
Abstract
Recent advances in culture-free methods of studying the human microbiome, coupled with strong bioinformatics tools, have provided new insights on the role of the human microbiome in health and disease. The human gut, in particular, houses a vast number and diverse variety of microbes. A plethora of evidence has demonstrated the significant effects of the gut microbiome on local and systemic immunity. Studies in hematopoietic stem cell transplantation recipients provided early evidence of the involvement of the gut microbiome in the development of graft-versus-host disease and its related mortality. Cancer immunotherapy and checkpoint inhibitors, in particular, harness the power of the host’s immune system to fight a range of malignancies. Resistance to immunotherapy and fatal immune-related adverse events both continue to be challenges in the field. The role of the human gut microbiome in affecting the response to immunotherapy was recently uncovered through a series of preclinical and clinical studies. The evidence presented in these studies provides tremendous potential for gut microbes to be used for biomarker development and therapeutic intervention trials.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
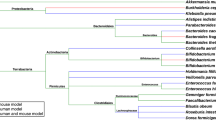
Intestinal microbiota play an important role in shaping local and systemic host immune responses. |
Tumor response to cancer immunotherapy, including stem cell transplant and checkpoint blockade agents, appears to be modulated by the gut microbiome in both murine models and human studies. |
Gut microbiota also modulate a variety of chemotherapy- and immunotherapy-related toxicities ranging from gastrointestinal toxicities to graft-versus-host disease. |
1 Introduction
The human gut microbiome refers to the collective community of commensal microorganisms residing in our intestinal lumen and their respective genome. The intestinal lumen houses the largest number and diversity of microbes, including bacteria, fungi, archaea, viruses, and protozoans. Our insight into the complex community of organisms inhabiting the human body was mainly derived through culturing these organisms. Traditional culture-based methods used in the past failed to detect multitudes of ‘unculturable’ microbes. With the advent of next-generation sequencing, microbiologists began to explore microbial nucleic acid abundantly found in human body surfaces and secretions. The 16s ribosomal RNA (rRNA) genes are highly conserved bacterial genetic units with enough inter-species variability to make them excellent targets for identifying specific bacterial genera in a sample. Sequencing 16s rRNA along with sequencing entire microbial genomes (an approach also referred to as metagenomics shotgun sequencing) provided scientists with massive amounts of data, allowing us to decipher various aspects of the human microbiome [1]. The rapid improvement in these culture-free methods along with strong bioinformatics tools allowed a deeper understanding of the gut microbiome and its role in a variety of diseases ranging from autoimmune to endocrine and metabolic disorders, and most recently cancer (Table 1) [2]. These microbes were also shown to be an important modulator of systemic immunity and inflammation through complex interactions with the host immune system and various microbial metabolites [3].
2 Evidence Linking the Gut Microbiome to Response and Toxicity of Cancer Therapies
2.1 The Gut Microbiome and Traditional Cytotoxic Chemotherapy
In the field of cancer therapeutics, preclinical models suggest involvement of the gut microbiome in the response to traditional cytotoxic chemotherapeutic agents, such as cyclophosphamide and platinum salts [4, 5]. The therapeutic effects of cyclophosphamide are thought to partially be mediated through an anti-tumor immune response. Systemic translocation of gut microbes plays an important role in eliciting cyclophosphamide-associated immune response in murine models through an increase in a pathogenic subset of T helper (Th) cells (Th17) and memory Th cells [4]. The intestinal microbiota also play an important role in reactivating a metabolite, SN-38 glucuronide, of the chemotherapeutic agent irinotecan, and this results in adverse drug reactions, including severe diarrhea [6].
