
Abstract
Background and Objectives
In Japan, polypharmacy reduction policy, which reduces the reimbursement of medical cost, was introduced to address unnecessary psychotropic polypharmacy. The rule was applied to the prescriptions of three or more anxiolytics or three or more hypnotics in the policy introduced in 2012. The prescriptions of four or more antidepressants or four or more antipsychotics were added to the rule in the policy revised in 2014. Furthermore, the prescriptions of three or more drugs of anxiolytics, hypnotics, antidepressants, or antipsychotics were subject to the reduction criteria of the policy revision in 2016. Benzodiazepine receptor agonists (BZs) are classified both into anxiolytics and hypnotics, and the reduction rule was not applied to the category of BZs before April 2018. This study aimed to examine the effect of the policy on the prescriptions of four drug categories as well as BZs from the point of view of the number of drugs and doses.
Methods
This was a retrospective observational study using a large-scale Japanese health insurance claims database. Patients who were prescribed at least one psychotropic drug (anxiolytic, hypnotic, antidepressant, or antipsychotic) during the study period (from April 2011 to March 2017) were selected. Segmented regression analysis was used to analyze the proportions of patients with three or more or four or more drugs as well as patients above clinically recommended doses, and the means of the average daily doses by drug category.
Results
A total of 312,167 patients were identified as a study population. The proportions of patients with three or more drugs in anxiolytics, hypnotics, antidepressants, and antipsychotics significantly decreased after the introduction or revisions of the policy, but not BZs. The proportions of patients with three or more drugs in March 2017 were 0.9%, 2.0%, 1.2%, 2.4%, and 8.9% in anxiolytics, hypnotics, antidepressants, antipsychotics, and BZs, respectively. The effect of the policy in reducing the proportions of patients above clinically recommended doses was identified in antipsychotics after the revision in 2016, but not identified in the sum of anxiolytics and hypnotics as well as BZs after the revision in 2014, and antidepressants after the revision in 2016. The proportions of monotherapy were increased from April 2011 to March 2017 only for antidepressants (76.9% → 80.8%) and antipsychotics (79.8% → 82.1%), and not changed or decreased for anxiolytics (85.2% → 85.7%), hypnotics (78.6% → 77.6%), sum of anxiolytics and hypnotics (68.1% → 65.7%), BZs (68.0% → 67.3%), and sum of psychotropic drugs (52.1% → 49.9%).
Conclusions
The polypharmacy reduction policy reduced the proportions of patients with three or more drugs in four drug categories, but not BZs. Only limited effects were seen for reducing the proportions of patients above clinically recommended doses. The policy was revised in April 2018 again. Further investigation is needed to examine the effect of the revision in 2018.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Psychotropic drugs such as anxiolytics, hypnotics, antidepressants, and antipsychotics are commonly prescribed in the treatment of mental and behavioral disorders [1]. Psychotropic polypharmacy is also common in clinical practice [2,3,4]. Mojtabai and Olfson reported that the proportion of patients with two or more psychotropic drugs increased from 42.6 to 59.8% from 1996–7 to 2005–6 in office-based psychiatry practices in the USA [2]. Their study reported that the proportions of patients with two or more drugs of sedative-hypnotics, antidepressants, and antipsychotics within the drug category in 2005–6 were 17.8%, 25.4%, and 14.9%, respectively [2]. In Japan, the proportions of patients with two or more drugs of anxiolytics, hypnotics, antidepressants, and antipsychotics within the drug category were reported as 16.4%, 27.3%, 34.7%, and 30.0%, and those of three or more drugs were reported as 1.9%, 6.1%, 8.9%, and 8.5% based on claims data from the Japan Medical Data Center’s database in 2009 [5]. In addition, there is a report that the proportion of patients with two or more drugs of any anxiolytics or hypnotics was 54.6% in psychiatry and 20.4% in non-psychiatry based on claims data from the Japanese National Database in 2011 [6]. However, evidence supporting psychotropic polypharmacy is limited [3, 7,8,9,10]. Psychotropic polypharmacy increases the risk of adverse events and drug–drug interactions [2, 9, 11,12,13,14,15,16]. Several guidelines indicate that combination therapy (i.e., combination of several treatments including pharmacological and nonpharmacological treatments) and multiple prescription (i.e., prescription of two or more drugs within the drug category) are not standard therapy and should be considered only if a patient’s symptoms are moderate/severe or do not respond to an adequate dose and duration of a medication [17,18,19].
In Japan, polypharmacy reduction policy, which reduces the reimbursement of medical cost, was introduced in 2012 to address unnecessary psychotropic polypharmacy (Table 1) [20]. All citizens and residents in Japan are covered by health insurance systems. The reimbursement rate of the fee for continuous psychiatric outpatient services/consultation was reduced by 20% if three or more anxiolytics or three or more hypnotics were prescribed at one time in the policy introduced in April 2012. The policy was revised and tightened in October 2014 after the notification of the revision in April 2014, that is, antidepressants as well as antipsychotics were added to the fees reduction provision. The fee for continuous psychiatric outpatient services/consultation, prescription fees, and drug fees were not reimbursed or only partially reimbursed if three or more anxiolytics, three or more hypnotics, four or more antidepressants, or four or more antipsychotics were prescribed at one time. Furthermore, in April 2016, the policy was further tightened, and these fees were not reimbursed or only partially reimbursed if three or more anxiolytics, three or more hypnotics, three or more antidepressants, or three or more antipsychotics were prescribed at one time.
