
Abstract
Background
Adherence to inhaled medication regimens affects chronic obstructive pulmonary disease (COPD) prognosis and quality of life, and reduces the use of healthcare services, resulting in cost savings.
Objectives
To examine the effects of adherence to inhaled medication regimens on healthcare utilization and costs in high-grade COPD patients.
Methods
We performed an observational retrospective cohort study using a longitudinal data set from the Korean Health Insurance Review and Assessment Service (2008–2013) containing healthcare services’ information for 50 million beneficiaries. The study population was high-grade COPD patients. “Adherent” was defined as a patient attaining a medication possession ratio (MPR) ≥ 80%. We estimated the effects of adherence on the use of intensive care units (ICUs) and emergency rooms (ERs) using a multivariate logistic regression, and estimated the effects on costs (all-cause and COPD-related) using a generalized linear model, with adjustment for patient sociodemographic characteristics, health status, and comorbidities.
Results
Of 9086 high-grade COPD patients, adherence declined from 34.7 to 22.3% over 4 years. Adherence was inversely associated with use of ICUs and costs, and this association got stronger as the adherence period lengthened. Over the 4-year period, the adherent group had a lower likelihood of using ICUs [odds ratio (OR) = 0.74, 95% confidence interval (CI) 0.60–0.91] than the non-adherent group. Similarly, the adherent group had a 10.4% lower all-cause cost (p < 0.001) and an 11.7% lower COPD-related cost (p < 0.0001) versus the non-adherent group.
Conclusions
Adherence reduces healthcare utilization and costs, so adherence is not only clinically effective but also economically efficient. However, less than one-quarter of this population remained adherent over the 4-year period, suggesting that strategies are needed to improve adherence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Adherence to inhaled medications reduced admission to intensive care units and healthcare costs even in high-grade COPD patients. This observational study using a large data set on COPD population in South Korea showed that just less than one-quarter of the high-grade COPD population remained adherent over the 4-year period, suggesting that strategies are needed to improve adherence. |
1 Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of mortality and morbidity. It is projected to be the fourth leading cause of death globally, after ischemic heart disease, cerebrovascular disease, and HIV/AIDS, and seventh in terms of disability-adjusted life years (DALYs) [1]. COPD also confers a significant burden in South Korea, as a chronic health condition; in terms of DALYs, COPD increased sharply, to 5th-ranked in 2010 from 7th position in 2007, in South Korea [2]. A continuing increase in the burden of COPD is expected due to population ageing and changes in smoking patterns [3].
Exacerbations of COPD increase the risk of mortality [4] and the socioeconomic burden is significant among severe COPD patients [5]. Healthcare expenditure among high-grade COPD patients is three times greater than that of non-high-grade patients, and the number of high-grade COPD patients increased by 119.6% for the 5 years from 2006 to 2010, whereas non-high-grade COPD cases increased by 5% in the same period [6].
The condition of COPD cannot be reversed; however, appropriate management of COPD, combining medications and non-medication interventions can control symptoms, slow disease progression, and improve quality of life [7]. Inhaled medications are a crucial element in managing COPD, in which adherence to the treatment regimen can potentially affect disease prognosis and is associated with reduced healthcare use and better survival [8,9,10]. Additionally, medications, when used appropriately, can prevent more expensive healthcare services, such as hospitalization, emergency room (ER) visits, and/or admission to intensive care units (ICUs) [8, 11,12,13,14].
Adherence to medication is generally defined as the extent to which a patient takes medications as prescribed. However, adherence can have an overarching concept, as processes that have to occur for a patient to obtain the optimal benefit from a prescribed treatment regimen. This is sequence of events: (A) initiation, (B) implementation, and (C) persistence [15]. “Initiation” occurs when the patient takes the first dose of a prescribed medication and is typically a binary event whether or not patients start taking their medication. On the other hand, “implementation “is the extent to which a patient’s actual dosing corresponds to the prescribed dosing regimen, from initiation until the last dose is consumed. This is a longitudinal description of patient behavior over time. Lastly, “persistence” is the time elapsed from initiation, until treatment discontinuation. The focus of our manuscript will mostly address “implementation”. Despite the importance of inhaled medications in COPD treatment, with several studies being conducted on adherence and outcomes [8, 11,12,13,14, 16, 17], few have studied long-term adherence among high-grade COPD patients on a national scale. Our study will help to fill the knowledge gap in this area.
