will be the implications of the observed differences in test performance at group level for individuals in terms of clinical differences and ongoing neurological function in their everyday lives? To answer this, ongoing follow-up of rugby players would be needed.
From an injury prevention standpoint, work on scrums in New Zealand appears to have been successful in reducing some neck injuries [49]; however, the tackle is the phase of play in which most concussions occur. The tackle is a central element of rugby as a collision sport. We need to better understand the mechanisms of injury and phases of play so we can implement further injury prevention strategies to minimise the risk of injury. A number of variants of rugby exist. From a public health perspective, ongoing development and promotion of low-contact forms of the sport has the potential to provide most of the benefits of engaging in physical activity while avoiding many of the injury risks typically associated with participation.
There is a need for increased awareness of the potential long-term health impact of concussion in rugby and a culture shift towards taking head impact more seriously. Several high profile players in New Zealand have retired from professional rugby due to ongoing symptoms from having repeated concussions. Improved disclosure of head injury symptoms is needed if injured players are to receive diagnostic care and treatment to help mitigate potential long-term negative effects of concussion [7]. Accelerometer and video systems being trialled in community senior [50] and junior [51] rugby, may be able to provide data that will assist with monitoring players for concussion incidence. Additional refinement of concussion management tools and protocols may have an effect on long-term health outcomes. For example, the King–Devick test has been shown to be useful in the management of concussion in amateur rugby union and rugby league in New Zealand [52, 53].
This cross-sectional study has highlighted that playing rugby or sustaining concussions may be linked to worse cognitive functioning. Further studies examining players during and after their retirement from competitive sport are needed to clarify any associations between concussion and subconcussion exposure (number and severity) with neurocognition and multiple health risk factors. Academic performance progression in young athletes who have sustained concussion should also be examined.
4.3 Recommendations
Recommendations to address the implications for player neurocognitive health are as follows.
-
Players need to be advised of the potential increased long-term risk of cognitive impairment from playing rugby or sustaining concussion so they can make informed choices about engagement in rugby, and return to play following injury.
-
There is a need for prospective cohort studies of neurological health in current and former rugby players, taking into account exposure to concussive and subconcussive events.
5 Conclusions
This study provides evidence of small to moderate deficits in cognitive functioning of former elite and community-level rugby players in comparison to former non-contact-sport players, and in former players who have sustained concussions in comparison to former players who had no concussions. The rugby community needs to be aware of the potential risks if players sustain concussion, and ensure that players gain access to medical support if injury is suspected. There is a need for further prospective studies of neurological health in rugby players, taking into account concussive and subconcussive exposure.
References
McCrory P, Meeuwisse WH, Aubry M, Cantu B, Dvořák J, Echemendia RJ, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. 2013;47(5):250–8.
King D, Gissane C, Brughelli M, Hume PA, Harawira J. Sport-related concussions in New Zealand: a review of 10 years of Accident Compensation Corporation moderate to severe claims and costs. J Sci Med Sport. 2014;17(3):250–5.
England Professional Rugby Injury Surveillance Project Steering Group. England Professional Rugby Injury Surveillance Project 2013–2014 Season Report. Twickenham. 2014.
Theadom A, Starkey NJ, Dowell T, Hume PA, Kahan M, Feigin V. Sports-related brain injury in the general population: an epidemiological study. J Sci Med Sport. 2014;17(6):591–6.
Quarrie KL, Murphy IR. Towards an operational definition of sports concussion: identifying a limitation in the 2012 Zurich consensus statement and suggesting solutions. Br J Sports Med. 2014;48(22):1589–91.
Carney N, Ghajar J, Jagoda A, Bedrick S, Davis-O’Reilly C, du Coudray H, et al. Executive summary of concussion guidelines step 1: systematic review of prevalent indicators. Neurosurgery. 2014;75:S1–2.
Kerr ZY, Register-Mihalik JK, Marshall SW, Evenson KR, Mihalik JP, Guskiewicz KM. Disclosure and non-disclosure of concussion and concussion symptoms in athletes: review and application of the socio-ecological framework. Brain Inj. 2014;28(8):1009–21.
