
Abstract
Objectives
The aim of this study was to identify domains that determine quality of life in patients with peripheral arterial disease and find the patient-reported outcome measures that can examine the identified themes.
Methods
A systematic review of all the main six databases was undertaken to identify primary qualitative studies reporting on the health and/or quality of life of patients with peripheral arterial disease. The quality of studies was assessed using the Critical Appraisal Skills Program criteria. Findings from the included studies were analysed using framework analysis methodology. The identified themes were mapped against the items/domains of validated patient-reported outcome measures used in patients with peripheral arterial disease.
Results
The systematic review identified eight papers that fulfilled the inclusion criteria. The included papers reported the views of 186 patients with peripheral arterial disease including patients with intermittent claudication, critical ischaemia and amputation secondary to peripheral arterial disease. The overall quality of the included studies was good based on Critical Appraisal Skills Program criteria. Framework analysis identified 35 themes that were divided into six main groups: symptoms, impact on physical functioning, impact on social functioning, psychological impact, financial impact and process of care. The best-fit generic and disease-specific patient-reported outcome measures were the Nottingham Health Profile and the Vascular Quality of Life Questionnaire, respectively. None of the patient-reported outcome measures covered all the themes important to patients with peripheral arterial disease.
Discussion
The findings from the review identified the important domains that affect patients living with peripheral arterial disease. None of the current generic and disease-specific patient-reported outcome measures provide a comprehensive measure for all themes that impact the daily living of patients with peripheral arterial disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Peripheral arterial disease is a spectrum of conditions ranging from asymptomatic disease and minor claudication to limb loss |
Understanding and measuring quality of life in these patients is of paramount importance to guide intervention |
This systematic review is the most comprehensive attempt to measure the impact of this disease in its different manifestations and can help improve current measures used to measure quality of life |
1 Introduction
Population studies suggest that one in five people above the age of 60 years have some degree of peripheral arterial disease (PAD) in the lower limbs. The incidence of this disease increases with age [1]. Most patients with PAD are asymptomatic; however, patients can present with a spectrum of symptoms, reflecting different stages of the disease. The most common clinical presentation is intermittent claudication (IC), which is pain in the leg on walking; only 20% of these patients develop severe symptoms of critical limb ischaemia (CLI) [2]. Patients with CLI can present with rest pain, non-healing leg ulcers or gangrene; if they do not receive treatment they may lose part of their lower limbs [3, 4]. Patients with CLI have a high risk of mortality with nearly 25% dying and 30% requiring major lower limb amputation within 1 year [5, 6]. Symptomatic PAD results in significant functional limitations and reduced health-related quality of life in affected patients [5].
Peripheral arterial disease is a chronic disease and patients with this condition need support to choose the best treatment strategy to reduce the impact on their quality of life. Health-related quality of life can be measured using either generic or disease-specific patient-reported outcome measures (PROMs). Patient choice over treatment and care is a central feature of most advanced healthcare systems, it is proposed that information gathered by PROMs from patients directly can help inform the choice of treatments and promote equity as well as excellence [7].
Patients’ experience of treatment and care is a major indicator of quality and there has been a huge expansion in the development and application of PROMs. These instruments examine the most important issues to the patients by asking them directly about any changes. Patient-reported outcome measures provide an insight into the manner in which patients perceive their health and the impact that treatments have on their quality of life.
The aim of this study was to systematically review the qualitative evidence of people’s experiences of living with PAD. The identified domains were then mapped against the items/domains of identified validated generic and disease-specific PROMs [8]. The intention was to find the PROMs that captured the most important issues to patients with PAD.
2 Methods
The review aimed to find all the primary qualitative research studies (interview and/or focus groups) that explicitly investigated the impact of PAD on daily living, health and quality of life. The inclusion criteria included any patients with PAD (IC, CLI, ischaemic ulceration, necrosis, gangrene and amputation as a result of PAD). Any studies with undefined populations or mixed populations that included the views from patients not experiencing PAD were excluded.