2.2 The Gut Microbiome and Outcomes of Hematopoietic Stem Cell Transplantation
Hematopoietic stem cell transplantation (HSCT) is one of the earliest applications of cancer immunotherapy and remains a cornerstone of treatment for hematologic malignancies. Early preclinical evidence suggests an important role of the gut microbiota in the development of graft-versus-host disease (GVHD) in HSCT recipients [7, 8]. Subsequently, multiple studies have shown a correlation between the composition and diversity of the gut microbiome at the time of HSCT and several long- and short-term outcomes, including the development of GVHD, risk of relapse, and overall survival (OS) [9,10,11]. A single-center trial showed a decrease in the 2-year cumulative incidences of relapse among HSCT patients with abundance of Eubacterium limosum in their stool in comparison with patients without this bacteria (risk of relapses/progression of disease 19.8% and 33.8%, respectively) [9]. A retrospective analysis of HSCT recipients at the time of neutrophil engraftment showed an association between low diversity of the fecal microbiota and significantly increased mortality (52%) in comparison to a high diversity of the fecal microbiota (8%) [10]. Furthermore, increased bacterial diversity and increased amounts of the genus Blautia were both independently found to be associated with reduced GVHD-related mortality [11]. Patients undergoing HSCT routinely receive antimicrobial prophylaxis to prevent invasive infections. Broad-spectrum antibiotics are often administered for the treatment of neutropenic fever in this patient population. Retrospective studies examined the role of both prophylactic and broad-spectrum antibiotics on the gut microbiota and on the development of GVHD and related mortality. In a retrospective analysis of 857 allogeneic HSCT recipients, the use of specific broad-spectrum antibiotics (imipenem–cilastatin and piperacillin–tazobactam) was associated with increased GVHD-related mortality at 5 years [12]. This was associated with loss of several commensal gut bacteria, including Bacteroidetes, Lactobacillus spp., and Clostridia. On the other hand, a study of 112 children undergoing allogeneic HSCT found that gut decontamination using a variety of antimicrobial agents prior to transplant decreased the incidence of GVHD [13]. A randomized trial also showed that addition of metronidazole to ciprofloxacin for gut decontamination post-HSCT led to a decreased incidence of acute GVHD but no difference in chronic GVHD or OS [14]. Further randomized clinical trials are currently underway to address this issue. Results from these prospective trials will hopefully provide high-grade evidence in the future regarding the use of antibiotics in this population.
2.3 Impact of Gut Microbiota on Response to Immune Checkpoint Inhibition
The development of immune checkpoint inhibitors was a major breakthrough in cancer therapy. Monoclonal antibodies targeting the programmed death receptor (PD-1) and its ligand PD-L1 and the cytotoxic T lymphocyte-associated protein 4 (CTLA-4) receptor are widely used checkpoint blockade immunotherapy agents. Resistance to treatment remains a challenge, with both primary and secondary resistance impacting patient outcomes. Tumor intrinsic factors associated with response to therapy include expression of interferon-γ-associated genes, such as PD-L1, tumor mutational burden, and expression of neoantigens recognized by tumor-infiltrating lymphocytes (TILs) [15]. Other systemic factors include germline genetics and environmental- or microbiota-based factors [16, 17]. The effect of the gut microbiota on response to these agents has been detailed through a series of preclinical and clinical studies. In 2013, Iida et al. [5] demonstrated that mice grown in germ-free conditions and those treated with broad-spectrum antibiotics had poor response to a combination of intra-tumoral CpG-oligonucleotide immunotherapy and interleukin (IL)-10 antibodies [5]. The combination of intra-tumoral CpG-oligonucleotide, a Toll-like receptor 9 (TLR-9) ligand, and inhibitory IL-10 antibodies is known to decrease tumor growth in murine models by inducing a tumor necrosis factor (TNF)-α dependent immune response. The poor response to this combination in subcutaneous solid tumor murine models was associated with a decrease in TNF-α expression and production in the tumor microenvironment. Analysis of the gut microbiome in this murine model, revealed bacterial species Alistipes shahii as one of several overrepresented species in mice responding to immunotherapy. Enrichment of this bacterial species also correlated with increased TNF-α release in the tumor microenvironment. Oral administration of this bacteria to mice produced a TNF-α-dependent improvement in response to immunotherapy, providing strong preclinical evidence for potential therapeutic interventions utilizing bacterial agents in aiding response to immunotherapy.
