
Abstract
Introduction
Radiofrequency thermocoagulation (RFT) effectively alleviates idiopathic trigeminal neuralgia (ITN); however, postoperative facial numbness poses a significant challenge. This issue arises due to the close proximity of high-temperature thermocoagulation, which not only ablates pain-related nociceptive fibers but also affects tactile fibers. Intraoperative sensory stimulation voltage (SV), which reflects the distance between the RFT cannula and the target nerve, potentially possesses the ability to prevent tactile fiber injury. This study aimed to investigate the influence of SV on postoperative facial numbness and provide valuable insights to mitigate its occurrence.
Methods
A retrospective analysis was performed on 72 ITN patients with maxillary division (V2) pain who underwent RFT between 2020 and 2022. Among them, 13 patients with SV ≤ 0.2 V constituted the low SV group. Subsequently, a matched-cohort analysis was conducted on the remaining 59 patients. The patients paired with the low SV patients were subsequently enrolled in the high SV group, adhering to a 1:1 match ratio. The primary outcome was the facial numbness scale assessment at 3 days, 3 months and 6 months post-surgery. The pain intensity and medication burden served as the secondary outcomes.
Results
We successfully matched a cohort consisting of 12 patients in the low SV group and 12 patients in the high SV group. Each patient experienced various degrees of facial numbness at 3 days post-RFT. Notably, the low SV group exhibited a higher incidence of moderate numbness (66.7% vs. 16.67%, P = 0.036), whereas the high SV group had more cases of mild numbness at the 6-month follow-up (25% vs. 83.3%, P = 0.012). Both groups demonstrated significant decreases in pain intensity and medication burden compared to before the operation.
Conclusions
SV proved to be a reliable parameter for mitigating the degree of postoperative facial numbness in RFT treatment for ITN. A relatively high sensory SV ranging from 0.3 to 0.6 V during the RFT procedure results in less facial numbness in the treatment of ITN.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Radiofrequency thermocoagulation (RFT) has been routinely employed for treating trigeminal neuralgia, particularly in older patients with compromised fitness or a heightened surgical risk, but the concurrent occurrence of postoperative facial numbness poses a significant challenge in RFT treatment. This study aimed to investigate the impact of the intraoperative stimulation voltage (SV) on postoperative facial numbness, with the aim of minimizing the incidence of facial numbness associated with RFT in the treatment of idiopathic trigeminal neuralgia (ITN). |
What was learned from the study? |
Intraoperative SV proved to be a reliable parameter for minimizing the degree of postoperative facial numbness in RFT treatment. |
The preservation of an appropriate RFT ablation distance based on the intraoperative SV facilitates the reduction of facial numbness. |
Introduction
Idiopathic trigeminal neuralgia (ITN), also known as tic douloureux, is a condition characterized by severe facial pain without a clear cause, although it potentially involves vascular compression of the fifth cranial nerve [1, 2]. This painful disorder manifests as sudden paroxysmal attacks of knife-like, shock-like or lancinating pain in the somatosensory distribution of the trigeminal nerve, making it one of the most severe and debilitating facial pains [3, 4]. Despite an unclear origin, several effective treatment guidelines have been established, with radiofrequency thermocoagulation (RFT) of the trigeminal ganglion being a notably successful and minimally invasive option [5,6,7,8]. The routine use of RFT for ITN treatment is endorsed by clinical guidelines [9, 10], especially in older patients with compromised fitness or a heightened surgical risk, as well as in patients lacking neurovascular contact [11,12,13].
However, postoperative facial numbness, which occurs concurrently with facial pain relief, poses a substantial challenge in RFT treatment [14]. Aα and Aβ tactile fibers exhibit higher survivability in high-temperature environments than Aδ and C nociceptive fibers, suggesting the use of a temperature range that selectively targets nociceptive fibers for pain relief while preserving tactile fibers to prevent numbness [15, 16]. Temperatures exceeding 65 °C are known to destroy Aδ and C nociceptive fibers; however, the ideal temperature for selectively achieving this balance has not been reported [17]. Different doctors use different temperatures (60–90 °C) during the operation, based on their experience of optimizing the pain relief [10, 18, 19]. Currently, it is recommended that the thermocoagulation temperature in RFT procedures should not exceed 75 °C [14, 20]. This temperature threshold is implemented to achieve prolonged pain relief. However, facial numbness rates remain high, reaching 85–100% after surgery. Moreover, 30% of patients reported moderate or severe facial numbness even after a 10-year follow-up [20, 21]. This is a significant concern, as some ITN patients decline RFT treatment due to fear of postoperative facial numbness [14, 22].
