
Abstract
Background
Childhood acute respiratory infections (ARIs) are one of the most common reasons for primary care consultations and for receiving an antibiotic. Public awareness of antibiotic benefit and harms for these conditions is low. To facilitate informed decision making, ideally in collaboration with their doctor, parents need clear communication about benefits and harms. Decision aids may be able to facilitate this process.
Objective
The aim of this study was to evaluate the effectiveness of three decision aids about antibiotic use for common ARIs in children.
Methods
Adult parents of children aged 1–16 years (n = 120) were recruited from community settings and then randomised using a computer-generated randomisation sequence to receive a decision aid (n = 60) or fact sheet (n = 60). Allocation was concealed and used sealed and opaque sequentially numbered envelopes. Participants self-completed questionnaires at baseline and immediately post-intervention. The primary outcome was informed choice (conceptual and numerical knowledge; attitudes towards, and intention to use, antibiotics for a future ARI). Secondary outcomes were decisional conflict, decisional self-efficacy, and material acceptability.
Results
After reading the information, significantly more intervention group participants made an informed choice [57%] compared with control group participants [29%] [difference 28, 95% confidence interval (CI) 11–45%, p < 0.01], and had higher total knowledge [mean difference (MD) 2.8, 95% CI 2.2–3.5, p < 0.01], conceptual knowledge (MD 0.7, 95% CI 0.4–1.1, p < 0.01) and numerical knowledge (MD 2.1, 95% CI 1.6–2.5, p < 0.01). Between-group differences in attitudes or intention to use antibiotics were not significant. Most intervention group participants found the information understandable and liked the aids’ format and features.
Conclusion
The decision aids prepared parents to make an informed choice about antibiotic use more than fact sheets, in a hypothetical situation. Their effect within a consultation needs to be evaluated.
Clinical Trials Registration Number: ACTRN12615000843550.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
There is a trade-off between antibiotic benefits and harms for acute respiratory infections (ARIs) in children. To make informed decisions, parents need to understand these trade-offs. |
Decision aids can be used to help communicate evidence about antibiotic benefits and harms. |
In this randomised trial, decision aids improved parents’ knowledge and informed choice about antibiotic use for ARIs in a hypothetical situation. Effects of the decision aids in a consultation should be evaluated next. |
1 Introduction
Acute respiratory infections (ARIs) in children are one of the most common reasons for primary care consultations [1–5]. Antibiotic prescribing rates for common childhood ARIs remain excessive [2, 3, 5, 6], even after the dissemination of evidence that antibiotics typically have minimal benefit in reducing symptoms or complications [7–9], and that small benefits may be outweighed by harms. These include common and relatively minor harms, such as diarrhoea [10], but also the risk of contributing to antibiotic resistance [11]. Antibiotic resistance, now a global public health crisis, is directly caused by antibiotic use [12]. Reducing antibiotic use for ARIs in primary care is a priority because this use is the most common and least necessary of uses of antibiotics [12, 13].
Several factors influence whether antibiotics are prescribed in this setting. Children are perceived by doctors and parents to be more vulnerable than adults to the risk of harm from ARIs [14]. Diagnostic uncertainty is coupled with concern that the disease might progress, and many doctors perceive that patients/parents expect an antibiotic [15]. Patients generally overestimate the benefits of treatments and underestimate their harms [16]. This also applies to beliefs about antibiotics, with many parents overestimating antibiotic benefits and underestimating their harms [17, 18]. This can be a contributor to some patients believing that antibiotics are a necessary treatment for ARIs and explicitly requesting them [19]. Antibiotic prescribing reinforces expectations of antibiotics for future ARIs [20, 21].
The counterpoise between antibiotic benefits and harms suggests a need for preference-sensitive care. Shared decision making is a way to provide this [22], with its focus on communication and evidence-based practice skills, and steps that include eliciting patients’ expectations and preferences, clarifying misperceptions, and discussing evidence for the benefits and harms of each option [23]. Patient decision aids are one of several types of tools that can be used to support shared decision making. They can improve patients’ knowledge about treatment options, accuracy of perceptions about the benefits and harms of each option, active participation in decision making, and clinician–patient communication [24].
In a Cochrane review [25], we recently showed that interventions that aimed to facilitate shared decision making significantly reduced antibiotic prescribing for ARIs in primary care in the short-term, without an increase in reconsultations for the same illness episode or a decrease in patient satisfaction; however, the scope, extensive training requirements, and accessibility of most of these interventions are prohibitive to widespread and sustainable implementation. Some studies used written patient materials as a component of multifaceted interventions, but only two studies (one pilot [26], one main trial [27]) incorporated the use of a decision aid. The decision aid combined all ARIs into a single aid, was predominately aimed at clinicians (as it included diagnostic probabilities to assist with managing clinical uncertainty), and its acceptability to patients has not been evaluated. Further analysis of the main trial found no significant intervention effect on patients’ intention to engage in shared decision making for antibiotic use in future occurrences of ARIs, and concluded that patient-targeted interventions may be necessary to achieve this aim [28].