Okumura et al. reported the effect of the polypharmacy reduction policy for anxiolytics and hypnotics, which took effect in 2012 and 2014 [21]. Their study used a database of out-of-hospital prescriptions for outpatients dispensed by community pharmacies, thus it could not evaluate in-hospital prescriptions dispensed by pharmacies inside the hospitals. The aim of the policy is to reduce unnecessary psychotropic polypharmacy. Hence, it is important to follow not only out-of-hospital prescriptions but also in-hospital prescriptions. Moreover, their investigation period, which was between April 2011 and November 2014, seems to be too short to evaluate the effect of the policy revision in 2014, which took effect in October 2014. The polypharmacy reduction policy introduced in 2012 and revised and tightened in 2014 and 2016 was applied to the prescription of “3 or more” or “4 or more” drugs within the drug category (anxiolytics, hypnotics, antidepressants, and antipsychotics) (Table 1). Benzodiazepine receptor agonists (BZs), which are mainstay anxiolytics/hypnotics and have similar mechanisms of action, are classified both into anxiolytics and hypnotics (Table S1 of the Electronic Supplementary Material [ESM]). BZs have high potential for tolerance, dependence, and misuse as well as adverse events such as cognitive impairment, accidents, and falls [22]. The tolerance for BZs causes the increase of their daily dosage [23], which might cause more dependence and adverse events. Hence, promotion of proper prescription and proper use of BZs is an urgent matter. However, the polypharmacy reduction policy in Japan had not had a reduction rule for the category of BZs before April 2018. In addition, high-dose prescription of psychotropic drugs has been a problem in Japan [24, 25]. In particular, some studies indicate that Japanese patients receive higher doses of antipsychotics compared with patients in other countries [26,27,28]. It is also important to address unnecessary high-dose treatment, but this policy had the reduction rule just for the number of drugs, not for total doses although the potency is different between drugs (Table S1 of the ESM).
In this study, we aimed to examine the effect of the polypharmacy reduction policy on the prescriptions of four drug categories as well as BZs from the point of view of the number of drugs and doses using a large-scale Japanese healthcare claims database. This is the first report to evaluate the effect of the polypharmacy reduction policy on all psychotropic prescriptions including both out-of-hospital and in-hospital prescriptions covering the periods through pre-introduction to post-second revision of the policy (that is, between April 2011 and March 2017).
2 Materials and Methods
2.1 Data Source
This study was conducted using a large-scale, Japanese health insurance claims database developed by MinaCare Co., Ltd. (Tokyo, Japan). This database included about 5 million cumulative insured persons’, mainly company employees and their family members’ anonymized claims data provided by corporate health insurance societies. Elderly patients (aged ≥ 75 years) were not included in the database. In this study, monthly administrative claims data including pharmacy claims, medical claims, and diagnosis procedure combination (DPC) claims between April 2011 and March 2017 in health insurance societies that fully covered the investigation period were used. The DPC claims were based on the DPC system, which is a case-mix payment system, according to diagnosis and procedures, which consists of two elements: flat-fee per day payment and fee-for-service payment for inpatients hospitalized only in the DPC introduction hospitals (DPC hospitals) [29]. The database included information on patients’ characteristics (encrypted personal identifiers, age, and sex) and prescribed medications. Pharmacy claims included the information of out-of-hospital prescriptions for outpatients dispensed by community pharmacies, and DPC claims included that of in-hospital prescriptions for inpatients hospitalized in the DPC hospitals. Medical claims included the information of in-hospital prescriptions for outpatients as well as in-hospital prescriptions for inpatients admitted to the hospitals other than the DPC hospitals dispensed by pharmacies inside the hospitals.
2.2 Study Population and Outcome Measures
Patients who were prescribed at least one psychotropic drug (anxiolytic, hypnotic, antidepressant, or antipsychotic) between April 2011 and March 2017 (study period) were defined as a study population. We included both prevalent and new users of psychotropic drugs because our study aim was to evaluate the effect of the policy on this entire population of patients. The classification of the psychotropic drugs was based on the polypharmacy reduction policy in Japan [20] (Table S1 of the ESM). The monthly utilizations of psychotropic drugs were measured as the total number of prescribed drugs in each month by drug category. The number of prescribed drugs was counted based on generic names regardless of formulation.
In addition, the average daily dose of psychotropic drugs was calculated for each patient in each month by drug category and the mean of the average daily doses as well as the proportion of patients who were prescribed more than clinically recommended doses in Japan were calculated. Diazepam-equivalent doses for anxiolytics and hypnotics [30], imipramine-equivalent doses for antidepressants [31, 32], and chlorpromazine-equivalent doses for antipsychotics [33,34,35,36,37] were used (Table S1 of the ESM). For the means of the average daily doses and the proportions of patients above clinically recommended doses, the analysis in which anxiolytics and hypnotics were summed was conducted because BZs, which are mainstay anxiolytics/hypnotics and have similar mechanisms of action, are classified both into anxiolytics and hypnotics. The analysis for BZs was also conducted. The information of “days of supply” was partially missing (30–45% by drug category) in medical claims and DPC claims between April 2011 and March 2012 because entry of the information was not mandatory in these claims before April 2012 [38]. The information of “days of supply” was not missing after April 2012. Hence, the analyses for the means of the average daily doses and the proportions of patients above clinically recommended doses were conducted for the time period after April 2012.
