
Abstract
Background
Diabetes as the leading cause of mortality and morbidity, have been increased by about 35% from 2011 to 2015 worldwide. The objective of this study was to assess the trend and pattern of diabetes and prediabetes prevalence in Iran and also evaluate the diagnosis and status of diabetes management.
Methods
The results of this study are extracted from the National Stepwise approach to non-communicable disease risk factor surveillance (STEPS), conducted in 2007, 2011, 2016, and 2021 in Iran. We evaluated all obtained data by questionnaires (demographic, epidemiologic, risk-related behavioral data), physical measurements, and laboratory measures.
Results
The prevalence of diabetes almost doubled from 2007 to 2021 among adults 25 years old and above. Diabetes prevalence increased from 10.85% (95% CI:10.30–11.40) in 2016 to 14.15% (13.42–14.87) in 2021. Prediabetes prevalence increased from 18.11% (17.46- 18,76) in 2016 to 24.81% (23.88–25.74) in 2021. Diabetes diagnosis stayed constant hence; diabetes coverage improved from 56.87% (54.21–59.52) to 65.04% (62.40- 67.69). Despite an enhancement in diabetes diagnosis and coverage, diabetes effective care did not improve significantly during 2016 and 2021, with a number of 35.98% (32.60- 39.36) in 2016 and 31.35% (28.20- 34.51) in 2021.
Conclusion
The prevalence of diabetes and prediabetes in Iran is almost doubled during the past 14 years. Although, several health policies had been developed to improve the screening and quality of diabetes care; there are still significant gaps in the effective control of diabetes. Accordingly, the current care plan should be reviewed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Diabetes as a leading cause of morbidity and mortality worldwide is an important global public concern with a tremendous economic burden on society [1, 2]. According to World Health Organization WHO estimations, the number of people with diabetes will increase from 135 million in 1995 to 300 million in 2025 and the increase will be more prominent in developing countries (170% in developing countries and 42% in developed countries) [3]. Also, diabetes is associated with a greater impact on reducing life expectancy in developing countries, which is mainly due to lifestyle and modernization of the society rather than genetic or ethnic characteristics [4].
In Iran, the prevalence of diabetes in adults aged 25–70 years increased by 35% from 2011 to 2015 [5]. It is estimated that nearly 9.2 million Iranians are likely to have diabetes by the year 2030 [6]. A significant percentage of people in Iran (about 30%) are unaware of their illness and delay in the diagnosis of diabetes is associated with complications as well as the increase in costs of management [7, 8]. Diabetes has always been one of the top ten leading causes of death in Iran and thus assessing the prevalence and its changes is a priority, especially to help policymakers [9].
Although the trend of diabetes in Iran has been summarized in the previous reports [5] an update of diabetes prevalence in 2021 and critical appraisal of data on T2DM as well as related risk factors are lacking. Moreover, the previous study was point estimated and we tried to enhance the estimation method by applying sample and population weights.
The purpose of the present study was to provide comprehensive information regarding the trend of diabetes and prediabetes at the national and subnational levels in Iran and to evaluate the diagnosis and also treatment and control of diabetes based on the results of the STEP-wise approach to non-communicable disease risk factor surveillance (STEPS) study during 2007–2021.
Methods
Overview
In the current study, we used data from Iran STEPS 2007, 2011, 2016, and 2021 surveys. STEPS is a national large-scale cross-sectional study of individuals aged ≥ 18 years recruited from urban and rural areas of all 31 Iran’s provinces depleting a stratified random cluster sampling method. Only participants aged more than 25 years were eligible for lab measurements. In brief, STEPS 2007 was conducted on 29,991 individuals, 2011 on 12,104 individuals, 2016 on 31,50 individuals, and 2021 on 27,874 participants.
These surveys were conducted based on the standardized approach devised by the WHO, known as STEPS, to monitor NCD risk factors on a national level. The detailed methodology of this survey has been described elsewhere [10, 11].
Study design
The STEPS contains three phases, including (1) Questionnaire-based assessment, (2) Anthropometric measurement, and (3) Biochemical measurements. All STEPS participants were provided with detailed information regarding the study’s objectives and methods. Informed consent was obtained from all participants. All the participants included in this study were aged 18 years or above. Only participants aged more than 25 years were eligible for lab measurements.
