
Abstract
Background
Serplulimab is a novel, recombinant, humanized, monoclonal, anti-programmed death 1 antibody with a similar or better affinity and pre-clinical antitumor activity than pembrolizumab and nivolumab.
Objective
This phase I, open-label, dose-escalation study evaluated serplulimab in patients with advanced solid tumors. The second interim analysis of the dose-finding phase is reported here.
Methods
Adult patients with histologically confirmed metastatic/recurrent solid tumors who had progressed on, or were intolerant to/clinically unsuitable for standard treatment, were enrolled. Four intravenous serplulimab dose levels were evaluated: 0.3, 1.0, 3.0, and 10.0 mg/kg every 2 weeks in 28-day cycles for up to 2 years. Primary endpoints were the incidence of treatment-emergent adverse events and the maximum tolerated dose.
Results
By 27 July, 2020 (data cut-off), 29 patients with stage IV disease (34.5% with lung cancer) received one or more doses of serplulimab. One (3.4%) patient had completed treatment and 26 (89.7%) had discontinued from the study. The maximum tolerated dose was not reached. Twenty-two (75.9%) patients experienced treatment-emergent adverse events related to serplulimab, most frequently nausea (24.1%), with no notable differences in incidence between dose cohorts; of these, grade ≥ 3 events occurred in four (13.8%) patients. Pharmacokinetic data demonstrated minimal accumulation of serplulimab after repeated administration. Functional programmed death 1 blockade was observed across dose levels. Objective response and disease control rates were 8.0 and 60.0%, respectively.
Conclusions
Serplulimab was well tolerated and demonstrated antitumor activity. These data support further study of serplulimab in larger patient populations.
Clinical Trial Registration
ClinicalTrials.gov NCT03468751 (19 March, 2018).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Serplulimab, a novel anti-programmed death 1 monoclonal antibody, was well tolerated at doses of 0.3–10.0 mg/kg every 2 weeks; preliminary efficacy findings indicated encouraging antitumor activity. Results from the current study warrant further investigation of serplulimab in larger patient cohorts. |
Serplulimab has been approved by the China National Medical Products Administration for the treatment of microsatellite instability-high solid tumors, squamous non-small cell lung cancer, and extensive-stage small cell lung cancer. More clinical trials in various tumor types are being conducted, aiming to benefit a broader patient population. |
1 Introduction
The development of immune checkpoint inhibitors has driven dramatic advancements in cancer treatment over recent decades [1, 2]. Blockade of the programmed death 1 (PD-1) pathway by these agents has been shown to confer prolonged overall survival (OS) and reduced toxicity compared with traditional chemotherapies in a variety of solid tumors [3,4,5,6,7]. Despite the approval of multiple PD-1/programmed death ligand 1 (PD-L1) inhibitors for the treatment of cancers, the efficacy and safety of these approved anti-PD-1/PD-L1 agents vary in different diseases [8,9,10]. In the context of non-small-cell lung cancer, pembrolizumab plus chemotherapy significantly improved progression-free survival (PFS) and OS [11, 12], while a combination of nivolumab with an anti-cytotoxic T-lymphocyte antigen 4 antibody was necessary to confer survival benefits [13]; PD-L1 inhibitors such as durvalumab improved PFS and OS but to a lower extent, or required a combination with a cytotoxic T-lymphocyte antigen 4 inhibitor [14]. Whereas in small cell lung cancer, pembrolizumab [15] and nivolumab [16, 17] both failed to improve OS; only two PD-L1 inhibitors, atezolizumab [18] and durvalumab [19], were approved for extensive-stage small cell lung cancer. Furthermore, the improved survival benefits remained unsatisfactory for certain indications such as extensive-stage small cell lung cancer; the approved atezolizumab and durvalumab regimens extended median OS by only around 2 months. Despite the many available options, the discrepancy in regulatory approvals in various geographical regions and the relatively high cost of treatment render these anti-PD-1/PD-L1 agents largely unaffordable or unavailable to most of the world’s population. Coupled with the room for further improvement in the clinical benefits seen with these immune checkpoint inhibitors, there is a need for alternative options that can increase the patients’ accessibility to effective treatments.
Serplulimab (formerly HLX10) is a novel, recombinant, humanized, anti-PD-1 IgG4 monoclonal antibody. Serplulimab possesses a unique mode of PD-1 receptor recognition and has a higher affinity for human PD-1 than both pembrolizumab and nivolumab (KD 2.42 nM vs 8.04 nM vs 11.9 nM) [20, 21]. In pre-clinical studies, serplulimab demonstrated potent antitumor activity in vivo, which was at least as good as that observed with pembrolizumab and nivolumab. In addition, serplulimab was well tolerated in cynomolgus monkeys [20].
The safety and tolerability of serplulimab are being assessed in patients with advanced or metastatic solid tumors who were refractory to standard therapy, in a multicenter, prospective, phase I, open-label study (NCT03468751). At a previous analysis, serplulimab was found to be well tolerated, with promising signs of antitumor efficacy, including durable responses in several types of malignancy; the pharmacokinetic characteristics of serplulimab were similar to those reported for pembrolizumab and nivolumab [22]. Here, we present the findings of the second interim analysis.
