
Abstract
Background
Trabecular bone score (TBS), as a tool for measurement of bone microarchitecture, represents fracture risk independently of bone density. The aim of this study was to estimate the reference values of TBS in both genders among the Iranian population to evaluate osteoporotic fractures in the future.
Methods
The study was performed on healthy Iranian subjects who live in urban areas of Bushehr city, the capital of Bushehr province in southwestern Iran. The participants in this study were selected through a multistage, age and sex stratified, cluster random sampling. The TBS of L1-L4 was assessed by spine DXA images using TBS iNsight software (Discovery WI, Hologic Inc, USA). Age-related models of TBS were constructed using piecewise linear regression analysis.
Results
In total, 691 participants aged ≥ 18 years (381 men and 310 women) were selected for the study. The mean and standard deviation (SD) of TBS value for men was 1.420 ± 0.094 and the age at the peak TBS was 30.0 years. Among women, the corresponding value for the mean of TBS was 1.428 ± 0.070 and the age at the peak TBS was 24.5 years. Two SDs below the mean of TBS were 1.326 in men and 1.357 in women. Therefore, the following normal range for TBS values has been proposed: Among men, TBS ≥ 1.326 is considered to be normal; TBS between 1.231 and 1.326 is considered to be partially degraded microarchitecture; and TBS ≤ 1.231defined degraded microarchitecture. Among women, TBS categories are defined as normal ≥ 1.357, partially degraded between 1.287 and 1.357 and degraded ≤ 1.287.
Conclusions
This was the first study to propose evaluation of the normal range for TBS values in both genders in the Middle- East and Iran. According to our results: TBS ≤ 1.231 in men and TBS ≤ 1.287 in women is considered to be degraded microarchitecture among the Iranian population.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteoporosis as a high prevalence skeletal disease, defined by the presence of low bone mass and micro-architectural deterioration of bone tissue, and now up to 9 million osteoporotic fractures occur annually and mortality is more than 20 percent in the first years following a fracture [1]. Currently, the diagnosis and monitoring of osteoporosis in clinical practices is based on the assessment of bone mineral density (BMD) by dual energy X-ray absorptiometry (DXA) [2, 3]. Although the risk of fracture increases significantly with decreasing BMD, several studies verified that osteoporotic fractures occur across a wide spectrum of BMD [4,5,6]. Most fractures occur in the much larger group of individuals who do not fulfill the criteria for osteoporosis or even normal range of BMD value [7]. Consequently, using only BMD is inappropriate to differentiate subjects at risk of fracture from healthy subjects.
The main determinant factor of fracture risk is bone strength which is dependent on bone massand bone microarchitecture; due to this, only 70–75% of bone strength variation is illustrated by BMD, the remainder could be associated to bone quality parameters such as accumulation of micro-fractures, modified bone microarchitecture, mineral properties and bone remodeling disorders [8, 9]. Evaluation of bone microarchitecture requires certain methods such as high-resolution quantitative computed tomography (QCT), or trans-iliac bone biopsy with histomorphometry, which can be useful in the field of research, but there is little evidence to prove that they would gain any advantages in clinical practice for predicting fracture risk [10]. Trabecular bone score (TBS) is a textural index that evaluates pixel gray level variations in the lumbar spine DXA image with proprietary software, providing an indirect index of trabecular microarchitecture [11] .
Several studies have showed that vertebral fracture diagnosis is significantly increased by the combination of TBS and BMD compared with BMD alone [12, 13]. TBS can be used to predict future fracture risk in combination with BMD to increase the number of patients with well-identified risk. Furthermore, it is beneficial to improve the management of patients with secondary osteoporosis in which bone quality has a greater impact than bone quantity [14].
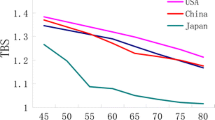
Therefore, TBS data is required for clinical use, as a reference value for populations around the world. However, few studies have reported normative values of TBS in France, Japan, and the USA, particularly among women [15,16,17]. Therefore, epidemiologic features of TBS such as age and sex-related changes in different ethnicities should be assessed throughout the world. On the other hand, as yet there is no available reference value of TBS for men in the Middle East. So far, this study aimed to develop age-related normative reference values for TBS in both genders in a population-based study in Iran.
