
Abstract
Background
An understanding of the humanistic and economic burden of individuals with symptomatic chronic obstructive pulmonary disease (COPD) is required to inform payers and healthcare professionals about the disease burden.
Objectives
The aim of this systematic review was to identify and present humanistic [health-related quality of life (HRQoL)] and economic burdens of symptomatic COPD.
Methods
A comprehensive search of online databases (reimbursement or claims databases/other databases), abstracts from conference proceedings, published literature, clinical trials, medical records, health ministries, financial reports, registries, and other sources was conducted. Adult patients of any race or gender with symptomatic COPD were included. Humanistic and economic burdens included studies evaluating HRQoL and cost and resource use, respectively, associated with symptomatic COPD.
Results
Thirty-two studies reporting humanistic burden and 74 economic studies were identified. Symptomatic COPD led to impairment in the health state of patients, as assessed by HRQoL instruments. It was also associated with high economic burden across all countries. The overall, direct, and indirect costs per patient increased with an increase in symptoms, dyspnoea severity, and duration of disease. Across countries, the annual societal costs associated with symptomatic COPD were higher among patients with comorbidities.
Conclusions
Symptomatic COPD is associated with a substantial economic burden. The HRQoL of patients with symptomatic COPD is, in general, low and influenced by dyspnoea.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Symptomatic chronic obstructive pulmonary disease (COPD) leads to impairment in the health state of patients. |
Symptomatic COPD was associated with high economic burden across all countries. It influenced both direct and indirect costs associated with symptoms, dyspnoea severity, and duration of disease. |
The health-related quality of life of patients with symptomatic COPD is, in general, low and influenced by multifactorial causality. |
1 Introduction
Chronic obstructive pulmonary disease (COPD) is characterised by varying degrees of airflow obstruction that reflect the severity of symptoms such as breathlessness, chronic cough, and wheeze [1]. It is the leading cause of morbidity and mortality across all countries with varying financial status [2] and thus imposes a challenging problem to the healthcare system [3]. Although the Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends routine use of the modified Medical Research Council (mMRC) and COPD Assessment Test (CAT) to assess and treat COPD symptoms, symptomatic COPD has not been defined adequately in the published literature [1]. Increases in the number and severity of general symptoms and in the disease severity of COPD are associated with a humanistic and economic burden [4–10]. Furthermore, various comorbid conditions such as cardiac disorders, diabetes, obesity, osteoporosis, lung cancer, pneumonia, and psychological disorders may further impact the disease process [11–13]. Taken together, COPD has a high-level impact on health-related quality of life (HRQoL) and healthcare resource utilisation [14].
Patients with COPD usually suffer from a marked deterioration in HRQoL [15]. This impact on HRQoL can be measured in terms of general health status, mental health, functional status, fatigue, and quality of sleep [16, 17]. The findings of these HRQoL instruments, which provide non-invasive patient-centered monitoring, reflect the humanistic burden of COPD [14]. Similarly, there exists a strong correlation between disease severity and economic burden [18]. The main focus of COPD treatment has been on the reduction and prevention of exacerbations [19], which are costly to treat and exert a negative impact on the HRQoL of the affected individuals [20]. Thus, patients with no or very few exacerbations also incur significant costs through repeated general practitioner (GP) visits and associated healthcare contact for their symptoms, in addition to a compromised HRQoL, indicating that symptomatic COPD is associated with high economic and humanistic burdens [10].
The objective of this systematic review was to identify and evaluate humanistic (HRQoL) and economic burdens among symptomatic patients with COPD.
2 Methods
2.1 Study Design
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [21]. It evaluated published evidence of humanistic burden of symptomatic COPD, as measured by HRQoL indices. The economic burden was assessed from cost-of-illness and resource use studies in patients with symptomatic COPD.
2.2 Information Sources
A comprehensive search of Excerpta Medica Database (EMBASE®), Medical Literature Analysis and Retrieval System Online (MEDLINE®), MEDLINE® In-Process, Cochrane Central Trials Register, Cochrane National Health Service Economic Evaluation Database (NHS EED), EconLit® , and Literatura Latino Americana em Ciências da Saúde (LILACS®) was performed from 2003 to 31 May 2013. In addition to database searching, abstracts from conference proceedings from the American Thoracic Society (ATS), American College of Chest Physicians (ACCP), European Respiratory Society (ERS), and International Society for Pharmacoeconomics and Outcomes Research (ISPOR) were hand searched from 2010 to 2013. A comprehensive search strategy was designed to retrieve relevant clinical data from published literature. An example of the search strategy is presented in detail in electronic supplementary Table S1.
The searches were restricted to include studies published in the English language, with the exception of LILACS®, which was not restricted to English articles. Relevant data from all included studies were extracted by a single reviewer, using a pre-defined extraction grid, which was subsequently validated by an independent reviewer. Thereafter, studies meeting the eligibility criteria were critically appraised using the Downs and Black checklist [22] for the humanistic burden, and the Drummond and Jefferson checklist for the economic burden [23].
2.3 Eligibility Criteria
The patient population of interest comprised adults of any race or gender with symptomatic COPD. Considerable variability in the definition of symptomatic COPD suggests that it is poorly defined in the clinical literature [1]. Therefore, in line with the GOLD guidelines, patients with one or more symptoms such as cough, breathlessness, sputum production, wheeze, and chest tightness were considered symptomatic [24]. Based on these recommendations, symptoms were also considered for evaluation in situations where they were based on physicians’ discretion only. Furthermore, the burden of symptomatic COPD patients in early stages might be higher than for non-symptomatic patients in slightly advanced disease, making quantification of this disease burden even more challenging. The GOLD guidelines have defined dyspnoea as a sense of increased effort to breathe, heaviness, air hunger, or gasping. In addition to the above mentioned criteria, the GOLD guidelines have recommended the mMRC scale and CAT for assessing COPD symptoms. An mMRC score ≥2 (breathlessness) and a CAT score ≥10 (high level of symptoms) represents patients with high symptoms [1]. Thus, patients with an mMRC score ≥2 and a CAT score ≥10 were also included in the review.
The humanistic burden was restricted to include cohort/longitudinal, case–control, cross–sectional, single-arm, and utility studies along with analyses of hospital records/databases and surveys. The outcomes of interest were patient-reported outcomes/HRQoL measures. Randomized controlled trials (RCTs) were excluded as they primarily focus on the assessment of efficacy and safety on a highly selective patient population rather than burden observed in clinical practice. Studies evaluating the impact of pharmacological or non-pharmacological interventions on improvement/deterioration of HRQoL were also excluded.
The economic burden was restricted to include cost studies/surveys/analysis and resource use studies in adult patients with symptomatic COPD, irrespective of the type of treatment investigated. As economic models present data for costs or cost effectiveness related to specific interventions under investigation, economic evaluations from modeling studies were excluded. The outcomes of interest were cost (direct, indirect, or total) and resource use associated with symptomatic COPD care.
