
Abstract
Background
Fundamental movement skill (FMS) competence is positively associated with physical activity (PA). However, levels of both FMS and PA are lower than expected. Current reviews of interventions to improve FMS and PA have shown that many school-based programs have achieved positive outcomes, yet the maintenance of these interventions is variable. Teachers play a central role in the success and longevity of school-based interventions. Despite the importance of teacher engagement, research into the nature and quality of teacher training in school-based PA and FMS interventions has received little attention.
Objective
The aim of this systematic review was to investigate the type and quantity of teacher training in school-based physical education PA and/or FMS interventions, and to identify what role teacher training had on the intervention outcome.
Methods
A systematic search of eight electronic databases was conducted. Publication date restrictions were not implemented in any database, and the last search was performed on 1 March 2015. School physical education-based interventions facilitated by a school teacher, and that included a quantitative assessment of FMS competence and/or PA levels were included in the review.
Results
The search identified 39 articles. Eleven of the studies measured FMS, 25 studies measured PA and three measured both FMS and PA. Nine of the studies did not report on any aspect of the teacher training conducted. Of the 30 studies that reported on teacher training, 25 reported statistically significant intervention results for FMS and/or PA. It appears that teacher training programs: are ≥ 1 day; provide comprehensive subject and pedagogy content; are framed by a theory or model; provide follow-up or ongoing support; and measure teacher satisfaction of the training, are more effective at improving student outcomes in FMS and/or PA. However, the provision of information regarding the characteristics of the teacher training was largely inadequate. Therefore, it was difficult to ascertain which teacher training characteristics were most important in relation to intervention effectiveness.
Conclusion
It is clear that whilst teachers are capable of making substantial improvements in student outcomes in PA and FMS, the findings of this review suggest the teacher training component of school-based PA and/or FMS interventions is not only under-reported but is under-studied, and, perhaps as a result, the value of teacher training is not widely understood. What remains unclear, due to poor reporting, is what role teacher training is having on these outcomes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
There is some evidence that teacher training programs within school-based fundamental movement skill (FMS) and/or physical activity (PA) interventions that: are ≥1 day; provide comprehensive subject and pedagogy content; are framed by a theory or model; provide follow-up or ongoing support; and measure teacher satisfaction of the training, are more effective at improving student outcomes in FMS and/or PA. |
However, this finding should be viewed with caution, as studies reporting on PA and/or FMS interventions in school physical education generally do not provide adequate detail on the characteristics of teacher training required for the intervention. |
To better inform the design of future effective school-based FMS and/or PA interventions, more consistent and comprehensive approaches to the reporting of teacher training are recommended. |
1 Introduction
Regular physical activity (PA) is associated with a large number of physical, psychological, and social health benefits for young people [1–3]. It is recommended that adolescents accumulate 60 min or more of moderate to vigorous physical activity per day, yet 80 % of adolescents fail to meet this [4–6]. Furthermore, PA declines with age, especially throughout adolescence [7]. Thus, we need to know more about factors associated with low levels of PA and what prevents and motivates participation in PA [8–10]. A well-documented correlate of PA in young people is proficiency in fundamental movement skills (FMS) [11]. FMS are typically classified into ‘object control skills’ (catching and throwing), ‘locomotor skills’ (running and jumping), and ‘stability skills’ (balancing and twisting) [11–13]. Competency in a range of FMS in childhood has been found to be a predictor of PA in adolescence [14]. However, many children fail to meet FMS proficiency level benchmarks [15–18]. As there is strong evidence for a positive association between FMS competency and PA in children and adolescents [11, 19], low FMS proficiency in children may negatively impact on their potential to be physically active in adolescence and adulthood.
School, via the curriculum, ethos, and community has been widely acknowledged as an ideal setting in which to provide PA opportunities, educate students about the importance of PA [20], and provide an important avenue for the delivery of health promotion programs [21]. The Health and Physical Education (HPE) curriculum is considered the focal point for PA promotion and FMS development in the school setting [22]. Indeed, school-based HPE programs have the potential to improve FMS proficiency and slow the age-related decline in PA in students [23, 24]. As such, these outcomes have been the focus of numerous school-based interventions, and multiple associated systematic reviews, and although not all school-based interventions have had positive outcomes [24], many interventions have been generally successful, showing small to moderate effect sizes in PA and/or FMS [25–27]. Furthermore, the variability in these intervention outcomes does not change the need to understand the characteristics and effects of teacher training in such interventions, as it is important to identify what sort of teacher training is most effective, in order to design the most effective FMS/PA interventions.
Few school-based FMS and/or PA studies have conducted follow-up assessments, however, to identify the long-term impact of the interventions [28]. The ultimate goal of an intervention that aims to change behavior and improve outcomes should be maintenance [28]. Interventions that prove to be effective in the long term should arguably be better suited for widespread scalability and translation and therefore influence policy decisions, government spending, and ultimately the health of children and adolescents as they progress to adulthood [28].
The sustainability of a school-based program depends on the extent to which the teachers continue to implement the program [29]. A recent meta-analysis of over 800 students demonstrated that teaching quality is the strongest school-related factor in improving student learning and achievement [30]. The majority of school-based PA programs utilize existing teachers to deliver interventions [24, 31]. Therefore, identifying factors that encourage the sustained implementation of school-based interventions facilitated by existing teachers is a necessary step in understanding and orchestrating the long-term change process required for school-based PA and/or FMS programs to be successful [32].
Pre-service teacher education programs play a significant role in ensuring teacher readiness with regard to delivering effective PA and FMS programs in schools [33, 34]. However, helping teachers evoke long-term behavior change extends beyond what is provided in pre-service education [32]. Thus, there is a clear need for continuing professional development to promote ongoing teacher learning and improve teacher instructional practices [35, 36]. The positive influence that teacher training or professional development programs have on teaching behavior has been well established in several school disciplines (e.g., science, mathematics) [37–39]. Despite the correlation between teacher training and improved teacher instructional practices, the literature is fraught with concern surrounding the current state of professional development in physical education (PE) [40, 41]. Indeed, a major barrier to implementing quality PE is the lack of appropriate teacher training [42].
The quality of teacher training in school-based PA and FMS interventions has received little attention [43]. Similarly, research on the impact of the nature and quality of teacher training in PE interventions targeting FMS and PA is largely absent from the literature [24, 28]. There is some evidence, with regard to broader teacher education, that professional development efforts that are guided by, provide both academic subject matter as well as pedagogy content, encourage a collaborative approach and active learning, are embedded within the role of a teacher, and are sustained and intensive, are more likely to result in improving teaching practices and improving student learning outcomes [44]. Therefore, the aim of this systematic review was to explore characteristics of teacher training used in school-based PE interventions in PA and/or FMS, and to investigate the importance of teacher training on these outcomes. The specific objectives of the evidence synthesis were to describe the following teacher training characteristics: the dose of training received; the modality of training; the model or theory used in the training; the characteristics of the trainer or facilitator and the trainee; trainee satisfaction with the program; and fidelity to the prescribed teaching practice. In addition, the review aimed to identify whether there is a link between certain teacher training characteristics and FMS and/or PA improvement.
2 Methods
The conduct and reporting of this review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement [45].