Despite the prevalence of antibiotic prescribing for common childhood ARIs in primary care, as well as the need for parents to be adequately informed prior to making preference-sensitive decisions in collaboration with their doctor about antibiotic use, there is a lack of existing brief decision support tools whose acceptability has been evaluated with parents. With the eventual goal of facilitating shared decision making about antibiotic use in ARI consultations, we developed three brief decision aids for parents relating to acute otitis media, acute pharyngitis (sore throat), and acute bronchitis in children. This study is one stage of a multi-stage evaluation, as is recommended in the development of decision aids [29]. The aim of the present study was to evaluate the ability of the decision aids to help parents make an informed choice in a hypothetical scenario, and parents’ perceptions of the usefulness and acceptability of the decision aids.
2 Methods
2.1 Study Design
This was a two-arm, parallel group, randomised trial.
2.2 Participants
A convenience sample of eligible parents was recruited between September and December 2015 from several community locations, such as playgroups in South-East Queensland, Australia. Adult (≥18 years) parents or primary caregivers of children aged 1–16 years (inclusive) were invited to participate. Children were not required to be experiencing an ARI at that time for parents to be eligible to participate. Eligible parents who were interested in participating were provided with a participant information sheet prior to being invited to provide voluntary written consent. The trial was approved by the Bond University Human Research Ethics Committee and was registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12615000843550).
2.3 Randomisation and Blinding
Eligible participants were randomly assigned to one of two information formats: one of the new decision aids (intervention) or a fact sheet (control), for one of three common childhood ARIs (acute otitis media, sore throat, and acute bronchitis). The randomisation sequence was computer-generated (www.randomization.com) by a researcher independent of the project team, who placed and sealed the allocated information format and corresponding pre- and post-questionnaire into sequentially numbered opaque envelopes. Group allocation was concealed to both participants and interviewers until written consent had been obtained.
2.4 Procedure
The consenting parent and study researcher signed and dated a consent form attached to the envelope. The researcher opened the envelope and asked the participant to self-complete the pretest questionnaire to assess baseline knowledge and attitudes about antibiotic use for the ARI covered in the information allocated to them, and the intention of using antibiotics when their child had a similar future illness. The researcher returned the completed questionnaire to the envelope, and then provided the participant with either the intervention or control information (for one of the three infections) that they had been randomised to. Participants could read the information at their own pace. The researcher unobtrusively recorded the time this took. After returning the intervention or control information to the envelope, the participant immediately completed the post-test questionnaire. This contained antibiotic knowledge, attitude, and intention questions identical to those in the baseline questionnaire, as well as questions about confidence in making a decision and any discomfort with the decision reached. A copy of the pre- and post-questions for acute otitis media are provided as an example in Online Resource 1. The interaction between the researcher and participant was standardised, and the written materials were provided to both groups in a neutral manner and with minimal interaction beyond conveying procedural instructions. Researchers did not provide participants with any additional information, or counsel them about ARIs or antibiotic use.
2.5 Intervention
The patient decision aids were systematically developed in accord with the updated review of the International Patient Decision Aids Standards (IPDAS) international quality criteria and development processes [29]. The content of each decision aid was informed by (i) findings from systematic reviews [15, 30] and observational studies [14, 17, 18, 31–33] exploring patients’ and parents’ beliefs about, and expectations of, antibiotics for ARIs; (ii) the relevant Cochrane systematic reviews (acute otitis media [7], acute bronchitis [8], sore throat [9]), and a meta-analysis of antibiotic harms [10] for quantification of antibiotic benefits and harms; and (iii) risk communication research about optimal methods for numerical, graphical and narrative presentation of benefit and harm data [34, 35].
The decision aids were evaluated for face and content validity with an advisory group of clinicians and researchers with clinical and research expertise in general practice, ARIs, infectious diseases, evidence-based practice and shared decision making. The decision aids were developed iteratively, and were reviewed and revised during pilot testing with a purposeful sample of eligible parents (n = 12) and general practitioners (n = 6). Figure 1 shows the front page of the two-page A4 decision aid for acute otitis media.

Front page of the A4-page decision aid for acute otitis media
2.6 Control
The fact sheets provided to the control group contained information currently available, for each ARI, to the Australian public from NPS MedicineWise, an independent, not-for-profit organisation who, as part of their activities, provide health information resources. Their website contained a downloadable fact sheet for acute otitis media and antibiotics in children [36]. For sore throat [37] and acute bronchitis [38], the consumer information on the website was not formatted for easy download or printing, therefore we converted it into a format that matched the acute otitis media fact sheet.