Materials and methods
The study was performed with the participation of healthy Iranian subjects who live in urban areas of Bushehr city, the capital of Bushehr province in southwestern Iran. The participants aged > = 18 years were selected using multistage, age and sex-stratified, cluster random sampling. All individuals were evaluated for eligibility criteria. We selected subjects who did not have any metabolic diseases (cardiovascular disease, diabetes, and hypertension), any kind of cancer and they were not taking any medications that may affect muscle functions or weight (corticosteroids, bisphosphonates, parathyroid hormone, calcium, and vitamin D). Also, we included subjects with a body mass index (BMI) between 18 and 30 Kg/m2. Among the 920 individuals who were invited, a total of 818 attended the clinic (response rate: 88.9%). All individuals were evaluated for the eligibility criteria. The study was approved by the National Institute for Medical Research Development. A written informed consent was signed by all the participants.
Measurements
The participants were interviewed by trained nurses and then they completed a questionnaire regarding socio-demographic data, lifestyle factors, history of medical and drug use. Anthropometric measurements were taken with shoes removed and with the participants wearing light clothing. Height and weight were measured with a fixed stadiometer and a digital scale according to the standard protocol. A flexible circumference measuring tape was used to measure waist circumference (WC); at a point midway between the iliac crest and the lowest rib in the standing position, and the hip circumference was measured at the widest part of the hips [18].
Body composition for each participant was measured using dual x-ray absorptiometry (DXA, Discovery WI, Hologic Inc, USA). The BMD was measured at the lumbar spine (L1-L4), proximal femur and total hip. According to the rules of the International Society for Clinical Densitometry (ISCD) we excluded vertebral fractures or degenerative changes with a 1 standard deviation (SD) BMD from immediately adjacent vertebra[19].
Also, the TBS of L1-L4 was assessed using TBS iNsight® software installed on our dual x-ray absorptiometry (DXA) machine (Discovery WI, Hologic Inc, USA). The procedure was carried out by a trained operator and in accordance to the manufacturer’s instructions and the time required for the evaluation of each person was 20 min.
Statistical analysis
The normality of distribution of TBS and lumbar spine BMD (LS-BMD) was assessed using of Shapiro-Wilk test. Data are shown as mean ± SD or percentages according to distribution. Comparisons between groups were made using a t-test for continuous variables and the chi-squares tests for percentages.
The piecewise linear regression model was developed to represent an age-related change in TBS. A cutoff of the segments was determined by utilizing “Segmented package” in R software. The number of segments of this model was set to three, by the scatter gram of TBS against age. Then, the peak of TBS was determined by fitting a linear regression model in the segment including the peak of TBS for each gender group and the mean of the predicted values was considered as the peak of TBS. Two SDs below the mean of TBS in both genders are considered as the cutoff values of TBS for low-quality bone. The values between one SD and two SDs below mean TBS is considered as intermediate bone quality and the values higher than one SD below mean of TBS was defined as normal bone quality.
The analysis was performed using STATA (Release 12.Statistical software, College Station, Texas: STATA Corp LP) and R (R I 386 3, 5, 1).
Results
In total, 691 participants with a mean age 52.12 ± 19.48 were included in the analysis. Characteristics of the study population are presented in Table 1. There was a significant difference in waist circumference, weight, and height between men and women. Also, TBS L1-L4, BMDs of lumbar spine and femoral neck in men were higher than in women.
