
Abstract
Purpose
The prevalence of overweight/obesity and abdominal obesity is increasing worldwide, accompanied by an increase in the incidence of non-communicable diseases. This study aims to determine the trends of Body Mass Index (BMI) and prevalence of overweight/obesity and abdominal obesity changes in Iranian adult population from 2004 to 2021.
Methods
We conducted this study based on the eight national surveys of noncommunicable disease risk factor surveillance (STEPS) from 2004 to 2021 in Iran. We estimated the crude and standardized mean of BMI and prevalence of general and abdominal obesity in these eight STEPS surveys data. Data weighted using post-stratification method and the trends depicted based on the standardized estimates.
Results
Between 2004 and 2021, and based on the standardized estimates, the mean of BMI increased from 25.19 kg/m2 in 2004 to 26.63 kg/m2 in 2021 (P-value for trend = 0.03). The standardized mean of WC increased from 86.38 cm in 2004 to 91.65 cm in 2021 (P-value for trend = 0.38). The standardized prevalence of obesity (class I and II) increased from 14.54% in 2004 to 20.17% in 2021 (P-value for trend = 0.01). The standardized prevalence of obesity class III increased from 0.82% in 2004 to 1.35% in 2021 (P-value for trend = 0.03). The standardized prevalence of abdominal obesity based on the national and international cut-points increased, but the trend was not statistically significant [(National cut-point: 27.53% in 2004 to 40.43% in 2021 (P-value for trend = 0.71)) (International cut-point: 27.58% in 2004 to 41.81% in 2021 (P-value for trend = 0.06))].
Conclusion
The standardized mean of BMI and prevalence of overweight/obesity and abdominal obesity increased among Iranian adults between 2004 and 2021. Because of the negative public and clinical health implications of obesity, health policymakers should develop comprehensive programs to control this increasing trend of weight gain.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obesity is a global public health problem that affects both adults and children. The prevalence of overweight or obese adults increased more than two-fold globally from 1980 to 2023 [1, 2]. In the United States, obesity increased by 0.2% annually from 1999 to 2012, affecting about 35% of the US population [3,4,5,6]. Obesity is also more common among specific populations, with obesity prevalence being 18.9% in the lowest-income group, 19.9% in the middle-income group, and 10.9% in the highest-income group [7].
The leading indicators of obesity are body mass index (BMI) and abdominal obesity, which are assessed using the waist circumference (WC) and waist-hip ratio (WHR) [8]. Studies have shown that these indicators are associated with Non-Communicable Diseases (NCDs) morbidity and mortality, such as cardiovascular diseases (CVDs) and type II diabetes mellitus (T2DM). Therefore, one of the aims of the WHO Action Plan for the Prevention and Control of NCDs 2013–2021 was to halt the rise of obesity by 2025 [9]. To achieve this goal, it is essential to have reliable information on the level, trend, and distribution of NCD risk factors, including overweight and obesity, among different population groups.
The WHO STEPwise approach to surveillance for NCDs risk factors (STEPS) is a WHO's recommended approach to determining public health priorities as a baseline for health interventions through determining the prevalence of risk factors for NCDs such as biological and modifiable behavioral risk factors by standardized STEPS instrument for reliable data collection [10]. STEPS surveys have further shown the complex interplay of various factors in the obesity epidemic. One includes age, as a STEPS survey conducted in Brazil revealed a steady increase in obesity from childhood to adulthood. The STEPS survey 2011 showed that, overall, 22.3% of Iranian adults aged ≥ 15 years had an abnormal accumulation of body fat (14% of males and 27.7% of females). In addition, at least 33.78, 10.25, and 30.56% of the prevalent diabetes mellitus (DM) could be attributed to overweight (BMI > 25 kg/m2), general obesity (BMI ≥ 30 kg/m2), and central obesity (waist circumference ≥ 90 cm), respectively [11, 12].
This nationwide study aimed to estimate the prevalence of general and abdominal overweight/obesity and the distribution of standardized BMI and waist circumference mean levels among the Iranian adult population by sex, age groups, and geographical distribution, using the national and subnational representative samples of eight STEPS survey from 2004 to 2021. This study provides valuable information on the trend of prevalence of overweight/obesity in the Iranian population and can contribute to the development of policies and programs to prevent and control NCDs.
