
Abstract
Purpose of Review
To provide a glimpse into some of the newer methods of performing IOL calculations and recent literature on which formulas and calculation strategies have been recommended for a certain subset of eyes.
Recent Findings
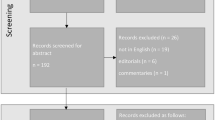
A literature review was performed to investigate all the relevant, recently published studies on the progress, comparisons, and recent advancements of IOL calculations. Based on this review, the appropriate history, evolution, progress, limitation, and recent advancements are analyzed and explained. A plethora of IOL formulas and calculation strategies have been developed to help surgeons achieve the most desired post-operative outcome for their patients.
Summary
Modern IOL formulas, calculation strategies, and biometric devices perform well for average eyes; however, they remain less optimal for eyes with atypical biometric parameters. There is no single solution that has been deemed as the perfect formula which can simplify the process and consistently provide accurate results for all types of eyes. Over the years, a number of different formula optimization strategies have been devised for traditional IOL formulas and newer, more sophisticated IOL formulas with advanced mathematical algorithms have been developed. By addition of new input parameters and use of complex mathematics to better estimate post-operative lens position, these solutions may minimize refractive error. These methods may provide increasing improvement in both typical and atypical eyes in the years to come.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cataract is the leading cause of reversible blindness in the world as it is responsible for approximately 51% of worldwide sight loss [1]. Cataract surgery is the most performed surgical procedure in ophthalmology. As more and more individuals continue to live longer, the need for performing cataract surgeries will only increase.
One of the most crucial components of cataract surgery occurs in the pre-operative stages when the surgeon decides on which intraocular lens (IOL) to implant in a patient’s eye [2]. This step is facilitated by the vital process of performing accurate IOL calculations to achieve the desired target refraction. A complex two-lens system is established after the surgery which consists of the cornea and the IOL which replaces the opacified natural lens of the eye. This system is at the core of IOL power calculations [3]. Indeed, the process of performing accurate IOL calculations is a critical factor in optimizing refractive outcomes.
Given the importance and complexity of this process, a plethora of individuals and groups have described a number of various IOL formulas, observations, intuitions, or “rules of thumb” to help surgeons achieve optimal results. In the past decade, a new wave of mathematical formulas has emerged to help the surgeon pick the most appropriate IOL for target refraction. Usually, this target is chosen to achieve emmetropia or a slight degree of myopia [4,5,6].
Almost all IOL formulas are structured similarly to calculate for vergence and predict the post-operative anterior chamber depth (ACD) or estimated lens position (ELP) [3, 7]. These formulas are composed of two-key input parameters which are representative of each eye: axial length and corneal power. These variables are used to help calculate the vergence and ELP [7]. However, high expectations from cataract surgery have fueled the development of newer generation of IOL formulas, which more input parameters and advanced mathematical algorithms to further refine their results and reach the targeted post-operative refraction.
Evolution of Current IOL Calculation Methods
Since the invention of the IOL by Sir Harold Ridley in 1951, IOL formulas have grown in their capabilities and complexities from one generation of formulas to the next. The “third-” and “fourth-generation” of IOL formulas are the most prominently used today. In the 1990s, the third-generation of IOL formulas (Holladay I, SRK/T, and Hoffer Q) was described in the literature. These formulas treated the ELP as a function of both axial length and corneal power, and not merely axial length. These theoretical improvements are the reasons these formulas are still used today for their accuracy and simplicity [3].
The “fourth-generation” of IOL formulas (Holladay II, Barrett, Olsen, and Haigis) improved on the previous generation [8]. In addition to corneal power and axial length variables, these formulas included additional variables such as patient age, measured anterior chamber depth, white-to-white measurement, and lens thickness. By incorporating additional variables within their calculation, these formulas improved not only the vergence calculation but also more importantly the ELP calculation.