Apart from the temperature, the proximity of the active tip of the cannula needle to the target nerve significantly influences the balance of pain relief and facial numbness. Closer needle tips under the same temperature conditions result in greater nerve injury, Conversely, the temperature decreases as the needle moves farther away from the nerve tissue [23,24,25]. During RFT surgery, the sensory stimulation voltage (SV) is commonly used to pinpoint the needle tip [26]. The SV serves as a potential indicator of the distance between the active tip and the target division of the trigeminal ganglion [27]. Maintaining an appropriate distance ensures that heat selectively ablates nociceptive fibers, preventing unintended damage to tactile fibers and minimizing the risk of facial numbness. Despite the potential of SV as a guiding parameter, conclusive evidence regarding the optimal SV for directing the RFT procedure remains elusive. This method offers a standardized approach for determining the distance between the needle tip and the target nerve, diminishing reliance on the doctor’s experience and minimizing the occurrence of facial numbness after RFT (Fig. 1).

Schematic illustration of the use of the stimulation voltage (SV) as a potential indicator of high- or low-temperature ablation of the target nerve
In the current research, we attempt to explore the impact of varying the SV during surgery on postoperative facial numbness through a matched-cohort analysis. A consistent set of patient characteristics are used to compare the clinical outcomes obtained when using high and low SV. Our aim is to provide valuable insights that can be instrumental for mitigating the occurrence of facial numbness associated with RFT in the treatment of ITN.
Participants and Methods
Participants
The study adhered to the Helsinki Declaration and received approval from the ethics committee of our hospital (LYS 2019-125). Written informed consent was obtained from all participating patients. This retrospective matched-cohort study involved an examination of our surgery database to identify patients who received RFT for treating the maxillary division (V2) of ITN between 2020 and 2022. ITN was diagnosed by the criteria of the International Classification of Headache Disorders II (2004): manifests as recurrent, unilateral, abrupt electric shock-like pains lasting from a fraction of a second to 2 minutes, often triggered by innocuous stimuli, and confined to the distribution of one or more divisions of the trigeminal nerve [28].
From this database, we identified 72 patients who had received RFT on the V2 branch for ITN treatment and collectedthe demographic, RFT temperature, pain intensity, pain duration, pain side and presentation data for those patients. Based on the medical records, 13 patients with a sensory SV of no more than 0.2 V during the RFT procedure were enrolled in the low SV group. The rest of the 59 patients underwent RFT with an SV ranging from 0.3 to 0.6 V. Subsequently, we conducted an exclusion and matching process, pairing patients in the low SV group with some of the remaining 59 patients, and those patients paired with low SV patients were enrolled in the high SV group (match ratio 1:1). This matching was based on specific criteria: patient characteristics, pain intensity (a difference of < 1 in the numeric rating scale (NRS) score), pain duration (a difference of < 3 months), the side of pain and RFT temperature. The individual characteristics of the patients in both groups were well balanced in terms of age (difference < 5 years), gender (identical) and weight (variation < 5 kg). Pain intensity was assessed based on their worst pain level in the last 24 h without the use of analgesics.
Inclusion Criteria and Exclusion Criteria
Inclusion criteria: (1) presentation of ITN for more than 2 years; (2) NRS value of pain greater than 6; (3) patients with ITN only involving the V2 branch; (4) undesirable pain control with medications; (5) age 40–80 years; (6) patients were treated with RFT for ITN treatment.
Exclusion criteria: (1) refusal to participate; (2) uncooperative behavior or intellectual inability to complete the self-evaluation questionnaires; (3) unstable medical illness or severe organ failure or a history of drug abuse; (4) failure to contact.