2.4 Humanistic Assessments
The humanistic burden of illness (e.g. COPD) is characterised by the impact of illness on health and consequences of treatment, including impact on HRQoL or the relationship between various HRQoL scales and symptomatic COPD, loss of productivity and absenteeism, and frequency of clinical events (i.e. exacerbations, severity of symptoms). The complete list of HRQoL scales included in this review is available in electronic supplementary Table S2. Moreover, the relationship between patients’ demographic and comorbid characteristics (age, gender, body mass index [BMI], smoking status, comorbid conditions, etc.) and their humanistic burden was also evaluated.
2.5 Cost Assessments
The economic burden was characterised by the estimation of cost-of-illness (direct, indirect, and total) required for treating the COPD cohort of interest. These included costs associated with symptoms (severity and frequency) and dyspnoea care (based on the MRC dyspnoea scale score), and costs related to comorbidity.
3 Results
3.1 Study Characteristics
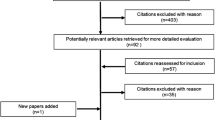
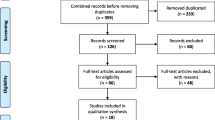
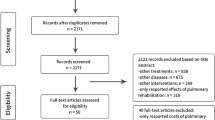
A total of 32 studies reporting humanistic burden and 74 economic studies specifically reporting cost and resource use involving patients with symptomatic COPD were included. Six studies reported both humanistic and economic impact of COPD. Figure 1 shows the study selection process, in line with PRISMA guidelines. The characteristics of patients and studies included in the humanistic burden review are presented in Table 1. The impact of varying levels of symptoms on the humanistic burden in patients with symptomatic COPD is presented in electronic supplementary Table S3.

Study selection process, in line with the PRISMA guidelines. PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses, NOI Not of Interest, SGA Subgroup Analysis
3.2 Humanistic Burden
3.2.1 Impact of Demographic Factors on Humanistic Burden of Symptomatic Chronic Obstructive Pulmonary Disease
Mollaoglu and colleagues observed that with advancing age (age groups 65–69, 70–74, and ≥75 years), elderly patients with symptomatic COPD demonstrated a trend towards increasing fatigue, disability, and overall decrease in energy (p > 0.05). Moreover, females were associated with higher fatigue and low energy levels compared with males, which was attributed to traditional female responsibilities within a family; however, the association was not statistically significant. Married patients had significantly increased fatigue compared with their single counterparts (p = 0.02). Furthermore, lower education level and employment (housewives and full-time employees) were associated with lower overall HRQoL (p > 0.05) [25].
3.2.2 Impact of Respiratory Symptoms and Dyspnoea
An increase in the severity of respiratory symptoms was associated with a corresponding decline in the HRQoL of patients [4, 5, 25–28].
Antoniu and colleagues evaluated HRQoL by categorising patients on the basis of symptom levels (mild, moderate, and severe). Patients experiencing severe sputum and cough had significantly higher fatigue and disability levels and significantly lower energy levels compared with patients with mild symptoms [28]. In contrast, a study by Al Moamary and colleagues revealed no significant differences in HRQoL in patients experiencing cough and wheezing evaluated using CAT and Chronic Respiratory Questionnaire–Self-Administered Standardized (CRQ-SAS) scores [4].
Based on the AQ20 score, patients reporting frequent cough, breathlessness during domestic work, and chest problems experienced limitation in full enjoyment of their life, whereas patients who did not present any respiratory symptoms scored the best possible result (score 0) [29]. Another study by Bellas and colleagues evaluated the relationship between cough and HRQoL in patients with COPD by using the CAT and the Leicester Cough Questionnaire (LCQ) as a cough-specific HRQoL measure. It was observed that increasing cough severity was associated with greater impairments in HRQoL [5].
This was also reflected in a significantly high mean of poor self-rated sleep quality [Pittsburgh Sleep Quality Index (PSQI)] in patients with a higher frequency of nocturnal wheezing, worrying, and uncontrolled thoughts. Other specific respiratory symptoms, not significant but associated with poor sleep quality, included cough, dyspnoea, chest pain, heartburn, and palpitations [30].
The association of dyspnoea with humanistic burden of symptomatic COPD was assessed in six studies. An increase in MRC scores from 0 to 4 was associated with worsening of HRQoL [4, 25, 27, 31–33]. Punekar and colleagues demonstrated a greater impairment in HRQoL with higher levels of dyspnoea, such that EuroQol (EQ-5D) utilities ranged from 0.88 to 0.17 in the primary care physician (PCP) cohort and 0.88 to 0.29 in the respiratory specialist cohort, with MRC score increasing from 0 to 4 [33]. Furthermore, among elderly patients, an increase in the severity of dyspnoea from mild to severe was associated with an increase in fatigue and disability and decrease in energy levels [25]. In a cross-sectional survey by Al Moamary and colleagues, patients with shortness of breath had significantly lower HRQoL compared with patients with no symptoms of shortness of breath on using the CAT score in contrast to the CRQ-SAS score, where association was negative but statistically non-significant [4]. Furthermore, using Short Form-12 (SF-12), the questionnaire-based ‘symptom of grade 2 dyspnoea’ reported the lowest mean Physical Component Summary (PCS), whereas dyspnoea attacks had the lowest mean Mental Component Summary (MCS). Both scores decreased significantly with increasing number of symptoms; however, this was more evident for physical than mental scores. The larger impact of dyspnoea on these scores could be attributed to other disease conditions such as heart disease [27].
3.2.3 Impact of Time to Occurrence of Symptoms
Patients with symptomatic COPD experiencing daytime as well as night-time symptoms had lower HRQoL compared with patients with either or none of the symptoms [33, 34]. Multivariate analysis demonstrated significant impact of both symptoms on HRQoL after controlling for age, comorbidities, country, and treatment setting measured using the EQ-5D [33]. Sullivan and colleagues showed that compared with patients without symptoms, those with both or either (night-time/early morning) symptoms reported worse HRQoL and dyspnoea, as indicated by significantly lower SF-12 PCS and MCS mean scores (p < 0.01), as well as higher CAT and mMRC mean scores (p < 0.01) [34].
3.2.4 Impact of Comorbidities
Life-event stress is associated with depressive symptoms and worse HRQoL in elderly individuals with COPD. It was observed that life-event stress was associated with more depressive symptoms and worse QoL in individuals with symptomatic COPD [35]. Carvounis and colleagues also showed that the mean Geriatric Depression Scale (GDS) score for patients >65 years was low (7.8 ± 0.9), indicating mild depression. These patients also presented with a higher risk of exacerbations [36].
3.3 Economic Burden
Results from the published studies reporting cost and healthcare resource use were variable and could be attributed to a number of influencing parameters (country, patient characteristics, disease severity, and the cost/resource item). Characteristics of patients and studies included in the economic review are presented in Table 2. The economic burden of symptomatic COPD is presented in electronic supplementary Tables S4 and S5.