2.3 Statistical Analysis
Characteristics of patients who had any prescription records for psychotropic drugs were summarized using descriptive statistics in each segment period, where the definition of the segment is given below. Segmented regression analysis of interrupted time series [39] using SAS proc autoreg (SAS/ETS software, version 9.4 of the SAS System for Microsoft Windows, SAS Institute Inc., Cary, NC, USA) was conducted to estimate the changes following the introduction or revisions of the polypharmacy reduction policy for psychotropic drugs. This method allows the assessment of how much an intervention such as policy introduction affects specific outcomes immediately and over time. Each segment of the series is allowed to exhibit both a level (intercept) and a trend (slope). A change in level, i.e., an increase or decrease in the outcome after the intervention, constitutes an abrupt intervention effect. A change in trend is defined by an increase or decrease in the slope of the segment after the intervention as compared with the segment preceding the intervention. A change in trend represents a gradual change in the value of the outcome during the segment [39]. In this study, dependent variables of the segmented regression analysis were the proportions of patients in various categories (three or more drugs, four or more drugs, patients above clinically recommended doses) and the means of the average daily doses by drug category. The analysis for the proportions of patients with three or more or four or more drugs were conducted for four drug categories (anxiolytics, hypnotics, antidepressants, and antipsychotics) and BZs. The analyses for the proportions of patients above clinically recommended doses and the means of the average daily doses were conducted for sum of anxiolytics and hypnotics, BZs, antidepressants, and antipsychotics. Independent variables were level and trend change indicator variables for each of the segmented period.
Study period was divided into five segments: period 1; “Baseline” (from April 2011 to March 2012), period 2; “Introduction of the policy” (from April 2012 to March 2014), period 3; “Notification of the revision in 2014” (from April 2014 to September 2014), period 4; “Enforcement of the revision in 2014” (from October 2014 to March 2016), and period 5; “Revision in 2016” (from April 2016 to March 2017). We considered the period 3 as a “phase-in” period before the first revision because the first revision of the polypharmacy reduction policy was notified in April 2014 and enforced in October 2014. The segmented regression analysis was carried out in steps. First, stepwise autoregression with a significance level of 0.05 was used to select the appropriate autocorrelation structure for the full model. Following selection of the autocorrelation structure, the full model was examined in terms of appropriateness of autocorrelation structure (generalized Durbin–Watson test) and for the degree of heteroscedasticity (Portmanteau Q test, Engle’s Lagrange multiplier test). Next, the most parsimonious model was identified by successively eliminating least significant regression terms. The significance level of 0.05 was used as the criterion for retention. The final parsimonious model was again examined for the appropriateness of autocorrelation structure and for the degree of heteroscedasticity.
In addition, observed changes of the proportions of patients by the number of prescribed drugs were described and plotted for four drug categories of psychotropic drugs, sum of anxiolytics and hypnotics, BZs, and sum of psychotropic drugs (i.e., sum of anxiolytics, hypnotics, antidepressants, and antipsychotics) to capture the long-term prescription trend between April 2011 and March 2017. The analysis restricted to the patients who were continuously enrolled in the database during the study period was conducted as a sensitivity analysis to examine the robustness of the results. Data analyses other than the segmented regression analysis were conducted using R version 3.4.1 (R Foundation for Statistical Computing, Vienna, Austria).
3 Results
3.1 Patient Characteristics
A total of 312,167 patients had at least one prescription record for psychotropic drugs during the study period. The patient characteristics were stable throughout the study period (Table 2).
3.2 Effect of the Polypharmacy Reduction Policy for Psychotropic Drugs
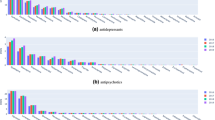
The observed changes of the proportions of patients by the number of prescribed drugs are shown in Table 3 and plotted in Fig. S1 of the ESM. The estimated changes of the proportions of patients with “3 or more” or “4 or more” drugs following the introduction or revisions of the polypharmacy reduction policy based on the most parsimonious segmented regression model are shown in Table 4 and Fig. 1.

Estimated changes of the proportions of patients with three or more/four or more drugs by drug category based on the most parsimonious segmented regression model: a anxiolytics (≥ 3), b hypnotics (≥ 3), c antidepressants (≥ 3), d antidepressants (≥ 4), e antipsychotics (≥ 3), f antipsychotics (≥ 4), and g benzodiazepine receptor agonists (BZs) (≥ 3). Black circle, observed; solid line, estimated piecewise linear trend; dotted line, predicted curve based on an autoregressive model
For anxiolytics and hypnotics, the polypharmacy reduction policy was introduced in April 2012 and revised in October 2014. The revision of the policy in 2014 was notified in April 2014 (Table 1). For the proportions of patients with three or more anxiolytics, there were immediate and notable decreases in the levels at three timepoints (policy introduction in April 2012, notification of the revision in April 2014, and enforcement of the revision in October 2014); there was a slight positive change in the trend (slope) at the policy introduction in April 2012 compared with the preceding period (Table 4), but the overall slope remained slightly negative throughout the study period (Fig. 1a). For the proportions of patients with three or more hypnotics, there was a decrease in the level at the enforcement of the revision in October 2014; there were negative changes in the trends at two timepoints (policy introduction in April 2012 and notification of the revision in April 2014) followed by a positive change in the trend after the enforcement of the revision in October 2014 (Table 4), although the overall slope was consistently negative after April 2012 (Fig. 1b). The largest negative change in the trend compared to the preceding period was observed after the notification of the revision in April 2014. The proportions of patients with “3 or more anxiolytics” and “3 or more hypnotics” decreased from 1.9% and 4.8% in April 2011 to 0.9% and 2.0% in March 2017, respectively (Table 3).