2.1 Inclusion Criteria
2.1.1 Types of Participants
Target groups were comprised of:
-
1.
Primary/elementary (approximately 5–12 years of age), middle (approximately 12–14 years of age), and/or secondary school (12–18, or 14–18 years of age in areas with middle school) students.
-
2.
Typically developing children or adolescents, which could include overweight or obese, or disadvantaged students.
2.1.2 Types of Interventions
Studies were included if:
-
1.
The intervention was school-based (primary, middle, or secondary) or curriculum-based, and conducted or facilitated by a school teacher within PE.
-
2.
A component of the intervention targeted physical activity and/or FMS improvement.
-
3.
Quantitative assessment or analysis of FMS competence and/or PA levels was a primary or secondary outcome of the study.
-
4.
The study design included an experimental or quasi-experimental randomized controlled trial (RCT).
2.2 Exclusion Criteria
Studies identified through the literature search were excluded if:
-
1.
They were conducted in school but not in PE (e.g., after-school program, recess or lunchtime).
-
2.
They were conducted in PE but not by a teacher employed by the school (e.g., intervention was facilitated by a member of the research team, or an external specialist employed specifically to facilitate the intervention).
-
3.
Target participants were from special populations (i.e., developmental delay).
-
4.
Interventions were conducted in early childcare, preschool, kindergarten (prior to school), or at university.
-
5.
They were unpublished reports, conference papers, or dissertations.
-
6.
They were not published in the English language.
2.3 Information Sources and Search
2.3.1 Study Selection
Relevant studies were identified by means of electronic searches on EBSCOhost and Informit and scanning reference lists of included articles. The EBSCOhost platform supplied access to: MEDLINE, PsycINFO, Scopus, ERIC, Education Source, Education Research Complete, and SPORTDiscus databases. On the Informit platform the health and education categories were searched. Each of the databases was searched independently. Publication date restrictions were not applied in any search, and the last search was conducted on 1 March 2015.
Search strategies used in the databases included combinations of key search terms, which were divided into four concepts: (1) setting (School* OR “secondary college” OR “secondary education” OR “primary education” OR “elementary education” OR “elementary school” OR “primary school” OR “middle school” OR “secondary school” OR “high school”); (2) study design (Intervention* OR program* OR strategy* OR trial* OR experiment* OR “Random Control Trial” OR “quasi-experimental”); (3) intervention type (“Physical*N2 active*” OR “physical education” OR “fundamental movement skill*” OR “fundamental motor skill*” OR “motor skill*” OR “movement skill*” OR “motor development”); (4) facilitator (Teacher OR Educator OR Leader OR Instructor). Boolean searches were also carried out using “AND” and “OR” to combine concepts. MEDLINE and Informit were searched separately as they have different limitations (e.g., Informit does not allow OR truncations in phrases).
Following the initial search, the first author (NL) removed all duplicates and screened the titles and abstracts. Only articles published or accepted for publication in peer-reviewed journals were considered. A second author (NE) checked decisions, and any disagreements were resolved by discussion and collaboration with a third author (LMB). Full-text articles were further evaluated separately for relevance by two authors (NL and NE) and labeled ‘yes’, ‘no’, or ‘maybe’. The reviewers conferred and, following discussion on any inconsistencies, agreement was reached on all articles. The reference lists of included articles were scanned to identify additional relevant articles.
2.3.2 Data Collection Processes
One author (NL) extracted study data relating to: the general characteristics of each study (i.e., author, date, study name, country, sample, study design, intervention design and duration, behavioral theories, and measures and outcomes); and the teacher training characteristics (i.e., reporting of teacher training, dose of training, model, theory or framework used in teacher training, trainee and trainee characteristics, trainer and trainer characteristics, trainee satisfaction with training, and fidelity of teaching).
2.3.3 Risk of Bias
Each of the included studies was independently analyzed by two reviewers (NL and NE) using a standardized process adapted from the Consolidated Standards of Reporting Trials Statements and previously used quality criteria [24] to obtain consistent data across all studies (Table 1). As recommended by the PRISMA statement, these items were not numerically summarized to provide final scores, instead each criterion was considered in isolation. Initial agreement between raters was high (95 %). Differences in risk of bias assessment were firstly discussed between NL and NE, and then any unresolved differences at this point were discussed within the group of five authors facilitated by author NL. Consensus was achieved on all included studies. Each item on the scale was coded as yes (Y) if ‘explicitly described and present’, no (N) if ‘absent’, or unclear (?) if ‘unclear or inadequately described’. Methodological ‘risk of bias’ scores are provided in Table 2.
3 Results
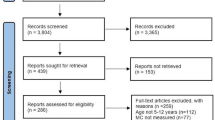
The initial search identified 5840 papers: 4884 via EBSCOhost, 283 via MEDLINE, and 673 via Informit. After removing duplicates and reviewing the titles and abstracts, 3911 were identified as being potentially relevant, and full-texts were then obtained. Of these, 3795 were excluded for not meeting one or more of the inclusion criteria. The search of reference lists from relevant papers and reviews yielded five more publications. 116 full-text articles were assessed for eligibility, 70 were subsequently excluded for several reasons (Fig. 1). This resulted in the inclusion of 46 publications, which covered 42 interventions. Seven papers described follow-up, protocol, process evaluation, and/or mediation analyses, so papers from a single study were combined and treated as one. The exception was McKenzie and Alcaraaz [46], as the authors reported on a different outcome (i.e., FMS) from the original research conducted by Sallis and McKenzie [47], which was PA; therefore, McKenzie and Alcaraaz [46] is included as an independent paper. The final review was conducted on 39 papers. An overview of study characteristics of the 39 eligible studies is presented in Electronic Supplementary Material Table S1.

Systematic reviews and meta-analysis (PRISMA) statement flowchart of studies through the review process
Seventeen studies were published between 2010 and 2014 [48–64], 16 studies between 2000 and 2009 [65–81], and six studies between 1990 and 1999 [46, 47, 82–85]. Most of the studies were conducted in the USA and Australia. Six studies were conducted in secondary schools (i.e., grades 7–12) [54, 56, 58, 65, 72, 75], three in middle school (i.e., grades 6–8) [55, 76, 80], one study investigated both primary (i.e., kindergarten–grade 6) and secondary school [51], and the remaining 30 were conducted in the primary school setting. There were 23 randomized control trials [46–48, 50, 53–55, 57–62, 65, 66, 70, 73–76, 80, 82, 83], and 17 quasi-experimental studies [49, 51, 52, 56, 63, 64, 67–69, 71, 72, 77–79, 81, 84, 85]. The sample sizes ranged from four [52] to approximately 5106 [83].
Twelve of the 39 studies did not report a behavioral theory or model used to inform the intervention [48, 49, 52, 56, 60–63, 67, 77, 84, 85]. The remaining 27 studies included behavioral theories, with the most predominant being the socio-ecological model [50, 57, 66, 75, 76, 80] and the social-cognitive model [59, 65, 69, 71, 80, 82, 83]. Thirty-three studies had a duration of 12 weeks or more [46, 47, 49–51, 54–66, 69–72, 74–80, 82–85], five of the studies reported an intervention of less than 12 weeks [48, 67, 68, 73, 86], and one study did not report the intervention duration [52].