3.3.1 Resource Use and Direct Costs
Two global surveys provided comprehensive evidence on the economic burden of COPD across countries. Symptomatic COPD was associated with high economic burden across all countries studied in these two surveys [37, 38]. The Confronting COPD survey was a large-scale international survey conducted across eight countries in Europe and North America (between August 2000 and January 2001). The annual direct costs of COPD for the year 2002 ranged from US$522 in France to US$4119 in the US. The composition of direct costs differed between countries, with more than 50 % of direct costs resulting from inpatient admissions in Canada, Italy, Spain, the UK, and the US, and almost 50 % due to regularly prescribed medicines in The Netherlands [38]. In the US, the mean direct annual per patient costs of PCP visits, specialist visits, and emergency room (ER) visits for the year 2002 were US$225.19, US$150.20, and US$289.10, respectively (data evaluated between August 2000 and January 2001). Patients in the US also reported the maximum specialist visits, with a mean of 1.8 visits per patient in the past year [39]. The costs were lowest in France, with oxygen therapy accounting for 25 % of the total direct costs [38, 39].
Another large survey (the BREATHE study, conducted between June 2010 and December 2011) was conducted in 2012 in 11 countries of the Middle East and North Africa. Physician consultations were the most frequently utilised resource, followed by ER visits and hospitalisations. Resource use was significantly higher in subjects with more symptoms (CAT score ≥10) compared with those with fewer symptoms (p < 0.0001) [37]. Murtagh and colleagues reported that using a random sample of the Northern Ireland population (for the year 2000), the mean direct healthcare cost for each COPD patient was estimated at £171.69 (US$309) per annum, as per the year 2000 estimates [40].
Dalal and colleagues evaluated the direct healthcare costs (data evaluated between 1 January 2005 and 30 September 2008) associated with COPD care during 2008 in a hospital setting among COPD patients aged ≥40 years. The mean costs for emergency department (ED) visits were US$647 (SD US$445), simple admissions were US$7,242 (SD US$7,987), and complex admissions (intensive care unit [ICU; general, surgical, or medical] or intubation) were US$20,757 (SD US$41,370). Complex admissions accounted for 20.9 % of the total costs for COPD management in a hospital setting [41].
3.3.2 Impact of Demographic Characteristics
An association between age of patients with COPD and increase in healthcare resource utilisation was observed, whereas gender was not considered as an independent predictor of healthcare resource utilisation [42–45]. Readmission at least twice in the first year of follow-up was observed among 9 % of total patients with COPD studied and was related to increasing age and male gender [46]. However, Berkius and colleagues observed that although the majority of readmissions were observed in women, female gender was not an independent determinant of readmission [odds ratio (OR) 0.97; 95 % confidence interval (CI) 0.75–1.25]. Age was observed to be independently associated with readmissions, with older patients demonstrating less chance of being readmitted (OR 0.68; 95 % CI 0.59–0.79 per 10-year increase in age) [42]. Furthermore, with an increase in years of schooling, a fall in direct medical costs associated with COPD was observed [40].
3.3.3 Impact of Respiratory Symptoms and Dyspnoea
In multiple studies across several countries evaluating data from the Confronting COPD survey, costs were higher in patients with severe dyspnoea [MRC dyspnoea scale (dyspnoea score 5)] compared with those with mild (dyspnoea score 0–2) and moderate (dyspnoea score 3–4) dyspnoea [9, 39, 47–51]. In the UK, costs ranged from €590 (direct cost €395; indirect cost €195) in patients with mild dyspnoea, to €4,670 (direct cost €3,036; indirect cost €1,634) in those with severe dyspnoea in the Confronting COPD survey [9]. In Italy, the corresponding costs ranged from €441 in patients with mild dyspnoea to €6,365 in those with severe dyspnoea in the Confronting COPD survey [48].
The annual costs per patient increased with an increase in dyspnoea severity (according to the mMRC criteria) and duration of the disease (higher cost in the second year). However, it was observed that with the exclusion of medication costs, the costs 2 years post-diagnosis decreased compared with the costs 1 year post-diagnosis (£2,499.85 and £3,149.53, respectively). This could be attributed to better symptom control and disease management strategies in the primary care setting [52]. Gabriel and colleagues reported that COPD patients with chronic symptoms of airflow obstruction were associated with a higher rate of hospital service utilisation (1000/year) (19.6, 95 % CI 8.8–43.7 vs. 3.3, 95 % CI 0.8–13.2) compared with those without chronic symptoms [53].
3.3.4 Impact of Comorbid Conditions
Across countries, the annual societal costs associated with symptomatic COPD were higher among patients with comorbidities compared with those without any comorbidity [9, 39, 41, 47–51]. The rate of hospital admissions, ER visits, and physician consultations was higher among patients with comorbidities [37]. Perera and colleagues [54] reported that comorbidities were associated with significantly higher hospitalisation costs in the US (p < 0.001).
3.3.5 Indirect Cost
Very few studies have examined the impact of symptomatic COPD on indirect costs, despite the fact that these are quite substantial. In the US, productivity loss was significantly higher in patients with both night-time and early morning symptoms compared with those without symptoms [55]. The Confronting COPD survey estimated the average indirect costs among US participants at 27 % of the total societal costs [39]. In Italy, costs due to absenteeism from work decreased significantly over a period of time due to the substantial decline in the number of exacerbations experienced by patients with COPD [56]. These observations were in line with those of an analysis based on an RCT in patients with COPD in which the increased cost of treatment was offset by indirect cost savings as a result of a decrease in the frequency of exacerbations [57].
4 Discussion
The current systematic literature review was undertaken to establish evidence on humanistic burden (based on HRQoL parameters) and economic burden in patients with symptomatic COPD.
4.1 Humanistic Burden
The results of humanistic burden showed variability in the inclusion criteria based on disease severity evaluated by using spirometry (mild, moderate, severe, and very severe) at the time of diagnosis. The evaluated studies included patients aged ≥40 years, with few studies particularly focussing on geriatric patients (>65 years of age) [25, 35, 58–60]. Patients with symptomatic COPD were associated with impaired HRQoL. These findings are in line with the findings from Jones and colleagues who reported impaired HRQoL in patients with a CAT score ≥10 [61].
Demographic factors such as age and gender, and other factors such as marital status, education level, or employment status, were found to have an impact on the humanistic burden of the disease. An association between advancing age and deteriorating HRQoL was reported in a majority of the studies (n = 17). In addition, duration of illness was the disease-driven factor, while severity of dyspnoea and time of symptoms (daytime or night-time symptoms) were disease-specific factors affecting the humanistic burden of the disease [4, 30, 33, 36, 62]. These findings are in line with the findings of the systematic review conducted by Tsiligianni and colleagues [63], where gender, BMI, smoking, symptoms, comorbidity, depression, anxiety, and exacerbations were reported as important parameters impacting the HRQoL of patients with COPD. Therefore, treatment strategies should also influence modifiable demographic factors to improve HRQoL in the COPD patient population.
Disease-specific symptoms such as dyspnoea considerably influenced the health of patients with COPD [31, 32, 63]. A longer duration of illness, longer hospital stay, and higher number of hospitalisations were other important factors influencing HRQoL in patients with symptomatic COPD [25, 28, 63, 64]. HRQoL also deteriorated with an increase in general respiratory symptoms and their severity. The symptoms evaluated in these studies included breathlessness or shortness of breath while walking, cough, sputum, wheeze, fatigue, and disability [4–6, 8, 25–27, 29, 63]. Therefore, a symptom-oriented approach involving treatment strategies aimed at severity of dyspnoea and exacerbations may improve HRQoL of COPD patients.