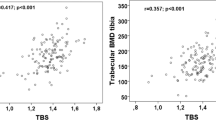
Correlation coefficients between TBS and demographic and BMD variables are shown in Table 2. There is a negative correlation between TBS and age and the Pearson’s correlation coefficient between TBS and age was larger among women than men (in women r = -0.548, 95% CI: -0.622 to -0.465 and in men r = -0.283 95% CI: -0.373 to -0.187. TBS showed a significant positive correlation with LS-BMD and femoral neck BMD (FN-BMD) in both genders. Both correlations of TBS and LS-BMD (0.793 vs. 0.688) and FN-BMD (0.530 vs. 0.445) were stronger among women than men.
The decreasing trends of TBS and LS-BMD with increasing age were observed in Table 3. The means of TBS and LS-BMD decreased in age group 18–24 years to age group 80 + years in both genders.
The three-piecewise linear regression model was developed to represent an age-related change in TBS of both genders. Based on these models, age points with the highest TBS values are estimated (Fig. 1]. The mean and standard deviation (SD) of TBS value for men was 1.420 ± 0.094 and the age at the peak TBS was 30.0 years. Among women, the corresponding value for the mean of TBS was 1.428 ± 0.070 and the age at the peak TBS was 24.5 years. Two SDs below the mean of TBS were 1.326 in men and 1.357 in women.

Scatter plots of Trabecular Bone Score (TBS) of lumbar spine against age with a piecewise linear regression line in men and women
Therefore, the following normal range for TBS values has been proposed: Among men, TBS ≥ 1.326 is considered to be normal; TBS between 1.231 and 1.326 is considered to have partially degraded microarchitecture, and TBS ≤ 1.231defined degraded microarchitecture.
Among women, TBS categories are defined as normal ≥ 1.357, partially degraded between 1.287 and 1.357 and degraded ≤ 1.287 (Table 4]. According to this categorization, 16.2% of all participants (6.6% of men and 27.9% of women) had low-quality bone.
Discussion
This study reported the peak and cutoff of TBS in a general representative population. The peak of TBS was observed at near 24 years old in women and around 30 years old in men. We used pricewise regression for estimation of cutoff for low quality microarchitecture in a representative sample of general population. Although, we found a similar peak bone trabecular score in both sexes, the cutoff for low quality bone that was determined by two standard deviations lower than the mean peak of TBS, also the intermediate quality of bone that was defined by more than one standard deviation to two standard deviations lower than the mean peak of TBS were different between genders. Among men, TBS ≥ 1.326 is considered to be normal; TBS between 1.231 and 1.326 is considered to be partially degraded microarchitecture, and TBS ≤ 1.231defined degraded microarchitecture.
Among women, TBS categories are defined as normal ≥ 1.357, partially degraded between 1.287 and 1.357 and degraded ≤ 1.287. The cutoff TBS for male was lower than female (1.28 vs. 1.23 for women and men, respectively).
Trabecular bone score is a newly introduced parameter for evaluating bone microarchitecture quality. By adding this parameter to exist predicting fracture models such as FRAX, it may improve the accuracy of these models [20]. In a meta-analysis, McCloskey et al. assessed that a cutoff of 1.23 (the lowest tertile) for TBS was useful for prediction of fractures and TBS had added value to FRAX [21]. In another study on hyperparathyroidism post-menopausal women, the values of ≤ 1.24 and ≥ 1.35 were considered as cutoff values of TBS for degraded microarchitecture and normal bone quality, respectively [11]. It seems like a sound method could be applied for detecting peak TBS and its cutoff for low bone quality. We have followed the method that was utilized for the definition of osteoporosis based on the bone mineral mass [22]. Recently, another study in the Australian population found reference ranges for TBS among men and women. These cut-points were lower than our cut-points for a determination of partially degraded microarchitecture and degraded microarchitecture in men and women [23]. In men, these cutoffs were 1.003 and 1.201 and in women, 1.157 and 1.302, respectively. It seems that ethnicity is an important factor in bone quality [24].
A strong correlation between TBS and LS-BMD was observed, similar to other studies [16, 25]. This relationship is more prominent in females. Moreover, the relationship between TBS and age was stronger among women than in the men. It may be explained by the higher speed of decrease in bone quality with increasing age in women than men [16]. Also, this correlation is higher than the study of L. M. Del Rio et al. [13] which may be due to the sampling of our study, in that the subjects with health conditions such as diabetes that could cause discrepancies between LS-BMD and TBS were excluded [26].