For further information regarding the inclusion and exclusion criteria, refer to Table 1. This systematic review was undertaken and reported in accordance with the general principles recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. In accordance with the study protocol [9], searches were conducted from inception up to April 2017 in bibliographic databases including CINAHL via EBSCO, MEDLINE and MEDLINE in Process via Ovid, EMBASE via Ovid, PsycINFO via Ovid, Social Science Citation Index/Science Citation Index via Web of Science (Thomson Reuters), and Proquest dissertations and theses. No language or date constraints were applied.
The search strategy combined condition terms, terms for patient views and terms for qualitative studies (which augmented a qualitative study filter) [9]. Further details of the search strategy are provided in Appendix 1 (supporting information).
2.1 Study Selection
The search results were entered into Endnote X8™ (Thomson Reuters, Philadelphia, PA, USA) and two reviewers (AA, PP) independently screened the titles for inclusion and exclusion in accordance with the set criteria in the protocol. All titles were examined, and any citations that clearly did not meet the inclusion criteria (for example, mixed-population quantitative PROM data, unrelated to PAD) were excluded. For included titles, abstracts were read and for the included abstracts, full-text articles were obtained.
2.2 Quality Assessment
The Critical Appraisal Skills Program qualitative checklist instrument was used to assess the methodological quality of the included studies in the review [10]. This was selected as it assesses both the appropriateness and the quality of reporting of the studies included and is commonly used in qualitative reviews of evidence [11]. The Critical Appraisal Skills Program consists of ten questions about the qualitative methodology that are answered either as yes, no or unclear. Two of the authors (A.A. E.L.) independently examined the quality of each study and any inconsistencies were resolved by discussion or involving a third author (G.J.).
2.3 Data Extraction and Analysis
The data on authors, year of publication, country of study, number of participants, research aims, methods of recruitment, method of data collection, key results and analysis were extracted and tabulated for all the included studies. The first author (A.A.) uploaded all the papers into the qualitative data analysis software NVIvo10 (QSR International, Doncaster, VIC, Australia) and the primary and secondary texts (patient quotes reported in the articles and themes) were analysed. Framework analysis was used to identify common and variable themes within the text of each article [12]. The first stage of the analysis was undertaken by reading all the included papers to identify common terms and themes from within and across the articles. The second stage involved identifying a thematic framework by creating an initial coding scheme for the main themes; and eventually creating an index of themes. In the third stage, the thematic framework was applied to all the primary and secondary data in the included papers. A framework matrix was created to arrange the data per the thematic references in the fourth stage. In the fifth and final stage, themes were examined for their conceptual similarities and differences (mapping and interpretation stage). A second reviewer (E.L.) checked all the themes that were identified and differences in conceptualisation were discussed and adjusted.
2.4 Triangulation of Patient-Reported Outcome Measure Items with Qualitative Themes
To examine the extent to which the items within generic and PAD disease-specific PROMs corresponded to themes from the qualitative review, a triangulation approach was followed [13, 14]. The items from generic and disease-specific PROMs validated in patients with PAD [8] were examined in detail. The items from these instruments were mapped against the themes identified, and two researchers (A.A., E.L.) reviewed both the themes from the qualitative review and the PROM items/domains to evaluate whether the concepts were the same (agreement), offered similar concepts (partial agreement) or were not present (silence). The aim was to identify whether any of the instruments covered all the important issues from the PAD patients’ perspective.
3 Results
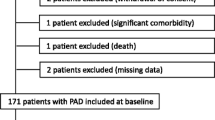
The database searches identified 1113 citations; after removing duplicates, 779 titles were assessed and subsequently 65 full-text papers were reviewed in detail. Finally, only eight papers fulfilled the inclusion criteria and were included in the qualitative evidence synthesis (see Fig. 1). The characteristics and main findings of the studies included in the qualitative synthesis are summarised in Table 2.

Preferred reporting items for systematic reviews and meta-analyses diagram: peripheral arterial disease qualitative systematic review
Two of the studies were conducted in the UK [15, 16], three in Sweden [17,18,19] and three in USA [20,21,22]. The studies were published between 1998 and 2015; the mean age of the participants in the included studies ranged from 64 to 77 years, and the percentage of male participants was 50–79%. The included studies reported the views of 186 patients with PAD including patients with IC, CLI and amputation of lower limbs as a result of PAD.