Methods
Study population
In accordance with the World Health Organization's STEPwise approach to Non-Communicable Disease (NCD) risk factor surveillance, this study was conducted based on eight national STEPS surveys from 2004 to 2021 in Iran [13,14,15,16,17]. The sample was selected from both urban and rural areas of Iran using the national postal code database that includes addresses of all residential buildings in the country. The sample included over 283,842 Iranian adults aged 18 and above selected from over 3000 clusters. The primary purpose was to assess three different levels of data based on three stages of the STEPs survey: Step one (complete questionnaires about sociodemographic information, medical history related to the main NCDs, etc.), Step two (physical measurements to assess overweight and obesity), and Step three (biochemical measurements to evaluate blood glucose, cholesterol, high-density lipids, and sodium and creatinine levels) [18].
Sampling was conducted using proportional-to-size cluster sampling from rural and urban areas within each province. The research tools included validated questionnaires containing demographic characteristics, living region addresses, and physical measurements using calibrated instruments. Body mass index (BMI) was calculated as weight (kg) divided by squared height (m2), and individuals were categorized according to the WHO criteria as underweight, normal, overweight, and obese [19]. Obese individuals were further classified as class I obese, class II obese, and class III obese [20].
Statistical analysis
Statistical analyses were performed to present descriptive statistics of interested variables by sex and age subgroups at national and subnational levels and geographic data sampling at provincial levels. The data were analyzed using Stata (version 11) and R (version 3.0.2) statistical software. This study used the post-stratification method to weigh the STEPS data from 2004 to 2011, for which a calculated weight was not available. For the rest of the data, their estimated weight was used. This weight was made based on the distribution of age, gender, and residency region in the population and the sample.
For a better comparison of the results of the eight STEPS surveys and considering the possibility of changing the age and urban/rural distribution of the population from 2004 to 2021, The results of all existing STEPS surveys, age, and urban/rural standardization of estimates using the direct standardization method based on the 2016 National Population and Housing Census conducted by Iran's Statistical Center.
After cleaning and preparing the samples and weighing them, point and interval estimations of mean BMI and waist circumference and the prevalence of various degrees of obesity were made based on BMI and abdominal obesity (according to Iranian and international waist circumference cut-off points [21]). Standardized estimates and non-parametric Mann–Kendall statistical tests were used to compare estimates at different time points.
Ethical Considerations
Ethical approval for each STEPS surveys was obtained from the Ethical Committee of the National Health Research Institute of the Islamic Republic of Iran (NIHR), and ethical consent for this study was obtained from the Ethical Committee of Endocrine and Metabolism Research Institute, Tehran University of Medical Sciences (IR.TUMS.EMRI.REC.1401.006), and participation was voluntary. Individuals who accepted to participate provided written informed consent. This study provides valuable information on the prevalence of NCD risk factors in the Iranian population and can contribute to developing policies and programs to prevent and control NCDs.
Results
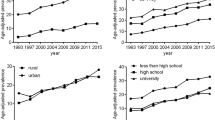
This study analyzed national STEPS surveys conducted between 2004 and 2021, which comprised eight surveys (Fig. 1). As shown in Table 1, the standardized mean of BMI exhibited a significant increase in the country during this period (25.19 kg/m2 in 2004 vs. 26.63 kg/m2 in 2021, P = 0.03), whereas the standardized mean of waist circumference also rose gradually, but this rise was not significant (86.38 cm in 2004 vs. 91.65 cm in 2021 P = 0.38). Furthermore, Table 1 indicates that the prevalence of obesity based on BMI criteria also escalated in the country. According to national [21] and international criteria [22], the prevalence of abdominal obesity also increased, but this increase was not statistically significant.