Variable definitions
Participants were divided into six age groups (25–34, 35–44, 45–54, 55–64, 65–74, and above). Diabetes was defined as Fasting Plasma glucose (FPG), or current self-reported diabetes medication [based on the intake of Oral Hypoglycemic Agents (OHA) and/or insulin injection]. Pre-diabetes was defined as 100 < FPG ≤ 125 mg/dl among those who were not recognized as diabetic. Diabetes diagnosis was defined as individuals’ self-report based on their physician’s diagnosis among all diabetic patients. Diabetes coverage is defined as the proportion of diabetic individuals who had taken medication routinely. American Diabetes Association (ADA) criteria were used to define diabetes effective care; accordingly, patients with FPG < 130 mg/dl were considered as having effective care [12].
The number of successfully completed years of schooling was used to define education, which was categorized into four subgroups [0 (Illiterate), 1–6, 7–12, and > 12 years] to define education level. Principal component analysis (PCA) was utilized to calculate the participants’ wealth index from household asset data. Individuals’ wealth indices were categorized into five quintiles from the poorest (first quintile) to the richest (fifth quintile). We used Global Physical Activity Questionnaire version 1 (GPAQ 1) to measure physical activity and the MET-min score was used to represent weekly physical activity [13]. Hypertension was defined as the presence of one of the following terms: systolic blood pressure ≥ 140 mmHg, or diastolic blood pressure ≥ 90 mmHg, or self-reported anti-hypertensive medications.
Data sources
Age-standardization of provincial diabetes and prediabetes prevalence was achieved according to the 2016 National Population and Housing Census conducted by Iran’s Statistical Center. A total of eight studies based on WHO STEPS have been surveyed in Iran in 2005, 2006, 2007, 2008, 2009, 2011, 2016, and 2021. The studies from 2006, 2008, and 2009 were excluded; because they did not contain biochemical measures including blood glucose. Moreover, the study from 2005 was excluded due to the differences in the sampling frame. We applied population and sampling weights to estimate the most accurate prevalence of diabetes and prediabetes.
Statistical analysis
All prevalence proportion have been presented with 95% Confidence Intervals (95% CI) in the tables after applying weights to the samples, based on the population size, age, and gender distribution (survey analysis) for the STEPS 2016 and 2021; hence, for the 2007 and 2011 weights calculated only based on population size. Multiple logistic regression was applied to determine the risk factor associated with diabetes prevalence, diagnosis, coverage, and effective care in 2021. All baseline variables (Sex, Age category, Area of residency, Education, Wealth index quintiles, Marital Status, BMI category, Insurance, Low physical activity, and Hypertension) were included in the multiple logistic models. All statistical analyses were performed by R software version 4.1.2 (http://www.r-project.org, RRID: SCR_001905.).
Results
The prevalence of diabetes doubled from 2007 to 2021 (7.23% (6.59,7.87) and 14.15% (13.42,14.87), respectively) (Fig. 1). Diabetes prevalence increased in all age categories except in 25–34 and 35–44 aged groups (from 2.66% (1.92, 3.40) and 5.84% (4.88,6.8) in 2007 to (0.37% (0.99,1.76) and 3.83% (3.2,4.45) in 2021 (Fig. 2). In 2021, Highest prevalence of diabetes was observed in individuals aged 65–74 years and was more prevalent in urban areas compared to rural areas (15.19% vs. 10.96%). Also, the most increase rate was observed in individuals with more than 12 years of education from 2011 to 2021 (4.68–10.01%). The diabetes prevalence increased mostly in individuals with the lowest wealth index from 7.02% to 2011 to 13.31% in 2021. Normal-weight individuals, with 18.5 ≤ BMI < 25, had the highest increase in the term of diabetes prevalence from 4.33 to 9.18%. Moreover, the diabetes prevalence almost doubled in obese individuals (30 ≤ BMI) from 11.31 to 21.77% between 2007 and 2021. Individuals with and without health insurance had almost the same rate of diabetes prevalence increase rate during the study period (Table 1). The detailed prevalence of diabetes in each STEPS study is demonstrated in Table 1.