3.1 Quality Assessment
The overall quality of the included studies was good and all the studies scored “yes” for almost all the criteria set in the Critical Appraisal Skills Program checklist [10]; however, four studies scored “can’t tell” regarding consideration of the relationship between participants and the researcher [16, 19,20,21]. Only one study scored “can’t tell” when assessing if the recruitment strategy was appropriate to the aims of the research [20]. For further detail on the quality of the included studies, see Appendix 2 (supporting information).
3.2 Analysis
The framework analysis of the primary and secondary data in the included papers identified six main issues including symptoms, physical functioning, impact on social functioning, psychological impact, financial impact and process of care. In total, 35 themes were identified. Table 3 shows the themes and subthemes and the sources from the included papers in this review.
3.2.1 Symptoms
This theme included several subthemes such as pain, altered sensation, cold extremities, weakness, mobility, ulcers, sexual functioning and symptom progression.
Pain This was identified in all the included papers, severity of the disease resulted in different experiences of pain and this was reflected in the pain subthemes. Patients described different experiences with the initial appearance of the symptoms. Pain was most commonly described as discomfort, ache, cramp and creeping feelings of fatigue that got worse the farther they walked.
“I get a cramping in the left calf.” “My legs get tired. I can feel it in my thighs.” [21]
“I get this terrible cramp in my legs and then I don’t know where to go.” [17]
The description of pain in the legs and feet was different for patients with CLI. Some of these patients described rest pain and burning sharp pain in their feet and legs. Patients with vascular-related amputation described the same type of continuous rest pain prior to their amputation.
“If I could, I would have taken an axe and chopped off my leg sooner just to get rid of the pain.”
“When asked, 85% of patients felt that intolerable ischemic rest pain is the most appropriate threshold for having their limb amputated, as opposed to ulceration, gangrene, or when their physician stated that limb salvage was no longer possible.”
“I definitely would have had the amputation at the same time point. My pain got so bad, I could not walk.” [25]
Rest pain was also reported to be particularly troublesome during the night causing sleep disturbances. Patients had to adapt their position to deal with this pain. Some reported sleeping in a chair to overcome the severity of this pain.
“Experiences such as being forced to sit in a chair during the nights to stand the pain contributed to tiredness and feelings of exhaustion.” [17]
“The greatest benefits of revascularisations were the relief from pain, the ability to sleep again.” [18]
Patients with failed revascularisation and subsequent amputation reported pain at the site of the amputated limb; however, the phantom pain experienced was tolerable compared to the ischaemic rest pain [22]. Furthermore, patients who underwent revascularisation complained of some residual pain following the procedure. Participants in one study reported that they avoided exercise following their intervention and some believed that the pain on walking was an indication that activity causes damage to their muscles and legs [16].
Altered Sensation Participants in five studies [15,16,17, 20, 21] reported altered sensation in the affected limb; these symptoms were experienced by patients prior to and following the procedures. The description of this altered sensation ranged from feeling “a dead weight”, especially in patients with CLI [15], to a minor intermittent tingling feeling in patients with IC [21]. Altered sensation secondary to revascularisation was caused by either nerve damage or swelling post-interventions [16].
Cold Extremities Patients with chronic severe lower limb ischaemia complained of cold feet and legs; some of these patients reported that despite revascularisation the symptom persisted [18]. One participant described this symptom in the following terms:
“I can get up and walk a little and so on. Yes, I have to live with it. It’s sleeping now here and it gets cold, like, but when I’m moving the circulation is better. So I see that I’m never going to get rid of it but I can live with it because it doesn’t hurt in that way that it did before the operation.” [18]
In one study, some participants experienced coldness in the affected limb pre-operatively, postoperatively and after discharge; however, it was worse before revascularisation [15].