2 Methods
2.1 Patients and Study Design
The dose-finding phase of this open-label, phase I, dose-escalation study was conducted at four sites in Taiwan. Eligible patients were adults (age ≥ 18 years) with histologically confirmed, measurable or evaluable advanced or metastatic solid tumors that were refractory to, intolerant to, or deemed clinically unsuitable for standard treatment, or had locally advanced disease that was not amenable to localized therapy. Other key inclusion criteria were Eastern Cooperative Oncology Group performance status ≤ 2 and adequate organ function. Patients with unresolved grade ≥ 2 toxicities from prior therapies, or unstable or uncontrolled medical conditions were excluded. A full account of the study eligibility criteria is provided in the Electronic Supplementary Material (ESM).
The study comprised a dose-finding and a dose-expansion phase. An adaptive Bayesian optimal interval trial design [23] was adopted to determine the rule of dose finding and the maximum tolerated dose (MTD) of serplulimab (Fig. e1 and Methods of the ESM). Four serplulimab dose levels were planned for evaluation (0.3, 1.0, 3.0, and 10.0 mg/kg), administered intravenously every 2 weeks (Q2W) on day (D)1 and D15 of each 28-day cycle (C). The MTD was to be selected at trial completion based on isotonic regression (target toxicity rate of 30%; Table e1 of the ESM). Treatment with serplulimab continued at the assigned dose level for a maximum of 2 years, or until progressive disease, withdrawal from the study, or death (whichever occurred first). Patients were followed for a minimum of 90 days after the last dose of serplulimab. For patients who experienced progressive disease and had not received additional anticancer therapy during the follow-up period, an option to re-initiate serplulimab treatment (at the same dose level) for another 12 months was given, provided that the study eligibility criteria and submission of a baseline tumor assessment (within 6 weeks prior to re-initiation of serplulimab treatment) were fulfilled.
The study was conducted in accordance with the principles of the Declaration of Helsinki, Good Clinical Practice guidelines, and local regulatory requirements. The study protocol, any amendments, and informed consent were approved by a central or independent institutional review board/ethics committee at participating sites. All patients provided written informed consent to participate prior to screening and enrollment.
2.2 Study Endpoints and Assessments
Primary endpoints were the number and proportion of patients with treatment-emergent adverse events (TEAEs) and identification of the MTD. All adverse events were monitored from the time of the first dose of serplulimab up to 90 days after the last dose. Adverse events were coded using Medical Dictionary for Regulatory Activities version 22.0 and graded for severity using National Cancer Institute Common Terminology Criteria for Adverse Events version 4.03. Adverse events that were considered either probably or possibly related to serplulimab were recorded as treatment-related adverse events (TRAEs).
Secondary endpoints were serum serplulimab pharmacokinetic parameters, immunogenicity, preliminary efficacy, pharmacodynamics of serplulimab, and potential predictive and prognostic biomarkers. The blood sampling schedule for the measurements of pharmacokinetic parameters and serplulimab anti-drug antibodies (ADAs) was provided in Table e2 of the ESM. Serplulimab ADAs were assessed by an electrochemiluminescence immunoassay (Frontage Laboratories, Inc., Exton, PA, USA). Efficacy endpoints included objective response rate (ORR), disease control rate, time to response, duration of response, and PFS; definitions are provided in Table e3 of the ESM. Tumor response was assessed by the investigator per Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1) and immune-based RECIST, or modified RECIST for patients with hepatocellular carcinoma (HCC) [24,25,26]. Tumor assessments were conducted every 8 weeks for the first 24 weeks, and every 12 weeks thereafter.
Programmed death 1 receptor occupancy on circulating CD3+ T cells was measured using flow cytometry (FACSCanto II Flow Cytometer; BD Biosciences, San Jose, CA, USA) and ex vivo interleukin-2 release was measured by an enzyme-linked immunosorbent assay (Human IL-2 ELISA Max Deluxe; BioLegend, San Diego, CA, USA). Tumor expression of PD-L1 was assessed by immunohistochemistry using fresh or archival (harvested ≤ 6 months before the first dose of serplulimab) tumor biopsy specimens, by three different assays: PD-L1 IHC 22C3 pharmDx (Agilent Technologies, Santa Clara, CA, USA), VENTANA PD-L1 SP142, and VENTANA PD-L1 SP263 (Roche Diagnostics, Mannheim, Germany). The same tumor biopsy samples were used to evaluate the immunohistochemistry staining patterns on tumor cells of the DNA mismatch repair proteins MLH1, MSH2, PMS2 (Agilent Technologies), and MSH6 (Epitomics, Burlingame, CA, USA). Microsatellite instability (MSI) status was assessed in tumor and blood samples using the MSI Analysis System, version 1.2 (Promega, Madison, WI, USA). All biomarker assessments were conducted at a central laboratory.