The strengths of this study include the following: a normal range of TBS was estimated in a general population-representative sample in a provincial capital city in the south of Iran. According to the best of our knowledge, this is the first study to determine the peak of TBS in South West Asia and North Africa among men and women.
We have some limitations in our study. We determined the cutoff based on a peak mean of TBS using a statistical method. For bone health parameters such as TBS, it is better to determine the cutoff based on clinical outcomes such as fracture of spines that should be determined in a longitudinal study. Another limitation of this study was that we did not have the lumbar spine t-score. In the results of the present study, we could not use osteoporosis in lumbar spine as a criterion to determine the cutoff of TBS.
In conclusion, TBS is a parameter for indicating quality of bone microstructure. It seems that the peak of TBS is observed in the third decade of age in both genders. The cutoff of TBS that has been determined in this study was higher in women than men. It seems that a longitudinal study may be required with a larger sample size in each age group to determine the cutoff of TBS according to clinical outcomes. A definition of a cutoff that will be accepted globally may help to change the complementary role of TBS for predicting fractures to a main facture predictor and may increase the clinical importance of this score.
References
Pisani P, Renna MD, Conversano F, Casciaro E, Di Paola M, Quarta E et al. Major osteoporotic fragility fractures: risk factor updates and societal impact. World J Orthop. 2016;7(3):171–81
Blake GM, Fogelman I. The role of DXA bone density scans in the diagnosis and treatment of osteoporosis. Postgrad Med J. 2007;83(982):509–17
Bazzocchi A, Diano D. Dual-energy x-ray absorptiometry in obesity. CMAJ. 2014;186(1):48
Johnell O, Kanis JA, Oden A, Johansson H, De Laet C, Delmas P et al. Predictive value of BMD for hip and other fractures. J Bone Miner Res. 2005;20(7):1185–94
Kanis JA, Black D, Cooper C, Dargent P, Dawson-Hughes B, De Laet C et al. A new approach to the development of assessment guidelines for osteoporosis. Osteoporos Int. 2002;13(7):527–36
Schuit SC, van der Klift M, Weel AE, de Laet CE, Burger H, Seeman E, et al. Fracture incidence and association with bone mineral density in elderly men and women: the Rotterdam Study. Bone. 2004;34(1):195–202.
Kazakia GJ, Majumdar S. New imaging technologies in the diagnosis of osteoporosis. Rev Endocr Metab Disord. 2006;7(1–2):67–74
Shepherd JA, Schousboe JT, Broy SB, Engelke K, Leslie WD. Executive summary of the 2015 ISCD position development conference on advanced measures from DXA and QCT: fracture prediction beyond BMD. J Clin Densitom. 2015;18(3):274–86
Hunt HB, Donnelly E. Bone quality assessment techniques: geometric, compositional, and mechanical characterization from macroscale to nanoscale. Clin Rev Bone Miner Metab. 2016;14(3):133–49.
Donnelly E. Methods for assessing bone quality: a review. Clin Orthop Relat Res. 2011;469(8):2128–38.
Silva BC, Boutroy S, Zhang C, McMahon DJ, Zhou B, Wang J, et al. Trabecular bone score (TBS)--a novel method to evaluate bone microarchitectural texture in patients with primary hyperparathyroidism. J Clin Endocrinol Metab. 2013;98(5):1963–70.
Rabier B, Heraud A, Grand-Lenoir C, Winzenrieth R, Hans D. A multicentre, retrospective case-control study assessing the role of trabecular bone score (TBS) in menopausal Caucasian women with low areal bone mineral density (BMDa): analysing the odds of vertebral fracture. Bone. 2010;46(1):176–81.