Weakness and Fatigue Weakness and fatigue was reported by participants in four studies [16, 17, 19, 20]. Some reported this symptom to be the first they experienced; describing fatigue on walking followed by pain and cramps the more they continued to walk [16, 19]. Some experienced loss of power with worsening fatigue as the disease progressed and many complained that despite intervention, the fatigue symptoms did not completely resolve. One patient described this symptom in the following terms:
“Yes, it’s just like it has taken the strength and power from me.” [17]
Many patients described that PAD meant living with long-term fatigue and powerlessness [17, 20].
Mobility All the included studies in this review highlighted problems with mobility to be the most important issue experienced by patients with PAD. The impact on mobility differed per the type of symptoms experienced, and the severity of the disease. The impact was worse in patients with CLI and amputees. Patients with IC reported reducing their walking to avoid the symptoms of pain. Patients with IC also reported employing specific strategies to avoid pain and discomfort on walking by stopping regularly, or avoiding walking uphill or upstairs [19,20,21].
“It depends completely on how hard I walk. If I walk very slowly, I can go many, many blocks, more than a dozen, or so. If I walk aggressively, I can start to feel something in maybe two blocks.” [21]
“I usually shy away from places where I won’t be able to sit down and rest.” [21]
Another patient reported:
‘‘You know hills and stairs; they’re the worst. And carrying things up the stairs is even worse.” [19]
Patients with CLI felt that their personal independence was compromised because of their problems with mobility. They felt the disease took away their ability to walk completely or reduced their walking ability. This meant for many of them limited daily activities such as housework, shopping and cleaning [17]. Many patients used aids such as walking sticks, walking frames and sometimes wheelchairs to overcome issues with mobility; these changes occurred over a long time to adjust to the symptoms [18].
Many patients with amputation secondary to PAD reported that problems with mobility had the biggest impact on their quality of life. The major issues with mobility included maintaining their balance, walking upstairs or up ramps. Most patients with amputations relied on using wheelchairs, even if they had prosthesis. Many also reported that they wished that they had met the prosthesis specialists prior to amputation, to prepare them for life after amputation [22].
Non-Healing Ulcers One of the most distressing symptoms experienced by patients with CLI was non-healing ulcers or wounds. Patients used terms like ‘painful’ and ‘disgusting’ to describe their ulcers. Many were concerned about the shape and colour of their leg; the shape of the ulcer had an impact on the type of clothes and shoes they could wear. Several patients also complained of recurrent leg ulcers as a result of PAD.
“It’s troublesome because it runs. That’s the hard thing and sometimes it hurts. It’s hard to wear shoes.” [17]
“Well, the district nurse came and looked at it and bandaged it. Then it was all right and then it came back, and then it was all right and then it came back again, so it is there now.” [17]
3.2.2 Sexual Functioning
Some patients described a decline in their sexual functioning as a result of PAD. Although only a minority of patients reported that this was important to their overall quality of life. The decline in sexual function was associated with progression of symptoms of the disease [22].
3.2.3 Symptom Progression
Participants in four studies understood that PAD is a chronic condition and that it can get worse [17, 18 20, 21] some reported that they are focusing on avoiding the progression of symptoms and worsening of PAD. Many patients’ post-intervention adopted new strategies to avoid further intervention by modifying their lifestyle and giving up causative agents such as smoking [18]. The perception of the amount of control participants had over their disease progression varied considerably across the studies. These perceptions ranged from having little or none, to having a great deal of control [20].
3.2.4 Impact on Physical Functioning
Participants in all the included studies described varying impacts on their ability to care for themselves independently [15,16,17,18,19,20,21,22], participate in exercise or perform their daily activities. The symptoms of pain and reduced mobility had the main impact on physical functioning. [22] Patients with severe lower limb ischaemia also suggested that their physical function was affected by a lack of sleep owing to their PAD symptoms, in addition to pain at rest or walking. [20].
3.2.5 Impact of Peripheral Arterial Disease on Social Functioning
Seven studies described the impact of PAD on social life. Many patients reported that their social life was compromised including not being able to maintain their personal role, lack of support from their social circle, isolation and the inability to perform their hobbies. Problems with isolation and lack of social support were worse among patients with amputations secondary to PAD; many of these patients felt that a social support group may improve their quality of life [22]. Patients with IC and CLI felt that their symptoms prevented them from keeping their hobbies, visiting family and friends, and taking part in many activities that they enjoyed [15,16,17,18,19,20,21].