The polypharmacy reduction policy for antidepressants and antipsychotics was introduced in October 2014 after the notification in April 2014 and tightened in April 2016 (Table 1). Thus, prescription of four or more antidepressants and four or more antipsychotics were subject to the reduction criteria in 2014, and prescription of three or more antidepressants and three or more antipsychotics were subject to the criteria in 2016 (Table 1). There were decreases in both the levels and trends of the proportions of patients with three or more antidepressants as well as antipsychotics after the policy revision in April 2016 (Table 4, Fig. 1c, e). There were some changes in the levels or trends of the proportions of patients with four or more antidepressants as well as antipsychotics between April 2014 and March 2017 (Table 4, Fig. 1d, f). Consistent downward trends (slopes) were seen throughout the study period, although the numerical values of the slopes varied in each segmented period for the proportions of patients with “3 or more” and “4 or more” antidepressants as well as antipsychotics (Fig. 1c–f). The proportions of patients with “3 or more” and “4 or more” antidepressants decreased from 4.5% and 0.7% in April 2011 to 1.2% and 0.1% in March 2017, respectively (Table 3). The proportions of patients with “3 or more” and “4 or more” antipsychotics decreased from 4.9% and 1.1% in April 2011 to 2.4% and 0.5% in March 2017, respectively (Table 3). For BZs, which are mainstay anxiolytics/hypnotics, the proportion of patients with three or more BZs had a downward trend before the introduction of the policy in April 2012, but the continuous downward trend was not seen after April 2012 (Table 4, Fig. 1g). In addition, there were no significant decreases in the levels of the proportions of patients with three or more BZs after the policy introduction in April 2012 as well as after the notification and enforcement of the revision in 2014. The proportion of patients with three or more BZs was still 8.9% in March 2017 (Table 3).
The proportions of patients with two drugs were unchanged or increased in all drug categories throughout the study period (Table 3, Fig. S1 of the ESM), which contrasted with the proportions of patients with three or more drugs that decreased after the introduction or revisions of the polypharmacy reduction policy. The proportions of patients with monotherapy were increased from April 2011 to March 2017 only for antidepressants (76.9% → 80.8%) and antipsychotics (79.8% → 82.1%), and not changed or decreased for anxiolytics (85.2% → 85.7%), hypnotics (78.6% → 77.6%), the sum of anxiolytics and hypnotics (68.1% → 65.7%), BZs (68.0% → 67.3%), and the sum of psychotropic drugs (52.1% → 49.9%).
The estimated changes of the proportions of patients above clinically recommended doses and the means of the average daily doses after April 2012 based on the most parsimonious segmented regression model are shown in Table 5 and Figs. 2 and 3. The polypharmacy reduction policy for anxiolytics and hypnotics was introduced in April 2012 and tightened in October 2014, and that for antidepressants and antipsychotics was introduced in October 2014 and tightened in April 2016. The revision of the policy in 2014 was notified in April 2014 (Table 1). For the sum of anxiolytics and hypnotics, BZs, antidepressants, and antipsychotics, the proportions of patients above clinically recommended doses had downward trends before the notification of the revision in April 2014, but the continuous downward trends were not seen after April 2014 (Table 5, Fig. 2a–d). There were some increases and decreases in the sum of anxiolytics and hypnotics, BZs, and antidepressants, but there were no statistically significant decreases in the levels or downward changes in the trends after the strictest revisions of the policy, that is after the notification and enforcement of the revision in 2014 for anxiolytics and hypnotics, and after the revision in 2016 for antidepressants (Table 5, Fig. 2a–c). In addition, the proportions of patients above clinically recommended doses were increased or not changed between March 2014 (before the notification of the revision in 2014) and March 2017 for the sum of anxiolytics and hypnotics, BZs, and antidepressants (Fig. 2a–c). On the other hand, for antipsychotics, there was a statistically significant downward change in the trend after the strictest policy revision in April 2016, and the proportion of patients above clinically recommended doses was decreased after April 2016 (Table 5, Fig. 2d).

Estimated changes of the proportions of patients above clinically recommended doses based on the most parsimonious segmented regression model: a sum of anxiolytics and hypnotics, b benzodiazepine receptor agonists (BZs), c antidepressants, and d antipsychotics. Black circle, observed; solid line, estimated piecewise linear trend; dotted line, predicted curve based on an autoregressive model

Estimated changes of the means of the average daily doses based on the most parsimonious segmented regression model: a sum of anxiolytics and hypnotics, b benzodiazepine receptor agonists (BZs), c antidepressants, and d antipsychotics. Black circle, observed; solid line, estimated piecewise linear trend; dotted line, predicted curve based on an autoregressive model
The means of average daily doses generally showed similar tendency to the proportions of patients above clinically recommended doses except the significant decreases after the enforcement of the revision in October 2014 for the sum of anxiolytics and hypnotics as well as BZs (Table 5, Fig. 3). As a whole, the means of the average daily doses were not decreased between March 2014 (before the notification of the revision in 2014) and March 2017 for antidepressants (Fig. 3c). On the other hand, the means of the average daily doses were decreased after the revision in April 2016 for the sum of anxiolytics and hypnotics, BZs, and antipsychotics (Fig. 3a, b, d).
The analysis based on the full segmented regression model generally yielded similar results (Tables S2 and S3 of the ESM). In addition, the results of the sensitivity analysis restricted to the patients who were continuously enrolled in the database during the study period supported the robustness of these results (data not shown).