2.3 Statistical Analyses
The maximum sample size for the dose-finding cohort was 30, with no more than ten cohorts (n = 3 per cohort). The trial would be terminated once the number of patients treated at a current dose reached 15. Statistical power was not employed to determine the maximum sample size.
Safety, immunogenicity, PFS, and biomarker data were evaluated in the all-treated population. Other efficacy endpoints and pharmacokinetics were analyzed using data from the response-evaluable set and pharmacokinetics data set, respectively; and pharmacodynamics were analyzed using the exploratory pharmacodynamic data set. Definitions of all analysis populations are provided in Table e4 of the ESM. The Kaplan–Meier method was used to analyze time-to-event variables; two-sided 95% confidence intervals (CIs) were calculated for medians using the Brookmeyer–Crowley method. Survival rates at specific timepoints were derived from Kaplan–Meier estimates with corresponding two-sided 95% CIs derived based on Greenwood’s formula. All data analysis outputs were produced using Statistical Analysis Software version 9.2 or later. The present interim analysis was implemented after at least 15 patients had received serplulimab 10.0 mg/kg Q2W.
3 Results
3.1 Patients
As of the data cut-off for this interim analysis (27 July, 2020), 49 patients were screened, and 29 were enrolled and received at least one dose of serplulimab (0.3 mg/kg, n = 3; 1.0 mg/kg, n = 4; 3.0 mg/kg, n = 6; 10.0 mg/kg, n = 16; Fig. e2 of the ESM). One (3.4%) patient had completed treatment and 26 (89.7%) had discontinued from the treatment; two (6.9%) patients remained on treatment. The most common reason for treatment discontinuation was adverse events (n = 8, 27.6%). The all-treated population and the pharmacokinetic data set included all 29 patients, the exploratory pharmacodynamic data set included 28 patients, and the response-evaluable set included 25 patients (Table e4 of the ESM).
Demographic and baseline characteristics were balanced among the four dose cohorts (Table 1). All patients had stage IV disease at baseline, and most (n = 23, 79.3%) had metastatic disease. The most common primary tumor location was the lung (n = 10, 34.5%). All patients had received at least one line of chemotherapy; one patient in the 3.0-mg/kg cohort, and one patient in the 10-mg/kg cohort received previous immunotherapy in the form of aldesleukin (a recombinant interleukin-2), and nivolumab, respectively. More than 58% of patients had received first, second, or third lines of treatment.
3.2 Safety and Tolerability
The mean ± standard deviation duration of serplulimab exposure and cumulative dose across the dose cohorts was 14.8 ± 12.9 weeks and 3122.8 ± 3807.9 mg, respectively. The mean relative dose intensity was similar across the four dose cohorts (0.3, 1, 3, and 10 mg/kg), at 97.2, 100, 100.9, and 96.7%, respectively.
A summary of TEAEs (overall and by dose cohort) is provided in Table e5 of the ESM; a list of the most commonly occurring TEAEs is provided in Table 2. A total of 28 (96.6%) patients experienced at least one TEAE, with no notable differences between the four dose cohorts. The most common TEAEs overall were decreased appetite (n = 12, 41.4%) and fatigue (n = 9, 31.0%). Among the grade ≥ 3 TEAEs reported in 15 (51.7%) patients, only anemia occurred in more than two patients (n = 3, 10.3%). Treatment-emergent adverse events led to death in five (17.2%) patients and to treatment discontinuation in ten (34.5%) patients. Serious adverse events occurred in 20 (69.0%) patients.
Twenty-two (75.9%) patients experienced TRAEs, with no notable differences in incidence between the dose cohorts (Table e5 of the ESM). The most frequently occurring were nausea (n = 7, 24.1%) and fatigue (n = 6, 20.7%). Treatment-related adverse events led to treatment discontinuation in two (6.9%) patients. Treatment-related adverse events were predominantly mild in severity; all of these 22 (75.9%) patients reported grade 1–2 TRAEs, while grade 3–4 and grade 5 TRAEs were reported for four (13.8%) and two (6.9%) patients, respectively. Treatment-related adverse events leading to death were thrombocytopenia in one patient (1.0-mg/kg cohort), and acute pancreatitis, myocarditis, sepsis, acute cholangitis, and acute hepatitis in the other patient (3.0-mg/kg cohort).
Five (17.2%) patients overall reported at least one immune-related adverse event (irAE), one of whom experienced grade ≥ 3 events (3.0-mg/kg cohort). Pruritus and pyrexia were the only irAEs that occurred in more than one patient (n = 2, 6.9% for each; Table e6 of the ESM). The MTD was not reached by the data cut-off.
3.3 Efficacy
Two (8.0%) patients achieved a partial response, one with malignant melanoma in the 3.0-mg/kg cohort and another with HCC in the 10.0-mg/kg cohort; there were no complete responses (CRs), and 13 (52.0%) patients had stable disease. The ORR and disease control rate were therefore 8.0 and 60.0%, respectively (Table 3). Time to response and duration of response were 1.8 months (56 days) and 6.5 months (197 days), respectively, for the patient in the 3.0-mg/kg cohort, and 8.3 months (253 days) and 2.8 months (85 days), respectively, for the patient (patient was still in response at the last tumor assessment) in the 10.0-mg/kg cohort. Best percentage reduction in tumor size for the two patients who achieved partial response was 42% (HCC) and 45% (malignant melanoma). The change from baseline in target lesion size over time is shown in Fig. 1.

