
Abstract
Background and Objective
The use and range of indications for anticoagulation therapy are steadily growing. The objective of this study was to develop a scoring model to predict the occurrence of significant bleeding in patients taking warfarin with a supra-therapeutic international normalized ratio.
Methods
Data were collected from the medical records of patients taking warfarin with an international normalized ratio > 3.5. The characteristics of bleeding episodes and the need for transfusion of blood products were recorded. Regression models were constructed to predict the occurrence of significant bleeding (requiring a transfusion of more than 2 units of packed red blood cells, intrapericardial or intracranial hemorrhage). The predictive values of previously published scores (ATRIA: anemia, hypertension, severe renal disease, age ≥ 75 years, or prior bleeding history; and ORBIT: old, reduced hemoglobin, bleeding history, kidney insufficiency or antiplatelet treatment) were compared with our New Bleeding Score (NBLDSCOR); the areas under the curve for the receiver-operating characteristic plots were compared using a non-parametric DeLong test.
Results
Significant bleeding was reported in 87 out of 389 admitted patients. With an area under the curve of 0.736 ± 0.032, NBLDSCOR was the best predictor of significant bleeding in this population. Neither ATRIA nor ORBIT was a good predictor of significant bleeding, where the area under the curve for the receiver-operating characteristic plot for ATRIA was 0.654 ± 0.034 and for ORBIT was 0.604 ± 0.033. The predictive power of NBLDSCOR was superior to ATRIA and ORBIT (p < 0.001), while there was no meaningful difference in the predictive powers of ATRIA and ORBIT.
Conclusion
The NBLDSCOR including age, negative Rhesus factor, low hemoglobin, renal impairment, and concomitant peptic ulcer and disseminated cancer is a good predictor of significant bleeding in this patient population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Significant bleeding with a supratherapeutic international normalized ratio with warfarin can be predicted using a score including age, presence of Rhesus factor, low hemoglobin, renal impairment, and concomitant peptic ulcer disease and disseminated cancer as influential factors. |
Calculating a score based on these factors increases the discriminatory power of previously suggested scores for predicting significant bleeding in patients with an increased international normalized ratio. |
1 Introduction
Currently, the range of indications for the use of anticoagulation therapy is steadily growing. Warfarin and other anticoagulants are effective in the primary and secondary prevention of life-threatening conditions such as embolic cerebrovascular events, myocardial infarction, and venous thromboembolism [1,2,3]. In parallel, the fear of iatrogenic hemorrhage risk discourages many clinicians from prescribing warfarin as the first line of anticoagulation. Anticoagulants, primarily warfarin, cause 10.2% of drug-related preventable adverse events in ambulatory clinical settings [4], reinforcing the need for a special focus on the ordering and monitoring stages of pharmaceutical care. Obviously, the rate of adverse events greatly depends on the characteristics and underlying disease of patients.
Accurate risk stratification according to the risk of hemorrhage would facilitate proper anticoagulation decision making for patients before the start of a treatment and the identification of individuals for whom the benefits of anticoagulants outweigh the risks. Furthermore, a valid bleeding risk scheme helps clinicians monitor anticoagulation therapy more carefully in patients at a high risk of bleeding [5]. Previous studies have suggested several clinical and laboratory variables for identifying those with an increased bleeding risk [6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21]. These include male sex, older age, previous history of bleeding, preexisting cardiac, hepatic, and renal disease, and the concomitant use of other drugs that may affect hemostasis. Most of these studies often calculate the associated risk for patients with atrial fibrillation (AF) [9, 11, 16,17,18,19,20,21]. The risk of bleeding for patients receiving warfarin anticoagulation for causes other than AF may still remain undetermined because of the lack of necessary clinical and paraclinical information [13, 15, 20]. Therefore, a need for a simple and accurate risk scoring system is still compelling to predict the occurrence of adverse significant bleeding events in patients receiving warfarin.
To our knowledge, no scoring system has been developed to assess the risk of significant bleeding in patients with a supra-therapeutic level of international normalized ratio (INR). We aimed to describe and validate a new hemorrhage risk stratification tool and compare its accuracy and safety to various published hemorrhage risk scores. We hypothesize that the new scoring system has a higher predictive value compared with the previously described scoring systems.