4.2 Economic Burden
Respiratory diseases are major causes of mortality and morbidity, and consume a considerable amount of healthcare resources. Among chronic respiratory diseases, COPD is associated with more healthcare consumption than other chronic diseases, and accounts for around five times as many hospital admissions in the UK compared with asthma [65]. A majority of included studies utilised reimbursement/claims/other databases as the sources of cost and resource use data. Variation in terms of country of study, year, currency, analysis perspective, disease severity, and cost/resource item under evaluation was observed in the published economic burden studies, making it difficult to compare across different health economies. Overall, both modifiable and non-modifiable demographic risk factors such as low education status, increasing age, and female gender were associated with greater annual societal costs. Higher societal costs were incurred for patients with increasing comorbidities, disease severity, frequency and severity of exacerbation, and symptoms. These factors directly influenced treatments administered, equipment used, labour, diagnosis, hospital admissions, PCP visits, specialist visits, ER visits, etc., thus, increasing the total direct costs across all the studies. Furthermore, indirect costs of absenteeism from work also suggest that a cost-effective treatment should focus on all aspects of the response to the disease per se, its consequence, and its progression.
4.3 Limitations
This systematic review is a qualitative evaluation of available evidence in symptomatic COPD; therefore, it does not provide a complete picture of COPD burden. Although better and reliable associations of various factors with symptomatic COPD can be achieved through quantitative analysis of HRQoL data, it was not conducted for the current review. Vague definitions of symptomatic COPD across studies made evidence generation a challenging task. In many studies, generic questionnaires [EQ-5D, SF-12, SF-36, and Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT–F)] were used to measure HRQoL, which are less sensitive when compared with disease-specific tools for COPD (Clinical COPD Questionnaire (CCQ), St. George’s Respiratory Questionnaire (SGRQ), Sino-Nasal Outcome Test-22 (SNOT-22), CAT, CRQ-SAS). Also, a majority of the studies (>50 %) recruited patients with symptomatic COPD from an outpatient setting, mostly primary care centres; therefore, they may not represent the COPD population at large. The HRQoL component of the review focused on studies published in English only. Non–English language studies meeting the inclusion criteria of the review were included only from the LILACS® database. Nearly 30 % of the included studies on humanistic and economic burden were published as conference abstracts. Very few studies presented evidence on indirect costs associated with symptomatic COPD, although indirect costs are a major contributor to the overall economic burden of symptomatic COPD. This could be attributed to the fact that symptoms act as triggers that generate indirect costs followed by direct costs from clinical evaluation and treatment. Therefore, a better understanding of symptoms and symptom control should be the primary focus of future research.
5 Conclusions
HRQoL among patients with symptomatic COPD, as well as management of the disease, were associated with a substantial burden, especially in the developed nations of Europe and North America. This is particularly relevant because the burden of symptomatic COPD patients in the early stages might be higher than for non-symptomatic patients in slightly advanced disease. Therefore, this review attempted to better understand and quantify this difficult-to-define symptomatic COPD. HRQoL in patients with symptomatic COPD was influenced by various factors, of which dyspnoea was the most important determinant. In terms of economic burden, after excluding increase in disease severity and exacerbations, the presence of comorbidities, increasing age, and female gender were the critical parameters associated with an increase in the societal burden of symptomatic COPD. Future COPD cost-of-illness studies should take into account all types of costs incurred by patients, including indirect costs, to determine the most appropriate estimation of economic burden of the disease. In addition, early diagnosis and better treatment and disease management strategies should be undertaken to further curtail the economic burden of symptomatic COPD on patients, especially in the developed nations of the world.
References
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2014. http://www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed 15 Mar 2014.
Calverley PM, Walker P. Chronic obstructive pulmonary disease. Lancet. 2003;362:1053–61.
Dal Negro R. Optimizing economic outcomes in the management of COPD. Int J Chron Obstruct Pulmon Dis. 2008;3:1–10.
Al Moamary MS, Tamim HM, Al-Mutairi SS, Al-Khouzaie TH, Mahboub BH, et al. Quality of life of patients with chronic obstructive pulmonary disease in the Gulf Cooperation Council countries. Saudi Med J. 2012;33:1111–7.
Bellas H, Connolly B, Birring S, Hurst B. Effect of cough on health-related quality of life in COPD [poster]. In: Presented at the European Respiratory Society Conference, Vienna. 2 Sep 2012. https://www.ersnetsecure.org/public/prg_congres.abstract?ww_i_presentation=56183. Accessed 10 Jul 2014.
Bentsen SB, Rokne B, Wahl AK. Comparison of health-related quality of life between patients with chronic obstructive pulmonary disease and the general population. Scand J Caring Sci. 2013;27:905–12.
Boros PW, Lubinski W. Health state and the quality of life in patients with chronic obstructive pulmonary disease in Poland: a study using the EuroQoL-5D questionnaire. Pol Arch Med Wewn. 2012;122:73–81.
Bridevaux PO, Gerbase MW, Probst-Hensch NM, Schindler C, Gaspoz JM, Rochat T. Long-term decline in lung function, utilisation of care and quality of life in modified GOLD stage 1 COPD. Thorax. 2008;63:768–74.
Britton M. The burden of COPD in the UK: results from the Confronting COPD survey. Respir Med. 2003;97 Suppl C:S71–9.
Punekar YS, Shukla A, Mullerova H. COPD management costs according to the frequency of COPD exacerbations in UK primary care. Int J Chron Obstruct Pulmon Dis. 2014;9:65–73.
Baty F, Putora PM, Isenring B, Blum T, Brutsche M. Comorbidities and burden of COPD: a population based case-control study. PLoS One. 2013;8:e63285.
Garcia-Olmos L, Alberquilla A, Ayala V, Garcia-Sagredo P, Morales L, Carmona M, et al. Comorbidity in patients with chronic obstructive pulmonary disease in family practice: a cross sectional study. BMC Fam Pract. 2013;14:11.
Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32:962–9.
Fletcher MJ, Upton J, Taylor-Fishwick J, Buist SA, Jenkins C, Hutton J, et al. COPD uncovered: an international survey on the impact of chronic obstructive pulmonary disease [COPD] on a working age population. BMC Public Health. 2011;11:612.
Jones P, Lareau S, Mahler DA. Measuring the effects of COPD on the patient. Respir Med. 2005;99 Suppl B:S11–8.
Gupta B, Kant S. Health related quality of life (HRQoL) in COPD. Internet J Pulm Med 2009;11:1. http://www.ispub.com/journal/the_internet_journal_of_pulmonary_medicine/volume_11_number_1a/article/health-related-quality-of-life-hrqol-in-copd.html. Accessed 10 Jul 2014.
Hynninen MJ, Pallesen S, Nordhus IH. Factors affecting health status in COPD patients with co-morbid anxiety or depression. Int J Chron Obstruct Pulmon Dis. 2007;2:323–8.