Percentage change from baseline in tumor burden over time (response-evaluable set)
At the time of this interim analysis, 21 (72.4%) patients in the all-treated population had either experienced progressive disease or had died, with a median PFS of 3.5 months (107.0 days, 95% CI 58.0–170.0; Fig. e3 of the ESM). Median PFS was 1.7 months (51.0 days, 95% CI 39.0–107.0) in the 0.3-mg/kg cohort, 2.7 months (81.5 days, 95% CI 53.0–110.0) in the 1.0-mg/kg cohort, 3.8 months (114.5 days, 95% CI 38.0–not evaluable) in the 3.0-mg/kg cohort, and 3.8 months (117.0 days, 95% CI 54.0–232.0) in the 10.0-mg/kg cohort. Kaplan–Meier estimates of PFS at 3, 6, and 9 months were 51.4, 30.0, and 15.0%, respectively.
3.4 Pharmacokinetics and Immunogenicity
Summaries of key pharmacokinetic parameters by dose cohort after single administration (C1D1) and repeated administration (C3D1; steady state) are provided in Tables e9 and e10 of the ESM. Serplulimab serum concentration increased with increasing dose, peaking at the end of or shortly after the infusion and decreasing gradually thereafter. Concentrations remained above the lower limit of quantitation for all patients through D15 for all doses (Fig. 2a). Steady state was reached by the fifth infusion (Fig. 2b). Exposure to serplulimab after the first administration, as reflected by area under the concentration–time curve from time 0 to infinity and maximum concentration, increased in a generally dose-proportional manner (Fig. 2c). The pharmacokinetic profile of serplulimab showed a slow rate of clearance and a low volume of distribution at both C1D1 and C3D1. Elimination half-life was 118.9–180.4 h and 134.5–234.9 h at C1D1 and C3D1, respectively. The accumulation ratio based on maximum concentration and on the area under the concentration–time curve at steady state was low and generally consistent across the dose levels (geometric mean 1.2–1.5 and 1.2–2.0, respectively), indicating minimal accumulation of serplulimab after the administration of multiple doses.

Serum concentration–time profiles of serplulimab a after the first administration (cycle 1, day 1, linear and semi-logarithmic scales) and b at steady state (cycle 3, day 1, linear and semi-logarithmic scale), and c dose proportionality of serplulimab after the first administration (pharmacokinetic data set). Symbols and error bars indicate the mean ± standard deviation. AUC0–inf area under the concentration–time curve from time 0 to infinity, C1D1 day 1 of cycle 1, C3D1 day 1 of cycle 3, Cmax maximum concentration, h hours
Of the 29 patients in the all-treated population, one (3.4%) patient (esophageal squamous cell carcinoma, 0.3-mg/kg cohort) developed serplulimab ADAs. Positive ADA test results were recorded for that patient from C2D1 to C6D1 and at the follow-up visit 1, with a titer range of 60–480. At C3D1, the pharmacokinetic parameters for this ADA-positive patient were substantially lower than that for their ADA-negative counterparts in the 0.3-mg/kg cohort.
3.5 Potential Biomarkers
As assessed by DNA mismatch repair, one of the 29 patients (HCC, 10-mg/kg cohort) in the all-treated population showed a loss of nuclear expression on both MSH2 and MSH6, indicating an mismatch repair germline mutation; Lynch syndrome was suspected, and was interpreted as being MSI-high. This patient was one of the two who achieved a partial response. Based on the MSI status assessed by the Promega MSI Analysis System, one (3.4%) patient had MSI-low (MSI-L) tumor cells (0.3 mg/kg cohort) and 21 (72.4%) patients were MSI stable (Table e7 of the ESM). Rates of PD-L1 positivity varied from 13.8% to 31.0% according to the PD-L1 detection assay used; the highest rate was obtained with the PD-L1 IHC 22C3 pharmDx assay (Table e7 of the ESM). The two patients who achieved a partial response were PD-L1 negative according to all three PD-L1 detection assays. No association was found between biomarker expression and the best percentage change from baseline in tumor burden (Fig. 3).