Gardner A, Iverson GL, Williams WH, Baker S, Stanwell P. A systematic review and meta-analysis of concussion in rugby union. Sports Med. 2014;44(12):1717–31.
Kirkwood G, Parekh N, Ofori-Asenso R, Pollock AM. Concussion in youth rugby union and rugby league: a systematic review. Br J Sports Med. 2015;49(8):506–10.
Broglio SP, Eckner JT, Paulson HL, Kutcher JS. Cognitive decline and aging: the role of concussive and subconcussive impacts. Exer Sport Sci Rev. 2012;40(3):138–44.
Iverson GL, Brooks BL, Collins MW, Lovell MR. Tracking neuropsychological recovery following concussion in sport. Brain Inj. 2006;20(3):245–52.
Iverson GL, Gaetzy M, Lovell MR, Collins MW. Cumulative effects of concussion in amateur athletes. Brain Inj. 2004;18(5):433–43.
Hume PA, Quarrie K, Lewis G, Theadom A. IRB/NZR/AUT RugbyHealth project final report. A technical report to the International Rugby Board and New Zealand Rugby. Auckland: Sport Performance Research Institute New Zealand, Auckland University of Technology, New Zealand. 2015.
Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption—II. Addiction. 1993;88(6):791–804.
Gualtieri CT, Johnson LG. Reliability and validity of a computerized neurocognitive test battery CNS Vital Signs. Arch Clin Neuropsych. 2006;21(7):623–43.
Boyd A. CNS Vital Signs manual. 2015. http://www.cnsvitalsigns.com/WhitePapers/CNSVS-BriefInterpretationGuide.pdf. Accessed Feb 2015
Gualtieri CT, Johnson LG. Neurocognitive testing supports a broader concept of mild cognitive impairment. Am J Alzheimers Dis Other Demen. 2005;20(6):359–66.
Hopkins WG. A scale of magnitudes for effect statistics. In: Hopkins WG (ed). A new view of statistics. 2002. http://www.sportsci.org/resource/stats/effectmag.html. Accessed 26 Jan 2009.
Alberts JL, Linder SM. The utilization of biomechanics to understand and manage the acute and long-term effects of concussion. Kinesiol Rev. 2015;4(1):39–51.
DeKosky S, Ikonomovic M, Gandy S. Traumatic brain injury: football, warfare, and long-term effects. N Engl J Med. 2010;363:1293–6.
Hollis SJ, Stevenson MR, McIntosh AS, Shores EA, Collins MW, Taylor CB. Incidence, risk, and protective factors of mild traumatic brain injury in a cohort of Australian non professional male rugby players. Am J Sport Med. 2009;37(12):2328–33.
Shuttleworth-Edwards AB, Smith I, Radloff SE. Neurocognitive vulnerability amongst university rugby players versus noncontact sport controls. J Clin Exp Neuropsychol. 2008;30(8):870–84.
West S. Substance abuse among persons with traumatic brain injury: a review. Neurorehab Neural Repair. 2011;25(1):3–8.
Holsinger T, Steffens D, Phillips C, Helms M, Havlik R, Breitner J. Head injury in early adulthood and the lifetime risk of depression. Arch Gen Psychiatry. 2002;59(1):17–22.
Guskiewicz KM, Marshall SW, Bailes J, McCrea M, Harding HP, Matthews A, et al. Recurrent concussion and risk of depression in retired professional football players. Med Sci Sport Exer. 2007;39(6):903–9.
Lehman E, Hein M, Baron S, Gersic C. Neurodegenerative causes of death among retired National Football League players. Neurology. 2012;79(19):1970–4.
Casson IR, Siegel O, Sham R, Campbell EA, Tarlau M, DiDomenico A. Brain damage in modern boxers. JAMA. 1984;251(20):2663–7.
Gronwall D, Wrightson P. Delayed recovery of intellectual function after minor head injury. Lancet. 1974;304(7881):605–9.