Hilleman DE, Dewan N, Malesker M, Friedman M. Pharmacoeconomic evaluation of COPD. Chest. 2000;118:1278–85.
Hessey SM, Jarad NA. Reducing exacerbations of chronic obstructive pulmonary disease (COPD): a review of current pharmacological strategies. West Engl Med J. 2012;111:1.
Wang Q, Bourbeau J. Outcomes and health-related quality of life following hospitalization for an acute exacerbation of COPD. Respirology. 2005;10:334–40.
Moher D, Liberati A, Tetzlaff J. Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377–84.
Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ Economic Evaluation Working Party. BMJ. 1996;313:275–83.
Lu M, Yao WZ, Zhong NS, Zhou YM, Wang C, Chen P, et al. Asymptomatic patients of chronic obstructive pulmonary disease in China. Chin Med J (Engl). 2010;123:1494–9.
Mollaoglu M, Fertelli TK, Tuncay FO. Fatigue and disability in elderly patients with chronic obstructive pulmonary disease (COPD). Arch Gerontol Geriatr. 2011;53:e93–8.
Hens G, Vanaudenaerde BM, Bullens DM, Piessens M, Decramer M, Dupont LJ, et al. Sinonasal pathology in nonallergic asthma and COPD: ‘united airway disease’ beyond the scope of allergy. Allergy. 2008;63:261–7.
Voll-Aanerud M, Eagan TM, Wentzel-Larsen T, Gulsvik A, Bakke PS. Respiratory symptoms, COPD severity, and health related quality of life in a general population sample. Respir Med. 2008;102:399–406.
Antoniu SA, Puiu A, Zaharia BG, Azoicai D. Age has no significant impact on health-related quality of life in patients hospitalized for COPD exacerbations. Value Health. 2011;14:A498.
Mazur W, Kupiainen H, Pitkaniemi J, Kilpelainen M, Sintonen H, Lindqvist A, et al. Comparison between the disease-specific Airways Questionnaire 20 and the generic 15D instruments in COPD. Health Qual Life Outcomes. 2011;9:4.
Scharf SM, Maimon N, Simon-Tuval T, Bernhard-Scharf BJ, Reuveni H, Tarasiuk A. Sleep quality predicts quality of life in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2011;6:1–12.
Jones PW, Adamek L, Nadeau G, Banik N. Comparisons of health status scores with MRC grades in COPD: for the GOLD 2011 classification. Eur Respir J. 2013;42:647–54.
Lopez Jove OR, Giugno E, Galdames A, Barrionuevo V, Rey S, Tabaj G, et al. Quality of life in patients with COPD: its relation to GOLD stages and dyspnea. In: Presented at the American thoracic society international conference; 18–23 May 2012; San Francisco (CA). http://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2012.185.1_MeetingAbstracts.A1517. Accessed 10 Jul 2014.
Punekar YS, Rodriguez-Roisin R, Sculpher M, Jones P, Spencer M. Implications of chronic obstructive pulmonary disease (COPD) on patients’ health status: a western view. Respir Med. 2007;101:661–9.
Sullivan SD, Cai Q, Mocarski M, Stephenson JJ, Tan H, et al. Patient-reported quality of life and dyspnea among COPD patients with nighttime and/or early morning symptoms. Value Health. 2013;16:A239.
Lu Y, Nyunt MS, Gwee X, Feng L, Feng L, Kua EH, et al. Life event stress and chronic obstructive pulmonary disease (COPD): associations with mental well-being and quality of life in a population-based study. BMJ Open. 2012;2:e001674.
Carvounis CP, Nikas N, Panitti E. Epidemiological survey in primary care patients with chronic obstructive pulmonary disease in Greece. The EPIPTOSI study. Pneumon. 2012;25:386–94.
Polatli M, Ben Kheder A, Wali S, Javed A, Khattab A, Mahboub B, BREATHE Study Group, et al. Chronic obstructive pulmonary disease and associated healthcare resource consumption in the Middle East and North Africa. The BREATHE study. Respir Med. 2012;106(Suppl 2):S75–85.
Wouters EF. Economic analysis of the Confronting COPD survey: an overview of results. Respir Med. 2003;97 Suppl C:S3–14.
Halpern MT, Stanford RH, Borker R. The burden of COPD in the USA: results from the Confronting COPD survey. Respir Med. 2003;97 Suppl C:S81–9.
Murtagh E, O’Neill C, McAllister D, Kee F, Macmahon J, Heaney LG. A cross-Ireland. Treat Respir Med. 2006;5:495–501.
Dalal AA, Shah M, D’Souza AO, Rane P. Costs of COPD exacerbations in the emergency department and inpatient setting. Respir Med. 2011;105:454–60.
Berkius J, Nolin T, Mardh C, Karlstrom G. Walther SM; Swedish Intensive Care Registry. Characteristics and long-term outcome of acute exacerbations in chronic obstructive pulmonary disease: an analysis of cases in the Swedish Intensive Care Registry during 2002–2006. Acta Anaesthesiol Scand. 2008;52:759–65.
Fuhrman C, Roche N, Vergnenegre A, Zureik M, Chouaid C, Delmas MC. Hospital admissions related to acute exacerbations of chronic obstructive pulmonary disease in France, 1998–2007. Respir Med. 2011;105:595–601.
Lampela P, Saynajakangas O, Keistinen T. Is the treatment of acute COPD exacerbations in Finland shifting to general practitioners? Scand J Prim Health Care. 2006;24:140–4.
Varol Y, Varol U, Baser Z, Usta L, Balci G, Özacar R. The cost of COPD exacerbations managed in hospital. Turk Toraks Derg. 2013;14:19–23.
Johannesdottir SA, Christiansen CF, Johansen MB, Olsen M, Xu X, Parker JM, et al. Hospitalization with acute exacerbation of chronic obstructive pulmonary disease and associated health resource utilization: a population-based Danish cohort study. J Med Econ. 2013;16:897–906.
Chapman KR, Bourbeau J, Rance L. The burden of COPD in Canada: results from the Confronting COPD survey. Respir Med. 2003;97 Suppl C:S23–31.
Dal Negro R, Rossi A, Cerveri I. The burden of COPD in Italy: results from the Confronting COPD survey. Respir Med. 2003;97 Suppl C:S43–50.
Izquierdo JL. The burden of COPD in Spain: results from the Confronting COPD survey. Respir Med. 2003;97 Suppl C:S61–9.
Piperno D, Huchon G, Pribil C, Boucot I, Similowski T. The burden of COPD in France: results from the Confronting COPD survey. Respir Med. 2003;97 Suppl C:S33–42.
Wouters EF. The burden of COPD in The Netherlands: results from the Confronting COPD survey. Respir Med. 2003;97 Suppl C:S51–9.
Punekar YS, Wurst K, Shukla A. COPD management costs among newly diagnosed COPD patients in the UK primary care Setting. In: Presented at the American thoracic society international conference; 17–22 May 2013; Philadelphia, PA. Available at: http://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2013.187.1_MeetingAbstracts.A4373. Accessed 10 Jul 2014.