4 Discussion
In this study, we investigated the effect of the polypharmacy reduction policy for psychotropic drugs in the period between April 2011 and March 2017. The proportions of patients with three or more anxiolytics significantly decreased after the introduction of the policy in 2012 as well as after the notification and enforcement of the revision in 2014. The proportions of patients with three or more hypnotics significantly decreased after the notification and enforcement of the revision in 2014. In addition, the proportions of patients with three or more antidepressants and three or more antipsychotics significantly decreased after the revision in 2016. These results indicated that the polypharmacy reduction policy led to significant decreases in the proportions of patients with three or more drugs in all categories of the psychotropic drugs (anxiolytics, hypnotics, antidepressants, and antipsychotics). On the other hand, there were no significant decreases in the proportions of patients with three or more BZs after the policy introduction in 2012 as well as after the notification and enforcement of the revision in 2014. The increases in the level of the proportion of patients with three or more antidepressants after the enforcement of the revision in October 2014 as well as with three or more antipsychotics after the notification of the revision in April 2014 seemed to be due to the increases of the proportions of patients with three antidepressants or three antipsychotics after the reduction for the prescription of four or more drugs (Fig. S1c and S1d of the ESM). The change in the trend of the proportion of patients with three or more BZs after the introduction of the policy in April 2012 was thought to be due to the changes of prescriptions of anxiolytics and hypnotics, but there were no significant decreases after April 2012. The proportions of patients with monotherapy were increased from April 2011 to March 2017 only for antidepressants and antipsychotics, and not changed or decreased for anxiolytics, hypnotics, sum of anxiolytics and hypnotics, BZs, and sum of psychotropic drugs. The proportions of patients with two or more drugs in March 2017 were still 14.3%, 22.4%, 19.2%, and 17.9% in anxiolytics, hypnotics, antidepressants, and antipsychotics, and 34.3%, 32.7%, and 50.1% in the sum of anxiolytics and hypnotics, BZs, and sum of psychotropic drugs, respectively.
The study using a large and representative sample of visits to office-based psychiatrists in the USA reported that the proportions of patients with two or more drugs in 2005–6 were 17.8%, 25.4%, and 14.9% in sedative-hypnotics, antidepressants, and antipsychotics, respectively [2]. The study using Australian pharmaceutical claims data showed that the proportions of patients with two or more drugs in 2015 were 3.7%, 7.3%, and 2.9% in antidepressants, antipsychotics, and BZs, respectively [40]. The Research on Asian Psychotropic Prescription Patterns (REAP) for antidepressants reported that the proportions of patients with two or more antidepressants were 3–25% in five East Asian countries in 2004 [41]. We cannot compare these figures directly because the databases, populations, and study periods were different, but the proportions of patients with two or more drugs within the drug category in Japan did not seem to be lower than these countries even in 2017.
In Japan, the high rate of antipsychotic polypharmacy compared with other countries has been known for a few decades [42, 43], and some clinical trials were conducted to simplify antipsychotic prescription in Japan [44,45,46]. There had been efforts to reduce antipsychotic polypharmacy, but drastic measures to address it had been needed. The polypharmacy reduction policy reduced antipsychotic polypharmacy and the mean daily dose of antipsychotics. The decreasing trend shown in the present study corresponded with the other report [43]. However, the REAP for antipsychotics in 2016 indicated that the rate of psychotropic polypharmacy including within- and between-drug categories and high-dose treatment for patients with schizophrenia was the highest in Japan among 15 Asian countries/areas [26, 47], and further improvement will be needed.
The polypharmacy reduction policy in Japan had not had a reduction rule for the category of BZs before April 2018. BZs were separately classified into anxiolytics and hypnotics, and therefore, if two BZs of anxiolytics and one BZ of hypnotics were prescribed at one time, a fees reduction was not applied. In the present study, there were no significant decreases in the proportions of patients with three or more BZs after the policy introduction in 2012 and the notification and enforcement of the revision in 2014. The reduction policy should be applied to polypharmacy of BZs because they have similar mechanisms of action and safety profiles.
Various policies to reduce the prescription of BZs were introduced in Western countries. In the USA, Medicare Part D, which is a prescription drug coverage program, excluded BZs from coverage in 2006 [48, 49]. In the Netherlands, BZs were excluded from the Dutch reimbursement list when used as anxiolytics, hypnotics, or sedatives in 2009 [50, 51]. Furthermore, in France, the new payment system started in 2012, in which general practitioners could receive monetary benefit in the case that they reduced the prescription of BZs in some criteria [52]. In the Netherlands case, the prescription of BZs was decreased, but in the USA and France cases, the prescription of BZs was not decreased. There are limitations to compare these policies because the policy characteristics and environments are different between countries, but some political intervention will be needed in Japan based on the lessons from other countries. Actually, in Japan, the new reduction rule for BZs was introduced in April 2018, in which the reimbursement rates of the prescription fees are reduced by about 30–40% if BZs are prescribed for more than 12 months with the same dosage and regimen [20]. This fees reduction seemed to be applied in April 2019 when 12 months passed after the rule was enforced. The effect of this rule needs to be investigated, but there is some doubt about the effect because this fees reduction is not applied if the dosage or regimen of BZs is changed within 12 months.