Rabadi M, Jordan B. The cumulative effect of repetitive concussion in sports. Clin J Sports Med. 2001;11(3):194–8.
Austin D, Gabbett T, Jenkins D. Tackling in professional rugby league. J Strength Cond Res. 2011;25(6):1659–63.
Dretsch MN, Silverberg ND, Iverson GL. Multiple past concussions are associated with ongoing post-concussive symptoms but not cognitive impairment in active-duty army soldiers. J Neurotrauma. 2015;32(17):1301–6.
Arciniegas DB, Anderson CA, Topkoff J, McAllister TW. Mild traumatic brain injury: a neuropsychiatric approach to diagnosis, evaluation, and treatment. Neuropsychiatr Dis Treat. 2005;1:311–27.
Fleminger S, Ponsford J. Long term outcome after traumatic brain injury. Br Med J. 2005;331:1419–20.
Decq P, Gault N, Blandeau M, Kerdraon T, Berkal M, ElHelou A, et al. Long-term consequences of recurrent sports concussion. Acta Neurochir (Wien). 2016;158(2):289–300.
De Beaumont L, Brisson B, Lassonde M, Jolicoeur P. Long-term electrophysiological changes in athletes with a history of multiple concussions. Brain Inj. 2007;21:631–44.
De Beaumont L, Lassonde M, Leclerc S, Théoret H. Long-term and cumulative effects of sports concussion on motor cortex inhibition. Neurosurgery. 2007;61(2):329–36.
De Beaumont L, Theoret H, Mongeon D, Messier J, Leclerc S, Tremblay S, et al. Brain function decline in healthy retired athletes who sustained their last sports concussion in early adulthood. Brain. 2009;132(Pt 3):695–708.
Dean PJA, Steer A. Long-term effects of mild traumatic brain injury on cognitive performance. Front Hum Neurosci. 2013;7:30.
McCrory P, Meeuwisse WH, Kutcher JS, Jordan BD, Gardner A. What is the evidence for chronic concussion-related changes in retired athletes: behavioural, pathological and clinical outcomes? Br J Sports Med. 2013;47:327–30.
Alexander DG, Shuttleworth-Edwards AB, Kidd M, Malcolm CM. Mild traumatic brain injuries in early adolescent rugby players: long-term neurocognitive and academic outcomes. Brain Inj. 2015;29(9):1113–25.
Shuttleworth-Edwards AB, Radloff SE. Compromised visuomotor processing speed in players of Rugby Union from school through to the national adult level. Arch Clin Neuropsychol. 2008;23(5):511–20.
Guskiewicz KM, Marshall SW, Bailes J, McCrea M, Cantu RC, Randolph C, et al. Association between recurrent concussion and late-life cognitive impairment in retired professional football players. Neurosurgery. 2005;57(4):719–26.
Statistics New Zealand. Statistics New Zealand census data. Wellington. Statistics New Zealand. 2006. http://www.stats.govt.nz/Census/about-2006-census/information-by-variable/cigarette-smoking-behaviour.aspx. Accessed 15 Dec 2014.
Kerr ZY, Mihalik JP, Guskiewicz KM, Rosamond WD, Evenson KR, Marshall SW. Agreement between athlete-recalled and clinically documented concussion histories in former collegiate athletes. Am J Sport Med. 2015;43(3):606–13.
Kerr Z, Marshall S, Guskiewicz K. Reliability of concussion history in former professional football players. Med Sci Sport Exerc. 2012;44(3):377–82.
Kerr Z, Marshall S, Harding HJ, Guskiewicz K. Nine-year risk of depression diagnosis increases with increasing self-reported concussions in retired professional football players. Am J Sport Med. 2012;40(10):2206–12.
Arnaiz E, Almkvist O, Ivnik RJ, Tangalos EG, Wahlund LO, Winblad B, et al. Mild cognitive impairment: a cross-national comparison. J Neurol Neurosurg Psychiatry. 2004;75(9):1275–80.
Bruscoli M, Lovestone S. Is MCI really just early dementia? A systematic review of conversion studies. Int Psychogeriatr. 2004;16(2):129–40.