2.7 Outcomes
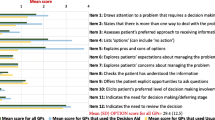
Our primary outcome was a composite measure of informed choice. This is based on the multidimensional model of informed choice [39], which has been previously used in trials of decision aids [40, 41], and contains constructs of decision quality that are often used when evaluating decision aids [42]. It consists of three constructs: knowledge, attitudes, and intentions. A participant’s choice was considered to be informed if his/her level of knowledge was adequate, and their attitudes and intention consistent [40] (i.e. positive attitude to antibiotic use and high intention to use; or negative attitude to antibiotic use and low intention to use). There were ten knowledge questions (see Table 2)—five assessing conceptual knowledge questions about antibiotic use for the relevant ARI (true/false), and five assessing numerical knowledge about the quantitative benefits and harms of antibiotic use (open-ended responses). A score of ≥50% (with at least two correct numerical items) was set as the threshold for adequate knowledge [43]. Attitude to antibiotic use was measured using a validated 6-item scale [40, 41, 44], with five response options (‘strongly disagree’ to ‘strongly agree’), forming a scale from 6 to 30. The threshold for a positive attitude (to antibiotic use) was set at 24, based on previous work [40]. A single question with five response options (‘definitely will not’ to ‘definitely will’) was used to assess the intention to use an antibiotic for a child’s ARI in the future. Secondary outcomes were decisional conflict (10-item low-literacy decisional conflict scale) [45]; self-efficacy in decision making (four items from the decision self-efficacy scale) [46]; and usability and acceptability of the decision aids [40].
2.8 Sample Size Calculation
Using an alpha of 0.05 and 90% power to detect a difference of 30% (based on data from previous studies [47, 48]) in the proportion of people who made an informed choice, we estimated a minimum of 104 people would be required. This was rounded to 108 to enable equal group sizes.
2.9 Statistical Analysis
Quantitative data were entered into Stata version 13 (StataCorp LP, College Station, TX, USA). Responses to numerical knowledge questions were considered correct if a participant’s answer was within ±10 of the actual estimate. For example, in the acute otitis media question about the number of children out of 100 who will get better without antibiotics, in which the answer was 84, any response in the range of 74–94 was marked as correct. When analysing responses to the intention question, the ‘likely to’ and ‘definitely will’ response categories were collapsed to indicate a positive intention, and ‘definitely will not’ and ‘not likely to’ were collapsed to indicate a negative intention.
The primary analysis was a comparison of the proportion of participants in the intervention and control groups who were making an informed choice. Continuous outcomes were analysed using independent sample t tests, and categorical and binary outcomes were analysed using Chi square tests. Adjustment for differences between the groups in the baseline intention-to-use measure was performed using ordinal logistic regression for the between-group analysis for post-intervention responses to this question. Data from open-ended questions about the acceptability of the aids were categorised independently by two authors for thematic analysis.
3 Results
During the recruitment phase (September–December 2015), 141 eligible participants were invited to participate, 120 were recruited and none were lost to follow-up (Fig. 2). Most participants were Australian-born, female, between 36 and 45 years of age, married or living with a partner, had completed tertiary education, and were employed full-time. Baseline characteristics for the two groups were similar for all characteristics except education, in which a higher proportion of participants in the intervention group had a higher level of educational attainment (Table 1). Although the groups did not differ on baseline knowledge scores (conceptual, numerical or combined) (Table 2), we conducted a post hoc analysis using logistic regression to adjust for level of educational attainment, and found it was not statistically significant and did not lead to any substantial change in the primary outcome.

Flow of participants through the trial
Baseline knowledge level was moderate in both groups (Table 2). The intervention group’s mean conceptual knowledge score (maximum possible score of 5) was 3.0, while the control group’s score was 3.1. Numerical knowledge scores (out of 5) were lower, with a mean of 1.5 in both groups. Baseline attitude towards antibiotic use was positive in 18% of participants in the intervention group and 19% of participants in the control group, while a greater proportion of intervention group participants (42%) had a positive intention to future antibiotic use than in the control group (32%). At baseline, the proportion of participants who made an informed choice about antibiotic use was low and similar between the intervention (15%) and control (18%) groups.