Further evidence emerged when genetically identical mice grown at different facilities were noted to display differences in growth rates of melanoma tumors. Surprisingly, this difference in tumor growth was shown to be mediated by the gut microbiome [18]. Fecal transfer and co-housing of mice from different facilities successfully delayed tumor growth in the mice group with the more aggressive tumors. Several microbial species were differentially enriched in each group’s stool specimens. Enrichment of Bifidobacterium spp. positively correlated with delayed tumor growth in these mice and with higher CD8 + tumor-infiltrating T cells after administration of anti-PD-L1 therapy. Oral administration of Bifidobacterium alone resulted in enhanced tumor control through CD8 + T cells, resembling the response to anti-PD-L1 therapy. Combination treatment with Bifidobacterium and anti-PD-L1 therapy nearly abolished tumor outgrowth in these mice [18]. This strong preclinical evidence for the role of Bifidobacterium in enhancing the response to PD-L1 therapy provides the basis for future clinical trials examining oral administration of this bacteria to patients receiving PD-L1 therapy.
Broad-spectrum antibiotics and germ-free conditions were also shown to compromise response to anti-CTLA-4 therapy in sarcoma, melanoma, and colon cancer murine models. These mice showed decreased activation of splenic effector CD4 + T cells and a decrease in TILs, both of which are thought to be critical players in the immune response produced by anti-CTLA-4 therapy. Bacteroides thetaiotaomicron and B. fragilis were shown to be necessary for anti-CTLA-4 antibody efficacy in these mice [19]. Oral administration of B. fragilis, immunization with its polysaccharides, and adoptive transfer of B. fragilis-specific T cells each overcame the negative effects of broad-spectrum antibiotics and germ-free conditions. These bacteria elicited an IL-12-dependent anti-tumor Th1 response, proving the important role they play in the immune response produced by anti-CTLA-4 therapy [19].
Building on these preclinical studies, Matson et al. [20] examined the gut microbiome in metastatic melanoma patients and showed that several bacterial species were differentially enriched in patients responding to anti-PD-L1 and anti-CTLA-4 immunotherapy in comparison to non-responders. Two species of Bifidobacterium were among six other species that were associated with response to immunotherapy in this cohort. This is consistent with the previously mentioned studies in murine models showing an important role for Bifidobacterium in controlling melanoma tumors. A ratio of beneficial to non-beneficial gut bacterial species was shown to predict response to immunotherapy in this cohort of melanoma patients. This ratio could be developed in the future as a promising biomarker for response to immunotherapy to help identify patients more likely to benefit from checkpoint blockade therapy. To further study the gut microbiome of these patients, ‘murine avatars’ were created through stool transfer from responding and non-responding patients into germ-free mice. These murine avatars recapitulated the response phenotype of the donors, providing evidence that the microbiota signature of these patients could be transferred to produce distinct responses [20].
3 Clinical Evidence Linking Antibiotic Use to Decreased Response to Immunotherapy
Routy et al. [21] showed differential enrichment of specific bacterial species in non-small cell lung cancer (NSCLC) and renal cell carcinoma (RCC) patients responding to immunotherapy in comparison with non-responders [21]. Murine avatars created through stool transfer from NSCLC patients also recapitulated the clinical response phenotype in germ-free and antibiotic-treated mice. Enrichment of Akkermansia muciniphila at diagnosis correlated positively with response to immunotherapy in these patients. Oral supplementation with A. muciniphila to non-responder murine avatars restored the efficacy of PD-1 blockade and increased the levels of IL-12 secreted from dendritic cells [21]. Central memory CD4 + T cells were also observed in the tumor bed and tumor-draining lymph nodes after supplementation with A. muciniphila, providing clues to the underlying mechanisms [17]. Routy et al. [21] also examined the role of antibiotic treatment in affecting response to checkpoint blockade immunotherapy through a retrospective analysis of NSCLC, RCC, and urothelial carcinoma patients treated with anti-PD-1 and -PD-L1 therapy. Of these patients, 