In the present study, the proportions of patients above clinically recommended doses were increased or not changed between March 2014 (before the notification of the revision in 2014) and March 2017 for the sum of anxiolytics and hypnotics, BZs, and antidepressants although there were some increases and decreases. For antipsychotics, the proportion of patients above clinically recommended doses was decreased after the revision in April 2016. There were immediate increases in the levels of the proportions of patients above clinically recommended doses for sum of anxiolytics and hypnotics as well as BZs after the notification of the revision in April 2014. The increases of the means of the average daily doses were also identified at that time. The temporal increases of the doses by switching of medications seemed to be one of the reasons. This tendency corresponded with the other report [21]. The effect of the policy in reducing the proportions of patients above clinically recommended doses was identified in antipsychotics after the policy revision in 2016, but not identified in the sum of anxiolytics and hypnotics as well as BZs after the notification and enforcement of the revision in 2014, and antidepressants after the revision in 2016. Thus, in the present study, only limited effects were seen for reducing the proportions of patients above clinically recommended doses although the proportions of patients with three or more drugs were decreased after the introduction or revisions of the polypharmacy reduction policy. The rule considering total doses in addition to the number of prescribed drugs should be taken into account in this policy because the potency is different between drugs (Table S1 of the ESM). On the other hand, the means of the average daily doses in the sum of anxiolytics and hypnotics as well as BZs were decreased after April 2016, although there was no policy revision for anxiolytics and hypnotics at that time. Further investigation is needed to examine the trend after March 2017.
There are some limitations in this study. First, the results might have been biased because of changes in the study population and simultaneously occurring other interventions [53]. However, the patient characteristics were stable during the study period, and the sensitivity analysis restricted to the patients who were continuously enrolled in the database during the study period yielded similar results. In addition, other interventions, if any, should not have had a big enough impact to reverse the effect of the polypharmacy reduction policy because this policy is the only one to penalize prescribers. Second, because the insurance claims included a monthly summary of healthcare services provided by healthcare providers, drugs prescribed in each month was regarded as a simultaneous prescription. We did not evaluate out-of-hospital/in-hospital prescriptions separately and could not evaluate prescriptions based on psychiatry/non-psychiatry separately. However, we believe it is important to examine whole prescriptions for each patient using the claims data, which includes all prescribed drugs covered by the health insurance system, to evaluate the actual condition of psychotropic polypharmacy. Third, as mentioned in the methods section, we could not evaluate the effect of the introduction of the policy in 2012 on the proportions of patients above clinically recommended doses and the mean daily doses for the sum of anxiolytics and hypnotics as well as BZs because of the lack of information before April 2012. We were, however, able to evaluate the effect of the policy revision in 2014 on the proportions of patients above clinically recommended doses and the means of the average daily doses. As the rule of the fees reduction in 2014 was much stricter than that in 2012 (Table 1), our study did cover the most important parts of the policies. Fourth, elderly patients aged ≥ 75 years were not included because the claims data used in this study were mainly for those covered by employment-based health insurance. There is a limitation to generalize these findings to the elderly population and the population covered by other types of insurance. Last, we did not investigate any effectiveness indicators such as disease improvement or deterioration, rates of adverse events, medical resource utilization, and medical cost. Further investigation is needed to examine the effect of the policy on such effectiveness indicators.
5 Conclusions
This study demonstrated that the polypharmacy reduction policy for psychotropic drugs led to decreases in the proportions of patients with three or more drugs in anxiolytics, hypnotics, antidepressants, and antipsychotics, but not BZs. The proportions of monotherapy were increased only for antidepressants and antipsychotics, and not changed or decreased for anxiolytics, hypnotics, sum of anxiolytics and hypnotics, BZs, and the sum of psychotropic drugs. In addition, only limited effects were seen for reducing the proportions of patients above clinically recommended doses. Further investigation is needed to examine the effect of the following revision of the policy enforced in April 2018 on psychotropic prescription including BZs.
References
Linden M, Lecrubier Y, Bellantuono C, Benkert O, Kisely S, Simon G. The prescribing of psychotropic drugs by primary care physicians: an international collaborative study. J Clin Psychopharmacol. 1999;19:132–40.
Mojtabai R, Olfson M. National trends in psychotropic medication polypharmacy in office-based psychiatry. Arch Gen Psychiatry. 2010;67:26–36.
Nørgaard A, Jensen-Dahm C, Gasse C, Hansen ES, Waldemar G. Psychotropic polypharmacy in patients with dementia: prevalence and predictors. J Alzheimers Dis. 2017;56:707–16.
Hung GC, Yang SY, Chen Y, Lin SK. Psychotropic polypharmacy for the treatment of bipolar disorder in Taiwan. Psychiatr Serv. 2014;65:125–8.
Mishima K. Survey on prescription of psychotropic drugs using claims data (in Japanese). Domestic and international comparative study for psychotropic prescriptions, 2010 study report. Tokyo: Ministry of Health, Labour and Welfare study results database; 2012. p. 15–30.
Arakawa R, Okumura Y, Ikeno T, Kim Y, Ito H. Actual status of prescription patterns of anxiolytics and hypnotics in outpatients using National Database of Health Insurance Claim Information and Specific Medical Checkups (in Japanese). Jpn J Clin Psychiatry. 2015;44:1003–10.
National Association of State Mental Health Program Directors (NASMHPD) Medical Directors Council and State Medicaid Directors. Technical report on psychiatric polypharmacy. 2001. Available from: https://www.nasmhpd.org/sites/default/files/Polypharmacy.pdf. Accessed 11 July 2019.
Moore TA, Buchanan RW, Buckley PF, Chiles JA, Conley RR, Crismon ML, et al. The Texas Medication Algorithm Project antipsychotic algorithm for schizophrenia: 2006 update. J Clin Psychiatry. 2007;68:1751–62.
Galling B, Roldán A, Hagi K, Rietschel L, Walyzada F, Zheng W, et al. Antipsychotic augmentation vs. monotherapy in schizophrenia: systematic review, meta-analysis and meta-regression analysis. World Psychiatry. 2017;16:77–89.
Inada K. Problem of polypharmacy (in Japanese). Modern Physician. 2014;34:665–8.