To further improve the use of these formulas, various studies have shown that certain formulas are more accurate for certain types of eyes. One particular study of note compared third-generation IOL formulas and found that Hoffer Q was most ideal for eyes with axial length 20-to-21 mm, Holladay I for 21-to-21.5 mm, and SRK/T for > 27 mm. Further improvement of outcomes was demonstrated by applying the Wang-Koch adjustment to the axial length parameters when using the Holladay I formula [9].
Lastly, these IOL formulas can be personalized to achieve improved outcomes. This may be done by modifying the manufacturer’s A-constant finetune modern IOL formulas based on post-operative outcomes. Surgeons may choose to optimize the A-constant based on their data or simply use one from the User Group for Laser Interference Biometry (ULIB)—a collaborative library of optimized A-constants for the commonly used IOLs [10••].
New Formulas
Although the results of IOL calculations have drastically improved since the days of the first IOL, approximately 25% of eyes do not reach their desired post-operative target refraction [6]. There remains a clear paucity of a single, unified solution which promises accurate outcomes for both the “average” eye and an eye with atypical parameters. This lack of a singular solution has led surgeons to invest a significant portion of their time and energy to pick a single formula from a pack of other formulas which they hope will work better for a given eye. The uncertainty and need surrounding IOL calculations has led to the development of a newer generation of IOL formulas.
The H-5 formula by Hoffer is one of the “fifth-generation” of IOL formula which was developed recently. It is based on the original third-generation Hoffer Q formula. To help more eyes reach their target, the formula considers multiple input parameters such as gender and race variables. Specification of such parameters helps the formula achieve a level of increased customization with regard to a patient’s eye. For example, this formula takes gender differences into account as men tend to have increased axial length, with deeper anterior chambers and flatter corneas compared to women.
Newer and more complex IOL formulas have recently been developed which involve a “big data” approach and complex mathematical algorithms. Ladas and co-authors [10••] described a novel method of amalgamating modern IOL formulas in three dimensions. By deriving a formula from this combined “super surface” helped to create a unified IOL “super formula” to achieve increased accuracy for all eyes. The Ladas Super Formula is now using post-operative outcomes and artificial intelligence (AI) to “learn” and further improve itself by minimizing errors in IOL calculations. It is essentially a “hybrid” formula which uses known formulas that work well for a particular eye, in concert with AI to improve areas of itself that need improving.
The Hill-RBF formula is another example of an IOL formula which uses patient outcomes in combination with advanced mathematical techniques to improve refractive outcomes. It is based entirely on a machine-learned algorithm based on a dataset of around 600 or more patients with a single lens type and biometer. The FullMonte formula is another example of a formula that is based on machine learning and mathematical neural networks. It uses the Monte Carlo Markov Chain algorithm.
Recent Articles that Compare Formulas
A plethora of studies have been published which have compared many of the modern third-, fourth-, and fifth-generation of IOL formulas. A recent study compared the Hoffer Q, Holladay I, Holladay II, SRK/T, Barrett, Haigis, and T2 formulas using more than 3000 eyes [11•]. For axial lengths 22 mm and greater, the Barrett formula was the best performing formula.
Hoffer and Savini’s analysis [12•] of studies looked at the third- and fourth-generation IOL formulas to find the most ideal formulas to use for short and long eyes. It found that Haigis, Hoffer Q, and Holladay II formulas were most ideal for eyes less than 22 mm of axial length; and Barrett, Haigis, Olsen, and SRK/T formulas were the most accurate for eyes longer than 26 mm of axial length.
Gökce [13•] and co-authors compared 7 IOL formulas (Barrett Universal II, Haigis, Hill-RBF, Hoffer Q, Holladay 1, Holladay 2, and Olsen) in short eyes with axial length less than 22 mm. Although this case series included only 67 patients, it concluded that Hoffer Q and Holladay II had slightly myopic results, and Olsen had hyperopic results. And, when the mean numeric error was adjusted to zero, there was no statistically significant difference between each of the 7 formulas.