The purpose of our study was to investigate the association of medication adherence with health and economic outcomes, particularly for high-grade COPD patients. To our knowledge, this is the first reported observational study on long-term adherence to inhaled medications among high-grade COPD patients using Health Insurance Review and Assessment (HIRA) data: that is, claims data from the Korean National Health Insurance (NHI) scheme. Under the terms of universal health coverage in South Korea, all healthcare providers and citizens are required to join the NHI, which is based on a fee-for-services program with the exception of seven conditions. HIRA data are generated in the process of reimbursing providers under the NHI scheme, and contain relevant information on healthcare services for almost 50 million beneficiaries. These include procedures, surgeries, examinations, and treatments (including prescriptions), as well the socio-demographic characteristics of patients.
We first examined the use of, and adherence to, inhaled medications among high-grade COPD patients. Then, we explored how adherence affected healthcare use in terms of ICU and ER visits, and healthcare service costs (both all-cause and COPD related).
2 Methods
2.1 Data Source and Study Population
We used a longitudinal data set from the HIRA from 2009 to 2013 that contained information pertaining to healthcare services for almost 50 million beneficiaries in South Korea. The data set contained general information, as well as files on healthcare services, diagnoses, and outpatient prescriptions. We obtained information from the general file on patients’ sociodemographic characteristics, such as age, gender, and type of insurance, which is an indirect indicator of socioeconomic status (medical aid vs health insurance), as well as on payers’ payments, and patients’ out-of-pocket payments. We obtained information on treatments, procedures, and prices from the healthcare services file, and information on diagnoses from the diagnosis file. Information about prescriptions—including drug codes, dates of dispensing, days of supply, and unit prices—was retrieved from the health services file for inpatient prescriptions, and from the outpatient prescription file for outpatient prescriptions. These files also identify possible resource utilization sources, such as inpatients, outpatients, ER visits, and ICU admissions. To identify medications by therapeutic class, we linked files with a database, which contained names, manufacturers, and active ingredients for COPD medications, by using drug codes.
The population of interest was high-grade COPD patients aged 40 years or older. We limited our study population to high-grade COPD patients to ensure long-term use of medications for management of COPD. We extracted high-grade COPD patients in two stages. We first identified COPD patients as those who satisfied the following criteria: (1) age ≥ 40 years, (2) a history of ICD-10 codes related to COPD (J43. x–J44.x, except J43.0), and (3) at least two claims for COPD medications, including a long-acting β2 agonist (LABA), a long-acting muscarinic antagonist (LAMA), inhaled corticosteroids (ICS) plus a LABA, a short-acting β2 agonist (SABA), a short-acting muscarinic antagonist (SAMA), a SABA + a SAMA, a systemic β-agonist, or methylxanthine (in 2009). Next, we identified high-grade COPD patients from among the group by applying an operational definition of those who had visited a tertiary hospital for COPD and (1) were prescribed ICS + a LAMA or a LAMA for > 6 months, (2) had at least two prescriptions for systemic steroids with ICS + a LABA, (3) had at least two prescriptions for systemic steroids + a LABA or a LAMA, or (4) had at last two prescriptions for systemic steroids + a LABA and a LAMA prescribed together.
2.2 Use of and Adherence to Inhaled Medication Regimens for COPD
We adopted the medication possession ratio (MPR) to measure the use of inhaled medications. MPR is the proportion of days covered by inhaled medications during the study period. We limited inhaled medications to long-acting inhaled LABA, LAMA, and ICS + LABA (Table 1). The MPRs were calculated according to the index date, defined as the first date of medication prescription in 2009. The MPRs were measured for 1- (365 days), 2- (730 days), 3- (1095 days) and 4-year periods (1460 days).