Tiihonen J, Suokas JT, Suvisaari JM, Haukka J, Korhonen P. Polypharmacy with antipsychotics, antidepressants, or benzodiazepines and mortality in schizophrenia. Arch Gen Psychiatry. 2012;69:476–83.
Gören JL, Parks JJ, Ghinassi FA, Milton CG, Oldham JM, Hernandez P, et al. When is antipsychotic polypharmacy supported by research evidence? Implications for QI. Jt Comm J Qual Patient Saf. 2008;34:571–82.
Urichuk L, Prior TI, Dursun S, Baker G. Metabolism of atypical antipsychotics: involvement of cytochrome p450 enzymes and relevance for drug-drug interactions. Curr Drug Metab. 2008;9:410–8.
Westaway K, Sluggett JK, Alderman C, Procter N, Roughead E. Prevalence of multiple antipsychotic use and associated adverse effects in Australians with mental illness. Int J Evid Based Healthc. 2016;14:104–12.
Nemeroff CB, DeVane CL, Pollock BG. Newer antidepressants and the cytochrome P450 system. Am J Psychiatry. 1996;153:311–20.
Preskorn SH, Borges-Gonzalez S, Flockhart D. Clinically relevant pharmacology of neuropsychiatric drugs approved over the last three years: part II. J Psychiatr Pract. 2006;12:312–6.
National Institute for Health and Care Excellence. Depression in adults: recognition and management. Clinical guideline [CG90]. Last updated: 2018. Available from: https://www.nice.org.uk/guidance/cg90. Accessed 11 July 2019.
Herzog DP, Wagner S, Ruckes C, Tadic A, Roll SC, Härter M, et al. Guideline adherence of antidepressant treatment in outpatients with major depressive disorder: a naturalistic study. Eur Arch Psychiatry Clin Neurosci. 2017;267:711–21.
The American Psychiatric Association. Practice guidelines for the psychiatric evaluation of adults. 3rd ed. 2015. Available from: https://doi.org/10.1176/appi.books.9780890426760.pe02. Accessed 31 July 2019.
Ministry of Health, Labour and Welfare. Medical fee revision (in Japanese). Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000106602.html. Accessed 11 July 2019.
Okumura Y, Inada K, Matsumoto T, Shimizu S. Changes in high-dose and combined anxiolytic-hypnotic prescription in outpatient psychiatric practice after regulatory action (in Japanese). Jpn J Clin Psychopharmacol. 2015;18:1173–88.
Medicines Management Programme. Guidance on appropriate prescribing of benzodiazepines and z-drugs (BZRA) in the treatment of anxiety and insomnia. 2018. Available from: https://www.hse.ie/eng/about/who/cspd/ncps/medicines-management/bzra-for-anxiety-insomnia/bzraguidancemmpfeb18.pdf. Accessed 11 July 2019.
Tamburin S, Federico A, Faccini M, Casari R, Morbioli L, Sartore V, et al. Determinants of quality of life in high-dose benzodiazepine misusers. Int J Environ Res Public Health. 2017. https://doi.org/10.3390/ijerph14010038.
Inagaki A, Tomita M. Novel antipsychotics, antipsychotic polypharmacy and high-dose treatment in Japan (in Japanese). Jpn J Clin Psychopharmacol. 2003;6:391–401.
Nakagawa A, Mishima K, Inagami A, et al. International comparison of psychotropic medication prescription patterns (in Japanese). Special Research Summary Report in 2010. 2012. Available from: http://mhlw-grants.niph.go.jp/niph/search/NIDD00.do?resrchNum=201005018A. Accessed 11 July 2019.
Park YC, Yang SY, Chong MY, Kanba S, Sartorius N, Shinfuku N, et al. Differences in high dose antipsychotic prescriptions in patients with schizophrenia in Asian countries/areas: findings from the REAP-AP Study. Psychiatry Investig. 2018;15:1007–8.
Shinfuku N, Tan CH. Pharmacotherapy for schizophrenic inpatients in East Asia: changes and challenges. Int Rev Psychiatry. 2008;20:460–8.
Inagaki A. Validity of high-dose and multiple prescription of antipsychotics (in Japanese). Schizophr Front. 2005;6:58–62.
Nakamura K. Diagnosis procedure combination database would develop nationwide clinical research in Japan. Circ J. 2016;80:2289–90.
Inagaki A, Inada T. Dose equivalence of psychotropic drugs. Part XXIV: dose equivalence of anti-anxiolytics/hypnotics: eszopiclone (in Japanese). Jpn J Clin Psychopharmacol. 2012;15:1403–6.
Inagaki A, Inada T. Dose equivalence of psychotropic drugs. Part XVIII: dose equivalence of psychotropic drugs: 2006-version (in Japanese). Jpn J Clin Psychopharmacol. 2006;9:1443–7.
Inagaki A, Inada T. Dose equivalence of psychotropic drugs. Part XXVII: dose equivalence of novel antidepressants II: venlafaxine (in Japanese). Jpn J Clin Psychopharmacol. 2018;21:547–62.
Inagaki A, Inada T. Dose equivalence of psychotropic drugs. Part XX: dose equivalence of injectable antipsychotics (in Japanese). Jpn J Clin Psychopharmacol. 2007;10:2373–7.
Inagaki A, Inada T. Dose equivalence of psychotropic drugs. Part XXI: dose equivalence of novel antipsychotics: blonanserin (in Japanese). Jpn J Clin Psychopharmacol. 2008;11:887–90.
Inagaki A, Inada T. Dose equivalence of psychotropic drugs. Part XXII: dose equivalence of depot antipsychotics III: risperidone long-acting injection (in Japanese). Jpn J Clin Psychopharmacol. 2010;13:1349–53.