Quarrie KM, Gianotti S, Hopkins WG, Hume PA. Effect of nationwide injury prevention programme on serious spinal injuries in New Zealand rugby union. Br Med J. 2007;334:1150–3.
King DA, Hume PA, Brughelli M, Gissane C. Instrumented mouthguard acceleration analyses for head impacts in amateur rugby union players over a season of matches. Am J Sports Med. 2015;43(3):614–24.
King DA, Hume PA, Gissane C, Clark T. Similar head impact acceleration measured using instrumented ear patches in a junior rugby union team during matches in comparison with other sports. J Neurosurg Pediatr. 2016;18(1):65–72.
King D, Brughelli M, Hume PA, Gissane C. Concussions in amateur rugby union identified with the use of a rapid visual screening tool. J Neurol Sci. 2013;326(1–2):59–63.
King D, Gissane C, Hume PA, Flaws M. The King-Devick test was useful in management of concussion in amateur rugby union and rugby league in New Zealand. J Neurol Sci. 2015;351(1–2):58–64.
Acknowledgments
We thank Dr Martin Raftery (World Rugby/International Rugby Board [IRB]) for initiating the IRB/New Zealand Rugby/Auckland University of Technology (IRB/NZR/AUT) RugbyHealth project and for providing feedback on the technical report that formed the basis of this article. Thanks to Peter Griffiths and Serene Lorimer who provided research administration for the project, Dr Ian Murphy (New Zealand Rugby), Heath Mills (New Zealand Rugby Players Association) and Rob Nichol (New Zealand Cricket Players Association) who endorsed the project and helped with promotion of the study and recruitment of players. We also gratefully recognise the support of Alan Boyd, Chief Executive Officer (CEO) of CNS-VS, for his support and for providing advice on the analysis and interpretation of the data.
Contributors
Professor Patria Hume collaborated in designing the overarching IRB/NZR/AUT RugbyHealth project, was responsible for the original conception of the study, wrote the funding application, obtained ethical approval, helped recruit participants, helped with analyses of data, provided interpretation of the results, and co-authored the manuscript. Dr Alice Theadom determined the assessment protocols, helped recruit participants, provided interpretation of the results, and co-authored the manuscript. Associate Professor Gwyn Lewis helped recruit participants, helped with analyses of data, provided interpretation of the results, and co-authored the manuscript. Dr Ken Quarrie (New Zealand Rugby) initiated the IRB/NZR/AUT RugbyHealth project, analysed the data, provided interpretation of the results, and co-authored the manuscript. Scott Brown provided liaison for participants for the study, helped recruit participants, and co-authored the manuscript. Dr Rosamund Hill provided clinical interpretation advice and co-authored the manuscript. Professor Stephen Marshall provided statistical advice and co-authored the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The study was funded by World Rugby (IRB), the Sport Performance Research Institute New Zealand (SPRINZ), the National Institute for Stroke and Applied Neurosciences (NISAN), and the Health and Rehabilitation Research Institute (HRRI) of AUT, and NZR.
Competing interests
Kenneth L. Quarrie was employed by NZR prior to and throughout the duration of the project. World Rugby and NZR provided funding for the project. Patria A. Hume, Alice Theadom, Gwyn N. Lewis, Scott R. Brown, Rosamund Hill and Stephen W. Marshall declare that they have no conflicts of interest.
Ethical approval
The study was performed in accordance with the ethical standards of the Declaration of Helsinki, given ethics approval was obtained from the AUT Ethics Committee (AUTEC #12/252). Participants provided informed consent after reading a participant information sheet about the project.
Additional information
This article is part of the Topical Collection on Rugby Health.
Rights and permissions
About this article

Cite this article
Hume, P.A., Theadom, A., Lewis, G.N. et al. A Comparison of Cognitive Function in Former Rugby Union Players Compared with Former Non-Contact-Sport Players and the Impact of Concussion History. Sports Med 47, 1209–1220 (2017). https://doi.org/10.1007/s40279-016-0608-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-016-0608-8