Melles [14••] and co-authors analyzed results of 7 IOL formulas (Barrett Universal II, Haigis, Hoffer Q, Holladay 1, Holladay 2, Olsen, and SRK/T) in more than 18,000 eyes split between two different monofocal lenses. The Wang-Koch axial length adjustment was also applied to certain formulas for axial length greater than 25 mm. The Barrett formula performed significantly better than the other formulas for both IOLs. The Wang-Koch adjustment resulted in a shift from hyperopic to myopic outcomes in long eyes.
Popovic [15•] and co-authors further studied the effect of Wang-Koch adjustment to the Holladay I formula in more than 200 eyes longer than 25 mm. The studied concluded that the Wang-Koch adjustment should only be used in eyes longer than 27 mm when using the Holladay I formula.
Some of the newer generation of IOL formulas (Hill-RBF, FullMonte method, and Ladas Super Formula) was studied along with Holladay I and Barrett formula [16••]. Slightly better results were achieved by the Holladay I and Barrett formula. However, of the three newer generation IOL formulas, the Ladas Super Formula had the lowest mean absolute error and was the best performing formula for short axial lengths.
Conclusion
Cataract surgeons dedicate a significant portion of their pre-operative workflow towards performing IOL calculations, picking a formula, and selecting the most appropriate lens power to implant into a given patient’s eye. This may be a challenging and time-consuming process for many surgeons given the number of formulas and factors to consider with each eye. Since there has not been a single perfect IOL formula or solution which can help to simplify this complex process, surgeons have always relied on using multiple IOL formulas and picking one which they feel will suit their needs.
Lens calculations have certainly come a long way since the days of the earliest methods by Binkhorst, Colenbrander, and Fyodorov. Despite the advancements, the current “success rate” of IOL calculations has generally remained around 70–80% in the past two-to-three decades. Regardless of this arduous process, expectations from cataract surgery remain high from both patients and surgeons. Current IOL calculation formulas generally perform well for average eyes. However, due to the mathematical and biometric imperfections, these formulas remain suboptimal in eyes with atypical values of axial length, keratometry, and anterior chamber depth.
Several new IOL formulas have been developed in the past decade which have sought to improve post-operative outcomes by introducing additional variables and incorporated advanced mathematical techniques. However, the data on these new formulas is still lacking. Few studies have been performed that have compared several formulas against each other which have shown that Barrett is the best performing overall formula from the previous generations. Use of Wang-Koch adjustment may be beneficial for longer eyes with Holladay I formula. These studies have also shown promising results with the newer generation IOL formulas which use artificial intelligence and big data approach. Ladas Super Formula has proven to show the lowest mean absolute error in this group. However, these new formulas will continue to evolve with time and could be the way forward in IOL calculations where unprecedented results are achieved in lens calculations. More comparison studies will need to be performed to compare these formulas as they continue to improve with time to help provide a more conclusive calculation solution.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96:614–8. https://doi.org/10.1136/bjophthalmol-2011-300539.
Lee AC, Qazi MA, Pepose JS. Biometry and intraocular lens power calculation. Curr Opin Ophthalmol. 2008;19:13–7.
Shammas HJ. Part A: biometry and intraocular lens power calculation. In: Colvard DM, editor. Achieving excellence in cataract surgery: a step-by-step approach; 2009.
Beiko GH. Comparison of visual results with accommodating intraocular lenses versus mini-monovision with a monofocal intraocular lens. J Cataract Refract Surg. 2013;39:48–55. https://doi.org/10.1016/j.jcrs.2012.08.059.
Narváez J, Zimmerman G, Stulting RD, Chang DH. Accuracy of intraocular lens power prediction using the Hoffer Q, Holladay 1, Holladay 2, and SRK/T formulae. J Cataract Refract Surg. 2006;32:2050–3.
Aristodemou P, Cartwright NEK, Sparrow JM, Johnston RL. Formula choice: Hoffer Q, Holladay 1, or SRK/T and refractive outcomes in 8108 eyes after cataract surgery with biometry by partial coherence interferometry. J Cataract Refract Surg. 2011;37:63–71. https://doi.org/10.1016/j.jcrs.2010.07.032.
Olsen T. Calculation of intraocular lens power: a review. Acta Ophthalmol Scand. 2007;85:472–85.