Radiofrequency Thermocoagulation Procedure
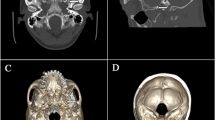
Under computed tomography (CT) guidance, all procedures were conducted by a well-trained pain physician in a disinfected examination room. We have previously described the procedure for RFT in detail [13, 29, 30]. Briefly, guided by CT fluorescence, a puncture channel to the oval foramen was identified, marked and navigated using a 22-gauge radiofrequency needle with a 5-mm active tip. After sterilization and local anesthesia, the needle was inserted into the oval foramen under CT guidance (Fig. 2). Sensory stimulations were performed to validate and readjust the needle position. In particular, the voltage was recorded during sensory stimulation (50 Hz, 0.1 ms) to induce an aching or tingling sensation within the somatosensory distribution. If the voltage required was more than 0.6 V, the position of the cannula tip was supposed to be readjusted to get a tingling sensation at lower voltage. After the needle position was confirmed through electrical stimulation, thermocoagulation of the Gasserian ganglion on the affected side was performed at 70–75 °C for 120 s, with two circles for each patient.

Oval foramen puncture under computed tomography (CT) guidance. a A puncture channel to the oval foramen was identified and marked. b The needle was inserted into the oval foramen. c Intracranial view of the insertion of the needle beyond the internal orifice of the oval foramen. d Coronal view of the insertion of the needle beyond the internal orifice of the oval foramen. a–c Three-dimensional reconstruction CT imaging; d plain CT scan. Each tailed pink arrow points to the oral foramen; each tailless green arrow points to the puncture needle
Follow-Up
Demographic information, such as age, height, weight and sex, was extracted from medical records. Additionally, details on pain intensity, pain duration, side of pain, Medication Quantification Scale Version III (MQS) and RFT temperature were examined. We conducted routine outpatient/telephone follow-ups at 3 days, 3 months and 6 months following the operation. The follow-up records for enrolled patients were retrospectively analyzed to evaluate the degree of facial numbness, pain relief and MQS and to identify any potential adverse effects.
-
(1)
Facial numbness: the degree of skin numbness in the V2 branch distribution area was assessed based on a rating scale that measured the following categories: mild = no obvious numbness, has no influence on daily life; moderate = frequently affects daily life; severe numbness = persistently affects daily life or there is painful numbness [13].
-
(2)
Numeric rate scale, NRS: pain intensity was evaluated before and after treatment using the NRS. Total scores ranged from 0 (no pain at all) to 10 (the worst imaginable pain). Postoperative pain relief of 50% was defined as effective.
-
(3)
Medication Quantification Scale Version III (MQS): medicine burden was assessed using the MQS for patients with ITN [31]. The MQS quantifies the patient’s medication regimen, considering both the types of medication and their respective dosages. It generates a weighted final score reflecting the overall “medication burden.”
-
(4)
Complications: adverse effects and complications related to the procedure (masseter weakness, corneitis, hearing loss, dropping eyelid, limited mouth opening or other) were recorded.
Statistical Analysis
The data were analyzed using GraphPad Prism software (GraphPad Software, Inc., USA). Results conforming to a normal distribution were presented as the mean ± standard deviation (SD). The Student t-test and the chi-square test were used to compare quantitative data and enumerated patient demographic data as well as the incidence of numbness. Repeated measurement analysis of variance was applied to assess the changes in pain intensity and medication burden over the follow-up period. Statistically significant differences were indicated by P < 0.05.
Results
Demographic Data
Through the application of the exclusion criteria, we successfully assembled and matched a cohort for RFT comprising 12 patients in the low SV group (1 patient was excluded due to heart failure) and an equivalent number of 12 patients in the high SV group (Fig. 3). No patients were lost during the 6-month follow-up period. Pre-surgery patient characteristics and demographics, including age, sex, weight, RFT temperature, pain duration, pain side and pain intensity were recorded. Upon comparing these factors between the two groups, no significant differences were observed in these key baseline variables (all P > 0.05) (Table 1).