After the materials had been read, more participants in the intervention group [28% more, 95% confidence interval (CI) 11–45%, p < 0.01] than in the control group made an informed choice about antibiotic use for a child’s future ARI. Individual constructs of this composite outcome also reflect this (Table 2). Intervention group participants also had higher scores for total knowledge [mean difference (MD) 2.8, 95% CI 2.2–3.5, p < 0.01], conceptual knowledge (MD 0.7, 95% CI 0.4–1.1, p < 0.01) and numerical knowledge (MD 2.1, 95% CI 1.6–2.5, p < 0.01). More participants in the intervention group had adequate knowledge than in the control group (48% more, 95% CI 33–63%; p < 0.01).
At post-intervention, there were no significant differences between the number of participants in each group who had a positive attitude towards antibiotic use. After adjustment for the baseline difference between groups in the proportion of participants with a positive intention to antibiotic use, the intervention group participants were more likely to have a positive intention than those in the control group, but the difference was not statistically significant (odds ratio 0.43, 95% CI 0.18–1.09, p = 0.08). Decisional conflict scores were low, and self-efficacy for making the decision was high, in both groups, with no significant between-group differences (Table 2).
Table 3 summarises participants’ views about the intervention and control materials. The majority of participants thought the length of materials was just right, although significantly more in the intervention group (90%) compared with the control group (60%) [95% CI 15–45%, p < 0.01]. The time in minutes taken to read the information was similar in both groups, with a mean (SD) of 4.3 (1.4) in the intervention group and 4.7 (2.2) in the control group. There were no significant differences between the groups in the proportion of participants who thought the information was new, clear and easy to understand, and helpful in deciding about antibiotic use for a child’s illness. Significantly more participants who received a decision aid (95%) than control information (76%) agreed or strongly agreed they would recommend the information to other parents deciding about antibiotic use for a child with an ARI (19% difference, 95% CI 7–31%, p < 0.01).
More participants who received decision aids provided a response to the open question “What did you like about the information sheet?”. Frequent responses included the format, structure and content; that the information was concise, clear, and easy to read and/or understand; and the graphical representation of benefits and harms numerical information. A few participants (n = 5) also indicated that they liked the neutral presentation of information. In response to the question “How could the decision aids be improved?” a few suggestions included adding information on viral versus bacterial aetiology (n = 1), the role of antibiotics in preventing complications (n = 1), types of antibiotics (n = 1), and other treatment options (n = 2).
4 Discussion
We developed and evaluated the effect of decision aids on parents’ ability to construct informed preferences and make informed choices about antibiotic use in three common childhood ARIs in the context of a hypothetical decision, as a precursor to evaluating their effect on facilitating shared decision making during a clinical consultation. This trial found that the decision aids enabled more parents to make an informed choice about antibiotic use in this type of hypothetical situation and improved parents’ knowledge, but did not alter their attitudes towards antibiotic use or their intention to use antibiotics when their child has an ARI in the future.
The findings that the decision aids substantially improved conceptual and numerical knowledge are consistent with systematic review findings on the effects of decision aids on knowledge and risk perception accuracy for other treatment decisions [24]. The substantial improvement in numerical knowledge in the intervention group is not surprising as the information was only provided in the decision aids. The importance of improving this type of knowledge comes from studies showing that patients typically overestimate the benefits and underestimate the harms of treatments [16], including for antibiotics in ARIs [17, 18]. These overly optimistic expectations contribute to unnecessary treatment [16]. Shared decision making provides the opportunity to redress this [23], with clinicians and patients able to discuss the likelihood of benefit and harm, and the trade-off between the two. It is unclear to what extent individuals, when deciding about antibiotic use, weigh more proximal individual perceptions about antibiotic benefit and harm, against the more distal individual or community consequences of antibiotic resistance (the ‘tragedy of the commons’ [49]). Measurement of parents’ risk perceptions about the benefits and harms of antibiotics is another contribution of this study to the literature. As far as we are aware [16], no other studies have quantified people’s expectations about antibiotic benefits and harms, and for their use in any condition. Our baseline knowledge scores provide this information and reveal that parents generally have inaccurate risk perceptions about antibiotic benefits and harms. Inaccurately high expectations of antibiotic benefits in ARIs have been reported in primary care paediatricians and have been identified as a driver of inappropriately high prescribing rates [50]; understanding the contribution that patients/parents also bring to the consultation is important when exploring the issues surrounding antibiotic decision making.
After reading the materials, there was reduction in the proportion of parents who had a positive attitude to antibiotic use in both groups, although the difference between the groups was not significant. The intervention and control materials took different approaches to trying to influence parents’ attitudes about antibiotics; the fact sheets explicitly stated that antibiotics were unnecessary and the decision aids presented the benefits and harms in a balanced manner (which is a criterion for the presentation of information in a decision aid [51]). The proportion of parents who intended to use antibiotics in the future also decreased in both groups but did not differ between the groups. As decisions about antibiotic use typically occur in the context of a consultation with a doctor, it is not possible to know from this study, which used a hypothetical situation, what effect the decision aids may have on parents’ attitudes and actual antibiotic use when their child is ill. It may be that both authoritatively presented information, which directs parents not to take antibiotics, and information that presents the benefits and harms, and encourages parents to be involved in making the decision, may alter attitudes and behaviour. However, when it comes to health decisions, the majority of participants prefer to be involved in decision making [52–54]. For decisions about antibiotics for children, most parents (75%) prefer to participate in making this decision with their doctor [18].