2 Patients and Methods
This is a retrospective cross-sectional study conducted through the evaluation of medical records for patients admitted during January 2016 through March 2018 with excessive warfarin anticoagulation at two university-affiliated cardiology hospitals in Tabriz, Iran. The study protocol was reviewed and approved by the Institutional Review Board and Ethics Committee of Tabriz University of Medical Sciences. This study was exempted from the informed consent process owing to the retrospective design of the study, but all patient data were handled with special care to assure that patient confidentiality was maintained. Patient records were examined for “warfarin overdose”, “warfarin toxicity”, or “supra-therapeutic INR” using admission diagnosis codes.
2.1 Study Population
Patients receiving warfarin and presenting with symptomatic bleeding or who were admitted based on purely incidental findings of supratherapeutic INR (> 3.5) were enrolled in the study. We excluded patients with accidental or intentional (i.e., suicide attempt) ingestion of warfarin, high INR unrelated to warfarin therapy, and records with missing data. Indications for warfarin therapy included the presence of valvular and non-valvular AF, status after implantation of mechanical and bioprosthetic heart valves, the presence of left ventricular clots, deep vein thrombosis, pulmonary thromboembolism, cerebrovascular attacks, and those with transient ischemic attacks who have been administered warfarin for stroke prevention.
2.2 Data Collection
A trained research physician used standardized forms to collect patient baseline information at the time of hospital discharge or presentation to the ambulatory clinic. Patient characteristics including sex, age, level of education, place of residence, indication for warfarin treatment, dosage (milligrams), duration of treatment, and the status of INR testing were recorded for each participant. Medication history and information on concomitant use of platelet inhibitors, antibiotics, or amiodarone and the presence of comorbid conditions [i.e., diabetes mellitus, hypertension, smoking, ischemia, congestive heart failure, chronic obstructive pulmonary disease, chronic kidney disease (estimated glomerular filtration rate < 60 mL/min), cerebrovascular accident, peptic ulcer disease, or neoplastic disease] were also collected. Polypharmacy was defined as concomitant use of five or more medications.
Furthermore, clinical manifestations of bleeding such as petechia/ecchymosis, hematoma, and gastrointestinal and intracranial bleeding were recorded. Electrocardiographic, echocardiographic, and laboratory findings were also documented at the time of admission. Laboratory data included a complete coagulation profile [prothrombin time, partial thromboplastin time, INR, platelet count, complete blood cell count, ABO and Rhesus (Rh) blood group] and renal function tests (blood urea nitrogen and creatinine) at the time of admission. Hemoglobin and coagulation profiles were also measured daily until the patients were deceased or discharged from the hospital.
Bleeding complications were treated by a hospitalist and generally included injectable vitamin K, and/or packed red blood cells (PRBC), fresh frozen plasma transfusion, based on the severity of symptoms. The therapeutic information was also documented. Moreover, hospital length of stay was collected.
2.3 Definition of Bleeding Risk Schemes
We compared the predictive performance of our score, named New Bleeding Score (NBLDSCOR) to that of three existing scores, CHA2DS2-VASc, ORBIT, and ATRIA [22]. Components of the CHADS-Vasc score were defined by sex, age at inclusion, a diagnosis of heart failure, hypertension, diabetes mellitus, previous history of stroke (ischemic stroke, unspecified stroke, transient ischemic attach, or systemic emboli), and vascular disease (prior myocardial infarction and peripheral arterial disease). The ORBIT score was derived from 556 patients in a retrospective cohort study [23]. ORBIT is an acronym for: age Older than 74 years, Reduced hemoglobin or presence of anemia or abnormal hemoglobin/hematocrit (hemoglobin < 13 g/dL or hematocrit < 40% for male individuals and hemoglobin < 12 g/dL or hematocrit < 36% for female individuals), Bleeding history, Insufficient kidney function (eGFR < 60 mL/min/1.73 m2), or Treatment with any antiplatelet drug. The ATRIA score was derived from 461 major hemorrhages occurring in 9186 adults with AF enrolled in a large community-based cohort in Northern California [9] and calculated using the following: anemia (hemoglobin < 13 g/dL in men and < 12 g/dL in women), severe renal disease (eGFR < 30 mL/min/1.73 m2), age ≥ 75 years, prior bleeding history, and hypertension. Our final model for calculating the NBLDSCOR included age, Rh factor, eGFR, peptic ulcer disease, low hemoglobin, and disseminated cancer.