Wang L, Shirayama M, Ma XJ, Kohnen T, Koch DD. Optimizing intraocular lens power calculations in eyes with axial lengths above 25.0 mm. J Cataract Refract Surg. 2011 Nov;37(11):2018–27. https://doi.org/10.1016/j.jcrs.2011.05.042.
User Group for Laser Interference Biometry. Available at: http://ocusoft.de/ulib/. Accessed July 3, 2018.
•• Ladas JG, Siddiqui AA, Devgan U, Jun AS. A 3-D “super surface” combining modern intraocular lens formulas to generate a “super formula” and maximize accuracy. JAMA Ophthalmol. 2015;133:1431–6. https://doi.org/10.1001/jamaophthalmol.2015.3832 This study describes a novel method of representing IOL formulas in 3-D, and describes the derivation for the IOL “super formula” from the “super surface.”.
• Kane JX, Heerden AV, Atik A, Petsoglou C. Intraocular lens power formula accuracy: comparison of 7 formulas. J Cataract Refract Surg. 2016;42:1490–500. https://doi.org/10.1016/j.jcrs.2016.07.021 This study compares accuracy of 7 IOL formulas (Barrett Universal II, Haigis, Hoffer Q, Holladay 1, Holladay 2, SRK/T, and T2) using IOLMaster biometry and optimized lens constants.
• Hoffer KJ, Savini G. IOL power calculation in short and Long eyes. Asia Pac J Ophthalmol (Phila). 2017;6:330–1. https://doi.org/10.22608/APO.2017338 This study is an analysis of various studies published in the past 50 years to understand which IOL formulas are most appropriate for eyes shorter than 22 mm and longer than 26 mm.
• Gökce SE, Zeiter JH, Weikert MP, Koch DD, Hill W, Wang L. Intraocular lens power calculations in short eyes using 7 formulas. J Cataract Refract Surg. 2017;43:892–7. https://doi.org/10.1016/j.jcrs.2017.07.004 This study evaluated 7 IOL formulas (Barrett Universal II, Haigis, Hill-RBF, Hoffer Q, Holladay 1, Holladay 2, and Olsen) for eyes 22 mm or shorter.
•• Melles RB, Holladay JT, Chang WJ. Accuracy of intraocular lens calculation formulas. Ophthalmology. 2018;125:169–78. https://doi.org/10.1016/j.ophtha.2017.08.027 This study compared the accuracy of several IOL formulas (Barrett Universal II, Haigis, Hoffer Q, Holladay 1, Holladay 2, Olsen, and SRK/T) in a large cohort of eyes which received two different types of lens implants.
• Popovic M, Schlenker MB, Campos-Möller X, Pereira A, Ahmed IIK. Wang-Koch formula for optimization of intraocular lens power calculation: evaluation at a Canadian center. J Cataract Refract Surg. 2018;44:17–22. https://doi.org/10.1016/j.jcrs.2017.09.035 This study evaluated the Wang-Koch axial length adjustment to the Holladay I formula and elucidated the range of axial length where it would be most beneficial.
•• Kane JX, Van Heerden A, Atik A, Petsoglou C. Accuracy of 3 new methods for intraocular lens power selection. J Cataract Refract Surg. 2017;43:333–9. https://doi.org/10.1016/j.jcrs.2016.12.021 This study compares three new methods (Hill-RBF, FullMonte, and the Ladas Super Formula) of performing IOL calculations in addition to comparing these methods to Holladay I and Barrett Universal II formulas.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Uday Devgan reports other from Advanced Euclidean Solutions outside the submitted work. In addition, Dr. Devgan has a patent Advanced Euclidean Solutions pending. Aazim A. Siddiqui declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Cataract
Rights and permissions
About this article

Cite this article
Siddiqui, A.A., Devgan, U. Mastering Lens Calculations: New Formulas and Comparisons. Curr Ophthalmol Rep 6, 233–236 (2018). https://doi.org/10.1007/s40135-018-0186-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40135-018-0186-z