National trend of standardized prevalence of overweight (A), National trend of standardized prevalence of obesity class I, II (B), National trend of standardized prevalence of obesity class III (C), Mean of body mass index (BMI) (D), Mean of waist circumference (E), Prevalence of abdominal obesity according to international waist circumference cut-off points (F), prevalence of abdominal obesity according to Iranian waist circumference cut-off points (G), among Iranian adult population (95% CI)
Table 2 presents the standardized mean of BMI during the years 2004 to 2021 in the gender, age, and area of residency subgroups and suggests that there is an upward trend in the standardized mean of BMI in Iran among females and males, in all age groups, and among urban and rural residents, but this trend is not statistically significant (P > 0.05).
Table 3 compares the prevalence of overweight, class I, II obesity, and class III obesity among two genders, different age groups, and urban and rural residents during different years. The results demonstrate that among females, males, different age groups, and different residency areas, the increasing trend of overweight, obesity class I, II, and obesity class III in Iran was observed from 2004 to 2021. Still, this trend was not statistically significant (P > 0.05).
Table 4 compares the prevalence of abdominal obesity based on the national and international criteria among two genders, different age groups, and urban and rural residency during different years. Our result demonstrates an insignificant increase in abdominal obesity, similar to class I and II obesity.
Discussion
The current study investigated BMI trends and obesity prevalence based on BMI and waist circumference. Gender, age, and residency area divided the results. According to the outcomes of this investigation, BMI, the prevalence of obesity, and the standardized mean waist circumference have a statistically significant augmenting tendency in the country, but this increasing trend is not significant in the prevalence of abdominal obesity. Our results showed females in 2011 (1.73%), population over 60 years old in 2011 (3.51%), and urban residents in 2011 (1.77%) have the highest national prevalence of BMI-based obesity (class III). Also based on national cut-point, males in 2021 (37.44%), over 60-year-old population in 2021 (63.01%) and residents of urban areas in 2021 (34.64%) have the highest national prevalence of abdominal obesity. Based on the international cut-point, females in 2021 (47.12%), people over 60 years old in 2011 (72.84%), and urban residents in 2021 (32.32%) have the highest national prevalence of abdominal obesity.
Different investigations were conducted in the same geographical area but in different time periods. In these studies, the mean of variables was similar to ours [12, 23, 24], of course considering that these investigations are basically a cross-section of our inquiry, the similarity was not far from expected. As a next step, the tendency of alterations recorded during the inquiry was checked with other studies. In most studies in different regions of the world, the tendency of weight gain was seen, in India [25] (continent of Asia) during the 2016 STEPS, in the United States [26] (the American continent) from 2011 to 2018 based on the National Health and Nutrition Examination Survey (NHANES) investigations and also cross-sectional research conducted in Libya [27] (the African continent), and in Lebanon [28] (Eastern Mediterranean Regions). It seems that a weight gain tendency has been seen in most parts of the world which can be a serious alarm for the world community. Weight gain is a warning to increase the incidence of NCDs such as diabetes, hypertension, and cardiovascular diseases, which can reduce the quality of life, have severe complications, and impose a heavy disease burden on the healthcare system.
Global investigations also demonstrated a significant increase in obesity prevalence in the Eastern Mediterranean and North African regions by comparing BMI between 1980 and 2008 [29]. Also, a worldwide systematic review stated that on all the continents, the weight of individuals is increasing [30]. However, whether this increase was significant needs to be noted, but this point confirms the current study's findings. An exciting survey by Buyun Liu et al. [26] stated that weight, BMI, obesity, and abdominal obesity prevalence rates have augmented from 2011 to 2018 in the United States. However, this rate is different for various ethnicities. Although a significant BMI and waist circumference increase was observed among Hispanic, non-Hispanic white, and non-Hispanic Asian groups, this pattern was not observed for the non-Hispanic Black group. For abdominal obesity, a considerable increase was observed among non-Hispanic Asians but not among other racial or ethnic groups. Mean age-adjusted lean mass decreased in the non-Hispanic Black group and increased in the non-Hispanic Asian group, but no statistically significant alterations were observed in other racial or ethnic groups. Given that the investigation was conducted in one region and at one time, it seems that the effect of economic and social variables, etc., have been removed, and the most considerable effect is the effect of ethnicity. Considering that the Iranian (white Caucasian) is a non-Hispanic race, this investigation confirms our outcomes about weight gain and, in general, weight; this investigation and other investigations point to the fact that body weight is increasing progressively in the world and Iran.