2.4 Statistical Analysis
Data were collected into an Excel worksheet and then exported into the Statistical Program for Social Sciences (SPSS Version 24.0, IBM Inc., Chicago, IL, USA) for statistical analysis. Nominal variables were analyzed using the chi-square test and reported as numbers and percentages. Continuous variables were analyzed with t tests if they followed a normal distribution and were reported as mean ± standard deviation. Mann–Whitney U tests were used if the normality was rejected for the numerical variables and data were expressed as median with interquartile range. Odds ratios were calculated and reported along with 95% confidence intervals.
The outcome variable was the occurrence of significant bleeding as defined by the presence of bleeding into the cranial or pericardial cavity with compression effects on the brain or the heart, or any other bleeding that required a transfusion of at least 2 units of packed red blood cells. Multivariate regression models were constructed for the risk of significant bleeding and a p value < 0.05 was regarded as statistically significant. Multivariate analysis was created by including any factors that seemed to have a near-significant effect on the occurrence of significant bleeding. Additional scores such as ATRIA, ORBIT, and CHA2DS2-VASc were calculated for all patients. Following the multivariate analysis, a new score was calculated including all factors with significant p values multiplied by its regression coefficient. Bonferroni correction was applied for multiple comparisons. The predictive values of previously published scores (ATRIA, ORBIT, and CHA2DS2-VASc) and our own score were assessed by multiple receiver-operating characteristic analysis. After calculation of the new bleeding scores and the commonly used scoring system for each individual patient, the area under the receiver-operating characteristic curve method (AUC, a measure of their c-index) was performed for each scoring system to calculate its predictive power. Their respective AUCs were then compared according to the De Long and Clarke-Pearson method.
3 Results
Medical records of 485 patients admitted with excessive warfarin anticoagulation were screened, and after excluding records with the study exclusion criteria (n = 96), 389 patients (221 women and 168 men) with a mean age of 64 ± 16 years were enrolled. The most common comorbidity was hypertension (43%) followed by renal diseases (36%), congestive heart failure (22%), and diabetes mellitus (17%). Moreover, a previous history of cerebrovascular events was common (14%). The most common indication for anticoagulation was non-valvular AF in 29% of patients followed by mechanical heart valve (26%) and pulmonary thromboembolism (23%).
A total of 321 patients (82.5%) presented with symptomatic bleeding and 68 (17.5%) were admitted based purely on incidental findings of supratherapeutic INR. The admission level of INR was 7.51 ± 2.64 with an average duration prothrombin time of 36.3 ± 6.4 s. Gastrointestinal bleeding, epistaxis, and intra-cranial hemorrhage were among the most common manifestations, constituting 17%, 9%, and 4% of admitted patients, respectively. Polypharmacy was noted in 31% of the patients at the time of admission and 123 patients (32%) were concomitantly using anti-platelet drugs (aspirin or clopidogrel).
Significant bleeding was reported in 87 patients from whom 17 had intracranial hemorrhage/hematoma, three had intrapericardial bleeding with signs of cardiac tamponade, and the remaining 67 patients mainly experienced gastrointestinal bleeding requiring a transfusion of 2 or more units of PRBC. The characteristics of subjects with non-significant and significant bleeding are summarized in Table 1. In a total of 21 patients, the resultant hypovolemic shock necessitated a transfusion of 4 or more units of PRBC. The characteristics of these patients are shown in Table 2. Univariate analyses along with the odds ratios and 95% confidence intervals of contributing risk factors for developing significant bleeding and hypovolemic shock are shown in Tables 1 and 2, respectively. Accordingly, the prevalences of disseminated cancers and peptic ulcer and chronic kidney diseases were higher among patients with significant bleeding. Moreover, congestive heart failure comorbidity was more common among patients requiring a transfusion of more than 4 units of PRBC.