Eleven of the studies measured FMS [46, 48, 49, 51, 56, 63, 64, 67, 73, 77, 84]. Significant FMS outcomes were reported in all but one [73]. Another 25 studies measured PA [47, 52–55, 57–62, 65, 66, 68, 69, 71, 72, 74–76, 79, 80, 82, 83, 85] Significant outcomes were reported in 18 of these, and non-significant outcomes were reported in seven studies [52, 53, 55, 62, 65, 80, 82]. Three studies measured both FMS and PA [50, 70, 78].
3.1 Teacher Training Characteristics
Teacher training was not reported in almost a quarter of the studies (23 %, 9/39) [48, 49, 52, 53, 63, 64, 67, 72, 77]. In one of these studies, it was reported that the teachers had received training prior to the intervention, yet no further teacher training detail was provided in the paper [49]. However, for eight studies, although new practices, content or pedagogy were implemented by the teacher as part of the intervention, teacher training was not reported. The remaining 30 studies did report some aspect of teacher training in the intervention, such as: (1) the dose of teacher training; (2) the model, theory or framework used in the teacher training; (3) the trainer and trainee, and their characteristics; (4) teacher satisfaction with the training; and (5) teacher fidelity in attending the training and delivering the training program (Tables 3, 4).
Of these studies, 25 achieved statistically significant intervention results for FMS and/or PA, yet the effect sizes, or actual changes in the intervention outcomes, were variable. Of the studies which reported a change in PA per day, four reported a change of >10 min per day [50, 57, 69, 83], one reported a change of 7 min per day [66], and five reported small/negligible change (5 min or less per day) [47, 59, 62, 65, 80]. The studies that reported on change in PA during PE, reported changes ranging from an 8 % [71] to a 23 % increase [85]. Four studies reported a small (>10) total percentage increase in PA [68, 70, 75, 78], and two others reported changes in unique measures of PA e.g., 1.4 pentathlon hours [60] or step counts [74]. Of the five studies which reported FMS outcomes, two reported small effect sizes [51, 56], one reported a unit change of 4.9 [50], and two studies reported increases in total FMS of 21 % [46] and 26 % [78] (Table 4).
3.1.1 Dose of Teacher Training
For the purpose of this review, the ‘dose’ of training that the teacher received was divided into three components: (1) the duration of training, (2) the mode of training (i.e., face-to-face, written resources, follow-up or ongoing support, additional resources, other), and (3) the content of the training (i.e., subject content, pedagogical content). Of the 30 studies that reported teacher training in the intervention, 22 described all three components of the dose [46, 47, 50, 54–62, 65, 66, 70, 71, 74, 76, 78, 79, 82, 83]; however, the degree of detail presented in each category was highly variable. Eight of the studies did not report on one or more of the dose components when reporting on teacher training [51, 68, 69, 73, 75, 80, 84, 85]. Each component of the ‘dose’ of training is described in detail below.
The duration of the teacher training was reported in 24 of the 30 studies that reported teacher training [46, 47, 50, 54–62, 65, 66, 70, 71, 74–76, 78, 79, 82, 83, 85]. Of those, 16 studies reported a training duration of 1 day or greater [46, 47, 50, 55–57, 59, 61, 65, 66, 74–76, 78, 79, 83]. All but one of the 16 studies [55] showed significant intervention results. Seven studies reported teacher training of less than 1 day [54, 58, 60, 62, 71, 79, 82]. The shortest training duration was a 20-min briefing [58]. Two of the studies reported the training descriptively, rather than reporting actual training duration, i.e.: ‘comprehensive’ (85); ‘intense entrance workshop’ [70].
The mode of training (i.e., face-to-face, written resources, follow-up or ongoing support, additional resources) was reported in all but four of the 30 studies [51, 68, 84, 85]. Twenty-one reported using multi-modal methods of training delivery, whereas five studies provided only a single mode [50, 54, 60–62]. Of the studies that used multi-modal delivery of teacher training, 81 % [17/21] reported significant intervention outcomes. The most frequently used mode of teacher training was face-to-face (i.e., workshops or seminars), with only one study not using this method in their training [58]. The next most frequently used mode was written resources (e.g., electronic or print resource provision), with 19 of the 26 studies including this method [46, 55–59, 65, 66, 69–71, 73–76, 78, 79, 82, 83]. Nine of the 26 studies reported providing additional resources as part of their teacher training (e.g., activity tasks sheets, student workbooks, or activity bins) [55, 59, 66, 69, 71, 74, 76, 78, 83]. Ongoing or follow-up support (i.e., on-site visitations or consultation, or follow-up meetings) was reported by 12 of the studies [46, 47, 55, 57, 59, 65, 66, 75, 76, 79, 80, 83]. In addition, three of the studies provided ‘other’ support or incentives as part of their training delivery, which included financial support or the provision of relief teachers to allow teachers to attend training [46, 55, 82].
Only one of the 30 studies that reported teacher training did not report on the content (i.e., specific lesson content to be taught to students by teachers, and/or the recommended pedagogy to be used) of the teacher training program [85]. Ten of the 29 studies provided comprehensive information regarding teacher training content (i.e., both subject content and pedagogical content) [46, 47, 50, 55, 56, 70, 76, 78, 79, 83] (Table 4). Of those ten studies, 90 % reported significant intervention effects. Another nine of the 29 studies partially reported on content (i.e., either specific lesson content or pedagogy was omitted) [51, 54, 58, 68, 69, 71, 73, 80, 82], and ten studies only provided a brief statement of the training content (e.g., intervention objectives were conveyed to teachers via seminars) [57, 59–62, 65, 66, 74, 75, 84].
3.1.2 Model, Theory, or Framework of Teacher Training
Only seven of the 30 studies that reported teacher training reported integrating a model, theory or framework into the teacher training [50, 51, 55, 56, 59, 76, 85]. Of these studies, all but one [55] showed a statistically significant intervention effect. Four of these integrated the same behavioral theory as was used in the main intervention [50, 51, 76, 85]. Three other studies incorporated a collaborative and/or cooperative framework into their professional learning [55, 56, 59].
3.1.3 Teacher Trainee and Trainer Characteristics
Of the 30 studies that reported teacher training, two studies did not report the type of teacher that was trained [51, 84]. In 12 studies the trainee was reported to be a specialist PE teacher [54–56, 58, 60, 65, 68, 73, 79, 80, 83, 85]; nine of the 12 studies had significant intervention effects. In eight studies the trainee was a generalist classroom teacher [50, 62, 66, 69–71, 74, 78], with significant intervention effects displayed in all but one study [62]. In eight other studies the trainees were both generalist classroom teachers and PE teachers [46, 47, 57, 59, 61, 76, 82, 83]. One study reported the trainee as ‘the person in charge of the girls PE’ [75], not specifying whether that was a specialist or generalist teacher. Of the 28 studies that reported on the trainee, the characteristics of the trainee (i.e., trainee experience or qualifications) were only reported in eight [47, 56, 61, 68, 69, 71, 76, 79]. Six of the studies did not report who facilitated the training [51, 54, 61, 62, 69, 84]. Of the 24 studies that did, it was predominantly reported that the trainer was a member of the research team, or a specialist in PE. However, only six of the 24 studies presented information on trainer characteristics (i.e., trainer qualification and/or experience) [46, 55, 66, 69, 76, 79].