Best percentage change from baseline in target lesion size according to biomarkers a microsatellite instability, b mismatch repair, and c programmed death ligand 1 (PD-L1) [all-treated population]. One patient in the 3.0-mg/kg cohort and two patients in the 10.0-mg/kg cohort died prior to their first post-baseline tumor assessment, and thus there were no data on best percentage change from baseline in target lesion size to report. One patient in the 3.0-mg/kg cohort did not have biomarker assessments, and thus was not plotted on the graphs; the best percentage change from baseline in target lesion size for this patient was − 12.2%. Programmed death ligand 1 was measured by the Dako PD-L1 IHC 22C3 pharmDx assay. MMR mismatch repair, MSI(-H/-L) microsatellite instability (high/low), MSS microsatellite stable, NA not applicable, PD progressive disease, PR partial response, SD stable disease, UE unevaluable
3.6 Exploratory Pharmacodynamic Analyses
3.6.1 Programmed Death 1 Receptor Occupancy
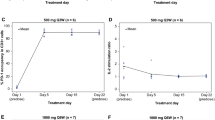
Programmed death 1 receptors on circulating CD3+ T cells were almost completely occupied by serplulimab from 24 hours after the first dose (mean range 98.1–100.1%) and remained high throughout the study, irrespective of dose levels (Table e8 and Fig. e4a of the ESM). Target engagement was observed even at the lowest dose (0.3 mg/kg), and PD-L1 occupancy was sustained at rates > 88% throughout the study in that cohort. Changes in the PD-1 receptor occupancy of individual subjects within each dose cohort followed the same trend as the mean for that cohort.
3.6.2 Interleukin-2 Stimulation Ratio
The mean interleukin-2 stimulation ratio decreased between baseline and 24 hours post-dose, with values of around 1 (range 0.9–1.2) in all dose cohorts, and remained stable until the end of the study, indicating a sustained and maximal functional blockade (Table e8 and Fig. e4b of the ESM).
4 Discussion
The findings of this phase I study provide insight into the safety, antitumor activity, and pharmacokinetic and pharmacodynamic characteristics of serplulimab in patients with advanced or metastatic solid tumors. Serplulimab was well tolerated at doses of 0.3–10.0 mg/kg Q2W, with no unexpected safety signals; the MTD was not reached. Serplulimab demonstrated antitumor activity; two patients achieved a partial response and 13 had stable disease, yielding an ORR of 8.0% and a disease control rate of 60.0%.
The TRAEs reported for serplulimab were generally consistent with the safety profile of pembrolizumab in another phase I trial [27]. The irAEs reported for serplulimab were similar to those of pembrolizumab and nivolumab [28,29,30]; in all but one patient they were grade 1–2, with only pruritus and pyrexia occurring in more than one patient. Grade ≥ 3 irAEs occurred in one (3.4%) patient in the current trial, while they were reported in up to 24 and 11% of patients receiving nivolumab and pembrolizumab, respectively [31]. There were no cases of immune-mediated pneumonitis or hypothyroidism, which are known irAEs associated with immune checkpoint inhibitors. These findings should be interpreted in light of the known variation in irAEs according to tumor type, patient comorbidities, and prior treatment history, as well as certain lifestyle factors [30].
The pharmacokinetic profile of serplulimab demonstrated low clearance, limited volume of distribution, and a long elimination half-life; exposure increased approximately dose proportionately. These pharmacokinetic characteristics are also exhibited by pembrolizumab and nivolumab [31, 32]. The volume of distribution at steady state (3.3–3.7 L across doses) was comparable to those for nivolumab and pembrolizumab (central/peripheral volumes of distribution: 3.6/2.8 L and 3.5/4.1 L, respectively), as was clearance at steady state with serplulimab 1.0–10.0 mg/kg (0.01 L/h [0.24 L/day] vs 0.22–0.25 L/day for pembrolizumab) [31]. Accumulation of serplulimab was minimal after repeated administration, with ratios similar or slightly lower than those reported for pembrolizumab and nivolumab (Rac 1.2–2.0 across doses for serplulimab vs 2.1 for pembrolizumab and 3.7 for nivolumab, respectively) [28, 29]. Serplulimab, like other PD-1 inhibitors, appears to have minimal potential for immunogenicity, with only one (3.4%) patient in the present study developing serplulimab ADAs (vs 11.2% [nivolumab] and 0.7–2.5% [pembrolizumab]) [31]. The small patient sample and differences in study design should be considered when interpreting this difference.
The pharmacodynamic findings demonstrate that serplulimab has a high affinity for the PD-1 receptor, and induced sustained target engagement throughout the study. Programmed death 1 binding was saturated and functional blockade was induced at the lowest dose of 0.3 mg/kg. Receptor occupancy may be greater with serplulimab (median > 88% at 0.3 mg/kg) than with nivolumab (median > 65% at doses of 1–10 mg/kg) [33]. Moreover, there appeared to be no dose dependency, as PD-1 receptor occupancy remained high across dose groups until the end of the study regardless of fluctuations in the mean serum serplulimab concentration.
Tumor response in this study might be confounded by a small patient sample that was heterogeneous with regard to tumor type, biomarker status, and treatment history. Early phase I trials of nivolumab and pembrolizumab have demonstrated similarly low response rates, but subsequent investigations in larger populations or populations selected for tumor types or tumor biomarkers have revealed greater efficacy. Therefore, the present efficacy findings support further investigation of serplulimab in selected and larger patient populations.
There is increasing interest in biomarkers that may predict response to immunotherapy, and while there is currently a plethora of potential candidates [34], none has yet been declared robust or been clinically validated. Most of the present study population had PD-L1-negative tumors; therefore, the potential predictive and prognostic potential of PD-L1 expression for serplulimab efficacy requires further exploration. In this study, no association was found between the biomarkers tested (MSI status, PD-L1 expression) and the best percentage change from baseline in tumor burden.