Considering clinical outcomes, patients who experienced a significant bleeding event were more likely to have major and non-fatal complications, higher hospitalization length, and be treated with PRBC or fresh frozen plasma than those with non-significant bleeding (Table 3). Variables associated with significant hemorrhage on univariate analysis were considered for the multivariate model used for scoring purposes. By univariate analysis, significant predictors of bleeding were Rh antigen, congestive heart failure, chronic kidney disease (eGFR ≤ 30 mL/min/1.73 m2), disseminated cancers, and peptic ulcer disease. The multivariate analysis model of prediction was constructed based on nearly significant factors (with p values ≤ 0.1 in univariate analyses) and covariates using significant bleeding as the primary dependent outcome variable (Table 4). Based on the results of this multivariate regression model, six variables emerged for calculation of the NBLDSCOR: (age group < 65: 0; 65–74: 1; and ≥ 75 years: 2) + (Rh factor positive: 0/Rh factor negative: 1) + (eGFR ≥ 30 mL/min/1.73 m2: 0/eGFR < 30 mL/min/1.73 m2: 3) + (no peptic ulcer disease: 0/peptic ulcer disease: 4) + (hemoglobin level > 12 g/dL in female individuals and > 13 g/dL in male individuals: 0/hemoglobin level ≤ 12 g/dL in female individuals and ≤ 13 g/dL in male individuals: 4) + (no disseminated cancer: 0/disseminated cancer: 5).
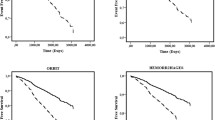
Table 5 shows the predictive power of clinical scores for the incidence of significant and non-significant bleeding among the entire study population. Accordingly, the discriminatory power for all scores ranged from 0.503 to 0.736; the estimated trends were statistically significant, except for the CHA2DS2-VASc score (p = 0.816). Figure 1 displays the predictive power (AUC) of each of the three models (NBLDSCOR, ORBIT, and ATRIA). Among those treated with warfarin, the highest discrimination was seen with the NBLDSCOR (AUC = 0.736), followed by the ATRIA scores. The CHADS-Vasc2 score exhibited relatively poor discrimination for bleeding risk among patients with supra-therapeutic INR. According to the analyses, reflecting the comparison of AUC (Fig. 1), the NBLDSCOR performed significantly better than ATRIA (p < 0.001) or ORBIT (p < 0.001) in predicting the occurrence of significant bleeding; however, the AUCs for ATRIA vs. ORBIT were statistically similar (p = 0.051).

Comparison of the area under the curve (AUC) for the receiver-operating characteristic curves of the three main models in predicting the occurrence of significant bleeding in patients receiving oral warfarin. ATRIA age > 75 years (0/2) + glomerular filtration rate < 30 mL/min (0/3) + anemia (0/3) + hypertension (0/1) + bleeding history (0/1), CI confidence interval, NBLDSCOR New Bleeding Score (age group < 65 years: 0; 65–74: 1; and ≥ 75 years: 2) + (Rhesus factor positive: 0/Rhesus factor negative: 1) + (estimated glomerular filtration rate ≥ 30 mL/min/1.73 m2: 0/estimated glomerular filtration rate < 30 mL/min/1.73 m2: 3) + (no peptic ulcer disease: 0/peptic ulcer disease: 4) + (hemoglobin level > 12 g/dL in female individuals and > 13 g/dL in male individuals: 0/hemoglobin level ≤ 12 g/dL in female individuals and ≤ 13 g/dL in male individuals: 4) + (no disseminated cancer: 0/disseminated cancer: 5), ORBIT older age (75 + years), reduced hemoglobin, bleeding history, insufficient kidney function, and treatment with antiplatelet drugs, SE standard error
4 Discussion
We found that existing clinical scores poorly predict major bleeding events in patients receiving oral anticoagulant therapy. As such, every effort should be made to address modifiable risk factors for bleeding including a low level of hemoglobin, renal impairment, and concomitant peptic ulcer disease and disseminated cancer in all patients receiving anticoagulation treatment who have a high NBLDSCOR. The new predictive risk model includes age, presence of Rh factor, low hemoglobin, renal impairment, and concomitant peptic ulcer disease and disseminated cancer. To the best of our knowledge, this is the first study comparing risk schemes in patients with supratherapeutic INR.
The recent introduction of simple tools for the estimation of bleeding risk among subjects taking oral anticoagulants has resulted in intensive interest in their comparative statistical performance and clinical utility. In a cohort of patients with AF undergoing anticoagulation, the ATRIA risk score failed to demonstrate significant correlations with clinically relevant bleeding, major bleeding, or death [13]. In another study conducted among patients with AF in USA, it has been proposed that the five-element ORBIT bleeding risk score had a better ability to predict major bleeding when compared with the ATRIA risk score [19]. Similarly, Senoo and colleagues suggest better discrimination with the ORBIT score compared with the ATRIA score for predicting major bleeding, although the difference was not statistically significant [21].