This investigation demonstrated that the standardized mean of BMI, the prevalence of class I, II, and III obesity, and the standardized mean of waist circumference and abdominal obesity are increasing according to international and national criteria by gender in the country. Still, there is no statistically significant discrepancy between periods in any of the two sexes (P > 0.05), and of course, in all these reports, on average, the condition of the female sex is more of a concern. Compared to other investigations, the initial outcomes of this investigation were in line with other studies, which demonstrated a higher prevalence of overweight, abdominal obesity, and class III obesity in females [21, 23, 27]. In the next step, comparing the tendency outcomes based on gender demonstrated that the weight and prevalence of obesity augmented in both sexes. This tendency was evident in both rural and urban areas, and it seems that the slope of the line of weight gain and obesity prevalence between the years 2000 and 2007 tended to flatten, which means that the increase in these two variables in this period of time probably does not have a statistically significant difference [31]. In the investigations, other variables have also been examined, such as education and the amount of food waste, which demonstrated that the level of education does not always indicate having a healthy lifestyle, and perhaps education in this way is not very effective [31]. In other periods, other investigations demonstrated that between 1993 and 2015, weight alterations based on BMI were statistically significant in both sexes, which is different from our analysis, which may be due to the difference in the period. The period examined in two studies as well as the racial, economic, and social differences, obviously, during this period, China had a faster economic growth tendency and moved towards industrialization more than Iran, an intriguing point that was mentioned in one investigation was that in the opinion of Chinese men, weight gain is faster than women. It is related to Chinese socio-cultural characteristics and states that in Chinese society, men are more interested in being big, and women are more interested in small body shapes, so men have paid less attention to their eating habits, which has caused these alterations [32].
Apart from China, the same tendency has also existed in other societies, and in Brazilian culture, the weight and prevalence of obesity in both sexes have significantly augmented between 1975 and 1997. Also, in these years, males and females have had a statistically significant discrepancy regarding weight gain and obesity prevalence, which is also contrary to our findings, which may be why the period of investigation in these two investigations was different. The outcomes could have been similar if the mentioned investigation had been done in the same period. One of the intriguing outcomes of the inquiry of Brazilian society, which is a developing country, was that in this investigation, it was stated that women who live in areas with higher income had lost weight on average, and this is the result of increasing information and education, and increased income and education as a possible solution to weight loss [33].
An essential point in the investigation of weight gain in the world is to investigate the alterations in the rate of weight gain because, in investigations, it seems that the augmentation in the incidence of obesity in the world has accelerated in recent years. Although the rate of obesity has augmented in most countries, its levels and tendencies are significantly different. The findings demonstrate that half of the augmentation in the incidence of obesity in the world occurred in the 20 years between 1980 and 2000. Half occurred in 8 years between 2000 and 2008 [34], which means that according to the speed of weight gain in The world has become increasingly aware that a finding is analogous to the tendency of weight gain in Iran because, after 2011, we can find an augmentation in the speed of weight gain in Iran.
Regarding the comparison of the two sexes in terms of weight gain, comparing the data of 2003–2004 with the data of 2011–2012 demonstrates no significant augmentation in variables related to weight and obesity and abdominal obesity in men or women. Only women had a linear tendency for significant augmentation in class III obesity, and this alteration was not significant among men [35], which confirms the outcomes of our investigation, which means that there is a slow alteration going on.
As mentioned earlier, one of the aspects of the augmentation in obesity in the world was the possibility of augmenting the incidence of NCDs such as diabetes, and the outcomes of the investigations demonstrate that obesity and weight are increasing in both sexes, and NCDs are also augmenting at the same rate [36, 37] and this outcome for us means facing a large number of chronic NCDs in Iran and other parts of the world.