3.1.4 Teacher Satisfaction with Training
Only 11 of the 30 studies reported on trainee satisfaction of the training program. The trainees were specialist PE teachers in three of the studies [55, 68, 83], generalist classroom teachers in three [50, 69, 74], and in five of the studies the trainees were both specialists and generalist teachers [46, 47, 59, 76, 84]. Only one of these studies [55] did not report positive overall intervention results. Satisfaction was determined via semi-structured interviews and/or surveys, with all nine studies reporting positive responses to the training.
3.1.5 Teacher Fidelity to Training Program
Seven of the 30 studies did not report on the teachers’ fidelity in delivering the intervention [51, 54, 57, 60–62, 85]. Of the 22 studies reporting on fidelity, nearly all (20/22) reported overall positive intervention outcomes. Ten studies used direct observation to determine teacher fidelity [47, 50, 59, 73, 75, 76, 78, 79, 83, 84], five used self-reporting [58, 66, 69, 74, 82], and five used both direct observation and self-reporting measures [55, 56, 68, 71, 80]. Three of the studies reported using informal methods, such as verbal feedback on incidental observation or collaboration following lesson implementation to enhance compliance to the intervention [46, 65, 70].
3.2 Risk of Bias in Studies
Table 2 displays the risk of bias for all studies. Five of the 39 studies clearly described randomization [50, 57, 58, 80, 82]. Nineteen studies reported randomization, but were not clear about the process [46, 47, 53, 59–62, 65–67, 70, 73–76, 78, 79, 83, 84]. The remaining 16 studies were not randomized. Four of the 39 studies did not use a valid measure of FMS and/or PA [52, 63, 74, 77], and an additional two studies were unclear [64, 84]. Six studies reported a blinded outcome assessment [50, 57, 58, 76, 80, 83], and one study was unclear [82]. Six studies reported that participants were analyzed in their allocated groups [50, 56–59, 73], 13 of the studies were unclear [48, 49, 54, 60, 62–65, 67, 71, 78, 79, 85], and one did not provide any information [74]. Twenty-four of the studies accounted for covariates in their groups [46, 47, 49, 50, 54–59, 62, 63, 65, 66, 70–72, 75, 76, 78–80, 82, 83]. Seven studies reported a power calculation for FMS or PA outcomes [50, 55, 57–59, 61, 71]. Eleven studies presented baseline characteristics separately for treatment groups [46, 47, 50, 55, 57, 59, 61, 62, 65, 66, 71]. Drop-out was reported in 16 studies [46, 49, 50, 52, 56–59, 61, 62, 66, 71–73, 79, 83]. Summary results, effect size estimates and precision estimates were reported in 15 studies [49–51, 53, 57, 59, 62, 65, 66, 69, 71, 76, 78, 80, 82].
4 Discussion
The aim of this systematic review was to describe the characteristics of teacher training used in school-based interventions and identify which characteristics are common among studies that reported statistically significant, positive changes in PA and/or FMS. Specifically, this review investigated the dose of training received, the modality of training, the model or theory used in the teacher training, the characteristics of the trainer and trainee, trainee satisfaction with the training program, and the fidelity of the prescribed teaching practice in the intervention. In addition, the review aimed to identify whether there was a link between certain teacher training characteristics and FMS and/or PA improvement. Approximately one-quarter of the studies included in this review did not report on any aspect of the teacher training conducted, despite teachers facilitating the school-based FMS and/or PA intervention [48, 49, 52, 53, 63, 64, 67, 72, 77]. Therefore, for these studies it is not possible to determine the extent of the influence that teacher training had on intervention outcomes. This is an important finding, as it shows that future studies in this area should document teacher training characteristics to enable us to understand better the role of teachers in such interventions. Subsequently, it may have the potential to facilitate a clearer understanding of the specific teacher characteristics that improve the quality or effectiveness of teaching in PE [86].
Of the 30 studies that reported on teacher training in the intervention, 25 achieved statistically significant intervention results for FMS and/or PA. Although these figures appear promising, there was a high risk of bias in many of the studies. Indeed, most studies scored poorly for risk of bias items [87], particularly assessor blinding and randomization processes (Table 2). In addition, whilst the p value can inform the reader whether an effect exists, the p value will not reveal the size of the effect, or the meaningfulness or practical significance of the effect. Therefore, reporting effect sizes or similar is recommended [88]. Of the 30 studies that reported on teacher training, the actual changes reported in the intervention outcomes were variable. Furthermore, because there was considerable heterogeneity among interventions, in regards to the measuring, recording and reporting of PA intervention outcome effects (e.g., PA minutes per PE lesson, moderate-to-vigorous physical activity (MVPA) minutes per day, PA per episodes/blocks, logged PA) and FMS outcomes (i.e., multiple assessment instruments reporting on different aspects of FMS in different manners), it made the comparison of intervention effects difficult. However, in general, the changes in FMS outcomes were small to medium, and similar to that found in the review conducted by Morgan et al. [25], and the changes in PA outcomes were generally small, and reflect those commonly identified in other school based PA interventions [26]. Interestingly, the SCORES intervention [50], an intervention which included eight of the nine teacher training characteristics being investigated in this review (Table 4), reported an increase of 13 min of MVPA per day, which is just under a quarter of the daily MVPA recommendations [4–6], and also reported an improved overall FMS competency of 4.9 skill components. Furthermore, the Middle School Physical Activity and Nutrition (M-SPAN) study [76] reported a large effect size (d = 0.93) for PA in the total group, and again, eight of the nine teacher characteristics investigated in this review were reported. Although the changes in outcome of the other studies included in this review were generally conservative, the public health implications of these findings are important. As most young people participate in some form of regular school-based PE, it has a vital role to play in their development of FMS, and provision of PA. Indeed, PE is a critical medium for providing instruction and opportunity for practice, which is recognized as one of the most influential factors in FMS development [25]. Therefore, even small increases in MVPA and/or FMS during PE are positive. As such, it is essential that specialist PE teachers, and/or classroom teachers, are provided with extensive and ongoing professional development in the delivery of FMS and/or PA within PE, to enhance the effectiveness of these programs [25]. Furthermore, the FMS interventions appeared to have larger effects than the PA interventions, and nearly all FMS interventions had a significant effect, which suggests FMS PE based interventions maybe more successful than PA PE interventions.
Moreover, of the 30 studies that did report on teacher training, minimal information was provided on the details of the training. For example, only eight of the 30 studies addressed all three elements of ‘dose’ (i.e., duration, mode, content). As the detail of information provided by each study varied, it was difficult to ascertain which aspects of teacher training were most important in relation to a positive FMS/PA outcome. Furthermore, there were significant differences in design, mode, duration, content, framework, trainee and trainer characteristics, which made comparisons between studies difficult. This further illustrates that without future effective documentation of the role of teachers in interventions we are unable to understand the contribution of teacher training in intervention outcomes.