The findings that decisional conflict was low in both groups and below the threshold (of 25) associated with an ability to implement decisions [45], and that decisional self-efficacy was high in both groups, also need to be interpreted cautiously. These scores might not reflect the actual decisional self-efficacy and decisional conflict that occurs when parents have a child ill with an ARI and have consulted a doctor about their child’s care. However, low decisional conflict may also reflect that ARIs are familiar to parents, occur frequently, are not perceived as serious, and hence the decision making associated with them is not likely to produce high levels of decisional conflict. In a review of decisional conflict in shared decision-making situations in Canadian primary care (including decision making about antibiotics for ARIs), a ‘clinically significant’ level of decisional conflict was found in a low proportion (10–31%) of encounters [55].
Development of the decision aids followed the recommended phased approach [29], and during development they were iteratively tested with patients and general practitioners, with feedback about the layout and wording incorporated into the version tested in the current study. Acceptability and usefulness of the decision aids was confirmed in this study, with most intervention group participants reporting them to be easy to read and understand, useful, and liking the length and visual presentation of probability data. Evaluation of the decision aids when they are used in a consultation with general practitioners and their effect on antibiotic use, as well as the quality of the decision making during consultations, will be the next phase. Whether using decision aids will alter antibiotic prescribing rates is unclear.
Strengths of our trial include the systematic development of the decision aids, randomised design, and no loss to follow-up. We prespecified a conservative threshold for the type of knowledge required to make an informed choice, using conceptual and numerical measurement, underpinned by a theoretical framework [43]. We also directly compared decision aids with consumer information of high standard (considerably greater than is routinely provided in primary care in Australia), which may have underestimated the effectiveness of the decision aids when used within a clinical context.
Limitations in the generalisability of results stem from asking parents about a hypothetical illness situation. Although this is somewhat mitigated by the high prevalence of ARIs during childhood [56] (ARIs are the most frequent reason for children to be seen by a primary care doctor), so few parents in this study will have not experienced their child having had at least one of these illnesses at least once. Nevertheless, the hypothetical scenario may have influenced measurement of some constructs of the composite informed choice endpoint, although this outcome has been used in other trials of decision aids in which participants were not necessarily needing to make a decision at the time of receiving a decision aid but perhaps at some point in the future (such as cancer screening decisions) [40, 57, 58]. Knowledge and risk perception is unlikely to be affected by the hypothetical scenario, whereas parents’ attitudes toward antibiotic use, intent to use an antibiotic, and level of decisional conflict might differ when their child is sick and there is a need to make and act on a decision. These constructs might also be influenced by the interaction with a doctor in a consultation (where the decision aids are ultimately intended for use). Parents’ judgement of the usability and acceptability of the materials is unlikely to be affected by the hypothetical setting. The high educational attainment of the participants in both study groups may limit generalisability. A further limitation is that recall accuracy (particularly of risk probability questions) may have been aided by administration of the post-test questionnaire immediately after reading the allocated information, although this would not be particularly different from how the aids would be used during primary care consultations, and is a common approach in trials of decision aids [24].
5 Conclusions
Brief decision aids about antibiotic use for common ARIs in children enabled more parents to make an informed choice about this decision in a hypothetical situation. However, substantial improvements in knowledge about the benefits and harms of antibiotics may not be sufficient to change parents’ attitudes about antibiotics or their intention to use them for a child with an ARI. Parents liked the format and structure of the decision aids, balanced content, and visual presentation of benefit and harm data. Evaluation of the effectiveness of the decision aids on antibiotic prescribing in primary care is required. Decision aids are intended for use as a tool to facilitate shared decision making between the doctor and patient during a clinical encounter, and their effectiveness in this clinical context needs to be established next.
References
Biezen R, Pollack AJ, Harrison C, Brijnath B, Grando D, Britt HC, et al. Respiratory tract infections among children younger than 5 years: current management in Australian general practice. Med J Aust. 2015;202(5):262–5.
Hersh AL, Shapiro DJ, Pavia AT, Shah SS. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics. 2011;128(6):1053–61.
Meropol SB, Chen Z, Metlay JP. Reduced antibiotic prescribing for acute respiratory infections in adults and children. Br J Gen Pract. 2009;59(567):e321–8.