Diabetes and Prediabetes prevalence pattern during study periods

Diabetes (A) and prediabetes (B) pattern in different age groups
Table 2 summarizes the prevalence of prediabetes during the study period. The Prediabetes prevalence in 2007 increased from 9.58 to 24.81% in 2021 with a 158.98% of relative change. This pattern was detected in all categories of ages (Fig. 2); Hence, individuals aged 35–44 years experienced the highest rate of escalation (from 9.43% to 2007 to 23.25% in 2021). The prevalence increase rate is almost equal in rural and urban areas (157.17% and 158.11%). Prediabetes prevalence had the same pattern as diabetes in different wealth indices, which increased the most in the poorest individuals from 9.85 to 26.36%. Between different categories of BMI levels, the highest increase rate was observed in underweight individuals (18.5 < BMI) from 6.75% to 2007 to 19.82% in 2021. The prevalence increase rate is almost equal in individuals with and without insurance (156.05% and 160.69%).
Diabetes/prediabetes prevalence in each province and geographical inequalities
Between 2007 and 2021, the highest increase in diabetes prevalence was in Ilam province from 3.43 to 9.29% (Supp Table 1) (Fig. 3). Sex-stratified age-standardized diabetes prevalence is illustrated in Fig. 4. During the 14 years of the study, the highest increase in prediabetes prevalence was in Alborz province from 2.43 to 23.06% (Supp Table 2)(Fig. 3). Sex-stratified age-standardized prediabetes prevalence is illustrated in Fig. 4. The highest to lowest diabetes and prediabetes prevalence ratios were estimated to compare the trend of differences between provinces in consequent years (Supp Tables 3 and 4). The ratio for diabetes prevalence decreased from 4.17 (highest: 13.56% (Qom), lowest: 3.25% (Hamedan)) in 2007, to 2.79 (Highest: 16.29% (Khuzestan), Lowest: 5.84% (Kermanshah)) in 2021, although the highest prevalence observed in 2011 with a number of 7.11. The prediabetes prevalence ratio consistently decreased during the study period from 8.83 to 2007 to 1.94 in 2021.

Age standardized diabetes (A.2007, B.2021) and prediabetes (C.2007, D.2021) prevalence

Age standardized prevalence of diabetes (A. Male, B. Female) and prediabetes (C. Male, D. Female) in 2021
Diabetes cascade of care
Diabetes prevalence increased from 10.85% to 2016 to 4.15% in 2021; meanwhile, diabetes diagnosis did not meet any significant changes during these years (74.63–73.28%)(Table 3); hence, diabetes treatment coverage increased significantly from56.87% in 2016 to 65.04% in 2021. Despite an enhancement in diabetes treatment coverage, diabetes effective care did not face any significant changes from 2016 to 2021 (35.98% and 31.35%, respectively).
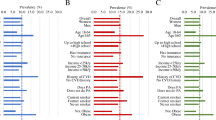
Higher age, living in urban areas, up to 7 years of education, being married or widow, higher BMI, low physical activity, and hypertension were associated with diabetes prevalence in 2021 (Table 4).
Diabetes in individuals of higher age was likely to be diagnosed except in patients aged 75 years and above (OR:1.76; CI:0.66 to 4.69). Patients in the highest wealth index quintiles had the highest risk of being diagnosed with diabetes compared to other wealth index groups (OR:1.69; CI:1.03 to 2.76). Moreover, being hypertensive and having insurance coverage were the two factors that increased the diagnosis of diabetes (Table 5).
Diabetes treatment coverage predictors are listed in Table 6. Patients aged between 55 and 64 years old, were the most covered individuals (OR:4.05; CI:1.72 to 9.52). The richest patients were more covered significantly (OR:1.76; CI:1.13 to 2.75). Having insurance and hypertension were also associated with higher coverage among diabetic patients (Table 6).
Diabetes effective care was significantly lower in patients aged between 45 and 54 and 65–74 years old (OR:0.29 and 0.30, respectively). Furthermore, patients in the 3rd quintile of the wealth index were less likely to have controlled glucose levels (OR:0.44; CI:0.27 to 0.70) (Table 7).
Discussion
These national population-based studies evaluated the prevalence, diagnosis, coverage, and effective care of diabetes and prediabetes during a period of 14 years in Iran. According to our findings, the prevalence of both diabetes and prediabetes doubled during the study period. In 2007, Diabetes had a heterogeneous geographical distribution pattern, while in 2021, eastern provinces had a higher prevalence than the national average. In terms of prediabetes, southeastern provinces higher prevalence than the national average; hence, this pattern could be observed in northeastern provinces in 2021. At the national level, diabetes diagnosis, and coverage had also increased between 20 and 30%; however, effective care dropped about 25% during this period.