Del Rio LM, Winzenrieth R, Cormier C, Di Gregorio S. Is bone microarchitecture status of the lumbar spine assessed by TBS related to femoral neck fracture? A Spanish case-control study. Osteoporos Int. 2013;24(3):991–8.
Shevroja E, Lamy O, Kohlmeier L, Koromani F, Rivadeneira F, Hans D. Use of Trabecular Bone Score (TBS) as a Complementary Approach to Dual-energy X-ray Absorptiometry (DXA) for Fracture Risk Assessment in Clinical Practice. J Clin Densitom. 2017;20(3):334–45.
Dufour R, Winzenrieth R, Heraud A, Hans D, Mehsen N. Generation and validation of a normative, age-specific reference curve for lumbar spine trabecular bone score (TBS) in French women. Osteoporos Int. 2013;24(11):2837–46.
Iki M, Tamaki J, Sato Y, Winzenrieth R, Kagamimori S, Kagawa Y, et al. Age-related normative values of trabecular bone score (TBS) for Japanese women: the Japanese Population-based Osteoporosis (JPOS) study. Osteoporos Int. 2015;26(1):245–52.
Simonelli C, Leib E, Mossman N, Winzenrieth R, Hans D, McClung M. Creation of an age-adjusted, dual-energy x-ray absorptiometry-derived trabecular bone score curve for the lumbar spine in non-Hispanic US White women. J Clin Densitom. 2014;17(2):314–9
Shafiee G, Ostovar A, Heshmat R, Darabi H, Sharifi F, Raeisi A, et al. Bushehr Elderly Health (BEH) programme: study protocol and design of musculoskeletal system and cognitive function (stage II). BMJ Open. 2017;7(8):e013606.
Lewiecki EM, Gordon CM, Baim S, Leonard MB, Bishop NJ, Bianchi ML, et al. International Society for Clinical Densitometry 2007 Adult and Pediatric Official Positions. Bone. 2008;43(6):1115–21.
Harvey NC, Gluer CC, Binkley N, McCloskey EV, Brandi ML, Cooper C, et al. Trabecular bone score (TBS) as a new complementary approach for osteoporosis evaluation in clinical practice. Bone. 2015;78:216–24.
McCloskey EV, Oden A, Harvey NC, Leslie WD, Hans D, Johansson H et al. A meta-analysis of trabecular bone score in fracture risk prediction and its relationship to FRAX. J Bone Miner Res. 2016;31(5):940–8
WHO. Prevention and management of osteoporosis: report of a WHO scientific group. http://wwww.hoint/iris/handle/10665/42841. 2003.
Anderson KB, Holloway-Kew KL, Hans D, Kotowicz MA, Hyde NK, Pasco JA. Reference ranges for trabecular bone score in Australian men and women: a cross-sectional study. JBMR Plus. 2019;3(6):e10133.
Jain RK, Narang DK, Hans D, Vokes TJ. Ethnic differences in trabecular bone score. J Clin Densitom. 2017;20(2):172–9
Bazzocchi A, Ponti F, Diano D, Amadori M, Albisinni U, Battista G, et al. Trabecular bone score in healthy ageing. Br J Radiol. 2015;88(1052):20140865.
Ebrahimpur MSF, Amini Nezhad F, Bagherzadeh M, Ostovar A, Shafiee G, Heshmat R. Effect of diabetes on BMD and TBS values as determinants of bone health in the elderly: Bushehr Elderly Health program. Diabetes Metab Disord J. 2019;18(1):99–106
Funding
This study was financially supported by a grant from the National Institute for Medical Research Development (Grant Number; 940613).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical aspects
The study was conducted according to the Declaration of Helsinki, with and all patients providing written informed consent to participate in it. The study was reviewed and approved by the Research Ethics Committee of the National Institute for Medical Research Development.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shafiee, G., Sharifi, F., Heshmat, R. et al. The reference value of trabecular bone score (TBS) in the Iranian population. J Diabetes Metab Disord 19, 493–498 (2020). https://doi.org/10.1007/s40200-020-00537-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40200-020-00537-w