Grijalva CG, Nuorti JP, Griffin MR. Antibiotic prescription rates for acute respiratory tract infections in US ambulatory settings. JAMA. 2009;302(7):758–66.
Rossignoli A, Clavenna A, Bonati M. Antibiotic prescription and prevalence rate in the outpatient paediatric population: analysis of surveys published during 2000–2005. Eur J Clin Pharmacol. 2007;63(12):1099–106.
Coco AS, Horst MA, Gambler AS. Trends in broad-spectrum antibiotic prescribing for children with acute otitis media in the United States, 1998–2004. BMC Pediatr. 2009;9:41.
Venekamp RP, Sanders SL, Glasziou PP, Del Mar CB, Rovers MM. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2015;(6):CD000219. doi:10.1002/14651858.CD000219.pub4.
Smith SM, Fahey T, Smucny J, Becker LA. Antibiotics for acute bronchitis. Cochrane Database Syst Rev. 2014;(3):CD000245. doi:10.1002/14651858.CD000245.pub3.
Spinks A, Glasziou PP, Del Mar CB. Antibiotics for sore throat. Cochrane Database Syst Rev. 2013;(11):CD000023. doi:10.1002/14651858.CD000023.pub4.
Gillies M, Ranakusuma A, Hoffmann T, Thorning S, McGuire T, Glasziou P, et al. Common harms from amoxicillin: a systematic review and meta-analysis of randomized placebo-controlled trials for any indication. Can Med Assoc J. 2015;187(1):E21–31.
Chung A, Perera R, Brueggemann AB, Elamin AE, Harnden A, Mayon-White R, et al. Effect of antibiotic prescribing on antibiotic resistance in individual children in primary care: prospective cohort study. Br Med J. 2007;335(7617):429.
World Health Organization. The evolving threat of antimicrobial resistance: options for action. 2012. http://whqlibdoc.who.int/publications/2012/9789241503181_eng.pdf. Accessed 11 Jan 2015.
Center for Disease Dynamics, Economics & Policy. The state of the world’s antibiotics, 2015. Washington, DC: Center for Disease Dynamics, Economics & Policy; 2015.
Cabral C, Lucas PJ, Ingram J, Hay AD, Horwood J. “It’s safer to…” parent consulting and clinician antibiotic prescribing decisions for children with respiratory tract infections: an analysis across four qualitative studies. Soc Sci Med. 2015;136–137:156–64.
Lucas PJ, Cabral C, Hay AD, Horwood J. A systematic review of parent and clinician views and perceptions that influence prescribing decisions in relation to acute childhood infections in primary care. Scand J Prim Health Care. 2015;33(1):11–20.
Hoffmann TC, Del Mar C. Patients’ expectations of the benefits and harms of treatments, screening, and tests: a systematic review. JAMA Int Med. 2015;175(2):274–86.
McNulty CA, Nichols T, French DP, Joshi P, Butler CC. Expectations for consultations and antibiotics for respiratory tract infection in primary care: the RTI clinical iceberg. Br J Gen Pract. 2013;63(612):e429–36.
Coxeter P, Del Mar C, Hoffmann T. Parents' expectations and experiences of antibiotics for acute respiratory infections in primary care. Ann Fam Med. 2017;15(2). doi:10.1370/afm.2040.
Scott JG, Cohen D, DiCicco-Bloom B, Orzano AJ, Jaen CR, Crabtree BF. Antibiotic use in acute respiratory infections and the ways patients pressure physicians for a prescription. J Fam Pract. 2001;50(10):853–8.
Butler CC, Rollnick S, Kinnersley P, Jones A, Stott N. Reducing antibiotics for respiratory tract symptoms in primary care: consolidating ‘why’ and considering ‘how’. Br J Gen Pract. 1998;48(437):1865–70.
Little P, Gould C, Williamson I, Warner G, Gantley M, Kinmonth AL. Reattendance and complications in a randomised trial of prescribing strategies for sore throat: the medicalising effect of prescribing antibiotics. Br Med J. 1997;315(7104):350–2.
Butler CC, Kinnersley P, Prout H, Rollnick S, Edwards A, Elwyn G. Antibiotics and shared decision-making in primary care. J Antimicrob Chemother. 2001;48(3):435–40.
Hoffmann TC, Montori VM, Del Mar C. The connection between evidence-based medicine and shared decision making. JAMA. 2014;312(13):1295–6.
Stacey D, Legare F, Col NF, Bennett CL, Barry MJ, Eden KB, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;(1):CD001431. doi:10.1002/14651858.CD001431.pub4.
Coxeter P, Del Mar CB, McGregor L, Beller EM, Hoffmann TC. Interventions to facilitate shared decision making to address antibiotic use for acute respiratory infections in primary care. Cochrane Database Syst Rev. 2015;(11):CD010907. doi:10.1002/14651858.CD010907.pub2.