The standardized mean BMI, mean prevalence of Class I, II, and III overweight and obesity, the standardized mean of waist circumference in different age groups, and mean prevalence of abdominal obesity based on national and international criteria all increased throughout this trend study. However, comparing the different periods showed no significant increase in any of these variables in any specific age group (P > 0.05). These initial results are consistent with other studies showing that BMI increases with age, which has been observed in other studies conducted in Iran and around the world [38, 39]; then, the present study is consistent with these other studies. Our reviews revealed that age groups were no longer employed in this manner, and in most studies, age was a covariate that was adjusted during the analyses; this makes it challenging to compare studies. Our comparison showed that the trend of weight gain in the Chinese population is also statistically significant, increasing in each age group. The disparity between our study and the present study is due to the difference in the time period investigated, race, socioeconomic factors, and cultural differences [32]. Another reason for the disparity may be the difference in eating habits. For example, 2.9% of each age group in Sudan and Jordan consumed sweetened beverages. In China, with a 269% increase in the consumption of sweetened beverages, people obtain about 20% of their daily energy intake from these beverages, which is a large amount [29, 32, 40].
A survey of urban and rural areas of the country showed the same increasing pattern in obesity. However, this trend of increasing BMI, obesity, and abdominal obesity was not statistically significant in rural or urban areas (P > 0.05). A preliminary comparative analysis of the results of this study with other studies found that our results align with other studies because, in all these studies, the mean BMI, the incidence of obesity, and abdominal obesity in the urban population were higher than in the rural population [12, 25]. In examining and comparing the results of the trend change in this study with other studies, it can be said that in both urban and rural areas, the weight and prevalence of obesity are increasing, and the trend is constant in both, but in general, the slope of the change line is lower in urban areas than in rural areas [31, 41]. This result was also repeated in our study.
In the study of Shujing Ma et al. [32], it is stated that the tendency to increase BMI and waist circumference in both urban and rural areas increased during the investigation period, and this increase was significant with a high slope, which is different from the outcomes of our investigation. Considering that this process of rapid alterations in China was discussed in the previous parts, we will not repeat the contents, but the intriguing point stated in this study was that the weight discrepancy between urban and rural areas in China is disappearing because in the rural areas; It seems in the rural area population’s information about nutritional habits is less, the physical activity has decreased, mechanical transportation has increased, and this has caused the distance between urban, and rural areas to decline; It is predicted that this distance will disappear and even be reversed. It seems that even if this relationship is not changed, given it is anticipated that the rate of urbanization will double by 2050 [29], and the BMI and incidence of obesity are consistently higher in the urban population; therefore, there is a possibility that the increasing tendency of global obesity will alter and gain more speed, and this alteration will probably cause an alteration in the incidence of NCDs in the general population.
The information on urban and rural areas is separate in the global investigations of the most scrutinized areas. This information was presented separately in China and Brazil. It seems that BMI and the incidence of obesity are augmenting among children in urban and rural areas, and this augmenting tendency has a significant slope [30]. This finding is not consistent with our outcomes. Considering the age discrepancy between the two investigations (the aforementioned investigation was conducted on children, and our study included the adult population), finding different outcomes is not far from expected. However, this investigation's outcomes remind us that the national survey of the tendency of obesity in children will probably be analogous to the outcomes of this investigation because the other outcomes of global investigations were very close to our results. This incidence of obesity at younger ages means that obesity-related diseases will also happen in more youthful generations in the near future. Considering that these children will be the adults of Iran's society in the future, it is expected that the tendency of alterations in the incidence of obesity in the country will also be significant.
As mentioned, obesity is a complex disease with many contributing factors. This study investigated the effects of age, sex, and residential areas on obesity, but other factors, such as economics, may also play a role. Improved individual economic status has been associated with a decrease in obesity rates[33]. At the macro level, studies have shown that weight gain in different countries weakly correlates with gross national income (GNI)[41]. Countries with higher GNIs tend to have higher average BMIs, which may be one reason for the difference in the trend of weight gain in Iran, where the trend of increasing GNI has also been relatively slow. However, we suggest further researches to confirm or refute this hypothesis.
Limitations
One of the limitations of this study is that, except for the STEPS of 2016 and 2021, in other STEPS surveys, only the weights of post stratification and none-response were used in the estimations.