Schematic illustration of the study design. a CONSORT flowchart of the study. b Scheme depicting the patient’s enrollment and follow-up evaluations. MQS Medication Quantification Scale Version III; RFT radiofrequency thermocoagulation; SV stimulation voltage
Facial Numbness
Each patient experienced various degrees of facial numbness at 3 days post-RFT. No statistically significant difference was observed in the intensity of facial numbness at 3 days and 3 months. The degree of facial numbness progressively diminished over the 6-month follow-up period. Notably, at 6 months post-operation, more patients reported mild numbness in the high SV group than in the low SV group, while more patients experienced moderate numbness in the low SV group than in the high SV group. Additionally, 1 patient in the low SV group experienced severe numbness (Table 2).
Pain Intensity
All of the 24 patients (100%) experienced significant pain relief at 3 days post-RFT procedure. At 6 months post-surgery, 22 patients reported effective pain relief. Only two individuals, one from each group, did not experience effective pain relief. One patient in the low SV group experienced a reduction in NRS from 8 to 5, while another patient in the high SV group reported a decrease from 7 to 5. The effective pain relief was 91.7% for both groups at 6 months. In both groups, the average NRS score exhibited a significant decrease, reaching its lowest intensity at 6 months post-operation. At each observation time point (3 days, 3 months and 6 months), the NRS scores were notably lower compared to the pre-surgery values in both groups (P < 0.05). However, there was no significant difference in the NRS value for pain relief between both groups (Table 3).
Medication Burden
The patients gradually discontinued their medications, including carbamazepine and oxcarbazepine, within 1 week after surgery. There was a significant MQS decrease at all observation time points compared to the pre-surgery values in both groups (P < 0.05). However, no significant difference was observed in MQS between both groups (Table 4).
Complications
Masseter muscle weakness was observed in 6 patients (50%) from the low SV group compared to 3 patients (25%) in the high SV group. However, there was no statistically significant difference in the incidence of masseter muscle weakness (P = 0.78). Fortunately, all patients experienced a recovery from masseter muscle weakness within 6 months. Moreover, no other severe complications occurred, including cranial nerve problems, carotid-cavernous fistula and mortality.
Discussion
In this matched cohort study, we conducted a comparative analysis of clinical outcomes for intraoperative low SV and high SV in RFT for treating ITN. Our primary objective was to establish a reliable method for accurately ablating hyporesistant nociceptive fibers while preserving hyper-resistant tactile fibers in RFT, with the aim of mitigating post-operational facial numbness. We assessed the occurrence of facial numbness after RFT, acknowledging that complete prevention is challenging, as all patients experienced varying levels of facial numbness. However, more patients reported mild numbness in the high SV group than in the low SV group and vice versa. Further, all 24 patients in both groups demonstrated a significant improvement in facial pain intensity after RFT, resulting in effective pain relief of 91.7% for both groups at 6 months. Additionally, the MQS value also decreased in both groups, providing additional evidence of medication burden mitigation and pain relief. No significant difference in NRS or MQS value was found between the two groups during the follow-up, indicating that both low and high SV intraoperation produce effective postoperative pain relief. The 6-month follow-up pain relief results align with previous reports, suggesting that our RFT technique is an effective percutaneous intervention for ITN treatment [23]. This implies that maintaining a suitable distance between the needle tip and target nerve through SV leads to effective nociceptive fiber ablation and reduces damage to tactile fibers. Therefore, this approach results in excellent pain relief and milder facial numbness.
ITN stands out as a frequently encountered pain disorder that poses a considerable challenge in terms of treatment. Over the course of 10 years, about half of ITN patients gradually develop resistance to pharmacological solutions, prompting the need for surgical intervention [5]. Among the various intervention techniques for ITN, microvascular decompression (MVD) and RFT have emerged as the most popular. The improvement in and widespread adoption of MVD have established it as the primary choice for ITN, offering long-term pain relief to approximately 70% of patients without causing postoperative facial numbness [32,33,34]. However, MVD possess a high recurrence rate of 1–5% and carries the highest risk of significant postoperative complications, including meningitis, cerebral spinal fluid leak, stroke, hemorrhage and death. These safety concerns restrict its application [35,36,37]. Since 1974, RFT has gained popularity as an effective and minimally invasive treatment [38, 39]. RFT of the trigeminal ganglion boasts a high success rate (comparable to MVD) in minimizing facial pain. Additionally, it offers the advantages of selectivity and positive patient acceptance and it has no associated mortality [5, 18, 40, 41].