Serplulimab was first approved by the China National Medical Products Administration for the treatment of adult patients with advanced, unresectable, or metastatic MSI-high solid tumors that have failed to respond to previous standard treatments [21, 35, 36]. The chosen registration dose of 3.0 mg/kg for the aforementioned first approval was selected based on a comprehensive analysis of the predicted clinical efficacy dose of serplulimab from our pre-clinical data, its pharmacokinetic/pharmacodynamic relationship, the safety and efficacy data of the dose escalation study, and comparisons of the activity and pharmacokinetic exposures with other drugs in the same class. In November 2022 and January 2023, serplulimab in combination with chemotherapy received additional National Medical Products Administration approvals for the first-line treatment of squamous non-small cell lung cancer [37] and the first-line treatment of extensive-stage small cell lung cancer [38, 39], respectively. Recently published data have also shown promising antitumor activity and a manageable safety profile with serplulimab administered in combination with chemotherapy in patients with esophageal squamous cell carcinoma [40], HCC [41], and cervical cancer [42].
Several limitations should be considered when interpreting the findings, including the phase I study design, the interim nature of the analyses, the small sample sizes for each cohort, and the variety of tumor types treated. Only Asian patients were enrolled in this study; however, serplulimab is currently being studied in more ethnically and racially diverse populations in international clinical trials. In addition, serplulimab dosing has yet to be optimized; the efficacy findings may have been limited by the treatment of some evaluable patients at suboptimal doses. Further studies in larger patient populations are warranted to confirm these findings.
5 Conclusions
Serplulimab was well tolerated at doses of 0.3–10.0 mg/kg Q2W. The pharmacokinetic profile of serplulimab was favorable, with minimal accumulation after repeated administration. Pharmacodynamic studies revealed that saturated PD-1 binding/functional blockade occurred at all doses tested. The immunogenic potential of serplulimab was also minimal. Preliminary efficacy findings showed promising antitumor activity. Taken together, these data support further study of serplulimab in larger patient cohorts.
References
Zou W, Wolchok JD, Chen L. PD-L1 (B7–H1) and PD-1 pathway blockade for cancer therapy: mechanisms, response biomarkers, and combinations. Sci Transl Med. 2016;8(328):328rv4. https://doi.org/10.1126/scitranslmed.aad7118.
Seidel JA, Otsuka A, Kabashima K. Anti-PD-1 and anti-CTLA-4 therapies in cancer: mechanisms of action, efficacy, and limitations. Front Oncol. 2018;8:86. https://doi.org/10.3389/fonc.2018.00086.
Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 2015;373(17):1627–39. https://doi.org/10.1056/NEJMoa1507643.
Ferris RL, Blumenschein G Jr, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. 2016;375(19):1856–67. https://doi.org/10.1056/NEJMoa1602252.
Cohen EEW, Soulières D, Le Tourneau C, Dinis J, Licitra L, Ahn M-J, et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet. 2019;393(10167):156–67. https://doi.org/10.1016/S0140-6736(18)31999-8.
Fradet Y, Bellmunt J, Vaughn DJ, Lee JL, Fong L, Vogelzang NJ, et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: results of >2 years of follow-up. Ann Oncol. 2019;30(6):970–6. https://doi.org/10.1093/annonc/mdz127.
Nishijima TF, Shachar SS, Nyrop KA, Muss HB. Safety and tolerability of PD-1/PD-L1 inhibitors compared with chemotherapy in patients with advanced cancer: a meta-analysis. Oncologist. 2017;22(4):470–9. https://doi.org/10.1634/theoncologist.2016-0419.
Yi M, Zheng X, Niu M, Zhu S, Ge H, Wu K. Combination strategies with PD-1/PD-L1 blockade: current advances and future directions. Mol Cancer. 2022;21(1):28. https://doi.org/10.1186/s12943-021-01489-2.
Passiglia F, Galvano A, Rizzo S, Incorvaia L, Listì A, Bazan V, et al. Looking for the best immune-checkpoint inhibitor in pre-treated NSCLC patients: an indirect comparison between nivolumab, pembrolizumab and atezolizumab. Int J Cancer. 2018;142(6):1277–84. https://doi.org/10.1002/ijc.31136.
Xu C, Chen Y-P, Du X-J, Liu J-Q, Huang C-L, Chen L, et al. Comparative safety of immune checkpoint inhibitors in cancer: systematic review and network meta-analysis. BMJ. 2018;363: k4226. https://doi.org/10.1136/bmj.k4226.
Gandhi L, Rodriguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078–92. https://doi.org/10.1056/NEJMoa1801005.
Paz-Ares L, Luft A, Vicente D, Tafreshi A, Gumus M, Mazieres J, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040–51. https://doi.org/10.1056/NEJMoa1810865.
Hellmann MD, Paz-Ares L, Bernabe Caro R, Zurawski B, Kim SW, Carcereny Costa E, et al. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N Engl J Med. 2019;381(21):2020–31. https://doi.org/10.1056/NEJMoa1910231.