The prevalence of diabetes and prediabetes showed an increasing pattern from 2007 to 2021. Similar to our findings, previous national studies reported an increase in the prevalence of diabetes and prediabetes [5, 14]. The increasing trend of diabetes and prediabetes in Iran is regardless of time period, age distribution, regional focus, diagnostic criteria as well as self-reported or clinically proven status. Thus, due to the several life-threatening complications associated with both diabetes and prediabetes, it is important to pay attention to the increasing trend and consider this issue as a priority in health policies. One of the nine WHO global monitoring framework targets to enable global tracking of progress in preventing and controlling major non-communicable diseases is to halt the rise of diabetes and obesity [15]. Iran, as a low- and middle-income country (LMIC), was not successful to reach this goal in past years.
The increase in the prevalence of diabetes was higher among females, urban areas, and older individuals compared to others. One possible explanation for the higher prevalence of diabetes in females might be the occurrence of gestational diabetes in this group [16], which highlights the necessity of policies to provide high-quality antenatal care for the diagnosis and treatment of gestational diabetes [17]. Moreover, the higher prevalence of obesity and overweight which is mainly due to multi-parity, unhealthy diet behaviors, and low levels of physical activity, is another explanation for the higher prevalence of diabetes in females compared to males [18, 19]. The higher prevalence of diabetes in urban areas can be due to changes in lifestyle, diet, obesity, and physical activity [20, 21]. Moreover, based on previous studies, the proportion of the population who had checked their blood glucose and was diagnosed with diabetes and got the proper treatment was also higher in urban areas [22]. This could also explain the higher prevalence of diabetes in urban areas and highlights the importance of applying screening programs in rural areas. Our study showed that diabetes diagnosis is less likely in elder individuals (< 70 years). This finding could be explained by the lack of typical diabetes symptoms in the elderly. Due to the increasing renal threshold for glucose in the elderly, thirst mechanisms are impaired and typical semiology including polyuria and polydipsia could not be identified in these patients. Moreover, common diabetes symptoms including neuropathy, nephropathy, cardiovascular complications, and recurrent urinary infections are usually wrongly attributed to aging [23].
According to our findings, diabetes diagnosis was 73.28% in 2021 and had an increasing pattern since 2007; however the most diagnostic rate was in 2016 (74.63%), which may be due to the health policies across the country during the past decades to educate people, screen, and treat diabetes. The increase in diabetes diagnosis is in line with previous national studies [14, 24]. Another explanation for increasing in diagnosis is that diabetes prevalence has been increasing during the study period and diagnosis growth could be due to rising prevalence. Diabetes diagnosis is significantly associated with glycemic control and reducing complications in diabetic patients [25] and thus, paying attention to diagnosis is a priority in health policies through social media and screening campaigns.
Despite the high level of diagnosis, the effective care of diabetes is still poor in Iran. Achieving a high level of effective care requires a comprehensive health delivery system providing high-quality services according to the needs of the patients, which may lead to improved health outcomes [26]. Despite the improvement in diabetes coverage, the effective care of diabetes remains the same during 2016 and 2021. This issue could have resulted from sanctions against Iran, which target the pharmaceutical industries and consumers. Sanctions caused the loss of reliable sources and obtaining low-quality materials which leads to decreased drug efficacy and unexpected toxicity [27]. The other explanation could be the high prevalence of diabetes in Iran, with an increasing rate from about 30% from 10.85% in 2016 to 14.15% in 2021. The inter-provincial difference in the country is the other driver of diabetes effective care [28]. This inequality, which is mainly due to economic and physical barriers, causes the different quality of health services provided in each province and has a strong influence on the screening, diagnosis, and treatment of non-communicable diseases [29]. According to our findings, despite the significant changes in the “highest to lowest diabetes prevalence ratio” among different provinces of Iran, we are far from our goals to come over provincial discrimination in Iran. Other drivers which impact healthcare services are outbreaks and epidemics. Per recent studies, diabetes care indices met a significant decrease during Coronavirus disease 2019 (COVID-19) pandemic [30]. This drop in diabetes care could be explained by the redistribution of health staff and facilities, lockdown policy, and community fear. Further research must be done in order to measure the quality of diabetes care and its improvement over the years in Iran. This lack of effective care is a warning sign and requires appropriate policies to improve the quality of services provided to diabetic patients. It should also be noted that despite the increase in the number of health centers providing diabetic care in the past decade and the significant allocation of costs to diabetic care, the status of diabetes effective care has not changed [31]. To reach the management goals in Iran, collaboration between the government, Non-Governmental Organisation (NGOs), healthcare professionals, and professional medical societies is mandatory [32]. It is suggested that the system of care for managing diabetes should be redesigned to provide accessible and high-quality services to diabetic patients in Iran [33].