Adherence was examined as a dichotomous variable, with “adherent” being applied to a patient who attained a specific level of use of inhaled medications. We defined adherence as an MPR ≥ 80%, consistent with literature reports [18,19,20]. The MPR was calculated according to the medication that had the greatest number of days of supply, if multiple COPD medications were in use. Days in hospital were counted as days covered by inhaled medications, assuming that COPD was properly treated while the subject was hospitalized.
2.3 Outcomes and Explanatory Variables
We assessed how adherence to inhaled medication regimens affected health and economic outcomes among high-grade COPD patients. Healthcare use, such as ER visits and ICU use, was examined as a form of health outcome and was limited to COPD-related issues. For economic outcomes, healthcare costs were examined, both all-cause and COPD related.
Explanatory variables included patient sociodemographic characteristics, health risks, and comorbid conditions. Sociodemographic characteristics included age, gender, and eligibility for medical aid. In capturing health risk data, history of hospitalization in the previous year, number of hospitalizations, total number of days in hospital, and number of outpatient visits, were adjusted for. Comorbidities included 13 conditions: ischemic heart disease, lung cancer, osteoporosis, depressive disorder, arthritis, diabetes mellitus, gastroesophageal reflux disease, pneumothorax, congestive heart failure, hypertension, hyperlipidemia, anemia, and metabolic syndrome.
2.4 Statistical Analyses
We first performed descriptive statistics to compare baseline characteristics between the adherent and non-adherent groups. Differences were tested for using Student’s t test for continuous variables and the χ2 test for categorical variables. We estimated associations between adherence to inhaled medication regimens with healthcare utilization and costs using the following:
-
Outcome i = f(Adherence i , Sociodemochar i , healthrisk i , comor i )
-
Outcome i : Patient i ’s ICU admission, ER visit, all-cause cost, and COPD-related cost
-
Adherence i : Patient i ’s adherence (adherent: MPR ≥ 80%, non-adherent: MPR < 80%)
-
Sociodemochar i : Patient i ’s sociodemographic characteristics
-
Healthrisk i : Patient i ’s health risk
-
Comor i : Patient i ’s comorbid conditions
Specifically, we estimated the effects of adherence on ER visits and ICU use by adopting a multivariate logistic regression, and the effects of adherence on costs by adopting a generalized linear model (GLM) with a log link and gamma distribution. The estimation was performed separately for four different periods: 1, 2, 3, and 4 years.
3 Results
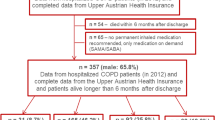
There were 9086 high-grade COPD patients who were followed up for 4 years, accounting for ~ 5% of all COPD patients (Table 2). Of them, 34.6% (n = 3148) were adherent to their inhaled medications. The adherent group showed a higher likelihood of receiving medical aid than the non-adherent group (23.7 vs 17.7%; p < 0.0001); furthermore, 41.6% of the adherent group were hospitalized in the previous year compared with 31.3% of the non-adherent group (p < 0.0001). The average length of stay in hospital was 19.9 days for the adherent group and 11.02 days for the non-adherent group (p < 0.0001). The number of outpatient visits was 7.9 for the adherent group and 3.2 for the non-adherent group (p < 0.0001). The adherent group was more likely to have comorbid conditions than the non-adherent group: 4.2% of the adherent group had ischemic heart disease, compared with 2.9% of the non-adherent group (p < 0.001). Osteoporosis was more prevalent in the adherent (1.5%) than the non-adherent group (1.0%; p < 0.05). The adherent group had a higher rate of depressive disorders and arthritis, but only depression was significantly more prevalent versus the non-adherent group (p < 0.001). Diabetes, pneumothorax, congestive heart failure, and metabolic syndrome were more prevalent in the adherent group, whereas anemia was more prevalent in the non-adherent group (Table 2). The adherent group had 50% higher costs than the non-adherent group. All-cause and COPD-related healthcare costs for the adherent group were US$3087 and US$2851, respectively, whereas they were US$1998 and US$1804, respectively, for the non-adherent group (Table 2).