28% were prescribed antibiotics within 2 months before or 1 month after treatment with anti-PD-1/PD-L1 therapies. The group of patients who received antibiotics around the time of their immunotherapy treatment had significantly shorter progression-free survival (PFS) and OS than patients with the same tumor types who did not receive antibiotics (median OS of 11.5 vs. 20.6 months, respectively, p = 0.001) [21]. Similar results were also reported by a separate group in RCC and NSCLC. This group’s analysis included patients who received anti-CTLA-4 therapy along with anti-PD-1/PD-L1 therapy. They found 20% of their patients with NSCLC and 13% of RCC patients received antibiotics within 30 days prior to immunotherapy. Again, the antibiotic group had significant reduction in PFS (median PFS of 1.9 vs. 7.4 months in RCC, p = 0.03; and 1.9 vs. 3.8 months in NSCLC, p = 0.03) and OS in both tumor types (median OS of 17.3 vs. 30.6 months in RCC, p = 0.03; and 7.9 vs. 24.6 months in NSCLC, p < 0.01). Higher rates of disease progression were reported for the RCC antibiotic subset (75% vs. 22%, p < 0.01) [22]. A limitation of both studies is an inability to account for confounders known to modulate the intestinal microbiome, such as diet, smoking status, and co-morbid conditions. In addition, in the study by Derosa et al. [22], patient populations were heterogeneous in terms of prior lines of therapy. Prior chemotherapy likely alters the gut microbiota significantly and could be another factor confounding these results. While both studies are challenged by the retrospective nature of the analyses, their results are consistent with preclinical evidence from murine models. These results call for further prospective trials examining the role of antibiotic use in patients treated with checkpoint blockade. Antibiotic use in these patients should be judiciously and carefully approached until further prospective data become available. The specific types of antibiotics to be avoided and whether other antimicrobial therapeutics also affect response to immunotherapy remain open questions warranting further investigation.
4 Impact of the Gut Microbiome on Immune-Related Adverse Events
Immune-mediated adverse events remain a significant source of morbidity for patients treated with immune checkpoint blockade therapy. Life-threatening colitis is one of the most common immune-related adverse events associated with these therapies. Dubin et al. [23] showed differential enrichment of bacterial species in pre-inflammation stool samples taken from melanoma patients treated with anti-CTLA-4 therapy who went on to develop colitis in comparison with those who did not develop colitis. Members of the Bacteroidetes phylum were found to be enriched in colitis-resistant patients. This is consistent with prior studies suggesting an immunomodulatory role of these commensal bacteria [24]. Using metagenomics shotgun sequencing, specific bacterial genetic pathways were found to be differentially enriched in colitis-resistant patients. Using machine learning, Dubin et al. [23] proposed an algorithm to predict which melanoma patients are at risk of developing immune-mediated colitis based on bacterial genetic pathway modules enriched in their stool. Chaput et al. [25] similarly showed that distinct baseline gut microbiota compositions were associated with development of colitis and with clinical response in metastatic melanoma patients treated with anti-CTLA-4 therapy. In this cohort, high proportions of Bacteroides were present at baseline in patients with poor clinical benefit and Faecalibacterium percentages were significantly higher in patients with long-term benefits. The baseline gut microbiome of patients prone to developing colitis were enriched in Firmicutes, while high proportions of Bacteroidetes was observed in patients who did not develop colitis in this cohort [25]. These distinct microbial compositions could be used to develop clinical tools to stratify patients at the start of treatment with checkpoint blockade therapy into groups with high and low risk of developing immune-mediated colitis. The ability to predict which patients will develop immune-mediated colitis is very valuable to clinicians who have to weigh the potential risks and benefits of immunotherapy for individual patients. A variety of immune-mediated adverse events other than colitis threaten patients who receive checkpoint blockade, and whether the gut microbiome influences their development as well remains a very important open question.