Strengths
STEPS studies are the nationwide observational studies, which provide the most novel data regarding all health parameters in Iran with a large population-based sample of both sexes and across a broad age spectrum, in urban and rural areas of all provinces of Iran. Moreover, this study evaluated the different diabetes control parameters and age-standardized prevalence rate and pattern, which could be utilized by policymakers to integrate appropriate diabetes control programs.
Limitations
The present study should be interpreted in the context of several possible limitations. First, the study protocol had some differences in 2007 and 2011 and it was only based on FBS levels, without any questionaries regarding diabetes medication to identify diabetes; hence, we tried to overcome this issue in 2016 and 2021 by adding more specific questions in the questionnaire. Second, the STEPS study was unable to classify diabetes into type 1 and type 2. Based on global goals for diabetes management, 80% of diabetic patients should have a HbA1c level below 8%. We were unable to calculate this factor in our results, which is suggested to consider in future studies.
Conclusion
The prevalence of diabetes and prediabetes in Iran is increasing and despite the high diagnosis, receiving effective care for diabetes is suboptimal. Although, several health policies had been developed in order to improve the screening and quality of diabetes care; however, there are still significant gaps in the effective control of the disease. Further studies are warranted to evaluate the detailed changes in the quality of diabetes care, which is important in understanding current gaps and filling them with proper health policies.
Abbreviations
- ADA:
-
American Diabetes Association
- COVID-19:
-
Coronavirus disease 2019
- FPG:
-
Fasting blood glucose
- GPAQ 1:
-
Global Physical Activity Questionnaire version 1
- HbA1c:
-
Glycated hemoglobin A1c
- NCD:
-
Non-communicable disease
- NGO:
-
Non-Governmental Organisation
- OHA:
-
Oral Hypoglycemic Agents
- PCA:
-
Principal component analysis
- STEPS:
-
Stepwise approach to non-communicable disease risk factor surveillance
- WHO:
-
World Health Organization
References
Bommer C, Sagalova V, Heesemann E, Manne-Goehler J, Atun R, Bärnighausen T, et al. Global economic burden of diabetes in adults: projections from 2015 to 2030. Diabetes Care. 2018;41(5):963–70.
Bommer C, Heesemann E, Sagalova V, Manne-Goehler J, Atun R, Bärnighausen T, et al. The global economic burden of diabetes in adults aged 20–79 years: a cost-of-illness study. The Lancet Diabetes & Endocrinology. 2017;5(6):423–30.
Jafarvand E, Ataey A, Edalati S. Epidemiology and death trends due to diabetes in Iran. Intern Med Today. 2021;27(2):198–213.
Roglic G, Unwin N, Bennett PH, Mathers C, Tuomilehto J, Nag S, et al. The Burden of Mortality Attributable to Diabetes: realistic estimates for the year 2000. Diabetes Care. 2005;28(9):2130–5.
Khodakarami R, Abdi Z, Ahmadnezhad E, Sheidaei A, Asadi-Lari M. Prevalence, awareness, treatment and control of diabetes among iranian population: results of four national cross-sectional STEPwise approach to surveillance surveys. BMC Public Health. 2022;22(1):1216.
Esteghamati A, Larijani B, Aghajani MH, Ghaemi F, Kermanchi J, Shahrami A, et al. Diabetes in Iran: prospective analysis from first nationwide diabetes report of National Program for Prevention and Control of diabetes (NPPCD-2016). Sci Rep. 2017;7(1):13461.