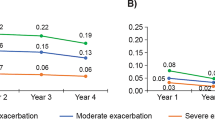
Among high-grade COPD patients, MPR and the percentage who were adherent to their inhaled medication regimens decreased over time (Fig. 1). For the 1-year period, the MPR was 58%, equivalent to medication use on 212 of 365 days and this decreased to 52.6% for the 2-year period, 48.4% for the 3-year period, and 45.5% for the 4-year period. The percentage of those adherent to their inhaled medications also declined over time. Specifically, 34.7% of high-grade COPD patients were adherent to inhaled medications for the 1-year period and this decreased continuously; to 28.1% for the 2-year period, 24.4% for the 3-year period, and only 22.3% over the 4-year period.

Medication possession ratio (MPR) and percentage in the adherent group
Adherence to inhaled medications was associated with reduced ICU use and this inverse association became stronger and statistically significant as the period of adherence lengthened (Table 3). Compared with non-adherent patients, the adherent group had 0.96 and 0.86 times the likelihood of being admitted to the ICU over the 1- and 2-year periods, respectively, although the differences were not statistically significant. However, this association became significant for the 3- (OR 0.71, 95% CI 0.67–0.88) and 4-year periods (OR 0.74, 95% CI 0.60–0.91). Unlike ICU use, we did not find an inverse association between medication adherence and a visit to ER. For the 1-year period, the adherent group had a 0.94 likelihood of visiting the ER than the non-adherent group, which was a statistically insignificant difference. However, the likelihood of visiting the ER became greater after 2 years of adherence: the adherent group had 1.32 times odds of visiting the ER (95% CI 1.14–1.53) for the 2-year period, a 1.39 times odds (CI 1.25–1.63) for the 3-year period, and 1.43 times odds (95% CI 1.25–1.30) for the 4-year period versus the non-adherent group.
Adherence to inhaled medications was associated with decreased healthcare costs and the extent of the decrease increased as the adherence period lengthened (Table 4). Compared with those in the non-adherent group, all-cause healthcare costs in the adherent group were significantly higher, at 14.4% for the 1-year period (p < 0.0001) and 8.4% for the 2-year period (p < 0.01). However, costs in the adherent group became lower than those in the non-adherent group from the 3-year period. All-cause costs for the adherent group were 5.2% for the 3-year period and 10.4% for the 4-year period lower than the costs for the non-adherent group (both p < 0.001). A similar trend was found for COPD-related costs. COPD-related costs decreased as the adherence period lengthened. For the 1-year and 2-year periods, COPD-related costs in the adherent group were greater than those in the non-adherent group, but the difference was statistically insignificant. However, the costs were 4.05% and 11.71% lower among the adherent patients for the 3-year and 4-year periods, respectively, versus the non-adherent patients.
4 Discussion
Appropriate use and adherence to medication regimens can prevent the use of non-medication healthcare service, such as ER and ICU visits and hospitalization, which are usually resource-intensive; thus, use of medication may result in cost savings for COPD treatment. Our study investigated this hypothesis empirically using HIRA data and showed mixed findings compared with existing studies [8, 11]. Adherence to inhaled medications reduced ICU use in the context of the 3-year period. The inverse relationship between medication use and ICU use grew stronger as the adherence period lengthened. Despite a poorer health status of adherent versus non-adherent patients, a reduction in ICU use indicates that adherence may be effective in delaying the progression of, and/or for managing, COPD. Moreover, adherence to inhaled medications reduced all-cause and COPD-related costs. The reduction in costs was statistically significant when the adherence period was long enough, and the magnitude of savings became larger as the adherence period became longer. This indicates that adherence had a positive effect in terms of preventing deterioration of the condition, thereby lowering the use of expensive healthcare services, such as ICUs, leading to cost reductions.
However, we did not find that adherence was associated with fewer ER visits, unlike some previous studies [11, 14]. The reasons for this are unclear, but there are several possibilities. The healthcare system in South Korea has a low barrier for patient access to ERs. Adherent patients, who would likely be more health conscious, may seek more healthcare services when they experience a symptom even if it is controllable or mild. However, ICU admission is via ERs or as an inpatient, when the patient’s condition has deteriorated seriously. Alternatively, adherent patients may have more frequent ER visits due to exacerbations of COPD or complications caused by the comorbid conditions that are more prevalent among them. Nonetheless, reductions in costs among adherent patients suggests that the overall savings from being adherent to inhaled medications are large enough to offset any increase in ER visits.