The findings of this review did manage to highlight several areas of inadequacies in the quality of teacher training for school-based PA and FMS interventions. While there is general agreement that no single approach to teacher training is effective for all teachers all of the time [40, 89], what is commonly acknowledged is that the quality of teacher training is critical to the desired outcome. If teachers receive well-designed, comprehensively integrated, and substantial training they can significantly increase student achievement [40, 90]. Conversely, if the professional development is brief, one-off, or fragmented, there is less likely to be a positive effect on student learning [91]. These inadequacies can be seen in both the design and delivery of the teacher training program, and also in the depth and consistency of the reporting of teacher training. Indeed, it is possible that the teacher training in these studies was inadequately reported, rather than inadequately conducted, and thus the actual quality of the teacher training may have been underestimated. This highlights the need for a consistent approach to teacher training design, delivery and reporting so we can better evaluate the intervention. The key concerns about the design and/or reporting of teacher training programs were: (1) the short durations; (2) lack of information on the provision of content, especially in regard to training the teacher in the pedagogy recommended in the intervention; (3) the lack of theory or framework included in the teacher training component; (4) lack of engagement between the teacher and interventionist, and the variable amount of follow-up or ongoing support provided throughout the intervention; and (5) the limited measure of teacher satisfaction. Each area of concern is expanded on below.
Over one-third of the studies that reported on the duration of teacher training reported less than one day of teacher training [54, 58, 60, 62, 71, 79, 82], with the shortest training being a 20-min briefing [58]. Ongoing teacher training is seen as a critical mechanism to facilitate teacher learning [36] and is viewed as central to improving education [88]. Professional development efforts that engage teachers for 1 day or more of learning have been shown to increase student achievement [92]. Indeed, in the current review 90 % of the studies reporting a teacher training duration of one day or more had positive intervention effects. Conversely, if teacher training is not ‘sustained’ (often defined as being less than 1 day of training duration [93]), training may be insufficient, and will be less likely to support teachers or facilitate long-term behavior change [36, 40, 41, 93]. Indeed, it has been demonstrated that the limited gains of MVPA in previous long-term studies could be partially attributed to inadequate investment in both personnel training programs and training time [55].
There was a considerable lack of information regarding the provision of content, especially in regard to training the teachers in the most effective or appropriate pedagogy to use when instructing the students in the intervention content. Indeed, less than one-third of studies provided comprehensive information on teacher training content (i.e., subject content and pedagogical content) [46, 47, 50, 55, 56, 70, 76, 78, 79, 83]. Of these few studies, nearly all reported positive intervention outcomes. Teachers are required to be highly qualified in the content area of the subject area in which they teach (i.e., high levels of content knowledge [CK]). However, expertise in content alone is inadequate. Effective teachers also possess a high level of pedagogical content knowledge (PCK), that being the skills and knowledge to successfully plan and implement a diversity of pedagogical approaches, which are dependent on individual student learning styles and developmental levels [94]. Importantly, the literature suggests that teachers who demonstrate high levels of both CK and PCK achieve better FMS outcomes for their students [95, 96]. Thereby, teacher training programs must not only present the lesson content, but, importantly, should also provide teachers with the skills, knowledge, and competence to successfully plan and implement and adapt the most effective teaching approaches to achieve the intervention outcomes [94, 97].
Under one-quarter of the studies presented here integrated a model, theory or framework in the teacher training [50, 51, 55, 56, 59, 76, 85]. It is well recognized that the use of established theory is important to the successful design and development of behavior-change curricula and intervention. Indeed, a recent systematic review [28] highlighted that utilizing a theoretical model may produce a sustained impact in PA, and should therefore be a priority in future PA research. However, specifics of how teacher training might incorporate theory in general, and motivational strategies in particular, were largely absent from the studies included in this review. Rink [98] suggests that all instructional methodologies are rooted in some form of learning theory and initiating any change process must involve some understanding of the theories that support it and subsequent assumptions about learning. Therefore, it is also essential to recognize the importance of incorporating theory into all aspects of project design, including teacher training.
Fewer than half of the studies provided ongoing or follow-up support (e.g., on-site visitations or consultation, or follow-up meetings) [46, 47, 55, 57, 59, 65, 66, 75, 76, 79, 80, 83]. This is consistent with a recent review of the sustained impact of PA and FMS interventions [28], which identified that many studies do not include post-intervention follow-up, support, training or consultation. Indeed, the absence of follow-up support may negatively influence the sustainability of a program in the school setting [28]. Teachers require approximately 130 h of engagement with a new intervention or concept, otherwise known as ‘active learning,’ to be able to transfer their learning to their own teaching context successfully [40]. Thus, maintaining face-to-face contact and providing teachers with opportunities to discuss implementation progress is essential in achieving intervention outcomes. Indeed, one of the most significant features of effective teacher training is the opportunity to reflect and collaborate [88, 93]. Furthermore, ongoing support can ensure the design and content of the program are constantly evolving to meet the specific needs of the teachers and school community, and thus can more successfully enable the ‘new’ approach to become embedded into usual teaching practice.
Few studies measured trainee satisfaction in the training program [46, 47, 50, 55, 59, 69, 74, 76, 83]. Of these studies, nearly all reported positive intervention results. To enhance teacher compliance with a program, teachers need to be satisfied with the content and context of the program [40]. Teachers engage more with program material when they perceive it to be practical and ‘hands on’, relevant and applicable [93, 99]. In contrast, if the teachers do not perceive the program to be challenging, thought-provoking, or providing ‘ideas’ and ‘practices’ they can use, they are less likely to value the program [93]. This highlights the importance of teacher collaboration in training program design, content and implementation. Specifically, to tailor programs to teachers and schools it is important to identify teachers’ needs before, and evaluate teacher satisfaction afterward, to determine how to improve or modify design iterations [92]. Furthermore, effectiveness of professional development should be measured not only at the level of teacher participation and satisfaction, but also at the level of the students with which the teachers interact [100]. For interventions to be truly effective, it is also important to consider the student voice, and to investigate the impact that advances in teacher learning have on student outcomes [100]. This enables the creation of teaching and learning processes, as well as outcomes, that are relevant and meaningful to both the teachers and the students [86].
It is clear that teachers play a central role in school-based PA/FMS intervention. However, their agency as effective facilitators will likely be determined, at least in part, by their perceptions, attitudes, and values of PA/FMS [32]. Although not investigated within the scope of this review, it is important to acknowledge the ‘value’ the teacher places on the teaching of PA and/or FMS within the scope of their role as a teacher, and understand that this will have an impact on the quality or effectiveness of their teaching [86, 100]. How teachers feel about playing a more active role in promoting PA or FMS arises from their personal experience as students, via pre service education, and importantly via ongoing professional development [32]. This emphasizes the important role that quality preservice training, in conjunction with ongoing professional development, can play in preparing teachers to be effective teachers and advocates of PA and FMS in the school setting.
The majority of studies included in the review presented statistically significant intervention results in FMS and/or PA, which may have been due to publication bias [101]. Only four studies [55, 62, 73, 82] did not achieve statistically significant intervention results. Interestingly, in three of these four studies [62, 73, 82] the pedagogy, theoretical model and/or teacher satisfaction were not included. Furthermore, training duration in all three was either less than one day [62, 82] or not reported [73]. In-service training enhances teacher confidence, which leads to more complete implementation and, in some cases, enhanced student outcomes [102]. Therefore, the omission of integral teacher training components in these three studies [62, 73, 82] may potentially have contributed to the null intervention results.