We previously compared the clinical outcomes of different branches of ITN, revealing that the V2 branch is the most frequently affected and achieves higher pain relief than other branches after RFT [12]. Consequently, we meticulously matched the demographic data, pain characteristics and RFT temperature to investigate the impact of intraoperative SV variation on the facial numbness in V2 pain patients. In addition to assessing pain relief using NRS, we also evaluated the patient’s medication burden using the MQS. This tool helps us to assess the correlation between drug dosage and the patient's clinical response, enabling a standardized dosage comparison across various medications [42]. The decrease in medication burden in both groups provides additional evidence underscoring the analgesic effectiveness of our RFT operation.
RFT procedures are performed under CT guidance. While X-ray allows observation of the basion, the nerve tissue and trigeminal ganglion remain unobservable. X-ray can be used to guide the needle into the oval foramen, its limitation lies in its inability to demonstrate proximity to the target nerve or trigeminal ganglion. The absence of a uniform distance between the needle tip and the target nerve may account for the lack of consensus on RFT temperature in clinical practice. Sensory SV testing is used to pinpoint the needle location, demonstrating the distance to the target nerve: the smaller the distance, the lower the SV (Fig. 1). Moreover, the ablated area in thermocoagulation is controlled by temperature on the basis of in vivo and in vitro study. The temperature gradually decreases as the active tip of the heat source moves away from the target nerve [43]. For precise ablation of nociceptive fibers, it is logical to control the distance to the active tip of the needle based on the SV value. When the SV exceeds 0.6 V, suggesting that the needle tip is positioned too far from the target nerve for effective heat ablation, the doctor topically adjusts the needle’s position to evoke an aching and tingling sensation within the nerve distribution area at a voltage below 0.6 V. To further determine a suitable needle-to-nerve distance validated by the SV, enrolled patients were categorized into two groups: low SV (≤ 0.2 V) and high SV (0.3–0.6 V). This observational research aims to ascertain the possibility of selectively ablating fibers, potentially leading to reduced postoperative facial numbness, by varying SV values.
Post-operational facial numbness is a principal drawback impeding the pervasive application of this procedure [44]. Although facial numbness tends to be associated with long-term pain relief and decreased pain recurrence, the numbness that accompanies pain relief indicates that excessive heat poses a risk of ablating both nociceptive and tactile fibers [5, 12]. Notably, the facial numbness is a significant concern for ITN patients. In the most severe situations, this numbness can itself be very painful, leading to a condition known as anesthesia dolorosa. In this study, we employed sensory SV to regulate the ablation distance while using a thermocoagulation temperature of 70–75 °C for RFT treatment [14, 20]. The results demonstrated that an SV range of 0.3 to 0.6 V can be used to validate the distance between the needle tip and target nerve, significantly reducing the numbness degree. In the high SV group, 83.3% of patients reported mild numbness with no obvious impact on their daily lives and no patients experienced severe numbness. In contrast, only 25% of the patients in the low SV group reported mild numbness, while 66.67% experienced moderate numbness, indicating that numbness frequently affects quality of life. Moreover, 16.67% of patients reported severe facial numbness which consistently impacted their daily lives. Our results indicate that an SV of 0.3–0.6 V effectively reduces facial numbness when an RFT temperature of 70–75 °C is used.
Nevertheless, 16.67% of the patients in the high SV group still experienced moderate facial numbness. The variation observed primarily arises from interindividual differences in the neurological resistance to heat. In a prior study, we investigated whether monitoring the trigeminal somatosensory-evoked potential, which reflects the extent of ablation, could minimize the individual differences [45]. However, this monitoring technique is intricate and challenging to widely applied. Therefore, further studies, especially in hospitals that lack the ability to monitor the trigeminal somatosensory-evoked potential, are warranted to explore the value of monitoring the SV in RFT concerning interindividual differences, aiming to minimize facial numbness.