3.2.6 Psychological Impact of Peripheral Arterial Disease
The papers reported that patients felt they had no control over their disease. This feeling was more common amongst patients who had undergone revascularisation but still had some residual symptoms, or those that developed complications [16]. Many patients had low self-esteem, and felt embarrassed because of their symptoms; for example, some participants described feeling embarrassed because they stopped frequently to ease the pain. Some reported making up excuses to stop, for example, pretending to be waiting for someone [19]. Patients also experienced issues of personal image and self-perception, with some patients feeling “old before their time” [19]. Patients also reported the emotional burden of PAD with many experiencing low mood and a sense of loss as a result of the disease or its complications [16,17,18,19,20,21]. Patients also reported symptoms of anxiety caused by fear of loss of independence, of amputation or of death [15,16,17,18, 20,21,22].
3.2.7 Financial Impact of Peripheral Arterial Disease
One study described the impact of the disease on participants’ employment, and their ability to carry out their tasks at work. Many participants in that study thought that these limitations may lead to job loss or the loss of an opportunity to be promoted. Some patients planned to change jobs because of their new symptoms [20].
3.2.8 Process of Care
All the studies reported that patients had limited understanding about the consequences of surgery. Patients with a diagnosis of IC and no intervention were not clear about their management, and did not understand why they were not offered interventions [15, 16]. Many patients did not view walking as therapy for their disease, and therefore avoided walking as they believed the claudication pain was a sign of damage caused to the leg by walking [16].
Many patients attempted to change their habits and devised strategies to manage their symptoms; this included alterations in walking by controlling pace, as well as planning stops for longer walks and taking pain relief [15, 16, 19]. However, side effects of pain relief medications were a cause for restricted use [17]. Some participants wished that their risk factors were modified earlier in the community including assistance to give up smoking [20].
Post-amputation, many participants felt that intolerable severe continuous ischaemic rest pain was the most appropriate threshold for amputation and saw no point in the revascularisation attempts at that stage. On patient said:
“Most people would try anything to save the leg.” [22]
“I definitely would have had the amputation at the same time point. My pain got so bad, I could not walk.” [22]
Patients with amputations also reported that meeting with the prosthetics specialists, and spending some time familiarising themselves with the rehabilitation services available, prior to the amputation would have helped their recovery [22].
Three main subthemes emerged in relation to shared decision making in this review; these were lack of knowledge, expectations and communication barriers. Several patients reported a lack of information about the disease and its progress [16]. Exercise therapy was recommended for some patients with claudication or post-operatively; however, patients did not understand the importance and relevance of this therapy, and some decided to do the opposite and avoid walking [15,16,17]. This was mainly because of communication barriers between clinicians and patients.
“When I was in the last time he (surgeon) was talking to a lady doctor and he said I was needing more but he started talking funny words that I did not understand.” [16]
“While I was told I had artery disease, I wasn’t told that I could lose my leg. I would have taken better care of myself.” [22]
However, sometimes this was because of a lack of engagement by the patients and handing control of the decision making to the clinicians.
“The likes of [surgeons], they know what they are talking about, they don’t say things unless they are sure so I accept what they want to do.” [15]
Patient expectation was also a significant issue. Some had no knowledge of the overall impact of the atherosclerosis on their health generally, and others expected the intervention to fully cure the disease. Although most patients reported satisfaction with their intervention, some were disappointed with the results post-operatively as they expected to return to their pre-disease state with no symptoms or disability [15, 16, 18, 22].