According to our findings, a comparison of bleeding risk schemas revealed that the predictive power of CHADS-Vasc2, ORBIT, and ATRIA scores was 0.50, 0.60, and 0.65 for major bleeding events, respectively. A recent Swedish study yielded a c-index score of 0.68 (0.65–0.70) for ORBIT among 8468 patients [15]. Moreover, in the study by Apostolakis et al. the predictive performances of the ATRIA scheme as reflected by the c-index were 0.50, 0.61, and 0.63 for clinically relevant bleeding, major bleeding, and death, respectively [13]. In contrast, Donzé et al. observed a higher discriminative power for ATRIA compared with the ORBIT score (0.61 vs. 0.56); however, the overall predictive accuracy of the scores was not significantly different from each other (p = 0.84) [12] and all clinical risk scores had a modest predictive value for predicting events. Therefore, clinical applicability and simplicity of the scheme are key considerations over statistical results.
In a large cohort study among 39,539 patients with non-valvular AF, Yao et al. concluded that CHA2DS2-VASc, CHADS2, ORBIT, and ATRIA risk scores had similar performance in predicting major and intracranial bleeding in patients taking non-vitamin K antagonist oral anticoagulants [22]. However, our results illustrated that CHA2DS2-VASc had the lowest performance for predicting major bleeding, which might be attributable to the fact that it has been designated particularly for predicting stroke risk. In a systematic review of the literature confined to AF populations receiving anticoagulation treatment, advanced age, uncontrolled hypertension, ischemic heart disease, cerebrovascular disease, anemia, concomitant antiplatelet therapy, and a previous history of bleeding have been identified as predictors of major bleeding events [24]. Another analysis concluded that labile INR control, advanced age, and concomitant use of aspirin or nonsteroidal anti-inflammatory medications were identified as predictors [25].
In our study, concomitant antiplatelet treatment was not different in patients with and those without significant bleeding. It should be noted that prescriptions can vary over time and do not represent reliable patient characteristics for the estimation of long-term risk. Likewise, a history of hypertension was similar between patients with non-significant and significant bleeding; thus, we did not account for hypertension history. The differences between the NBLDSCOR and the ARTIA score mainly involve the addition of the presence of the Rh factor and histories of peptic ulcer disease and disseminated cancer.
The presence of comorbid diseases, such as renal or hepatic insufficiency, is generally believed to increase the risk of major bleeding during anticoagulation therapy. We observed severe renal disease to be a powerful predictor of hemorrhage risk, consistent with several large cohort studies [20, 26]. However, the strongest predictor of major bleeding in our study was disseminated cancer. Prandoni et al. in 2002 found that patients with cancer are more likely to develop major bleeding during anticoagulant treatment than those without malignancy [27]. Similarly, a Swedish atrial fibrillation cohort study among 182,678 subjects showed that cancer was a significant predictor for major bleeding events [20]. Associations between prevalent cancer and bleeding risk have been speculated to be related to tissue aging, general frailty, and concealed causes of bleeding complications during antithrombotic treatment, probably owing to the mediation of the GDF-15 factor, a marker of cellular aging, cellular growth, oxidative stress, and inflammation [28]. Recently, Hijazi et al. proposed that increased levels of the biomarker GDF-15 were prominently associated with subsequent major bleeding events; thus, it was included in a new suggested bleeding risk score (ABC-bleeding score), which performed better than previous scores such as the ORBIT score [15]. However, because of a lack of data on cTn-hs and GDF-15 values, we could not evaluate its performance among our study population.
Furthermore, this analysis identifies peptic ulcer disease as a potential clinical condition that contributes to major bleeding among patients using anticoagulants. In accordance with this finding, Lee et al. observed a significantly lower incidence of major bleeding, decreasing from 30 to 14%, when oral anticoagulation therapy began after endoscopic confirmation of peptic ulcer healing. Interestingly, we also showed that the presence of Rh antigen was a negative predictor of major bleeding. Despite poor evidence evaluating whether Rh status was associated with major bleeding risk, a Turkish study in 2008 suggested Rh positivity to have an important role in patients with upper gastrointestinal bleeding, which was in contrast with our results [29].