Other complications, including masseter muscle weakness, were comparable for the two groups. Fortunately, all cases of muscle weakness events recovered with time, and no other severe complications occurred. Furthermore, it is crucial to note that there was no mortality related to the RFT procedures.
The inherent limitations of retrospective studies temper the conclusions drawn from this matched cohort comparison. The use of follow-up data may lead to potential recall bias. Moreover, all cases originated from a single center, emphasizing the need for larger trials involving multiple centers. Despite these limitations, this case–control study establishes a robust foundation for subsequent multicenter randomized controlled trials (RCTs).
Conclusion
RFT is highly effective in alleviating pain associated with ITN. A relatively high sensory SV ranging from 0.3 to 0.6 V results in less facial numbness than a low SV of less than 0.2 V in the treatment of ITN. Maintaining an appropriate RFT ablation distance based on the intraoperative SV leads to the selective ablation of nociceptive fibers, preventing unintended damage to tactile fibers. These findings offer valuable insights that can help to mitigate facial numbness occurrences associated with RFT in the treatment of ITN.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Zakrzewska JM, McMillan R. Trigeminal neuralgia: the diagnosis and management of this excruciating and poorly understood facial pain. Postgrad Med J. 2011;87(1028):410–6.
Cruccu G, Gronseth G, Alksne J, Argoff C, Brainin M, Burchiel K, et al. AAN-EFNS guidelines on trigeminal neuralgia management. Eur J Neurol. 2008;15(10):1013–28.
Koopman JS, Dieleman JP, Huygen FJ, de Mos M, Martin CG, Sturkenboom MC. Incidence of facial pain in the general population. Pain. 2009;147(1–3):122–7.
Dieleman JP, Kerklaan J, Huygen F, Bouma PAD, Sturkenboom M. Incidence rates and treatment of neuropathic pain conditions in the general population. Pain. 2008;137(3):681–8.
Bendtsen L, Zakrzewska JM, Abbott J, Braschinsky M, Di Stefano G, Donnet A, et al. European Academy of Neurology guideline on trigeminal neuralgia. Eur J Neurol. 2019;26(6):831–49.
Zakrzewska JM, Lopez BC, Kim SE, Coakham HB. Patient reports of satisfaction after microvascular decompression and partial sensory rhizotomy for trigeminal neuralgia. Neurosurgery. 2005;56(6):1304–11.
Al-Quliti KW. Update on neuropathic pain treatment for trigeminal neuralgia. The pharmacological and surgical options. Neurosciences (Riyadh). 2015;20(2):107–14.
Howard SD, Soti V. How far has radiofrequency thermocoagulation come along as a treatment procedure in treating trigeminal neuralgia patients? Cureus. 2023;15(6): e40311.
Chong MS, Bahra A, Zakrzewska JM. Guidelines for the management of trigeminal neuralgia. Cleve Clin J Med. 2023;90(6):355–62.
Emril DR, Ho KY. Treatment of trigeminal neuralgia: role of radiofrequency ablation. J Pain Res. 2010;3:249–54.
Taha JM, Tew JM Jr. Comparison of surgical treatments for trigeminal neuralgia: reevaluation of radiofrequency rhizotomy. Neurosurgery. 1996;38(5):865–71.
Tang YZ, Wu BS, Yang LQ, Yue JN, He LL, Li N, et al. The long-term effective rate of different branches of idiopathic trigeminal neuralgia after single radiofrequency thermocoagulation: a cohort study. Medicine (Baltimore). 2015;94(45): e1994.
Tang YZ, Jin D, Bian JJ, Li XY, Lai GH, Ni JX. Long-term outcome of computed tomography-guided percutaneous radiofrequency thermocoagulation for classic trigeminal neuralgia patients older than 70 years. J Craniofac Surg. 2014;25(4):1292–5.
Hong T, Ding Y, Yao P. Long-term efficacy and complications of radiofrequency thermocoagulation at different temperatures for the treatment of trigeminal neuralgia. Biochem Res Int. 2020;2020:3854284.
Letcher FS, Goldring S. The effect of radiofrequency current and heat on peripheral nerve action potential in the cat. J Neurosurg. 1968;29(1):42–7.