Gabriel SI, Teodorescu A, Dan DI, Maria A. Who win? Spirometry versus symptoms for predicting the longitudinal outcomes in COPD patients: 10 years observation. Eur Respir J. 2011;38(Suppl 55):949.
Perera PN, Armstrong EP, Sherrill DL, Skrepnek GH. Acute exacerbations of COPD in the US: inpatient burden and predictors of costs and mortality. COPD. 2012;9:131–41.
Cai Q, Sullivan SD, Stephenson JJ, Tan H, Kavati A, et al. Health-related quality of life and work productivity of employed COPD patients with nighttime and early morning symptoms. In: Presented at the American thoracic society (ATS) international conference; 17–22 May 2013; Philadelphia, PA. http://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2013.187.1_MeetingAbstracts.A2939. Accessed 10 Jul 2014.
Dal Negro R, Bonadiman L, Tognella S, Micheletto C, Turco P. The impact of LABA + ICS fixed combinations on morbidity and economic burden of COPD in Italy: a 6-year observational study. Ther Adv Respir Dis. 2011;5:83–90.
Ayres JG, Price MJ, Efthimiou J. Cost-effectiveness of fluticasone propionate in the treatment of chronic obstructive pulmonary disease: a double-blind randomized, placebo-controlled trial. Respir Med. 2003;97:212–20.
Hernandez C, Casas A, Escarrabill J, Alonso J, Puig-Junoy J, Farrero E, et al. CHRONIC project. Home hospitalisation of exacerbated chronic obstructive pulmonary disease patients. Eur Respir J. 2003;21:58–67.
Stridsman C, Mullerova H, Skar L, Lindberg A. Fatigue in COPD and the impact of respiratory symptoms and heart disease: a population-based study. COPD. 2013;10:125–32.
Aimonino Ricauda N, Tibaldi V, Leff B, Scarafiotti C, Marinello R, Zanocchi M, et al. Substitutive “hospital at home” versus inpatient care for elderly patients with exacerbations of chronic obstructive pulmonary disease: a prospective randomized, controlled trial. J Am Geriatr Soc. 2008;56:493–500.
Jones PW, Tabberer M, Chen WH. Creating scenarios of the impact of COPD and their relationship to COPD Assessment Test (CAT) scores. BMC Pulm Med. 2011;11:42.
Bestall JC, Paul EA, Garrod R, Granham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54:581–6.
Tsiligianni I, Kocks J, Tzanakis N, Siafakas N, van der Molen T. Factors that influence disease-specific quality of life or health status in patients with COPD: a review and meta-analysis of Pearson correlations. Prim Care Respir J. 2011;20:257–68.
Diamantea F, Tiskrika S, Karakontaki F, Mitromaras D, Stagaki E, Kastanakis E, et al. Factors determining duration of hospital stay in patients hospitalized for acute COPD exacerbation. Eur Respir J. 2011;38(Suppl 55):906.
Chung F, Barnes N, Allen M, Angus R, Corris P, Knox A, et al. Assessing the burden of respiratory disease in the UK. Respir Med. 2002;96:963–75.
Almagro P, Barreiro B, Ochoa de Echaguen A, Quintana S, Rodriguez Carballeira M, Heredia JL, et al. Risk factors for hospital readmission in patients with chronic obstructive pulmonary disease. Respiration. 2006;73:311–7.
Elmariami M, McGarry K, Yakubu D, Shamssain M. Association between respiratory viruses and exacerbations in COPD patients. Presented at the European Respiratory Society Conference; 18–22 Sep 2010; Barcelona. https://www.ersnetsecure.org/public/prg_congres.abstract?ww_i_presentation=47378. Accessed 10 Jul 2014.
Llor C, Molina J, Naberan K, Cots JM, Ros F, Miravitlles M, EVOCA study group. Exacerbations worsen the quality of life of chronic obstructive pulmonary disease patients in primary healthcare. Int J Clin Pract. 2008;62:585–92.
Goossens LM, Nivens MC, Sachs P, Monz BU. Rutten-van Molken MP. Is the EQ-5D responsive to recovery from a moderate COPD exacerbation? Respir Med. 2011;105:1195–202.
Loh LC, Lai CH, Liew OH, Siow YY. Symptomatology and health status in patients with chronic obstructive pulmonary disease. Med J Malaysia. 2005;60:570–7.
Mocarski M, Schaefer ML, Palsgrove A, Hareendran A, Houghton K, Carson RT, et al. Patients’ experience of nighttime COPD symptoms: results from qualitative research. Presented at the American thoracic society international conference; 13–18 May 2011; Denver (CO). http://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2011.183.1_MeetingAbstracts.A1479. Accessed 10 Jul 2014.
Partridge M, Vogelmeier C, Miravitlles M, Cazzola M, Leynaud D, Ostinelli J, et al. Sleep disturbance in patients with severe COPD. Presented at the European Respiratory Society Conference; 19 Sep 2010; Barcelona. https://www.ersnetsecure.org/public/prg_congres.abstract?ww_i_presentation=48684. Accessed 10 Jul 2014.
Shafiq I, Huggett K, Idris l, Rudran B, Shaw T. Use of COPD assessment (CAT) test in monitoring acute exacerbations [poster]. Presented at the European Respiratory Society Annual Congress; 24–28 Sep 2011; Amsterdam. http://f1000.com/posters/browse/summary/1089343. Accessed 10 Jul 2014.
Solem C, Sun S, Macahilig C, Katyal M, Gao X. Burden of COPD exacerbations in severe and very severe COPD patients: initial results of a nationally representative patient survey and chart review. Chest. 2012;142:718A.
Trappenburg JC, Touwen I, de Weert-van Oene GH, Bourbeau J, Monninkhof EM, Verheij TJM, et al. Detecting exacerbations using the Clinical COPD Questionnaire. Health Qual Life Outcomes. 2010;8:102.
Andreassen SL, Liaaen ED, Stenfors N, Henriksen AH. Impact of pneumonia on mortality and length of stay in patients hospitalized with acute COPD exacerbations. Eur Respir J. 2011;38(Suppl 55):565.
Asai N, Ohkuni Y, Iwasaki T, Matsunuma R, Nakashima K, Otsuka Y, et al. Efficacy and safety of single-dose 2.0 g azithromycin in the treatment of acute exacerbation of chronic obstructive pulmonary disease. J Infect Chemother. 2011;17:793–8.
Bahadori K, FitzGerald JM, Levy RD, Fera T, Swiston J. Risk factors and outcomes associated with chronic obstructive pulmonary disease exacerbations requiring hospitalization. Can Respir J. 2009;16:e43–9.
Bakerly ND, Davies C, Dyer M, Dhillon P. Cost analysis of an integrated care model in the management of acute exacerbations of chronic obstructive pulmonary disease. Chron Respir Dis. 2009;6:201–8.
Ban A, Ismail AR, Abdul Rahman A, Sulung S, Syed Mohamed A. Impact of clinical pathway on clinical outcomes in the management of COPD exacerbation. BMC Pulm Med. 2012;12:27.