Adherence to COPD medications reduces exacerbations, mortality, and the use of resource-intensive healthcare services, and improves quality of life [8, 11, 21]. The reduction in healthcare utilization leads to healthcare cost savings, and this has important implications for a healthcare system as a whole. Current healthcare programs are challenged with respect to sustainability because of rising healthcare expenditure due to an aging population, innovations in medical technologies, and changing treatment thresholds. Adherence to medication regimens can be cost efficient and clinically effective for treating COPD [22].
In our study, we observed suboptimal adherence to inhaled medications among high-grade COPD patients, and this adherence declined gradually as the observation period was extended. Indeed, only 22.3% of this population was adherent over the 4-year period, so 65–80% of high-grade COPD patients were not adhering to their inhaled medication regimens, which are an essential part of COPD treatment. Adherence to inhaled medications is lower than that for oral medications [23]. This lower rate may be related to the use of inhalers, which is a concern in the treatment of COPD, where the use of inhaled medications is increasingly advised. Patients tend not to prefer inhalers due to unease regarding use and the inconvenience of carrying one, which may be worsened by the introduction of additional inhalers with increased complexity [24, 25]. Inhalers are also relatively expensive versus oral medications, so patients may face a higher financial burden.
Our study had some limitations. The use of inhaled medications and adherence may have been overestimated, because we measured the use of medications with MPR and there is no guarantee that patients consumed the inhaled medications even if they possessed them. Furthermore, it is unknown whether the medication was correctly taken, i.e. good inhaler technique. Additionally, the MPR was calculated according to the medication that had the greatest number of days of supply, if multiple medications were in use. Information such as pulmonary function test results, Saint George’s Respiratory Questionnaire, COPD Assessment Test, and modified Medical Research Council Dyspnea Scale, and smoking history were not available in our data; thus, we cannot rule out the possibility of incomplete control of the severity of COPD. Lastly, medical cost of deceased patients during the follow up would be underestimated. Some patients may have high healthcare use within first 1–2 years and then died at some point.
Despite these limitations, this is the first reported observational study on adherence to inhaled medication regimens in high-grade COPD patients, with a follow-up of up to 4 years and using HIRA real-world data. Studying adherence using HIRA data has an advantage over clinical trials because the data reflect real-world clinical practices. Adherence rates of 70–90% in clinical trials [26,27,28] tend to be higher than those in clinical practice, which are 10–40% [29,30,31]. Our study confirmed this difference: adherence rates of 22.3–34.7% in our study differ significantly from the 79.8% reported in one representative clinical trial of COPD [8]. These differences in adherence rates are the result of various factors in clinical trials. These include regular monitoring which enhances patient adherence to the prescribed regimen (the Hawthorne effect [32]), availability of free medications which eliminates financial barriers, frequent contact between the patient and the trial site which reinforces adherence, and the possibility of selection bias when enrolling patients in the study. Regular clinical practice is quite unlike a clinical trial. Findings from real-world data can be more practical and reliable for clinical application. The use of HIRA data also allows for larger samples, per the present study, which may have been very close to the total high-grade COPD population of South Korea (because the data included claims from all individual beneficiaries in South Korea over the course of treatment from birth to death).
Our study is valuable in that it provided good evidence for the importance of inhaler adherence. Better policy and more interventions that focus on improving inhaler adherence in COPD are definitely needed. In Europe, for example, this has recently been advocated [33]. However, unfortunately, there has been no such a movement in Asia. Not only for the policy, but interventions are also needed. Recently, using advanced technique can help to increase adherence. Electronic audio recording device can be very useful to objectively assess adherence to inhalers in COPD patients [34]. Moreover, electronic monitoring devices can also be useful to monitor adherence [35].