Frigyesi TL, Siegfried J, Broggi G. The selective vulnerability of evoked potentials in the trigeminal sensory root of graded thermocoagulation. Exp Neurol. 1975;49(1 Pt 1):11–21.
Mittal B, Thomas DG. Controlled thermocoagulation in trigeminal neuralgia. J Neurol Neurosurg Psychiatry. 1986;49(8):932–6.
Kanpolat Y, Savas A, Bekar A, Berk C. Percutaneous controlled radiofrequency trigeminal rhizotomy for the treatment of idiopathic trigeminal neuralgia: 25-year experience with 1600 patients. Neurosurgery. 2001;48(3):524–32.
Sekimoto K, Koizuka S, Saito S, Goto F. Thermogangliolysis of the Gasserian ganglion under computed tomography fluoroscopy. J Anesth. 2005;19(2):177–9.
Tang YZ, Yang LQ, Yue JN, Wang XP, He LL, Ni JX. The optimal radiofrequency temperature in radiofrequency thermocoagulation for idiopathic trigeminal neuralgia: a cohort study. Medicine (Baltimore). 2016;95(28): e4103.
Yao P, Deng YY, Hong T, Wang ZB, Ma JM, Zhu YQ, et al. Radiofrequency thermocoagulation for V2/V3 idiopathic trigeminal neuralgia: effect of treatment temperatures on long-term clinical outcomes: a cohort study. Medicine (Baltimore). 2016;95(26): e4019.
Yao P, Hong T, Wang ZB, Ma JM, Zhu YQ, Li HX, et al. Treatment of bilateral idiopathic trigeminal neuralgia by radiofrequency thermocoagulation at different temperatures. Medicine (Baltimore). 2016;95(29): e4274.
Wang Z, Wang Z, Li K, Su X, Du C, Tian Y. Radiofrequency thermocoagulation for the treatment of trigeminal neuralgia. Exp Ther Med. 2022;23(1):17.
Mertyna P, Dewhirst MW, Halpern E, Goldberg W, Goldberg SN. Radiofrequency ablation: the effect of distance and baseline temperature on thermal dose required for coagulation. Int J Hyperthermia. 2008;24(7):550–9.
Obrzut SL, Hecht P, Hayashi K, Fanton GS, Thabit G 3rd, Markel MD. The effect of radiofrequency energy on the length and temperature properties of the glenohumeral joint capsule. Arthroscopy. 1998;14(4):395–400.
Shi W, Rudra R, Vu TN, Gordin Y, Smith R, Kunselman AR. Sensory stimulation threshold: a viable tool to improve the outcome of lumbar facet radiofrequency denervation? J Pain Res. 2021;14:2113–9.
Eskandar E, Kumar H, Boini A, Velasquez Botero F, El Hunjul GN, Nieto Salazar MA, et al. The role of radiofrequency ablation in the treatment of trigeminal neuralgia: a narrative review. Cureus. 2023;15(3): e36193.
Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia. 2004;24(Suppl 1):9–160.
Tang YZ, Jin D, Li XY, Lai GH, Li N, Ni JX. Repeated CT-guided percutaneous radiofrequency thermocoagulation for recurrent trigeminal neuralgia. Eur Neurol. 2014;72(1–2):54–9.
Li Y, Guo Y, Yang L, Ni J. Comparison of the short-term outcomes after low-temperature plasma radiofrequency ablation (coblation) in the Gasserian ganglion for the treatment of idiopathic trigeminal neuralgia. J Pain Res. 2019;12:1235–42.
Harden RN, Weinland SR, Remble TA, Houle TT, Colio S, Steedman S, et al. Medication Quantification Scale Version III: update in medication classes and revised detriment weights by survey of American Pain Society Physicians. J Pain. 2005;6(6):364–71.
Jannetta PJ. Arterial compression of the trigeminal nerve at the pons in patients with trigeminal neuralgia. J Neurosurg. 1967;26(1):159–62.
Tew JM Jr, Keller JT. The treatment of trigeminal neuralgia by percutaneous radiofrequency technique. Clin Neurosurg. 1977;24:557–78.