4.1 Strengths and Limitations
This review had several strengths, including a comprehensive search strategy across multiple databases with no date restrictions, extensive study detail extraction and broad inclusion criteria, high agreement levels for risk of bias, and alignment with PRISMA strategies. Limitations of the review included an English language requirement, and an inability to rule out publication bias.
5 Conclusions
It is clear from this review that both specialist PE teachers and highly trained classroom teachers are capable of making substantial improvements in student outcomes in PA and FMS. What remains unclear, largely due to poor reporting, is what role teacher training is having on these outcomes. Ongoing teacher training and support appears to be a key element of effective PE curriculums and successful interventions [40, 47, 103]. However, given the variability of reporting of teacher training characteristics provided by articles in the present review, links between teacher training and student outcomes were difficult to trace. Despite this limitation, the findings of this review suggest the teacher training component of school-based PA and/or FMS interventions is not only under-reported but often under-studied, and perhaps as a result, the value of teacher training is not widely understood. In addition, the findings point to a few key considerations when designing teacher training programs in school-based PE interventions, specifically: (1) a ‘sustained’ teacher training component (i.e., one day or more); (2) a multimodal approach to teacher training delivery, with a focus on ongoing consultation; (3) comprehensive intervention content including pedagogy that translates the content into practice; and (4) viewing the measurement of teacher satisfaction and fidelity as essential design elements. Papers should clearly report on teacher training characteristics to better inform the design of future effective school-based interventions.
References
Yang X, Telama R, Leskinen E, et al. Testing a model of physical activity and obesity tracking from youth to adulthood: the cardiovascular risk in young Finns study. Int J Obes. 2007;31:521–7.
Janssen L, LeBlanc A. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7:40.
Eisenmann JC, Wickel EE, Welk GJ, et al. Relationship between adolescent fitness and fatness and cardiovascular disease risk factors in adulthood: the Aerobics Centre Longitudinal Study (ACLS). Am Heart J. 2005;149:46–53.
Camacho-Miñano MJ, LaVoi NM, Barr-Anderson DJ. Interventions to promote physical activity among young and adolescent girls: a systematic review. Health Educ Res. 2011;26(6):1025–49.
Australian Bureau of Statistics. 2011–2013 Australian Health Survey: physical activity. 2013. http://www.abs.gov.au/australianhealthsurvey.
Hallal PC, Andersen LB, Bull FC, et al. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247–57.
Nader P, Bradley R, Houts R, et al. Moderate-to-vigorous physical activity from ages 9 to 15 years. JAMA. 2008;300(3):295–395.
Sallis J, Prochaska J, Taylor W. A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 2000;32(5):963–75.
Currie C, Zanotti C, Morgan A, et al. Social determinants of health and well-being among young people. Health behaviour in school-aged children (HBSC) study: international report from the 2009/2010 survey. Copenhagen: WHO Regional Office for Europe; 2012.
Bauman AE, Reis RS, Sallis JF, et al. Correlates of physical activity: why are some people physically active and others not? Lancet. 2012;380(9838):258–71.
Lubans DR, Morgan P, Cliff DP, et al. Fundamental movement skills in children and adolescents: review of associated health benefits. Sports Med. 2010;40(12):1019–35.
Ulrich D. Test of gross motor development. 2nd ed. Austin: Pro-Ed; 2000.
Gallahue DL, Ozmun JC, Goodway JD. Understanding motor development: infants, children, adolescents, adults. 7th ed. New York: McGraw-Hill; 2006. p. 2011.
Barnett LM, van Beurden E, Morgan PJ, et al. Childhood motor skill proficiency as a predictor of adolescent physical activity. J Adolesc Health. 2009;44:252–9.
Booth ML, Okley AD, Denney-Wilson E, et al. NSW Schools Physical Activity and Nutrition Survey (SPANS) 2010: full report. Sydney: NSW Department of Health; 2006.
Hardy LL, Barnett LM, Espinel P, et al. Thirteen-year trends in child and adolescent fundamental movement skills: 1997–2010. Med Sci Sports Exerc. 2013;45(10):1965–70.
Hardy LL, King L, Epinel P, et al. NSW Schools Physical Activity and Nutrition Survey (SPANS) 2010: full report. Sydney: NSW Department of Health; 2011.
Pill S, Priest T. South Australian Catholic primary schools sport association fundamental movement skills pilot project. ACHPER International Conference: Creating Active Futures. Brisbane: ACHPER; 2009. p. 257–69.
Robinson LE, Stodden DF, Barnett LM, et al. Motor competence and its effect on positive developmental trajectories of health. Open Access Sports Med (Auckland, NZ). 2015;45(9):1273–84.
International Union for Health Promotion and Education (IUHPE). Achieving health promoting schools: guidelines for promoting health in schools. United States Centers for Disease Control and Prevention (CDC). USA: SAGE Publishing; 2009.
Carter R. The impact of public schools on childhood obesity. JAMA. 2002;288(17):2180. doi:10.1001/jama.288.17.2180-JMS1106-6-1.
Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. http://www.cdc.gov/2014. Cited 14 April 2014.
School health guidelines to promote healthy eating and physical activity. MMWR Recomm Rep. 2011;60(Rr-5):1–76.
Russ L, Webster C, Beets M, et al. Systematic review and meta-analysis of multi-component interventions through schools to increase physical activity. J Phys Act Health. (In press).
Morgan PJ, Barnett LM, Cliff DP, et al. Fundamental movement skill interventions in youth: a systematic review and meta-analysis. Pediatrics. 2013;132(5):e1361–83.
Dudley D, Okely A, Pearson P, et al. A systematic review of the effectiveness of physical education and school sport interventions targeting physical activity, movement skills and enjoyment of physical activity. Eur Phys Educ Rev. 2011;17(3):53–78.
Dobbins M, Husson H, DeCorby K, et al. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst Rev. 2013;2:Cd007651.
Lai SK, Costigan SA, Morgan PJ, et al. Do school-based interventions focusing on physical activity, fitness, or fundamental movement skill competency produce a sustained impact in these outcomes in children and adolescents? A systematic review of follow-up studies. Sports Med. 2014;44(1):67–79.
Dusenbury L, Brannigan R, Falco M, et al. A review of research on fidelity of implementation: implications for drug abuse prevention in school settings. Health Educ Res. 2003;18(2):237–56.
Hattie J. Visible learning: a synthesis of over 800 meta-analyses relating to achievement. London: Routledge; 2013.
Sharma M. International school-based interventions for preventing obesity in children. Obes Rev. 2007;8(2):155–67.
Webster CA. Relationships between personal biography and changes in preservice classroom teachers’ physical activity promotion competence and attitude. J Teach Phys Educ. 2011;30(4):320–39.
Xiang P, Lowy S, McBride R. The impact of a field-based elementary physical education methods course on preservice classroom teachers’ beliefs. J Teach Phys Educ. 2002;21(2):145–61.
Hart MA. Influence of a physical education methods course on elementary education majors’ knowledge of fundamental movement skills. Phys Educat. 2005;62(4):198–204.
Murphy F, O’Leary M. Supporting primary teachers to teach children physical: continuing the journey. Irish Educ Stud. 2010;31(3):297–310.