3.2.9 Triangulation
The identified themes were compared to items from validated PROMs that were identified in a recent study [8]. These PROMs include the Peripheral Artery Disease Quality of Life Questionnaire, Vascular Quality of Life Questionnaire (VascuQoL), Australian Vascular Quality of Life Index, Peripheral Artery Questionnaire, Intermittent Claudication Questionnaire, Walking Impairment Questionnaire, EuroQoL-5D-3L (EQ-5D-3L), Nottingham Health Profile and the Medical Outcomes Study 36-Item Short Form. Two reviewers examined the overlap between the themes in the qualitative review and items in the validated PROMs; when there was a complete overlap between the theme and an item in a PROM, an agreement score (+) was awarded; however, when the theme was covered in a general question, a partial agreement score was awarded (±). For instance, EQ-5D has a domain about pain, this domain overlaps completely [is in agreement (+)] with the pain theme; the same domain overlaps with themes such as pain on walking, rest pain, night pain and phantom pain; although this domain in EQ-5D-3L does not ask about them specifically. When the theme is not covered at all, a silence score (−) was awarded; for example, in EQ-5D-3L, there are no questions about sexual functioning or altered sensation.
The best generic PROMs that captured all the important issues for patients with PAD was the Nottingham Health Profile and the disease-specific PROMs and the best fit with the themes from the qualitative review was the VascuQoL. However, VascuQoL did not cover issues important to patients who had an amputation secondary to PAD. The Walking Impairment Questionnaire only covered important symptoms, whereas the Intermittent Claudication Questionnaire only covered some of the themes important to patients with IC. For further details on the results of triangulation, see Table 4.
4 Discussion
We identified 35 themes associated with quality of life for those with different forms of PAD. These themes were divided into six groups: symptoms, physical functioning, impact on social functioning, psychological impact, financial impact and process of care
Measuring quality of life for people with PAD including patients with IC, CLI and amputation is of interest currently because of the introduction of new treatment modalities such as drug-eluting stents and drug-coated balloon angioplasty, as well as emerging evidence from trials comparing bypass operation to endovascular therapies. Outcome measures, such as limb salvage, patient survival, patency of bypass or vascularised artery, and re-intervention rates, have been used to compare outcomes between therapies for patients with PAD, and to inform decision making for patients with PAD. However, quality of life and functional status are what matters the most to patients [23, 24].
One of the strengths of this study is that the qualitative review included studies of patients with different manifestations of PAD, as PAD can present with a spectrum of symptoms, and with varying severity. The inclusion in the review of patients with IC, CLI and amputation ensured the variation of impacts on quality of life was captured. This is important owing to the complexity of PAD presentation because patients could have IC or CLI or had an amputation in one leg and experience a different stage of the disease in the other leg. Validated PROMs in this field cover only a stage of the disease. A comprehensive measure can be used to examine the outcomes of patients at different stages of the disease.
This review incorporated evidence from a previous systematic review [8] also conducted by the same research team, which identified PROMs validated for use with patients with PAD. In the triangulation section of this study, the themes from this qualitative review were mapped against the domains from the validated generic and disease-specific PAD PROMs that were identified in the separate review.
The main limitations of this study are that some of the included papers in the qualitative review did not specify the severity of PAD in the patients included. In other studies, the investigators reported the severity but did not distinguish between the themes based on the type of PAD. Furthermore, there was only one study that reported on the quality of life of patients with PAD-related amputation.
The review identified the important symptoms from the patients’ perspective, these included pain, altered sensation, cold extremities, fatigue/weakness, issues of mobility, ulcers, sexual functioning and symptom progression. This study also revealed that patients with critical ischaemia and IC post-intervention complained of some of these symptoms in varying degree. Furthermore, many patients with critical ischaemia expressed their views that quality of life and severity of symptoms should be considered when deciding the timing and type of intervention, whether that is revascularisation or amputation.
Amongst some academic and clinical circles, quality of life has confusingly come to be known as anything that is not clinical [25]. However, this review indicates that, when patients with PAD are asked, the distress related to symptoms is integral to their quality of life, and in some instances seeing beyond the distress of pain and lack of mobility is difficult. The type of pain, its onset, as well as the location, was different depending on the severity of disease; the same applied to fatigue, weakness, altered sensation and mobility. Mobility issues were different between a patient post-amputation, and someone with claudication; however, the issue remained relevant to both groups.
Issues relating to the impact on psychological well-being included the following subthemes: lack of control over life, negative impact on self-esteem, self-perception, impact on mood, fear of amputation, loss of independence and death. The impact of these problems differed between patients depending on whether they experienced claudication symptoms only, if they had severe ischaemia or if they had undergone an amputation.