Ogurtsova K, Guariguata L, Barengo NC, Ruiz PL-D, Sacre JW, Karuranga S, et al. IDF diabetes Atlas: global estimates of undiagnosed diabetes in adults for 2021. Diabetes Res Clin Pract. 2022;183:109118.
Dall TM, Yang W, Halder P, Pang B, Massoudi M, Wintfeld N, et al. The economic burden of elevated blood glucose levels in 2012: diagnosed and undiagnosed diabetes, gestational diabetes mellitus, and prediabetes. Diabetes Care. 2014;37(12):3172–9.
Lin X, Xu Y, Pan X, Xu J, Ding Y, Sun X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):14790.
Djalalinia S, Modirian M, Sheidaei A, Yoosefi M, Zokaiee H, Damirchilu B et al. Protocol design for large–scale cross–sectional studies of surveillance of risk factors of non–communicable diseases in Iran: STEPs 2016. Arch Iran Med. 2017;20(9).
Djalalinia SAS, Ghasemi E, Yoosefi M, Rezaei N, Farzi Y et al. Protocol design for surveillance of risk factors of non–communicable diseases during the COVID-19 pandemic: an experience from Iran STEPS Survey 2021. Arch Iran Med. 2022.
(ADA) ADA. American Diabetes Association diabetes mellitus Diagnosis [Available from: https://diabetes.org/diabetes/a1c/diagnosis.
WHO. Global physical activity questionnaire (GPAQ) 2021 [Available from: https://www.who.int/publications/m/item/global-physical-activity-questionnaire.
Mirzaei M, Rahmaninan M, Mirzaei M, Nadjarzadeh A, Dehghani Tafti AA. Epidemiology of diabetes mellitus, pre-diabetes, undiagnosed and uncontrolled diabetes in Central Iran: results from Yazd health study. BMC Public Health. 2020;20:1–9.
WHO. NCD global monitoring framework [Available from: https://www.who.int/teams/ncds/surveillance/monitoring-capacity/gmf.
Damm P, Houshmand-Oeregaard A, Kelstrup L, Lauenborg J, Mathiesen ER, Clausen TD. Gestational diabetes mellitus and long-term consequences for mother and offspring: a view from Denmark. Diabetologia. 2016;59:1396–9.
Au CPY, Raynes-Greenow CH, Turner RM, Carberry AE, Jeffery HE. Antenatal management of gestational diabetes mellitus can improve neonatal outcomes. Midwifery. 2016;34:66–71.
Tabatabaei-Malazy O, Saeedi Moghaddam S, Rezaei N, Sheidaei A, Hajipour MJ, Mahmoudi N, et al. A nationwide study of metabolic syndrome prevalence in Iran; a comparative analysis of six definitions. PLoS ONE. 2021;16(3):e0241926.
Djalalinia S, Yoosefi M, Shahin S, Ghasemi E, Rezaei N, Ahmadi N, et al. The levels of BMI and patterns of obesity and overweight during the COVID-19 pandemic: experience from the Iran STEPs 2021 survey. Front Endocrinol. 2022;13:1043894.
Khorrami Z, Yarahmadi S, Etemad K, Khodakarim S, Kameli ME, Hazaveh ARM. Urban-rural differences in the prevalence of self-reported diabetes and its risk factors: the WHO STEPS iranian noncommunicable disease risk factor surveillance in 2011. Iran J Med Sci. 2017;42(5):481.
Nejadghaderi SA, Ahmadi N, Rashidi M-M, Ghanbari A, Noori M, Abbasi-Kangevari M, et al. Physical activity pattern in Iran: findings from STEPS 2021. Front Public Health. 2023;10:1036219.
Aung WP, Htet AS, Bjertness E, Stigum H, Chongsuvivatwong V, Kjøllesdal MKR. Urban–rural differences in the prevalence of diabetes mellitus among 25–74 year-old adults of the Yangon Region, Myanmar: two cross-sectional studies. BMJ open. 2018;8(3):e020406.
Chentli F, Azzoug S, Mahgoun S. Diabetes mellitus in elderly. Indian J Endocrinol Metab. 2015;19(6):744–52.
Esteghamati A, Etemad K, Koohpayehzadeh J, Abbasi M, Meysamie A, Noshad S, et al. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005–2011. Diabetes Res Clin Pract. 2014;103(2):319–27.