Conclusion
In conclusion, to the best of our knowledge, the present study is the first in Iran to study and compare several STEPS surveys. According to the findings of this study, the standardized mean of BMI and prevalence of obesity based on BMI have increased significantly. The prevalence of abdominal obesity in Iran is rising with a slow slope. This increase in the obesity rate has potentially substantial negative public and clinical health implications. To prevent the increase of obesity-related NCDs, health policymakers should develop comprehensive programs; We also suggest that the following stages of STEPS surveys should also be investigated in future studies.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to the restrictions set by the funder of study, National Institute for Health Research, but are available from the corresponding author on reasonable request.
References
Salam MM, Yousuf R, Salam MW, Haque M. Obesity and overweight: a global public health issue. Adv Hum Biol. 2023;13(1). https://doi.org/10.4103/aihb.aihb_106_22.
Song L, Zhang Y, Chen T, Maitusong P, Lian X. Association of body perception and dietary weight management behaviours among children and adolescents aged 6–17 years in China: cross-sectional study using CHNS (2015). BMC Public Health. 2022;22(1):175. https://doi.org/10.1186/s12889-022-12574-6.
Wang Y, Beydoun MA, Min J, Xue H, Kaminsky LA, Cheskin LJ. Has the prevalence of overweight, obesity and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020;49(3):810–23. https://doi.org/10.1093/ije/dyz273.
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity among adults: United States. NCHS Data Brief. 2012;2013(131):1–8.
Abebe TB, Doyle MB, Khan A, Eagon JC, Dimou FM, Eckhouse SR, et al. Should bariatric surgery play a larger role in the management of pediatric patients with severe obesity and end-stage organ disease? Obes Surg. 2023;33(8):2585–7. https://doi.org/10.1007/s11695-023-06661-9.
Frazier SL. Increasing knowledge of and promoting positive attitudes towards the consumption of fruit and vegetables among pre-school children, parents, and teachers in three childcares in one city in a Midwestern United States county: A multi-level intervention of teachers, parents, and children. PhD diss., University of Michigan-Flint, 2023.
Soliman N, Huseth-Zosel A, Soliman AT. Obesity and overweight in children below 5 years of age: environmental, behavioural and social factors and their active use in prevention and management. World Nutrition. 2021;12(4):190–212.
Derby CA, Zilber S, Brambilla D, Morales KH, McKinlay JB. Body mass index, waist circumference and waist to hip ratio and change in sex steroid hormones: the Massachusetts Male Ageing Study. Clin Endocrinol (Oxf). 2006;65(1):125–31. https://doi.org/10.1111/j.1365-2265.2006.02560.x.
Organization WH. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. World Health Organization; 2013.
Bonita R, Winkelmann R, Douglas KA, de Courten M. The WHO Stepwise approach to surveillance (STEPS) of non-communicable disease risk factors. In Global behavioral risk factor surveillance. Boston, MA: Springer US, 2003;9–22.
Esteghamati A, Meysamie A, Khalilzadeh O, Rashidi A, Haghazali M, Asgari F, et al. Third national Surveillance of Risk Factors of Non-Communicable Diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemia. BMC Public Health. 2009;9:167. https://doi.org/10.1186/1471-2458-9-167.
Bakhshi E, Koohpayehzadeh J, Seifi B, Rafei A, Biglarian A, Asgari F, et al. Obesity and related factors in Iran: The STEPS Survey, 2011. Iran Red Crescent Med J. 2015;17(6):e22479. https://doi.org/10.5812/ircmj.17(6)2015.22479.
Nejadghaderi SA, Ahmadi N, Rashidi MM, Ghanbari A, Noori M, Abbasi-Kangevari M, et al. Physical activity pattern in Iran: findings from STEPS 2021. Front Public Health. 2022;10:1036219. https://doi.org/10.3389/fpubh.2022.1036219.
Hajebi A, Nasserinejad M, Azadnajafabad S, Ghasemi E, Rezaei N, Yoosefi M, et al. Physical inactivity, inequalities, and disparities across districts of Iran: a STEPs survey-based analysis. J Phys Act Health. 2023;20(8):735–41. https://doi.org/10.1123/jpah.2022-0113.