In the current study, sex, education, and concomitant diabetes mellitus, hypertension, and pulmonary diseases failed to demonstrate significant correlations with major bleeding events. Similarly, in the systematic review forming the basis for the UK National Institute for Health and Care Excellence clinical practice guidelines, it has been found that diabetes mellitus, controlled hypertension, and sex are not significant risk factors for bleeding [24]. Thus, the bleeding risk associated with such factors in anticoagulated populations requires further studies. Our study is limited by the lack of information relating to the history of alcoholism, the predisposing genetic factors (i.e., cytochrome P450 2C9), and the presence of a labile INR that have been included in some applicable risk scores in clinical practice such as HEMMORHAGE and HAS-BLED [6, 13, 17, 26].
5 Conclusion
To conclude, among patients taking oral anticoagulants using NBLDSCOR as a simple available score, it was shown to be the strongest predictor of major bleeding compared with existing surrogates of bleeding and stroke risk including CHA2DS2-VASc, ORBIT, and ATRIA scores. However, further prospective studies are needed to validate our findings. Careful assessment and active management of bleeding risk factors may be warranted in all patients taking oral anticoagulants who have a high NBLDSCOR.
References
Hurlen M, Abdelnoor M, Smith P, Erikssen J, Arnesen H. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002;347(13):969–74.
Investigators ESCoBotSI. Stroke prevention with the oral direct thrombin inhibitor ximelagatran compared with warfarin in patients with non-valvular atrial fibrillation (SPORTIF III): randomised controlled trial. Lancet. 2003;362(9397):1691–8.
Ridker PM, Goldhaber SZ, Danielson E, Rosenberg Y, Eby CS, Deitcher SR, et al. Long-term, low-intensity warfarin therapy for the prevention of recurrent venous thromboembolism. N Engl J Med. 2003;348(15):1425–34.
Gurwitz JH, Field TS, Harrold LR, Rothschild J, Debellis K, Seger AC, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289(9):1107–16.
Beyth RJ, Quinn L, Landefeld CS. A multicomponent intervention to prevent major bleeding complications in older patients receiving warfarin: a randomized, controlled trial. Ann Intern Med. 2000;133(9):687–95.
Lip GY, Andreotti F, Fauchier L, Huber K, Hylek E, Knight E, et al. Bleeding risk assessment and management in atrial fibrillation patients: a position document from the European Heart Rhythm Association, endorsed by the European Society of Cardiology Working Group on Thrombosis. Europace. 2011;13(5):723–46.
Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285(22):2864–70.
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263–72.
Fang MC, Go AS, Chang Y, Borowsky LH, Pomernacki NK, Udaltsova N, et al. A new risk scheme to predict warfarin-associated hemorrhage: the ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) Study. J Am Coll Cardiol. 2011;58(4):395–401.
Roldán V, Marín F, Fernández H, Manzano-Fernandez S, Gallego P, Valdés M, et al. Predictive value of the HAS-BLED and ATRIA bleeding scores for the risk of serious bleeding in a “real-world” population with atrial fibrillation receiving anticoagulant therapy. Chest. 2013;143(1):179–84.
Caldeira D, Costa J, Fernandes RM, Pinto FJ, Ferreira JJ. Performance of the HAS-BLED high bleeding-risk category, compared to ATRIA and HEMORR2HAGES in patients with atrial fibrillation: a systematic review and meta-analysis. J Interv Card Electrophysiol. 2014;40(3):277–84.
Donzé J, Rodondi N, Waeber G, Monney P, Cornuz J, Aujesky D. Scores to predict major bleeding risk during oral anticoagulation therapy: a prospective validation study. Am J Med. 2012;125(11):1095–102.
Apostolakis S, Lane DA, Guo Y, Buller H, Lip GY. Performance of the HEMORR2HAGES, ATRIA, and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation: the AMADEUS (Evaluating the Use of SR34006 Compared to Warfarin or Acenocoumarol in Patients With Atrial Fibrillation) Study. J Am Coll Cardiol. 2012;60(9):861–7.
Piccini JP, Fraulo ES, Ansell JE, Fonarow GC, Gersh BJ, Go AS, et al. Outcomes registry for better informed treatment of atrial fibrillation: rationale and design of ORBIT-AF. Am Heart J. 2011;162(4):606–12.e1.