One of the strongest findings of this study is that when the themes generated from the review were mapped against the generic and disease-specific PROMs validated in patients with PAD, none of them covered all of the important issues revealed by the review. This is likely because the review included studies that interviewed patients with IC-, CLI- and PAD-related amputations; therefore, including all the themes important to patients with symptomatic PAD. This provides important evidence for critically examining the content of PROMs currently being used in patients with PAD and particularly the generic measures such as the EQ-5D-3L and the Medical Outcomes Study 36-Item Short Form.
Both PROMs are used commonly to inform resource allocation decisions as well as to monitor quality of life. There are several concerns with generic PROMS, for instance, the EQ-5D-3L and Medical Outcomes Study 36-Item Short Form were designed by experts with no input from patients with PAD and their coverage does not include all the important issues to patients with IC, CLI and amputation secondary to PAD. The EQ-5D-3L has five dimensions of health: mobility, self-care, usual activities, pain and discomfort, and depression and anxiety. Respondents are asked to report their level of problems (no problems, slight/moderate problems or severe/extreme problems) on each dimension to provide an overall score for the health state. A key concern raised about this measure is the focus on physical health with little focus on psychological well-being.
5 Conclusions
The findings of this study can help to provide useful evidence for examining the content validity of different measures. This evidence can be used alongside quantitative psychometric evidence to design a new disease-specific measure. Our group designed this instrument and aims to perform a factor analysis and well as a further psychometric analysis in a large survey of patients with PAD.
Data Availability
The analysis data cannot be shared because some of the papers included in the systematic review have copyrights and these prohibit publishing them in other journals but allow researchers to use them for secondary analysis. These papers were uploaded into the software in which we performed the analysis. Supplementary materials are included regarding the search strategy and analysis.
References
Fowkes FG, Housley E, Cawood EH, Macintyre CC, Ruckley CV, Prescott RJ. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol. 1991;20(2):384–92.
Kannel WB, Skinner JJ Jr, Schwartz MJ, Shurtleff D. Intermittent claudication: incidence in the Framingham Study. Circulation. 1970;41(5):875–83.
American Diabetes Association. Peripheral arterial disease in people with diabetes. Diabetes Care. 2003;26(12):3333–41.
Leng GC, Lee A, Fowkes FG, Whiteman M, Dunbar J, Housley E, et al. Incidence, natural history and cardiovascular events in symptomatic and asymptomatic peripheral arterial disease in the general population. Int J Epidemiol. 1996;25(6):1172–81.
Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006;113(11):e454–63.
Park KB, Do YS, Kim DI, Kim DK, Kim YW, Shin SW, et al. The TransAtlantic InterSociety Consensus (TASC) classification system in iliac arterial stent placement: long-term patency and clinical limitations. J Vasc Interv Radiol. 2007;18(2):193–201.
Department of Health. Liberating the NHS: transparency in outcomes: a framework for the NHS. 2010. http://www.bad.org.uk/shared/get-file.ashx?itemtype=document&id=1280. Accessed 8 Jun 2017.
Poku E, Duncan R, Keetharuth A, Essat M, Phillips P, Woods HB, Palfreyman S, Jones G, Kaltenthaler E, Michaels J. Patient-reported outcome measures in patients with peripheral arterial disease: a systematic review of psychometric properties. Health Qual Life Outcomes. 2016;14(1):161.
Duncan R, Booth A, Woods HB, Essat M, Phillips P, Poku, E, Kaltenthaler E, Jones G, Michaels J. Understanding the experience and impact of living with a vascular condition from the patients’ perspective: qualitative evidence synthesis protocol. HEDS discussion paper. 2016. https://www.sheffield.ac.uk/polopoly_fs/1.552397!/file/DP_16_05.pdf. Accessed 8 Jun 2017.
Critical Appraisal Skills Program. 10 questions to help you make sense of qualitative research: CASP qualitative check list. 2006;1–6. http://media.wix.com/ugd/dded87_951541699e9edc71ce66c9bac4734c69.pdf. Accessed 3 May 2018.