5 Limitations and Future Directions
As mentioned earlier, the gut microbiome includes many other organisms in addition to bacterial microbes. Further studies looking into the role of the various non-bacterial organisms are needed to better understand this complex community. The intestinal microbiota heterogeneity can be affected by sex, age, diet, smoking, and body mass index [26, 27]. These factors can be difficult to account for in cancer studies but need to be kept in consideration for future studies. The ability to manipulate the microbiome through oral administration of bacteria was shown to be possible in murine models, but it remains unclear whether a similar response can be achieved in cancer patients. Several trials are looking into therapeutic manipulation of the gut microbiome of cancer patients through administration of probiotics and fecal transplants (Table 2).
The role of administering microbial products or ‘post-biotics’ instead of live microbes is also a largely unexplored area. This would be an attractive option, especially for cancer patients who are often immunocompromised and theoretically have a higher risk of infectious toxicities with administration of live bacteria. Several case reports describe bacteremia related to lactobacillus administration in neutropenic patients with hematologic malignancies [28]. At the same time, other bacterial strains were used safely in patients receiving chemotherapy for solid-organ malignancies [29]. The question of safety requires further studies delineating the safety of specific microbial strains in the various cancer-related immunocompromised states. Metabolomic-based studies targeted at identifying metabolites produced by our resident bacteria lead to better understanding of the products of these bacteria and their effects on the host. Identifying these metabolites opened a new frontier of administering non-live bacterial products—what is now commonly referred to as ‘post-biotics’. Post-biotics are non-viable products of bacterial metabolism that affect host responses in specific ways. Butyrate, for example, is a post-biotic with extensive preclinical data that implicates this short-chain fatty acid in gut barrier function and gut–mucosal immune homeostasis [30]. Combinations of immunotherapy with other agents, including chemotherapy and targeted therapies, are also being developed rapidly. The effects of combining chemotherapy and targeted agents with immunotherapy on the gut microbiome are still unclear and also require further studies.
6 Conclusion
The applications of cancer immunotherapy continue to rapidly expand, and our understanding of the gut microbiome and of how to modulate it is improving at a fast pace. We expect a wide range of applications for our growing knowledge of the human gut microbiome, from predicting response and toxicities, to altering response and decreasing resistance, to immunotherapy.
References
Qin J, Li R, Raes J, Arumugam M, Burgdorf KS, Manichanh C, et al. A human gut microbial gene catalogue established by metagenomic sequencing. Nature. 2010;464(7285):59–65. https://doi.org/10.1038/nature08821.
Lynch SV, Pedersen O. The human intestinal microbiome in health and disease. N Engl J Med. 2016;375(24):2369–79. https://doi.org/10.1056/NEJMra1600266.
Kim D, Zeng MY, Núñez G. The interplay between host immune cells and gut microbiota in chronic inflammatory diseases. Exp Mol Med. 2017;49(5):e339. https://doi.org/10.1038/emm.2017.24.
Viaud S, Saccheri F, Mignot G, Yamazaki T, Daillère R, Hannani D, et al. The intestinal microbiota modulates the anticancer immune effects of cyclophosphamide. Science. 2013;342(6161):971–6. https://doi.org/10.1126/science.1240537.
Iida N, Dzutsev A, Stewart CA, Smith L, Bouladoux N, Weingarten RA, et al. Commensal bacteria control cancer response to therapy by modulating the tumor microenvironment. Science. 2013;342(6161):967–70. https://doi.org/10.1126/science.1240527.
Guthrie L, Gupta S, Daily J, Kelly L. Human microbiome signatures of differential colorectal cancer drug metabolism. NPJ Biofilms Microbiomes. 2017;3:27. https://doi.org/10.1038/s41522-017-0034-1.
van Bekkum DW, Roodenburg J, Heidt PJ, van der Waaij D. Mitigation of secondary disease of allogeneic mouse radiation chimeras by modification of the intestinal microflora. J Natl Cancer Inst. 1974;52(2):401–4.
Jones JM, Wilson R, Bealmear PM. Mortality and gross pathology of secondary disease in germfree mouse radiation chimeras. Radiat Res. 1971;45(3):577–88.