Tabatabaei-Malazy O, SaeediMoghaddam S, Masinaei M, Rezaei N, MohammadiFateh S, Dilmaghani-Marand A, et al. Association between being metabolically healthy/unhealthy and metabolic syndrome in Iranian adults. PLoS One. 2022;17(1):e0262246. https://doi.org/10.1371/journal.pone.0262246.
Mahdavi M, Parsaeian M, Farzadfar F, Mohamadi E, Olyaeemanesh A, Takian A. Inequality in prevalence, awareness, treatment, and control of hypertension in Iran: the analysis of national households’ data. BMC Public Health. 2022;22(1):2349. https://doi.org/10.1186/s12889-022-14768-4.
Perseh L, Peimani M, Ghasemi E, Nasli-Esfahani E, Rezaei N, Farzadfar F, et al. Inequalities in the prevalence, diagnosis awareness, treatment coverage and effective control of diabetes: a small area estimation analysis in Iran. BMC Endocr Disord. 2023;23(1):17. https://doi.org/10.1186/s12902-023-01271-z.
World Health Organization. Regional Office for Europe. The WHO STEPwise approach to surveillance. World Health Organization. Regional Office for Europe. 2021. https://iris.who.int/handle/10665/341077. License:CCBY-NC-SA3.0IGO.
Haththotuwa RN, Wijeyaratne CN, Senarath U. Worldwide epidemic of obesity. In Obesity and obstetrics. Elsevier; 2020. p. 3–8.
Weisell RC. Body mass index as an indicator of obesity. Asia Pac J Clin Nutr. 2002;11:S681–4. https://doi.org/10.1046/j.1440-6047.11.s8.5.x.
Azizi F, Khalili D, Aghajani H, Esteghamati A, Hosseinpanah F, Delavari A, et al. Appropriate waist circumference cut-off points among Iranian adults: the first report of the Iranian National Committee of Obesity. 2010;243–44.
WHO Consultation on Obesity (1999: Geneva, Switzerland) & World Health Organization. Obesity : preventing and managing the global epidemic : report of a WHO consultation. World Health Organization; 2000. https://iris.who.int/handle/10665/42330.
Amin R, Kolahi AA, Sohrabi MR. Disparities in obesity prevalence in Iranian adults: cross-sectional study using data from the 2016 STEPS survey. Obes Facts. 2021;14(3):298–305. https://doi.org/10.1159/000516115.
Djalalinia S, Saeedi Moghaddam S, Sheidaei A, Rezaei N, Naghibi Iravani SS, Modirian M, et al. Patterns of obesity and overweight in the Iranian population: findings of STEPs 2016. Front Endocrinol (Lausanne). 2020;11:42. https://doi.org/10.3389/fendo.2020.00042.
Tripathy JP, Thakur JS, Jeet G, Chawla S, Jain S, Prasad R. Urban rural differences in diet, physical activity and obesity in India: are we witnessing the great Indian equalisation? Results from a cross-sectional STEPS survey. BMC Public Health. 2016;16(1):816. https://doi.org/10.1186/s12889-016-3489-8.
Liu B, Du Y, Wu Y, Snetselaar LG, Wallace RB, Bao W. Trends in obesity and adiposity measures by race or ethnicity among adults in the United States 2011–18: population based study. BMJ. 2021;372:n365. https://doi.org/10.1136/bmj.n365.
Lemamsha H, Randhawa G, Papadopoulos C. Prevalence of overweight and obesity among Libyan men and women. Biomed Res Int. 2019;2019:8531360. https://doi.org/10.1155/2019/8531360.
Nasreddine L, Naja F, Chamieh MC, Adra N, Sibai AM, Hwalla N. Trends in overweight and obesity in Lebanon: evidence from two national cross-sectional surveys (1997 and 2009). BMC Public Health. 2012;12(1):798. https://doi.org/10.1186/1471-2458-12-798.
Malik VS, Willett WC, Hu FB. Global obesity: trends, risk factors and policy implications. Nat Rev Endocrinol. 2013;9(1):13–27. https://doi.org/10.1038/nrendo.2012.199.
Wang Y, Lobstein T. Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes. 2006;1(1):11–25. https://doi.org/10.1080/17477160600586747.