Hijazi Z, Oldgren J, Lindbäck J, Alexander JH, Connolly SJ, Eikelboom JW, et al. The novel biomarker-based ABC (age, biomarkers, clinical history)-bleeding risk score for patients with atrial fibrillation: a derivation and validation study. Lancet. 2016;387(10035):2302–11.
García-Fernández A, Marín F, Roldán V, Galcerá-Jornet E, Martínez-Martínez JG, Valdés M, et al. The HAS-BLED score predicts long-term major bleeding and death in anticoagulated non-valvular atrial fibrillation patients undergoing electrical cardioversion. Int J Cardiol. 2016;217:42–8.
Omran H, Bauersachs R, Rübenacker S, Goss F, Hammerstingl C. The HAS-BLED score predicts bleedings during bridging of chronic oral anticoagulation. Thromb Haemost. 2012;107(01):65–73.
Zhu W, He W, Guo L, Wang X, Hong K. The HAS-BLED score for predicting major bleeding risk in anticoagulated patients with atrial fibrillation: a systematic review and meta-analysis. Clin Cardiol. 2015;38(9):555–61.
Obrien EC, Simon DN, Thomas LE, Hylek EM, Gersh BJ, Ansell JE, et al. The ORBIT bleeding score: a simple bedside score to assess bleeding risk in atrial fibrillation. Eur Heart J. 2015;36(46):3258–64.
Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33(12):1500–10.
Senoo K, Proietti M, Lane DA, Lip GY. Evaluation of the HAS-BLED, ATRIA, and ORBIT bleeding risk scores in patients with atrial fibrillation taking warfarin. Am J Med. 2016;129(6):600–7.
Yao X, Gersh BJ, Sangaralingham LR, Kent DM, Shah ND, Abraham NS, et al. Comparison of the CHA2DS2-VASc, CHADS2, HAS-BLED, ORBIT, and ATRIA risk scores in predicting non-vitamin K antagonist oral anticoagulants-associated bleeding in patients with atrial fibrillation. Am J Cardiol. 2017;120(9):1549–56. https://doi.org/10.1016/j.amjcard.2017.07.051.
Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med. 1998;105(2):91–9.
Hughes M, Lip G. Risk factors for anticoagulation-related bleeding complications in patients with atrial fibrillation: a systematic review. QJM. 2007;100(10):599–607.
Palareti G, Cosmi B. Bleeding with anticoagulation therapy: who is at risk, and how best to identify such patients. Thromb Haemost. 2009;101(2):268–78.
Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am Coll Cardiol. 2011;57(2):173–80.
Prandoni P, Lensing AW, Piccioli A, Bernardi E, Simioni P, Girolami B, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood. 2002;100(10):3484–8.
Wallentin L, Hijazi Z, Andersson U, Alexander JH, De Caterina R, Hanna M, et al. Growth differentiation factor 15, a marker of oxidative stress and inflammation, for risk assessment in patients with atrial fibrillation: insights from the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial. Circulation. 2014;130(21):1847–58.
Bayan K, Tüzün Y, Yılmaz Ş, Dursun M, Canoruc F. Clarifying the relationship between ABO/Rhesus blood group antigens and upper gastrointestinal bleeding. Dig Dis Sci. 2009;54(5):1029–34.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were received for the conduct of this study or the preparation of this article.
Conflict of interest
Leili Pourafkari, Aidin Baghbani-Oskouei, Safa Savadi-Oskouei, Samad Ghaffari, Raziye Parizad, Arezou Tajlil, and Nader D. Nader have no conflicts of interest that are directly relevant to the contents of this article.
Ethics approval
All procedures in this study were in accordance with the 1964 Declaration of Helsinki and the study protocol was reviewed and approved by the Institutional Review Board and Ethics Committee of Tabriz University of Medical Sciences.
Consent to participate
This study was exempted from the informed consent process because of the retrospective design of the study, but all patient data were handled with special care to assure that patient confidentiality was maintained.
Rights and permissions
About this article

Cite this article
Pourafkari, L., Baghbani-Oskouei, A., Savadi-Oskouei, S. et al. Prediction Model for Significant Bleeding in Patients with Supratherapeutic International Normalized Ratio After Oral Administration of Warfarin. Clin Drug Investig 39, 533–542 (2019). https://doi.org/10.1007/s40261-019-00774-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-019-00774-9