Johnson ML, Cho BC, Luft A, Alatorre-Alexander J, Geater SL, Laktionov K, et al. Durvalumab with or without tremelimumab in combination with chemotherapy as first-line therapy for metastatic non-small-cell lung cancer: the phase III POSEIDON study. J Clin Oncol. 2023;41(6):1213–27. https://doi.org/10.1200/JCO.22.00975.
Rudin CM, Awad MM, Navarro A, Gottfried M, Peters S, Csoszi T, et al. Pembrolizumab or placebo plus etoposide and platinum as first-line therapy for extensive-stage small-cell lung cancer: randomized, double-blind, phase III KEYNOTE-604 study. J Clin Oncol. 2020;38(21):2369–79. https://doi.org/10.1200/JCO.20.00793.
Owonikoko TK, Park K, Govindan R, Ready N, Reck M, Peters S, et al. Nivolumab and ipilimumab as maintenance therapy in extensive-disease small-cell lung cancer: CheckMate 451. J Clin Oncol. 2021;39(12):1349–59. https://doi.org/10.1200/JCO.20.02212.
Spigel DR, Vicente D, Ciuleanu TE, Gettinger S, Peters S, Horn L, et al. Second-line nivolumab in relapsed small-cell lung cancer: CheckMate 331☆. Ann Oncol. 2021;32(5):631–41. https://doi.org/10.1016/j.annonc.2021.01.071.
Horn L, Mansfield AS, Szczęsna A, Havel L, Krzakowski M, Hochmair MJ, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–9. https://doi.org/10.1056/NEJMoa1809064.
Paz-Ares L, Dvorkin M, Chen Y, Reinmuth N, Hotta K, Trukhin D, et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929–39. https://doi.org/10.1016/S0140-6736(19)32222-6.
Issafras H, Fan S, Tseng C-L, Cheng Y, Lin P, Xiao L, et al. Structural basis of HLX10 PD-1 receptor recognition, a promising anti-PD-1 antibody clinical candidate for cancer immunotherapy. PLoS ONE. 2021;16(12): e0257972. https://doi.org/10.1371/journal.pone.0257972.
Lee A. Serplulimab: first approval. Drugs. 2022;82(10):1137–41. https://doi.org/10.1007/s40265-022-01740-0.
Chao TY, Ho CL, Cheng WH, Chang CL, Hsieh YY, Jiang W, et al. A novel anti-PD-1 antibody HLX10 study led to the initiation of combination immunotherapy. Ann Oncol. 2019;30:ix109–10. https://doi.org/10.1093/annonc/mdz438.007.
Yuan Y, Hess KR, Hilsenbeck SG, Gilbert MR. Bayesian optimal interval design: a simple and well-performing design for phase I oncology trials. Clin Cancer Res. 2016;22(17):4291–301. https://doi.org/10.1158/1078-0432.CCR-16-0592.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47. https://doi.org/10.1016/j.ejca.2008.10.026.
Seymour L, Bogaerts J, Perrone A, Ford R, Schwartz LH, Mandrekar S, et al. iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017;18(3):e143–52. https://doi.org/10.1016/S1470-2045(17)30074-8.
Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. https://doi.org/10.1055/s-0030-1247132.
Patnaik A, Kang SP, Rasco D, Papadopoulos KP, Elassaiss-Schaap J, Beeram M, et al. Phase I study of pembrolizumab (MK-3475; anti-PD-1 monoclonal antibody) in patients with advanced solid tumors. Clin Cancer Res. 2015;21(19):4286–93. https://doi.org/10.1158/1078-0432.CCR-14-2607.
Merck & Co I. Keytruda® (pembrolizumab) prescribing information (August 2022 update). Whitehouse Station; 2022.
Bristol Myers Squibb. Opdivo® (nivolumab) prescribing information (July 2022 update). Princeton; 2022.
Khoja L, Day D, Wei-Wu Chen T, Siu LL, Hansen AR. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: a systematic review. Ann Oncol. 2017;28(10):2377–85. https://doi.org/10.1093/annonc/mdx286.
Centanni M, Moes DJAR, Trocóniz IF, Ciccolini J, van Hasselt JGC. Clinical pharmacokinetics and pharmacodynamics of immune checkpoint inhibitors. Clin Pharmacokinet. 2019;58(7):835–57. https://doi.org/10.1007/s40262-019-00748-2.
Brahmer JR, Hammers H, Lipson EJ. Nivolumab: targeting PD-1 to bolster antitumor immunity. Future Oncol. 2015;11(9):1307–26. https://doi.org/10.2217/fon.15.52.
Brahmer JR, Tykodi SS, Chow LQM, Hwu W-J, Topalian SL, Hwu P, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med. 2012;366(26):2455–65. https://doi.org/10.1056/NEJMoa1200694.
Bai R, Lv Z, Xu D, Cui J. Predictive biomarkers for cancer immunotherapy with immune checkpoint inhibitors. Biomark Res. 2020;8(1):34. https://doi.org/10.1186/s40364-020-00209-0.