Legare F, Labrecque M, LeBlanc A, Njoya M, Laurier C, Cote L, et al. Training family physicians in shared decision making for the use of antibiotics for acute respiratory infections: a pilot clustered randomized controlled trial. Health Expect. 2011;14:96–110.
Legare F, Labrecque M, Cauchon M, Castel J, Turcotte S, Grimshaw J. Training family physicians in shared decision-making to reduce the overuse of antibiotics in acute respiratory infections: a cluster randomized trial. Can Med Assoc J. 2012;184(13):E726–34.
Couet N, Labrecque M, Robitaille H, Turcotte S, Legare F. The impact of DECISION+2 on patient intention to engage in shared decision making: secondary analysis of a multicentre clustered randomized trial. Health Expect. 2015;18(6):2629–37.
Coulter A, Stilwell D, Kryworuchko J, Mullen PD, Ng CJ, van der Weijden T. A systematic development process for patient decision aids. BMC Med Inform Decis. 2013;13(Suppl 2):S2.
Cabral C, Horwood J, Hay AD, Lucas PJ. How communication affects prescription decisions in consultations for acute illness in children: a systematic review and meta-ethnography. BMC Fam Pract. 2014;15:63.
Hansen MP, Howlett J, Del Mar C, Hoffmann TC. Parents’ beliefs and knowledge about the management of acute otitis media: a qualitative study. BMC Fam Pract. 2015;16:82.
Cabral C, Ingram J, Hay AD, Horwood J. “They just say everything’s a virus”: parent’s judgment of the credibility of clinician communication in primary care consultations for respiratory tract infections in children: a qualitative study. Patient Educ Couns. 2014;95(2):248–53.
Salazar ML, English TM, Eiland LS. Caregivers’ baseline understanding and expectations of antibiotic use for their children. Clin Pediatr. 2012;51(7):632–7.
Trevena LJ, Zikmund-Fisher BJ, Edwards A, Gaissmaier W, Galesic M, Han PK, et al. Presenting quantitative information about decision outcomes: a risk communication primer for patient decision aid developers. BMC Med Inform Decis. 2013;13(Suppl 2):S7.
Carling CL, Kristoffersen DT, Flottorp S, Fretheim A, Oxman AD, Schunemann HJ, et al. The effect of alternative graphical displays used to present the benefits of antibiotics for sore throat on decisions about whether to seek treatment: a randomized trial. PLoS Med. 2009;6(8):e1000140.
NPS MedicineWise. My child has a middle ear infeciton: is an antibiotic necessary? 2015. http://www.nps.org.au/__data/assets/pdf_file/0006/72159/My-child-has-a-middle-ear-infection-is-an-antibiotic-necessary.pdf. Accessed 15 Jun 2015.
NPS MedicineWise. Sore throat. 2015. http://www.nps.org.au/conditions/ear-nose-mouth-and-throat-disorders/ear-nose-and-throat-infections/sore-throat. Accessed 15 Jun 2015.
NPS MedicineWise. Bronchitis. 2015. http://www.nps.org.au/conditions/respiratory-problems/respiratory-tract-infections/for-individuals/conditions/bronchitis. Accessed 15 Jun 2015.
Marteau TM, Dormandy E, Michie S. A measure of informed choice. Health Expect. 2001;4(2):99–108.
Hersch J, Barratt A, Jansen J, Irwig L, McGeechan K, Jacklyn G, et al. Use of a decision aid including information on overdetection to support informed choice about breast cancer screening: a randomised controlled trial. Lancet. 2015;385(9978):1642–52.
Smith SK, Trevena L, Simpson JM, Barratt A, Nutbeam D, McCaffery KJ. A decision aid to support informed choices about bowel cancer screening among adults with low education: randomised controlled trial. Br Med J. 2010;341:c5370.
Sepucha KR, Borkhoff CM, Lally J, Levin CA, Matlock DD, Ng CJ, et al. Establishing the effectiveness of patient decision aids: key constructs and measurement instruments. BMC Med Inform Decis. 2013;13(Suppl 2):S12.
Smith SK, Barratt A, Trevena L, Simpson JM, Jansen J, McCaffery KJ. A theoretical framework for measuring knowledge in screening decision aid trials. Patient Educ Couns. 2012;89(2):330–6.
Dormandy E, Michie S, Hooper R, Marteau TM. Informed choice in antenatal Down syndrome screening: a cluster-randomised trial of combined versus separate visit testing. Patient Educ Couns. 2006;61(1):56–64.