Carroll C, Booth A. Quality assessment of qualitative evidence for systematic review and synthesis: is it meaningful, and if so, how should it be performed? Res Synth Methods. 2015;6(2):149–54.
Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Bryman G, Burgess A, editors. Analysing qualitative data. London: Routledge; 1994. p. 173–94.
Farmer T, Robinson K, Elliott SJ, Eyles J. Developing and implementing a triangulation protocol for qualitative health research. Qual Health Res. 2006;16:377–94.
O’Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ. 2010;341:c4587.
Gibson JM, Kenrick M. Pain and powerlessness: the experience of living with peripheral vascular disease. J Adv Nurs. 1998;27:737–45.
Cunningham M, Swanson V, Pappas E, O’Carroll R, Holdsworth RJ. Illness beliefs and walking behaviour after revascularisation for intermittent claudication: a qualitative study. J Cardiopulm Rehabil Prev. 2014;34(3):195–201.
Wann-Hansson C, Hallberg IR, Klevsgard R, Andersson E. Patients’ experiences of living with peripheral arterial disease awaiting intervention: a qualitative study. Int J Nurs Stud. 2005;42:851–62.
Wann-Hansson C, Hallberg IR, Klevsgard R, Andersson E. The long-term experience of living with peripheral arterial disease and the recovery following revascularisation: a qualitative study. Int J Nurs Stud. 2008;45:552–61.
Egberg L, Andreassen S, Mattiasson AC. Experiences of living with intermittent claudication. J Vasc Nurs. 2012;30(1):5–10.
Treat-Jacobson D, Halverson SL, Ratchford A, Regensteiner JG, Lindquist R, Hirsch AT. A patient-derived perspective of health-related quality of life with peripheral arterial disease. J Nurs Scholarsh. 2002;34(1):55–60.
Schorr EN, Peden-McAlpine C, Treat-Jacobson D, Lindquist R. Characterization of the peripheral artery disease symptom experience. Geriatr Nurs. 2015;36(4):293–300.
Suckow BD, Goodney PP, Nolan BW, Veeraswamy RK, Gallagher P, Cronenwett JL, Kraiss LW. Domains that determine quality of life in vascular amputees. Ann Vasc Surg. 2015;29(4):722–30.
Abou-Zamzam AM, Lee RW, Moneta GL, et al. Functional outcome after infrainguinal bypass for limb salvage. J Vasc Surg. 1997;25:287–97.
Gulati S, Coughlin PA, Hatfield J, et al. Quality of life in patients with lower limb ischemia; revised suggestions for analysis. J Vasc Surg. 2009;49:122–6.
Bowling A. Measuring health: a review of quality of life measurement scales. Buckingham: Open University Press; 1997.
Author information
Authors and Affiliations
Contributions
Ahmed Aber contributed to the analysis and interpretation of data, drafting of the manuscript and critical revision; Elizabeth Lumley contributed to the analysis and interpretation of data and drafting of the manuscript; Patrick Philips contributed to reviewing the data as well as the analysis and drafting of the manuscript; Helen Buckley Woods performed the searches for the systematic review and assisted in drafting of the manuscript; Georgina Jones contributed to the study conception and design, analysis and interpretation of data, and drafting of the manuscript; and Jonathan Michaels contributed to the study conception and design, drafting of the manuscript and critical revision.
Corresponding author
Ethics declarations
Funding
This study was funded by the UK National Institute for Health Research under the Programme Grants for Applied Research Programme (RP-PG-1210-12009). The views expressed are those of the authors and not necessarily those of the National Health Service, the National Institute for Health Research or the Department of Health.
Conflict of interest
Ahmed Aber, Elizabeth Lumley, Patrick Phillips, Helen Buckley Woods, Georgina Jones and Jonathan Michaels have no conflicts of interest directly relevant to the content of this article.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Aber, A., Lumley, E., Phillips, P. et al. Themes that Determine Quality of Life in Patients with Peripheral Arterial Disease: A Systematic Review. Patient 11, 489–502 (2018). https://doi.org/10.1007/s40271-018-0307-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-018-0307-7