Shanghai Henlius Biotech, Inc. Henlius receives NMPA approval for its first innovative monoclonal antibody HANSIZHUANG. 2022. Available from: https://www.henlius.com/en/NewsDetails-3512-26.html. Accessed 13 Dec 2023.
Qin S, Li J, Zhong H, Jin C, Chen L, Yuan X, et al. Serplulimab, a novel anti-PD-1 antibody, in patients with microsatellite instability-high solid tumours: an open-label, single-arm, multicentre, phase II trial. Br J Cancer. 2022;127(12):2241–8. https://doi.org/10.1038/s41416-022-02001-3.
Shanghai Henlius Biotech, Inc. Henlius' novel anti-PD-1 mAb HANSIZHUANG (serplulimab) receives NMPA approval for the treatment of sqNSCLC. 2022. Available from: https://www.henlius.com/en/NewsDetails-3837-26.html. Accessed 13 Dec 2022.
Cheng Y, Han L, Wu L, Chen J, Sun H, Wen G, et al. Effect of first-line serplulimab vs placebo added to chemotherapy on survival in patients with extensive-stage small cell lung cancer: the ASTRUM-005 randomized clinical trial. JAMA. 2022;328(12):1223–32. https://doi.org/10.1001/jama.2022.16464.
Shanghai Henlius Biotech, Inc. Henlius’ novel anti-PD-1 mAb HANSIZHUANG (serplulimab) approved for the treatment of ES-SCLC. 2023. Available from: https://www.henlius.com/en/NewsDetails-3949-26.html. Accessed 13 Dec 2023.
Song Y, Zhang B, Xin D, Kou X, Tan Z, Zhang S, et al. First-line serplulimab or placebo plus chemotherapy in PD-L1-positive esophageal squamous cell carcinoma: a randomized, double-blind phase 3 trial. Nat Med. 2023;29(2):473–82. https://doi.org/10.1038/s41591-022-02179-2.
Ren Z, Shao G, Shen J, Zhang L, Zhu X, Fang W, et al. Phase 2 study of the PD-1 inhibitor serplulimab plus the bevacizumab biosimilar HLX04 in patients with previously treated advanced hepatocellular carcinoma. Liver Cancer. 2022;12:116–28. https://doi.org/10.1159/000526638.
An J, Wu L, Li X, Wang J, Hou X, Wang Q, et al. Efficacy and safety of serplulimab (an anti-PD-1 antibody) combined with albumin-bound paclitaxel in patients with advanced cervical cancer who have progressive disease or intolerable toxicity after first-line standard chemotherapy (074). Gynecol Oncol. 2022;166:S47. https://doi.org/10.1016/S0090-8258(22)01292-6.
Acknowledgements
The authors express their gratitude to the patients participating in this trial, their families, the study personnel at each study site, as well as the clinical study team (Medical R&D: Futang Yang, Qingyu Wang; Clinical Operation: Sha Deng, Haoyu Yu, Jing Li; Clinical Pharmacology: Liang Zhou; Statistics: Jiancheng Cheng), Jun Zhu, and Wenjie Zhang from Shanghai Henlius Biotech, Inc., for their support in study execution, study design, data acquisition, statistical analyses, and manuscript revisions. Medical writing support was provided by Jacqueline Kolston and Molly Yu of Parexel, and Shiqi Zhong and Chen Hu of Shanghai Henlius Biotech, Inc., and was funded by Shanghai Henlius Biotech, Inc.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was funded by Shanghai Henlius Biotech, Inc.
Conflict of interest
Ching-Liang Ho, Tsu-Yi Chao, Chia-Lun Chang, and Hsuan-Yu Lin have no conflicts of interest that are directly relevant to the content of this article.
Ethics approval
The study was conducted in accordance with the International Council for Harmonisation guidelines on Good Clinical Practice and all applicable regulatory requirements, including the Declaration of Helsinki, and was approved by the Taipei Medical University-Joint Institutional Review Board (TMU-JIRB No.: N201710016), the Institutional Review Board, Tri-Service General Hospital (TSGHIRB No.: 2-106-01-024), and the Institutional Review Board, Changhua Christian Hospital (CCH IRB No.: 190613).
Consent to participate
All participants gave written informed consent prior to participation.
Consent for publication
Not applicable.
Availability of data and material
The data generated during the current study are available from the corresponding author upon reasonable request.
Code availability
Not applicable.
Author contributions
Conceptualization: C-LH; formal analysis and investigation: C-LH, T-YC, C-LC, H-YL; writing, original draft preparation: C-LH; writing, review and editing: T-YC, C-LC, H-YL; supervision: C-LH.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ho, CL., Chao, TY., Chang, CL. et al. Safety, Tolerability, and Preliminary Efficacy of Serplulimab, a Novel Anti-PD-1 Antibody, in Patients with Metastatic or Recurrent Solid Tumors: A Phase I Study. BioDrugs 38, 287–299 (2024). https://doi.org/10.1007/s40259-023-00639-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40259-023-00639-w