Bertolini G, Confalonieri M, Rossi C, Rossi G, Simini B, Gorini M, GiViTI Group, et al. Costs of the COPD. Differences between intensive care unit and respiratory intermediate care unit. Respir Med. 2005;99:894–900.
Bingol H, Cingoz F, Balkan A, Kilic S, Bolcal C, Demirkilic U, et al. The effect of oral prednisolone with chronic obstructive pulmonary disease undergoing coronary artery bypass surgery. J Card Surg. 2005;20:252–6.
Camp PG, Burns J, Lane C, Sin D, van Eeden S. Factors associated with rehospitalization within 14 days of hospital discharge for an acute exacerbation of chronic obstructive pulmonary disease. Chest. 2010;138:472A.
Chandra D, Tsai CL, Camargo CA Jr. Acute exacerbations of COPD: delay in presentation and the risk of hospitalization. COPD. 2009;6:95–103.
Chen YH, Yao WZ, Cai BQ, Wang H, Deng XM, Gao HL, et al. Economic analysis in admitted patients with acute exacerbation of chronic obstructive pulmonary disease. Chin Med J (Engl). 2008;121:587–91.
Chen Y, Yao W, Kang J, Cai B, Zhou X, et al. Perception of patients with frequent exacerbation of COPD: National multi-center survey in China. In: Presented at the American thoracic society (ATS) international conference; 17–22 May 2013; Philadelphia, Pennsylvania. http://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2013.187.1_MeetingAbstracts.A1438. Accessed 10 Jul 2014.
Chmielowicz B, Panaszek B, Obojski A. Hospital management of patients with exacerbation of severe and very severe chronic obstructive pulmonary disease (COPD): protocol of treatment and discharge. In: Presented at the American thoracic society international conference; 13–18 May 2011; Denver, CO. http://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2011.183.1_MeetingAbstracts.A3119. Accessed 10 Jul 2014.
Dal Negro RW, Bonadiman L, Turati C, Turco P. Clinical and pharmacoeconomic profile of COPD patients with FEV1 50–60 % predicted: pilot study on the impact of the extended indication of ICS/LABA. Ther Adv Respir Dis. 2009;3:51–8.
Dalal AA, Shah MB, D’Souza AO, Lunacsek OE, Nagar SP, Crater GD. Observational study of the outcomes and costs of initiating maintenance therapies in patients with moderate exacerbations of COPD. Respir Res. 2012;13:41.
de Jong YP, Uil SM, Grotjohan HP, Postma DS, Kerstjens HA, van den Berg JW. Oral or IV prednisolone in the treatment of COPD exacerbations: a randomized, controlled, double-blind study. Chest. 2007;132:1741–7.
de Miguel-Diez J, Jimenez-Garcia R, Hernandez-Barrera V, Puente-Maestu L, Rodriguez-Rodriguez P, Lopez de Andres A, et al. Trends in hospital admissions for acute exacerbation of COPD in Spain from, 2006 to 2010. Respir Med. 2013;107:717–23.
Drescher GS, Carnathan BJ, Imus S, Colice GL. Incorporating tiotropium into a respiratory therapist-directed bronchodilator protocol for managing in-patients with COPD exacerbations decreases bronchodilator costs. Respir Care. 2008;53:1678–84.
Eaton T, Young P, Fergusson W, Moodie L, Zeng I, O’Kane F, et al. Does early pulmonary rehabilitation reduce acute health-care utilization in COPD patients admitted with an exacerbation? A randomized controlled study. Respirology. 2009;14:230–8.
Edelman DA, Maleyko-Jacobs S, White MT, Lucas CE, Ledgerwood AM. Smoking and home oxygen therapy: a preventable public health hazard. J Burn Care Res. 2008;29:119–22.
Geitona M, Hatzikou M, Steiropoulos P, Alexopoulos EC, Bouros D. The cost of COPD exacerbations: a university hospital-based study in Greece. Respir Med. 2011;105:402–9.
George PM, Stone RA, Buckingham RJ, Pursey NA, Lowe D, Roberts CM. Changes in NHS organization of care and management of hospital admissions with COPD exacerbations between the national COPD audits of 2003 and 2008. QJM. 2011;104:859–66.
Golmohammadi K, Jacobs P, Sin DD. Economic evaluation of a community-based pulmonary rehabilitation program for chronic obstructive pulmonary disease. Lung. 2004;182:187–96.
Hutchinson A, Brand C, Irving L, Roberts C, Thompson P, Campbell D. Acute care costs of patients admitted for management of chronic obstructive pulmonary disease exacerbations: contribution of disease severity, infection and chronic heart failure. Intern Med J. 2010;40:364–71.
Kruavit A, Thien F. Systemic corticosteroids are still inappropriately prescribed in hospital patients with COPD exacerbation. Respirology. 2013;18:58.
Lerikou M, Dimopoulos G, Tsiodras S, Chranioti A, Perros E, Anagnostopoulouet U, et al. Elderly vs non-elderly patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) due to a viral infection [poster]. In: Presented at the European Respiratory Society Conference, Vienna, 3 Sep 2012. https://www.ersnetsecure.org/public/prg_congres.abstract?ww_i_presentation=55529. Accessed 10 Jul 2014.
Limsuwat C, Nantsupawat T, Kijsirichareanchai K, Nugent K. Factors predicting length of stay in patients with chronic obstructive pulmonary disease exacerbations admitted to intensive care. J Invest Med. 2012;60:445.
Lindenauer PK, Rothberg MB, Pekow PS, Kenwood C, Benjamin EM, Auerbach AD. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007;357:2589–600.
Martinez CH, Raparla S, Plauschinat CA, Giardino ND, Rogers B, Beresford J, et al. Gender differences in symptoms and care delivery for chronic obstructive pulmonary disease. J Womens Health (Larchmt). 2012;21:1267–74.
Monteiro F, Cunha K, Silva R, TodoBom F, Lopes C, Azevedo P, et al. Is there a difference in outcome according to etiology of COPD exacerbation in patients admitted to an ICU? Eur Respir J. 2011;38(Suppl 55):2054.
Nangia V, Gandhi K. Use of procalcitonin to guide the antibiotic therapy in patients with an acute exacerbation of COPD in a resource-limited setting: a case-control study. In: Presented at the 22nd European Congress of clinical microbiology and infectious diseases, London, 2 Apr 2012. http://registration.akm.ch/einsicht.php?XNABSTRACT_ID=142089&XNSPRACHE_ID=2&XNKONGRESS_ID=161&XNMASKEN_ID=900. Accessed 10 Jul 2014.
Nasciben V. Resource use and costs of exacerbation management of chronic obstructive pulmonary disease patients under the private healthcare system in Brazil: role of maintenance treatment in the exacerbation prevention in severe patients. Value Health. 2011;14:A140.
Nielsen R, Johannessen A, Bakke PS, Askildsen JE, Omenaas ER, Gulsvik A. Aspects of healthcare utilisation in self-reported obstructive lung disease. Clin Respir J. 2009;3:34–41.