Roemling C, Qaim M. Obesity trends and determinants in Indonesia. Appetite. 2012;58(3):1005–13. https://doi.org/10.1016/j.appet.2012.02.053.
Ma S, Xi B, Yang L, Sun J, Zhao M, Bovet P. Trends in the prevalence of overweight, obesity, and abdominal obesity among Chinese adults between 1993 and 2015. Int J Obes (Lond). 2021;45(2):427–37. https://doi.org/10.1038/s41366-020-00698-x.
Monteiro CA, D’A Benicio MH, Conde WL, Popkin BM. Shifting obesity trends in Brazil. Eur J Clin Nutr. 2000;54(4):342–6. https://doi.org/10.1038/sj.ejcn.1600960.
Stevens GA, Singh GM, Lu Y, Danaei G, Lin JK, Finucane MM, et al. National, regional, and global trends in adult overweight and obesity prevalences. Popul Health Metr. 2012;10(1):22. https://doi.org/10.1186/1478-7954-10-22.
Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in obesity among adults in the United States, 2005 to 2014. JAMA. 2016;315(21):2284–91. https://doi.org/10.1001/jama.2016.6458.
Inoue Y, Qin B, Poti J, Sokol R, Gordon-Larsen P. Epidemiology of obesity in adults: latest trends. Curr Obes Rep. 2018;7(4):276–88. https://doi.org/10.1007/s13679-018-0317-8.
Pi-Sunyer FX. The obesity epidemic: pathophysiology and consequences of obesity. Obes Res. 2002;10 Suppl 2(S12):97S-104S. https://doi.org/10.1038/oby.2002.202.
Vaisi-Raygani A, Mohammadi M, Jalali R, Ghobadi A, Salari N. The prevalence of obesity in older adults in Iran: a systematic review and meta-analysis. BMC Geriatr. 2019;19(1):371. https://doi.org/10.1186/s12877-019-1396-4.
Msyamboza KP, Kathyola D, Dzowela T. Anthropometric measurements and prevalence of underweight, overweight and obesity in adult Malawians: nationwide population based NCD STEPS survey. Pan Afr Med J. 2013;15(1):108. https://doi.org/10.11604/pamj.2013.15.108.2622.
AlFaris NA, Alshwaiyat NM, Alkhalidy H, AlTamimi JZ, Alagal RI, Alsaikan RA, et al. Sugar-sweetened beverages consumption in a multi-ethnic population of middle-aged men and association with sociodemographic variables and obesity. Front Nutr. 2022;9:987048. https://doi.org/10.3389/fnut.2022.987048.
Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70(1):3–21. https://doi.org/10.1111/j.1753-4887.2011.00456.x.
Acknowledgements
All STEPS surveys have been funded by the National Institute for Health Research of Iran and Iran Ministry of Health and Medical Education. We would like to thank all of the researchers and personnel of STEPS surveys.
Funding
This study was funded by the Endocrinology and Metabolism Research Institute, Tehran University of Medical Sciences, Tehran, Iran (Number: 1400–02-105–1182).
Author information
Authors and Affiliations
Contributions
NE AND ZHT: Conceptualization, investigation, designing, visualization, writing – original draft. KKH and MM: Conceptualization, investigation, designing, visualization, writing – review & editing. DKH and FF: Investigation, writing – review & editing. OTM, HSE, SASH, AO and BL: Conceptualization, writing – review & editing. SHR: Conceptualization, designing, project administration, supervision, writing – review & editing. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The studies involving human participants were reviewed and approved by the ethical committee of the National Institute for Health Research and the ethical committee of Endocrine and Metabolism Research Institute, Tehran University of Medical Sciences (IR.TUMS.EMRI.REC.1401.006). Participation in surveys was voluntary and written informed consent was obtained from all of the participants.
Consent for publication
Not applicable.
Conflict of interests
The authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Efazati, N., Hoseini Tavassol, Z., khalagi, K. et al. General and abdominal obesity trends in the Iranian adult population from 2004 to 2021. J Diabetes Metab Disord 22, 1745–1761 (2023). https://doi.org/10.1007/s40200-023-01310-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40200-023-01310-5