Peled JU, Devlin SM, Staffas A, Lumish M, Khanin R, Littmann ER, et al. Intestinal microbiota and relapse after hematopoietic-cell transplantation. J Clin Oncol. 2017;35(15):1650–9. https://doi.org/10.1200/jco.2016.70.3348.
Taur Y, Jenq RR, Perales MA, Littmann ER, Morjaria S, Ling L, et al. The effects of intestinal tract bacterial diversity on mortality following allogeneic hematopoietic stem cell transplantation. Blood. 2014;124(7):1174–82. https://doi.org/10.1182/blood-2014-02-554725.
Jenq RR, Taur Y, Devlin SM, Ponce DM, Goldberg JD, Ahr KF, et al. Intestinal blautia is associated with reduced death from graft-versus-host disease. Biol Blood Marrow Transplant. 2015;21(8):1373–83. https://doi.org/10.1016/j.bbmt.2015.04.016.
Shono Y, Docampo MD, Peled JU, Perobelli SM, Velardi E, Tsai JJ, et al. Increased GVHD-related mortality with broad-spectrum antibiotic use after allogeneic hematopoietic stem cell transplantation in human patients and mice. Sci Transl Med. 2016. https://doi.org/10.1126/scitranslmed.aaf2311.
Vossen JM, Guiot HF, Lankester AC, Vossen AC, Bredius RG, Wolterbeek R, et al. Complete suppression of the gut microbiome prevents acute graft-versus-host disease following allogeneic bone marrow transplantation. PLoS One. 2014;9(9):e105706. https://doi.org/10.1371/journal.pone.0105706.
Beelen DW, Elmaagacli A, Müller KD, Hirche H, Schaefer UW. Influence of intestinal bacterial decontamination using metronidazole and ciprofloxacin or ciprofloxacin alone on the development of acute graft-versus-host disease after marrow transplantation in patients with hematologic malignancies: final results and long-term follow-up of an open-label prospective randomized trial. Blood. 1999;93(10):3267–75.
Gibney GT, Weiner LM, Atkins MB. Predictive biomarkers for checkpoint inhibitor-based immunotherapy. Lancet Oncol. 2016;17(12):e542–51. https://doi.org/10.1016/s1470-2045(16)30406-5.
Chowell D, Morris LGT, Grigg CM, Weber JK, Samstein RM, Makarov V, et al. Patient HLA class I genotype influences cancer response to checkpoint blockade immunotherapy. Science. 2018;359(6375):582–7. https://doi.org/10.1126/science.aao4572.
Chang L, Chang M, Chang HM, Chang F. Microsatellite instability: a predictive biomarker for cancer immunotherapy. Appl Immunohistochem Mol Morphol. 2018;26(2):e15–21. https://doi.org/10.1097/pai.0000000000000575.
Sivan A, Corrales L, Hubert N, Williams JB, Aquino-Michaels K, Earley ZM, et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti-PD-L1 efficacy. Science. 2015;350(6264):1084–9. https://doi.org/10.1126/science.aac4255.
Vétizou M, Pitt JM, Daillère R, Lepage P, Waldschmitt N, Flament C, et al. Anticancer immunotherapy by CTLA-4 blockade relies on the gut microbiota. Science. 2015;350(6264):1079–84. https://doi.org/10.1126/science.aad1329.
Matson V, Fessler J, Bao R, Chongsuwat T, Zha Y, Alegre ML, et al. The commensal microbiome is associated with anti-PD-1 efficacy in metastatic melanoma patients. Science. 2018;359(6371):104–8. https://doi.org/10.1126/science.aao3290.
Routy B, Le Chatelier E, Derosa L, Duong CPM, Alou MT, Daillère R, et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science. 2018;359(6371):91–7. https://doi.org/10.1126/science.aan3706.
Derosa L, Hellmann MD, Spaziano M, Halpenny D, Fidelle M, Rizvi H, et al. Negative association of antibiotics on clinical activity of immune checkpoint inhibitors in patients with advanced renal cell and non-small-cell lung cancer. Ann Oncol. 2018;29(6):1437–44. https://doi.org/10.1093/annonc/mdy103.