Aswathi V, Chowta MN, Achappa B, Madi D. Correlation of awareness of the disease with glycaemic control and diabetic complications among patients attending a tertiary care hospital. Clin Diabetol. 2019;8(3):143–53.
Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et al. High-quality health systems in the Sustainable Development Goals era: time for a revolution. The Lancet Global Health. 2018;6(11):e1196–e252.
Akbarialiabad H, Rastegar A, Bastani B. How sanctions have impacted iranian healthcare sector: a brief review. Arch Iran Med. 2021;24(1):58–63.
Fattahi N, Azadnajafabad S, Mohammadi E, Aminorroaya A, Rezaei S, Ghasemi E et al. Geographical, gender and age inequalities in non-communicable diseases both at national and provincial levels in Iran. J Diabetes Metabolic Disorders. 2021:1–7.
Khosravi Shadmani F, Farzadfar F, Larijani B, Mirzaei M, Haghdoost AA. Trend and projection of mortality rate due to non-communicable diseases in Iran: a modeling study. PLoS ONE. 2019;14(2):e0211622.
Mirahmadizadeh A, Sharifi MH, Hassanzadeh J, Heiran A, Ardekani FM, Hadizadeh N, et al. The effect of COVID-19 pandemic on diabetes care indices in Southern Iran: an interrupted time series analysis. BMC Health Serv Res. 2023;23(1):1–9.
Noshad S, Afarideh M, Heidari B, Mechanick JI, Esteghamati A. Diabetes care in Iran: where we stand and where we are headed. Annals of Global Health. 2015;81(6):839–50.
Dehghani Firouzabadi M, Sheikhy A, Poopak A, Esteghamati A, Mechanick JI, Dehghani Firouzabadi F. Challenges to Lifestyle Medicine for type 2 diabetes in Iran: a synoptic review. Am J Lifestyle Med. 2023:15598276231167787.
Moradi G, Shokri A, Mohamadi-Bolbanabad A, Zareie B, Piroozi B. Evaluating the quality of care for patients with type 2 diabetes mellitus based on the HbA1c: a national survey in Iran. Heliyon. 2021;7(3).
Acknowledgements
The authors would like to express their gratitude for their partnership with the Deputy for Research and Technology and the Deputy of Health of the Ministry of Health and Medical Education, the National Institute for Health Research, and the World Health Organization. The authors would also like to thank the Non-Communicable Diseases Research Center’s staff of the Endocrinology and Metabolism Population Sciences Institute of Tehran University of Medical Sciences for their wholehearted cooperation. We are also grateful for the help and guidance of Dr. Mohammad Mehdi Khadembashiri in applying some revisions. This conducted study was an endocrinology and metabolism fellowship thesis project of Dr. Aslan Ameli.
Funding
This study received no grants or funding support.
Author information
Authors and Affiliations
Contributions
Conceptualization: Aslan Ameli, Negar Rezaei, Bagher Larijani, Farshad Farzadfar. Data Curation: Moein Yoosefi, Naser Ahmadi. Formal Analysis: Naser Ahmadi. Investigation: Bagher Larijani and all of the co-authors. Methodology: Aslan Ameli, Ali Sheikhy, Ozra Tabatabaei-Malazy, Naser Ahmadi, Negar Rezaei, Bagher Larijani. Writing—Original Draft Preparation: Aslan Ameli, Ali Sheikhy, Ozra Tabatabaei-Malazy. All of the authors participated in rewriting and finalizing the article and approved it.
Corresponding author
Ethics declarations
Ethical considerations
Every participant received detailed information about the survey’s objectives and procedures. Participation in the survey was entirely voluntary, and both verbal and written consent were obtained from each participant. The study received ethical approval from the ethical committee of the National Institute for Health Research (ID: IR.TUMS.NIHR.REC.1398.006).
Conflict of interest
The authors had no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material {comment: please change “diabetes” in table-4 supplementary to “prediabetes” I uploaded new file as attachment}
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ameli, A., Sheikhy, A., Tabatabaei-Malazy, O. et al. The diabetes cascade of care through the 14 years in Iran: findings of nationwide STEPS surveys 2007–2021. J Diabetes Metab Disord 22, 1731–1743 (2023). https://doi.org/10.1007/s40200-023-01308-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40200-023-01308-z