Bechtel PA, O’Sullivan M. Effective professional development—what we now know. J Teach Phys Educ. 2006;25:368–78.
Hart J, Lee O. Teacher professional development to improve science and literacy achievement of English language learners. Biling Res J. 2003;27(3):475–501.
Huffman D, Thomas K, Lawrenz F. Relationship between professional development, teachers’ instructional practices, and the achievement of students in science and mathematics. Sch Sci Math. 2003;103(8):378–87.
Supovitz JA, Turner HM. The effects of professional development on science teaching practices and classroom culture. J Sci Teacher Ed. 2000;37(9):963–80.
Armour KM, Yelling M. Effective professional development for physical education teachers: The role of informal, collaborative learning. J Teach Phys Educ. 2007;26(2):177.
Bechtel PA, O’Sullivan M. Enhancers and inhibitors of teacher change among secondary physical educators. J Teach Phys Educ. 2007;26(3):221–35.
Morgan PJ, Hansen V. Classroom teacher’s perceptions of the impact of barriers to teaching physical education on the quality of physical education programs. Res Q Exerc Sport. 2008;4(79):506–16.
Kealey KA, Peterson AV Jr, Gaul MA, et al. Teacher training as a behavior change process: principles and results from a longitudinal study. Health Educ Behav. 2000;27(1):64–81.
Garet MS, Porter AC, Desimone L, et al. What makes professional development effective? Results from a national sample of teachers. Am Educ Res J. 2001;38(4):915–45.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
McKenzie TJ, Alcaraaz E, Sallis F. Effects on physical education program on children’s manipulative skills. J Teach Phys Educ. 1998;17:327–41.
Sallis JF, McKenzie JF, Alcarazaz JE, et al. The effects of a 2-year physical education program (SPARK) on physical activity and fitness in elementary school students. Am J Public Health. 1997;87:1328–33.
Bakhtiari S, Shafina P, Ziaee V. Effects of selected exercises on elementary school third grade girls students’ motor development. Asian J Sports Med. 2011;2:51–6.
Boyle-Holmes T, Grost L, Russell L, et al. Promoting elementary physical education: results of a school based evaluation study. Health Educ Behav. 2010;37:377–89.
Cohen KE, Morgan PJ, Plontikoff R, et al. Physical activity and skills intervention: SCORES cluster randomized controlled trial. Med Sci Sports Exerc. 2015;47(4):765–74.
Ericsson I. Effects of increased physical activity on motor skills and marks in physical education: an intervention study in school years 1 through 9 in Sweden. Phys Ed Sport Pedagogy. 2011;16(3):313–29.
Fogel VA, Miltenberger RG, Graves R, et al. The effects of exergaming on physical activity among inactive children in a physical education classroom. J Appl Behav Anal. 2010;43(4):591–600.
Gao Z, Lee AM, Xiang P, et al. Effect of learning activity on students’ motivation, physical activity levels and effort/persistence. ICHPER SD. 2011;6(1):27–33.
How YM, Whipp P, Dimmock J, et al. The effects of choice on autonomous motivation, perceived autonomy support, and physical activity levels in high school physical education. J Teach Phys Educ. 2013;32(2):131–48.
Jago R, McMurray RG, Drews KL, et al. HEALTHY intervention: fitness, physical activity, and metabolic syndrome results. Med Sci Sports Exerc. 2011;43(8):1513–22.
Kalaja SP, Jaakkola TT, Liukkonen JO, et al. Development of junior high school students’ fundamental movement skills and physical activity in a naturalistic physical education setting. Phys Ed Sport Pedagogy. 2012;17(4):411–28.
Kriemler S, Zahner L, Schindler C, et al. Effect of school based physical activity programme (KISS) on fitness and adiposity in primary schoolchildren: cluster randomised controlled trial. BMJ. 2010;340:c785.
Lonsdale C, Rosenkranz RR, Lubans DR, et al. A cluster-randomized controlled trial of strategies to increase adolescents’ physical activity and motivation during physical education lessons: the Motivating Active Learning in Physical Education (MALP) trial. BMC Public Health. 2012;12:834.
Magnusson KT, Sigurgeirsson I, Sveinsson T, et al. Assessment of a two-year school-based physical activity intervention among 7-9-year-old children. Int J Behav Nutr Phys Act. 2011;8:138.
Michaud V, Nadeau L, Martel D, et al. The effect of team pentathlon on ten- to eleven-year-old childrens’ engagement in physical activity. Phys Educ Sport Pedagogy. 2012;17(5):543–62.
Sacchetti R, Ceciliani A, Garulli A, et al. Effects of a 2-year school-based intervention of enhanced physical education in the primary school. J Sch Health. 2013;83(9):639–46.
Siegrist M, Hanssen H, Lammel C, et al. A cluster randomised school-based lifestyle intervention programme for the prevention of childhood obesity and related early cardiovascular disease (JuvenTUM 3). BMC Public Health. 2011;11:258.
Zrnzević N, Lilić L, Zrnzević J. Contribution of the experimental physical education curricula to the functional abilities development. Res Kinesiol. 2013;41(1):101–5.
Dobraš R, Dragosavljević P, Vučković I, et al. The impact of the motivational intervention on students’ motor abilities. Physical Culture/Fizicka Kultura. 2013;67(1):24–32.
Neumark-Sztainer DR, Friend SE, Flattum CF, et al. New moves-preventing weight-related problems in adolescent girls a group-randomized study. Am J Prev Med. 2010;39(5):421–32.
Ahamed Y, MacDonald H, Reed K. School-based physical activity does not compromise children’s academic performance. Med Sci Sports Exerc. 2007;39(2):371–6.
Akbari H, Abdoli B, Shafizadehkenari M, et al. The effect of traditional games in fundamental motor skill development in 7–9 year old boys. Iran J Pediatr. 2009;19(2):123–9.
Fairclough SJ, Stratton G. Effects of a physical education intervention to improve student activity levels. Phys Educ Sport Pedagogy. 2006;11(1):29–44.
Gorely T, Nevill ME, Morris JG, et al. Effect of a school-based intervention to promote healthy lifestyles in 7–11 year old children. Int J Behav Nutr Phys Act. 2009;6:5.
Graf C, Koch B, Falkowski G, et al. Effects of a school based intervention on BMI and motor abilities in childhood. J Sports Sci Med. 2005;15:361–87.
Harrison M, Burns C, McGuinness M, et al. Influence of a health education intervention on physical activity and screen time in primary school children: ‘Switch Off-Get Active’. J Sci Med Sport. 2006;9(5):388–94.
Jamner MS, Spruijt-Metz D, Bassin S, et al. A controlled evaluation of a school-based intervention to promote physical activity among sedentary adolescent females: project FAB. J Adolesc Health. 2004;34(4):279–89.
Maskell B, Shapiro DR, Ridley C. Effects of brain gym on overhand throwing in first grade students: a preliminary investigation. Phys Educat. 2004;61(1):14–22.
Naylor P, Macdonald H, Zebedee J, et al. Lessons learned from Action Schools! BC—an ‘active school’ model to promote physical activity in elementary schools. J Sci Med Sport. 2006;9(5):413–23.