O’Connor AM. User Manual—Decisional Conflict Scale (10 item question format). Ottawa, ON: Ottawa Hospital Research Institute, 1993 (updated 2010). 2010. https://decisionaid.ohri.ca/docs/develop/User_Manuals/UM_Decisional_Conflict.pdf. Accessed 5 May 2015.
O’Connor AM. User Manual—Decision Self-Efficacy Scale. Ottawa, ON: Ottawa Hospital Research Institute, 1995 (updated 2002). 2015. https://decisionaid.ohri.ca/docs/develop/user_manuals/UM_decision_selfefficacy.pdf. Accessed 5 May 2015.
Santesso N, Rader T, Nilsen ES, Glenton C, Rosenbaum S, Ciapponi A, et al. A summary to communicate evidence from systematic reviews to the public improved understanding and accessibility of information: a randomized controlled trial. J Clin Epidemiol. 2015;68(2):182–90.
Schwartz LM, Woloshin S, Welch HG. Using a drug facts box to communicate drug benefits and harms: two randomized trials. Ann Intern Med. 2009;150(8):516–27.
McCullough AR, Rathbone J, Parekh S, Hoffmann TC, Del Mar CB. Not in my backyard: a systematic review of clinicians’ knowledge and beliefs about antibiotic resistance. J Antimicrob Chemoth. 2015;70(9):2465–73.
Grossman Z, del Torso S, Hadjipanayis A, van Esso D, Drabik A, Sharland M. Antibiotic prescribing for upper respiratory infections: European primary paediatricians’ knowledge, attitudes and practice. Acta Paediatr. 2012;101(9):935–40.
Abhyankar P, Volk RJ, Blumenthal-Barby J, Bravo P, Buchholz A, Ozanne E, et al. Balancing the presentation of information and options in patient decision aids: an updated review. BMC Med Inform Decis. 2013;13(Suppl 2):S6.
Chewning B, Bylund CL, Shah B, Arora NK, Gueguen JA, Makoul G. Patient preferences for shared decisions: a systematic review. Patient Educ Couns. 2012;86(1):9–18.
Kiesler DJ, Auerbach SM. Optimal matches of patient preferences for information, decision-making and interpersonal behavior: evidence, models and interventions. Patient Educ Couns. 2006;61(3):319–41.
Coulter A, Jenkinson C. European patients’ views on the responsiveness of health systems and healthcare providers. Eur J Public Health. 2005;15(4):355–60.
Thompson-Leduc P, Turcotte S, Labrecque M, Legare F. Prevalence of clinically significant decisional conflict: an analysis of five studies on decision-making in primary care. Br Med J Open. 2016;6(6):e011490.
Gruber C, Keil T, Kulig M, Roll S, Wahn U, Wahn V. History of respiratory infections in the first 12 yr among children from a birth cohort. Pediatr Allergy Immunol. 2008;19(6):505–12.
Adab P, Marshall T, Rouse A, Randhawa B, Sangha H, Bhangoo N. Randomised controlled trial of the effect of evidence based information on women’s willingness to participate in cervical cancer screening. J Epidemiol Community Health. 2003;57(8):589–93.
Kellar I, Sutton S, Griffin S, Prevost AT, Kinmonth AL, Marteau TM. Evaluation of an informed choice invitation for type 2 diabetes screening. Patient Educ Couns. 2008;72(2):232–8.
Acknowledgements
The authors thank Bridget Abell, Sharon Sanders, and Laura Bergade for assistance with recruitment and survey administration, and Elaine Beller for statistical advice.
Authors contributions
All authors contributed to the study design and data interpretation. Tammy Hoffman conceptualised the decision aids, and Peter Coxeter, Tammy Hoffman and Chris Del Mar developed the decision aids and designed the trial protocol. Peter Coxeter led the administration of the trial and statistical analysis, and wrote the first draft of the article. All authors contributed to subsequent drafts and the final version.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was approved by the Bond University Human Research Ethics Committee and was conducted in accordance with the ethical standards of the Declaration of Helsinki. Informed consent was obtained from all participants prior to study enrolment.
Conflict of interest
Peter Coxeter, Chris Del Mar and Tammy Hoffman declare no competing interests.
Funding
The National Health and Medical Research Council funded the study (APP1044904), and the Australian Commission on Safety and Quality in Healthcare funded the development of the decision aids, but played no role in the conduct of the study, analysis, or interpretation of results.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Coxeter, P.D., Del Mar, C.B. & Hoffmann, T.C. Preparing Parents to Make An Informed Choice About Antibiotic Use for Common Acute Respiratory Infections in Children: A Randomised Trial of Brief Decision Aids in a Hypothetical Scenario. Patient 10, 463–474 (2017). https://doi.org/10.1007/s40271-017-0223-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40271-017-0223-2