Inagaki A, Inada T. Dose equivalence of psychotropic drugs. Part XXV: dose equivalence of depot antipsychotics IV: aripiprazole once-monthly (in Japanese). Jpn J Clin Psychopharmacol. 2015;18:1475–80.
Inagaki A, Inada T. Dose equivalence of psychotropic drugs. Part XXVI: dose equivalence of novel antipsychotics: asenapine (in Japanese). Jpn J Clin Psychopharmacol. 2017;20:89–97.
Department of Health, Ministry of Health, Labour and Welfare. Entry spec of claims through online or optical disk (version April 2012) (in Japanese). Various information of medical fee. 2012. Available from: http://www.iryohoken.go.jp/shinryohoshu/file/spec/24bt1_1_kiroku.pdf. Accessed 11 July 2019.
Wagner AK, Soumerai SB, Zhang F, Ross-Degnan D. Segmented regression analysis of interrupted time series studies in medication use research. J Clin Pharm Ther. 2002;27:299–309.
Brett J, Daniels B, Karanges EA, Buckley NA, Schneider C, Nassir A, et al. Psychotropic polypharmacy in Australia, 2006 to 2015: a descriptive cohort study. Br J Clin Pharmacol. 2017;83:2581–8.
Tanaka M, Nagai H, Uchida N, Kawaguchi Y, Fujii S, Nishimura R, et al. The pattern of antidepressant usage in East Asia: international collaborative prescription survey among 5 Asian countries and regions (REAP-AD) (in Japanese). Jpn J Clin Psychopharmacol. 2007;10:131–46.
Inagaki A. Antipsychotic polypharmacy: a comparison between Japan and foreign countries (in Japanese). Jpn J Psychiatr Treat. 2003;18:771–7.
Inagaki A. Current status of antipsychotic polypharmacy in the treatment for schizophrenia (in Japanese). Jpn J Clin Psychopharmacol. 2019;22:347–57.
Tanabe A. A study of reducing the number of antipsychotic drugs in chronic schizophrenia (in Japanese). Keio J Med. 2000;77:231–9.
Sukegawa T, Ito T, Hasegawa M, Mizuno Y, Inagaki A, Sakamoto H, et al. A randomized controlled trial on the dose reduction and simplification for polypharmacy of antipsychotics (in Japanese). Tottori J Clin Res. 2008;1:169–81.
Yamanouchi Y, Sukegawa T, Inagaki A, Inada T, Yoshio T, Yoshimura R, et al. Evaluation of the individual safe correction of antipsychotic agent polypharmacy in Japanese patients with chronic schizophrenia: validation of safe corrections for antipsychotic polypharmacy and the high-dose method. Int J Neuropsychopharmacol. 2015;18:1–8.
Shinfuku N, Hayakawa K, Shih-ku L, Kato T. Problems of Japan’s psychotropic prescription based on the Research on East Asian Psychotropic Prescription Pattern (REAP) (in Japanese). Jpn J Clin Psychopharmacol. 2017;20:983–91.
Lai LL, Bleidt BA, Singh-Franco D, Elusma C, Huh G. Trends in benzodiazepine prescribing under Medicare Part D in USA: outpatient settings 2005–2009. J Pharm Health Serv Res. 2015;6:133–8.
Stubbings J, Lau DT. Medicare Part D research highlights and policy updates, 2013: impact and insights. Clin Ther. 2013;35:402–12.
Hoebert JM, Souverein PC, Mantel-Teeuwisse AK, Leufkens HG, van Dijk L. Reimbursement restriction and moderate decrease in benzodiazepine use in general practice. Ann Fam Med. 2012;10:42–9.
Clay E, Falissard B, Moore N, Toumi M. Contribution of prolonged-release melatonin and anti-benzodiazepine campaigns to the reduction of benzodiazepine and Z-drugs consumption in nine European countries. Eur J Clin Pharmacol. 2013;69:1–10.
Rat C, Penhouet G, Gaultier A, Chaslerie A, Pivette J, Nguyen JM, et al. Did the new French pay-for-performance system modify benzodiazepine prescribing practices? BMC Health Serv Res. 2014;14:301.
Chen H, Nwangwu A, Aparasu R, Essien E, Sun S, Lee K. The impact of Medicare Part D on psychotropic utilization and financial burden for community-based seniors. Psychiatr Serv. 2008;59:1191–7.
Ministry of Education Culture, Sports, Science and Technology, Ministry of Health, Labour and Welfare. Ethical guidelines for epidemiological research. 2002. Available from: http://www.niph.go.jp/wadai/ekigakurinri/guidelines.pdf. Accessed 11 July 2019.
Acknowledgements
MinaCare Co., Ltd. provided the claims data. The authors acknowledge Mamoru Narukawa (Kitasato University) and Masayuki Kaneko (Kitasato University) for their useful advice on this study. The authors also acknowledge John Fowler for the grammar check.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Pfizer Japan Inc. provided financial support for the use of claims data.
Conflict of interest
Yoko Hirano is an employee of Pfizer Pharmaceuticals K.K. Yoichi Ii is an employee of Pfizer R&D Japan G.K. and holds stock/stock options of Pfizer Inc.
Ethics approval
This study did not require ethical committee review in accordance with current ethical standards for epidemiological studies in Japan [54].
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hirano, Y., Ii, Y. Changes in Prescription of Psychotropic Drugs After Introduction of Polypharmacy Reduction Policy in Japan Based on a Large-Scale Claims Database. Clin Drug Investig 39, 1077–1092 (2019). https://doi.org/10.1007/s40261-019-00838-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-019-00838-w