5 Conclusions
Adherence to inhaled medications reduced healthcare utilization and costs. The finding from our study, involving real-world data, has important implications for clinicians and policy makers. Adherence to inhaled medications that are an essential part of COPD treatment regimens results in cost savings due to reduced use of cost-intensive healthcare services in high-grade COPD patients. Adherence is not only clinically effective, but also economically efficient. However, less than one-quarter of high-grade COPD patients remained adherent during the 4-year period, suggesting that new strategies are needed to improve adherence in this population.
References
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442.
Oh IH, Yoon SJ, Kim EJ. The burden of disease in Korea. Healthcare Policy. 2011;54(6):646–52.
Yoon HK, Park YB, Rhee CK, Lee JH, Oh YM; Committee of the Korean COPD Guideline 2014. Summary of the Chronic Obstructive Pulmonary Disease Clinical Practice Guideline Revised in 2014 by the Korean Academy of Tuberculosis and Respiratory Disease. Tuberc Respir Dis (Seoul). 2017;80(3):230–40.
Jensen HH, et al. Potential misclassification of causes of death from COPD. Eur Respir J. 2006;28(4):781–5.
Jensen MB, et al. Chronic obstructive pulmonary disease involves substantial health-care service and social benefit costs. Dan Med J. 2013;60(1):A4557.
Kim J, et al. The health care burden of high grade chronic obstructive pulmonary disease in Korea: analysis of the Korean Health Insurance Review and Assessment Service data. Int J Chron Obstruct Pulmon Dis. 2013;8:561–8.
Restrepo R, et al. Medication adherence issues in patients treated for COPD. Int J Chron Obstruct Pulmon Dis. 2008;3:371–84.
Vestbo J, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–43.
Antoniu S. Adherence to inhaled therapy in COPD: effects on survival and exacerbations. Expert Rev Pharmacoecon Outcomes Res. 2010;10:115–7.
Asche C, et al. Adherence to current guidelines for chronic obstructive pulmonary disease (COPD) among patients treated with combination of long-acting bronchodilators or inhaled corticosteroids. Int J Chron Obstruct Pulmon Dis. 2012;7:201–9.
Toy EL, et al. Treatment of COPD: relationships between daily dosing frequency, adherence, resource use, and costs. Respir Med. 2011;105(3):435–41.
Simoni-Wastila L, et al. Association of chronic obstructive pulmonary disease maintenance medication adherence with all-cause hospitalization and spending in a medicare population. Am J Geriatr Pharmacother. 2012;10(3):201–10.
Ismaila A, et al. Impact of adherence to treatment with tiotropium and fluticasone propionate/salmeterol in chronic obstructive pulmonary diseases patients. Curr Med Res Opin. 2014;30(7):1427–36.
Butler RJ, et al. Effects of nonadherence with prescription drugs among older adults. Am J Manag Care. 2011;17(2):153–60.
Vrijens B, et al. What we mean when we talk about adherence in respiratory medicine. J Allergy Clin Immunol Pract. 2016;4(5):802–12.
Halpern R, et al. Outcomes associated with initiation of tiotropium or fluticasone/salmeterol in patients with chronic obstructive pulmonary disease. Patient Prefer Adherence. 2011;5:375–88.
van Boven JF, et al. Clinical and economic impact of non-adherence in COPD: a systematic review. Respir Med. 2014;108(1):103–13.
Avorn J, et al. Persistence of use of lipid-lowering medications: a cross-national study. J Am Med Assoc. 1998;279(18):1458–62.
Benner JS, et al. Long-term persistence in use of statin therapy in elderly patients. J Am Med Assoc. 2002;288(4):455–61.
Dor A, Encinosa W. How does cost sharing affect drug purchases? Insurance regimes in the private market for prescription drugs. Cambridge: National Bureau of Economic Research; 2004.
Takemura M, et al. Relationships between repeated instruction on inhalation therapy, medication adherence, and health status in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2011;6:97–104.
van Boven JF, et al. Enhancing respiratory medication adherence: the role of health care professionals and cost-effectiveness considerations. J Allergy Clin Immunol Pract. 2016;4(5):835–46.
Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63(9):831–8.