Pate RR, Ward DS, Saunders RP, et al. Promotion of physical activity among high-school girls: a randomized controlled trial. Am J Public Health. 2005;95(9):1582.
Sallis JF, McKenzie TL, Conway TL, et al. Environmental interventions for eating and physical activity: a randomized controlled trial in middle schools. Am J Prev Med. 2003;24(3):209–17.
Sollerhed AC, Ejlertsson G. Physical benefits of expanded physical education in primary school: findings from a 3-year intervention study in Sweden. Scand J Med Sci Sports. 2008;18(1):102–7.
van Beurden E, Barnett LM, Zask A, et al. Can we skill and activate children through primary school physical education lessons? “Move it Groove it”-a collaborative health promotion intervention. Prev Med. 2003;36(4):493–501.
Verstraete S, Cardon G, De Clercq D, et al. Effectiveness of a two-year health-related physical education intervention in elementary schools. J Teach Phys Educ. 2007;26(1):20–34.
Webber LS, Catellier DJ, Lytle LA, et al. Promoting physical activity in middle school girls: trial of activity for adolescent girls. Am J Prev Med. 2008;34(3):173–84.
Martin EH, Rudisill ME, Hastie PA. Motivational climate and fundamental motor skill performance in a naturalistic physical education setting. Phys Educ Sport Pedagogy. 2009;14(3):227–40.
Gortmaker SL, Peterson K, Wiecha J, et al. Reducing obesity via a school-based interdisciplinary intervention among youth: planet health. Arch Pediatr Adolesc Med. 1999;153(4):409–18.
Luepker RV, Perry CL, McKinlay SM, et al. Outcomes of a field trial to improve children’s dietary patterns and physical activity. The Child and Adolescent Trial for Cardiovascular Health. CATCH collaborative group. JAMA. 1996;275(10):768–76.
Pieron M, Cloes M, Delfosse C, et al. An investigation of the effects of daily physical education in kindergarten and elementary schools. Eur Phys Educ Rev. 1996;2(2):116–32.
Simons-Morton BG, Parcel GS, Baranowski T, et al. Promoting physical activity and a healthful diet among children: results of a school-based intervention study. Am J Public Health. 1991;81(8):986–91.
Dyson B. Quality physical education: A commentary of effective physical education teaching. Res Q Exerc Sport. 2014;85(2):144–52.
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151(4):W-65.
Sullivan G, Feinn R. Using effect size-or why the p value is not enough. J Grad Med Educ. 2012;4(3):279–82.
Guskey TR. Professional development and teacher change. Teach Teach. 2002;8(3):381–91.
Yoon KS, Duncan T, Lee SW-Y, et al. Reviewing the evidence on how teacher professional development affects student achievement. Washington, DC: Department of Education, Institute of Education Sciences, National Center for Education Evaluation and Regional Assistance, Regional Educational Laboratory Southwest; 2007.
Wei RC, Darling-Hammond L, Andree A, et al. Professional learning in the learning profession: a status report on teacher development in the United States and abroad. TX: Dallas; 2009.
Darling-Hammond L, Jaquith A, Hamilton M. Creating a comprehensive system for evaluating and supporting effective teaching, vol. 26. Stanford, California: Stanford Center for Opportunity Policy in Education (SCOPE); 2012.
Armour KM, Yelling MR. Continuing professional development for experienced physical education teachers: towards effective provision. Sport Educ Soc. 2004;9(1):95–114.
Lieberman LJ, Houston-Wilson C. Strategies for inclusion; a handbook for physical educators. Champaign: Human Kinetics; 2009.
Cohen R, Goodway JD, Lidor R. The effectiveness of aligned developmental feedback on the overhand throw in third-grade students. Phys Educ Sport Pedagog. 2012;17(5):525–41.
Hashweh MZ. Teacher pedagogical constructions: a reconfiguration of pedagogiacl content knowledge. Teach Teach. 2006;11(3):273–92.
Blank RK, de las Alas N. Effects of teacher professional development on gains in student achievement: how meta analysis provides scientific evidence useful to education leaders. Washington, DC: 2009.
Rink JE. Investigating the assumptions of pedagogy. J Teach Phys Educ. 2001;20(2):112–128.
Borko H. Professional development and teacher learning: mapping the terrain. Educ Res. 2004;33(8):3–15.
Wade RK. What makes a difference in inservice teacher education? A meta analysis of research. Educ Leadersh. 1985;42(4):48–54.
Dwan K, Altman DG, Arnaiz JA, et al. Systematic review of the empirical evidence of study publication bias and outcome reporting bias. PLoS One. 2008;3(8):e3081.
Ross JG, Luepker RV, Nelson GD, et al. Teenage health teaching modules: impact of teacher training on implementation and student outcomes. J Sch Health. 1991;61(1):31–4.
McKenzie TL, Dart JA, Sallis JF, et al. Evaluation of a widely disseminated physical education and professional development program by inservice teachers. (Abstract). Res Q Exerc Sport. 2003;74(1 Suppl):A-50-a-1.
Lubans DR, Morgan PJ, Weaver K, et al. Rationale and study protocol for the supporting children’s outcomes using rewards, exercise and skills (SCORES) group randomized controlled trial: a physical activity and fundamental movement skills intervention for primary schools in low-income communities. BMC Public Health. 2012;12(1):1.
Graf C, Koch B, Falkowski G, et al. School-based prevention: effects on obesity and physical performance after 4 years. J Sports Sci. 2008;26(10):987–94.
McMurray RG, Bassin S, Jago R, et al. Rationale, design and methods of the HEALTHY study physical education intervention component. Int J Obes. 2005;2009(33 Suppl 4):S37–43.
Schneider M, Hall WJ, Hernandez AE, et al. Rationale, design and methods for process evaluation in the HEALTHY study. Int J Obes. 2009;33(Suppl 4):S60–7.
Naylor PJ, Scott J, Drummond J, et al. Implementing a whole school physical activity and healthy eating model in rural and remote first nations schools: a process evaluation of action schools BC. Rural Remote Health. 2010;10:1296.
McKenzie TL, Nader PR, Strikmiller PK, et al. School physical education: effect of the child and adolescent trial for cardiovascular health. Prev Med. 1996;25(4):423–31.
Ward DS, Saunders R, Felton GM, et al. Implementation of a school environment intervention to increase physical activity in high school girls. Health Educ Res. 2006;21(6):896–910.
McKenzie TL, Prochaska JJ, Sallis JF, et al. Coeducational and single-sex physical education in middle schools: Impact on physical activity. Res Q Exerc Sport. 2004;75(4):446–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Lisa Barnett is supported by an Alfred Deakin Fellowship. Jo Salmon is supported by a National Health and Medical Research Council Principal Research Fellowship (APP1026216). No sources of funding were used to assist in the preparation of this review.
Conflict of interest
Natalie Lander, Narelle Eather, Phillip Morgan, Jo Salmon, and Lisa Barnett declare that they have no conflicts of interest that are relevant to the content of this review.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lander, N., Eather, N., Morgan, P.J. et al. Characteristics of Teacher Training in School-Based Physical Education Interventions to Improve Fundamental Movement Skills and/or Physical Activity: A Systematic Review. Sports Med 47, 135–161 (2017). https://doi.org/10.1007/s40279-016-0561-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-016-0561-6