Dubin K, Callahan MK, Ren B, Khanin R, Viale A, Ling L, et al. Intestinal microbiome analyses identify melanoma patients at risk for checkpoint-blockade-induced colitis. Nat Commun. 2016;7:10391. https://doi.org/10.1038/ncomms10391.
Troy EB, Kasper DL. Beneficial effects of Bacteroides fragilis polysaccharides on the immune system. Front Biosci (Landmark Ed). 2010;15:25–34.
Chaput N, Lepage P, Coutzac C, Soularue E, Le Roux K, Monot C, et al. Baseline gut microbiota predicts clinical response and colitis in metastatic melanoma patients treated with ipilimumab. Ann Oncol. 2017;28(6):1368–79. https://doi.org/10.1093/annonc/mdx108.
Haro C, Rangel-Zúñiga OA, Alcalá-Díaz JF, Gómez-Delgado F, Pérez-Martínez P, Delgado-Lista J, et al. Intestinal microbiota is influenced by gender and body mass index. PLoS One. 2016;11(5):e0154090. https://doi.org/10.1371/journal.pone.0154090.
Shanahan ER, Shah A, Koloski N, Walker MM, Talley NJ, Morrison M, et al. Influence of cigarette smoking on the human duodenal mucosa-associated microbiota. Microbiome. 2018;6(1):150. https://doi.org/10.1186/s40168-018-0531-3.
Lee AC, Siao-Ping Ong ND. Food-borne bacteremic illnesses in febrile neutropenic children. Hematol Rep. 2011;3(2):e11. https://doi.org/10.4081/hr.2011.e11.
Thomsen M, Clarke S, Vitetta L. The role of adjuvant probiotics to attenuate intestinal inflammatory responses due to cancer treatments. Benef Microbes. 2018. https://doi.org/10.3920/bm2017.0172.
Gonçalves P, Araújo JR, Di Santo JP. A cross-talk between microbiota-derived short-chain fatty acids and the host mucosal immune system regulates intestinal homeostasis and inflammatory bowel disease. Inflamm Bowel Dis. 2018;24(3):558–72. https://doi.org/10.1093/ibd/izx029.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Jason J. Luke has received the following funding: Department of Defense Career Development Award (W81XWH-17-1-0265), the Arthur J Schreiner Family Melanoma Research Fund, the J. Edward Mahoney Foundation Research Fund, Brush Family Immunotherapy Research Fund, and Buffet Fund for Cancer Immunotherapy.
Conflict of interest
Jason J. Luke declares the following: consultancy—7 Hills, Aduro, Actym, Alphamab Oncology, Amgen, Array, AstraZeneca, BeneVir, Bristol-Myers Squibb, Castle, CheckMate, Compugen, EMD Serono, Gilead, Ideaya, Janssen, Merck, NewLink, Novartis, RefleXion, Spring Bank, Syndax, Tempest, and WntRx; research support (all institutional except as marked)—AbbVie, Array (personal), Boston Biomedical, Bristol-Myers Squibb, Celldex, CheckMate (personal), Corvus, Delcath, Evelo (personal), Five Prime, Genentech, Immunocore, Incyte, MedImmune, Macrogenics, Novartis, Pharmacyclics, Palleon (personal), Merck, Tesaro, and Xencor; travel—Amgen, Array, AstraZeneca, BeneVir, Bristol-Myers Squibb, Castle, CheckMate, EMD Serono, Gilead, Ideaya, Janssen, Merck, NewLink, Novartis, and RefleXion. Patents: Jason J. Luke is a co-inventor on a patent submitted by the University of Chicago covering use of microbiota to improve cancer immunotherapy outcomes. Afaf E.G. Osman declares that she has no conflicts of interest that might be relevant to the contents of this manuscript.
Rights and permissions
About this article

Cite this article
Osman, A.E.G., Luke, J.J. The Impact of the Fecal Microbiome on Cancer Immunotherapy. BioDrugs 33, 1–7 (2019). https://doi.org/10.1007/s40259-018-0328-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40259-018-0328-8