Nikolakopoulou S, Hillas G, Veldekis D, Bakakos P. Exacerbations of chronic obstructive pulmonary disease (COPD): correlation of hospitalization days with epidemiological and clinical parameters. Presented at the European Respiratory Society Conference, Barcelona, 18–22 Sep 2010. http://www.ers-education.org/Media/Media.aspx?idMedia=138269. Accessed 10 Jul 2014.
Nishimura K, Yasui M, Nishimura T, Oga T. Clinical pathway for acute exacerbations of chronic obstructive pulmonary disease: method development and five years of experience. Int J Chron Obstruct Pulmon Dis. 2011;6:365–72.
Ornek T, Tor M, Altin R, Atalay F, Geredeli E, Soylu O, et al. Clinical factors affecting the direct cost of patients hospitalized with acute exacerbation of chronic obstructive pulmonary disease. Int J Med Sci. 2012;9:285–90.
Overbeek JA, Balp MM, Penning FJA, Dekhuijzen PNR, Herings RMC. Burden of exacerbations in patients with COPD in the Netherlands: a real-life study. Value Health. 2012;15:A560–1.
Ozkaya S, Findik S, Atici AG. The costs of hospitalization in patients with acute exacerbation of chronic obstructive pulmonary disease. Clinicoecon Outcomes Res. 2011;3:15–8.
Ramanath KV, Sabith JK. Pharmacoeconomic evaluation of acute exacerbations of COPD treatment in a rural tertiary care hospital. Int J Pharm Sci Res. 2012;3:1155–60.
Roberts MH, Borrego M, Petersen H, Kharat A, Blanchette C. Estimating the burden and course of severe COPD exacerbations in the U.S. hispanic population. In: Presented at the American thoracic society international conference, Denver, CO, 13–18 May 2011. http://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2011.183.1_MeetingAbstracts.A1496. Accessed 10 Jul 2014.
Romagnoli M, Dell’Orso D, Lorenzi C, Crisafulli E, Costi S, Lugli D, et al. Repeated pulmonary rehabilitation in severe and disabled COPD patients. Respiration. 2006;73:769–76.
Rosychuk RJ, Voaklander DC, Senthilselvan A, Klassen TP, Marrie TJ, Rowe BH. Presentations to emergency departments for chronic obstructive pulmonary disease in Alberta: a population-based study. CJEM. 2010;12:500–8.
Rowe BH, Rosychuk R, Espinola JA, Krishnan JA, Lang ES, Camargo CA Jr. Comparison of Canadian versus US emergency department visits and admission rates for acute exacerbations of chronic obstructive pulmonary disease. CJEM. 2010;12:247.
Mittmann N, Kuramoto L, Seung SJ, Haddon JM, Bradley-Kennedy C, Fitzgerald JM. The cost of moderate and severe COPD exacerbations to the Canadian healthcare system. Respir Med. 2008;102:413–21.
Shen N. The direct admitted medical cost of acute exacerbation of chronic obstructive pulmonary disease. Respirology. 2011;16:123.
Silver H, Blanchette CM, Roberts M, Petersen H, St Charles ME. Prevalence of comorbidities in patients hospitalized for COPD exacerbations and impact on impatient mortality and hospital expenditures. Presented at the American Thoracic Society International Conference, New Orleans, LA, 14–19 May 2010. http://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2010.181.1_MeetingAbstracts.A5943. Accessed 10 Jul 2014.
Simoens S, Decramer M, De Coster S, Celis G, Laekeman G. Clinical and economic analysis of antimicrobial therapy of chronic obstructive pulmonary disease exacerbations. Int J Clin Pract. 2007;61:200–6.
Sridhar M, Taylor R, Dawson S, Roberts NJ, Partridge MR. A nurse led intermediate care package in patients who have been hospitalised with an acute exacerbation of chronic obstructive pulmonary disease. Thorax. 2008;63:194–200.
Stein BD, Charbeneau JT, Lee TA, Schumock GT, Lindenauer PK, Bautista A, et al. Hospitalizations for acute exacerbations of chronic obstructive pulmonary disease: how you count matters. COPD. 2010;7:164–71.
Tanriverdi H, Besir H, Pekbak G. Direct costs of acute exacerbation of COPD patients in a second level hospital. Chest. 2012;142:A659.
Tsai CL, Lee WY, Delclos GL, Hanania NA, Camargo CA Jr. Comparative effectiveness of noninvasive ventilation vs invasive mechanical ventilation in chronic obstructive pulmonary disease patients with acute respiratory failure. J Hosp Med. 2013;8:165–72.
Veettil SK, Salmiah MA, Rajiah K, Suresh Kumar BR. Cost of acute exacerbation of COPD in patients attending government hospital in Kerala, India. Int J Pharm Pharm Sci. 2012;4(Suppl 3):659–61.
Vitacca M, Bianchi L, Bazza A, Clini EM. Advanced COPD patients under home mechanical ventilation and/or long term oxygen therapy: Italian healthcare costs. Monaldi Arch Chest Dis. 2011;75:207–14.
Vitacca M, Bianchi L, Guerra A, Fracchia C, Spanevello A, Balbi B, et al. Tele-assistance in chronic respiratory failure patients: a randomised clinical trial. Eur Respir J. 2009;33:411–8.
Wang Y, Humerfelt S, Lurås H, Dahl FA, Stavem K, Haugen T. Readmissions after hospitalization for acute exacerbation of chronic obstructive pulmonary disease. In: Presented at the 19th European Respiratory Society Conference, Vienna, 12–16 Sep 2009. http://www.ers-education.org/Media/Media.aspx?idMedia=139915. Accessed 10 Jul 2014.
Yang HY, Wu J, Zheng Y, Xie K, Jin L, Xie J, et al. Economic burden associated with acute exacerbations of chronic obstructive pulmonary disease in China. Value Health. 2012;15:A54.
Acknowledgments
Funding for this study was provided by GlaxoSmithKline. All listed authors met the criteria for authorship set forth by the International Committee for Medical Journal Editors. Editorial support, in the form of development, assembling tables and figures, collating author comments, copyediting, fact checking, and referencing, was provided by Dr Annirudha Chillar of Cactus Communications Inc., and was funded by GlaxoSmithKline.
Support and financial disclosure declaration
Funding for this study was provided by GlaxoSmithKline. Yogesh Suresh Punekar is employed by GlaxoSmithKline and owns stocks in the company. Kunal Srivastava, Deepika Thakur, and Sheetal Sharma are employed by Parexel (Heron Health), which was commissioned by GlaxoSmithKline to undertake the research for this systematic review. The authors state that they have full control of all primary data and they agree to allow the journal to review their data if requested.
Author contributions
Kunal Srivastava, Deepika Thakur, and Sheetal Sharma contributed equally in designing the study protocol, methodology, analysis, and manuscript writing. Yoghesh Suresh Punekar contributed in designing the study protocol, methodology, and manuscript writing, and is the overall guarantor for the manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Srivastava, K., Thakur, D., Sharma, S. et al. Systematic Review of Humanistic and Economic Burden of Symptomatic Chronic Obstructive Pulmonary Disease. PharmacoEconomics 33, 467–488 (2015). https://doi.org/10.1007/s40273-015-0252-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40273-015-0252-4