Delea TE, et al. Effects of fluticasone propionate/salmeterol combination on asthma-related health care resource utilization and costs and adherence in children and adults with asthma. Clin Ther. 2008;30(3):560–71.
Yu AP, et al. Therapy persistence and adherence in patients with chronic obstructive pulmonary disease: multiple versus single long-acting maintenance inhalers. J Med Econ. 2011;14(4):486–96.
van Grunsven PM, et al. Compliance during long-term treatment with fluticasone propionate in subjects with early signs of asthma or chronic obstructive pulmonary disease (COPD): results of the Detection, Intervention, and Monitoring Program of COPD and Asthma (DIMCA) Study. J Asthma. 2000;37(3):225–34.
Rand CS, et al. Long-term metered-dose inhaler adherence in a clinical trial. The Lung Health Study Research Group. Am J Respir Crit Care Med. 1995;152(2):580–8.
Kesten S, et al. Compliance with tiotropium, a once daily dry powder inhaled bronchodilator, in 1 year COPD trials. Chest. 2000;118(4):191S–191S.
Bender BG, Pedan A, Varasteh LT. Adherence and persistence with fluticasone propionate/salmeterol combination therapy. J Allergy Clin Immunol. 2006;118(4):899–904.
Breekveldt-Postma NS, et al. Persistence with inhaled corticosteroid therapy in daily practice. Respir Med. 2004;98(8):752–9.
Krigsman K, Nilsson JLG, Ring L. Adherence to multiple drug therapies: refill adherence to concomitant use of diabetes and asthma/COPD medication. Pharmacoepidemiol Drug Saf. 2007;16(10):1120–8.
Landsberger HA. Hawthorne Revisited: Management and the Worker, Its Critics, and Developments in Human Relations in Industry. Ithaca, NY: Cornell University; 1958.
van Boven JFM, Lavorini F, Dekhuijzen PNR, Blasi F, Price DB, Viegi G. Urging Europe to put non-adherence to inhaled respiratory medication higher on the policy agenda: a report from the First European Congress on Adherence to Therapy. Eur Respir J. 2017;49(5):1700076.
Sulaiman I, et al. Objective assessment of adherence to inhalers by patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(10):1333–43.
Taylor TE, Zigel Y, De Looze C, Sulaiman I, Costello RW, Reilly RB. Advances in Audio-Based Systems to Monitor Patient Adherence and Inhaler Drug Delivery. Chest. 2017. https://doi.org/10.1016/j.chest.2017.08.1162.
Acknowledgements
This study was conducted as a part of the project “Trends in medication utilization and adherence to medication among patients with chronic conditions: the case of COPD” by HIRA.
Author information
Authors and Affiliations
Contributions
J-AK contributed to the study concept and design, acquisition, analysis and interpretation of data for the study, drafted and revised the manuscript critically for important intellectual content, and provided statistical expertise. MKL contributed to the interpretation of the data for the study and revised the manuscript critically for important intellectual content. KK contributed to the interpretation of data for the study and revised the manuscript critically for important intellectual content. J-HP contributed to the data analysis for the study and revised the manuscript critically for important intellectual content. CKR contributed to the study concept and design, and interpretation of the data for the study and revised the manuscript critically for important intellectual content. All authors approved the final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Ethics Committee of Seoul St. Mary’s Hospital approved the present study. The requirement for informed consent from the patients studied was waived by the ethical review board by Seoul St. Mary’s Hospital, the Catholic University of Korea.
Conflict of Interest
CK Rhee received consulting/lecture fees from MSD, AstraZeneca, Novartis, GSK, Takeda, Mundipharma, Sandoz, Boehringer-Ingelheim, and Teva-Handok. Other authors have no competing interests to disclose.
Funding
No funding was provided for this study.
Rights and permissions
About this article

Cite this article
Kim, JA., Lim, M.K., Kim, K. et al. Adherence to Inhaled Medications and its Effect on Healthcare Utilization and Costs Among High-Grade Chronic Obstructive Pulmonary Disease Patients. Clin Drug Investig 38, 333–340 (2018). https://doi.org/10.1007/s40261-017-0612-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-017-0612-2