Wang DD, Raygor KP, Cage TA, Ward MM, Westcott S, Barbaro NM, et al. Prospective comparison of long-term pain relief rates after first-time microvascular decompression and stereotactic radiosurgery for trigeminal neuralgia. J Neurosurg. 2018;128(1):68–77.
Barker FGN, Jannetta PJ, Bissonette DJ, Larkins MV, Jho HD. The long-term outcome of microvascular decompression for trigeminal neuralgia. N Engl J Med. 1996;334(17):1077–83.
Elias WJ, Burchiel KJ. Microvascular decompression. Clin J Pain. 2002;18(1):35–41.
Resnick DK, Levy EI, Jannetta PJ. Microvascular decompression for pediatric onset trigeminal neuralgia. Neurosurgery. 1998;43(4):804–7.
Sweet WH, Wepsic JG. Controlled thermocoagulation of trigeminal ganglion and rootlets for differential destruction of pain fibers. 1. Trigeminal neuralgia. J Neurosurg. 1974;40(2):143–56.
Lopez BC, Hamlyn PJ, Zakrzewska JM. Systematic review of ablative neurosurgical techniques for the treatment of trigeminal neuralgia. Neurosurgery. 2004;54(4):973–82.
Teixeira MJ, Siqueira SR, Almeida GM. Percutaneous radiofrequency rhizotomy and neurovascular decompression of the trigeminal nerve for the treatment of facial pain. Arq Neuropsiquiatr. 2006;64(4):983–9.
Koopman JS, de Vries LM, Dieleman JP, Huygen FJ, Stricker BH, Sturkenboom MC. A nationwide study of three invasive treatments for trigeminal neuralgia. Pain. 2011;152(3):507–13.
Sterman-Neto H, Fukuda CY, Duarte KP, da Silva VA, Rodrigues ALL, Galhardoni R, et al. Balloon compression vs radiofrequency for primary trigeminal neuralgia: a randomized, controlled trial. Pain. 2021;162(3):919–29.
Vinas FC, Zamorano L, Dujovny M, Zhao JZ, Hodgkinson D, Ho KL, et al. In vivo and in vitro study of the lesions produced with a computerized radiofrequency system. Stereotact Funct Neurosurg. 1992;58(1–4):121–33.
Cheng JS, Lim DA, Chang EF, Barbaro NM. A review of percutaneous treatments for trigeminal neuralgia. Neurosurgery. 2014;10:25–33.
Zhao YX, Miao SH, Tang YZ, He LL, Yang LQ, Ma Y, et al. Trigeminal somatosensory-evoked potential: a neurophysiological tool to monitor the extent of lesion of ganglion radiofrequency thermocoagulation in idiopathic trigeminal neuralgia: a case-control study. Medicine (Baltimore). 2017;96(3): e5872.
Funding
This journal’s Rapid Service Fee and Open Access Fee were supported by Huhhot First Hospital and the Beijing Municipal Administration of Hospitals Incubating Program (code: PX2020033).
Author information
Authors and Affiliations
Contributions
Yuanzhang Tang designed the study, Aitao Wang, Jingjing Bian and Na Li drafted the manuscript. Jingjing Bian, Aitao Wang, Na Li and Jiaxiang Ni were responsible for the data collection. Yuanzhang Tang and Lea Zila carried out the statistical analyses and revised the article. Aitao Wang, Jingjing Bian and Na Li contributed equally to this paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
All of the authors/contributors—Aitao Wang, Jingjing Bian, Na Li, Jiaxiang Ni and Yuanzhang Tang—declare that they have no competing interests.
Ethical Approval
This retrospective cohort study was approved by the Medical Ethics Committee of Xuanwu Hospital, Capital Medical University (Beijing, China, LYS 2019-125). This study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Wang, A., Bian, J., Li, N. et al. Analyzing the Effect of Intraoperative Stimulation Voltage on Facial Numbness Following Radiofrequency Thermocoagulation in the Treatment of Idiopathic Trigeminal Neuralgia. Pain Ther 13, 543–555 (2024). https://doi.org/10.1007/s40122-024-00587-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40122-024-00587-5