
Abstract
We investigated the ophthalmologic manifestations and factors that influence outcomes in patients with myasthenia gravis (MG). We retrospectively analyzed the prevalence of neuro-ophthalmologic findings and clinical and outcome measures of 100 consecutive patients (53 males, 47 females), aged 55.7 ± 17.5 (range 15–85) years with an established diagnosis of MG. Forty-eight patients had purely ocular symptoms at the onset of disease (OMG) and 52 patients presented with generalized symptoms (GMG). Overall, 21 patients presented with extraocular muscle (EOM) weakness. Bilateral EOM weakness was seen in 12 patients, and unilateral EOM weakness was seen in nine patients. Diplopia responded partially to immunosuppressive treatments in 60% of patients with ophthalmoparesis. Twenty-five (52.1%) patients with ocular-onset MG converted to secondary GMG at a mean time of 14.5 months. Patients who developed secondary GMG were younger and had an earlier age of disease onset when compared with patients with pure OMG (p < 0.05). Patients with secondary GMG presented more frequently with ptosis and diplopia (72% vs. 28%) compared with patients with pure ocular MG who presented more frequently with isolated ptosis (66.7% vs. 33.3%) (p = 0.02). Remission and minimal manifestation status were achieved in 50 (79.3%) of all patients with a clinical follow-up ≥ 3 years. Poor outcome was associated with the presence of thymoma (p < 0.05). Myasthenic ophthalmoparesis is bilateral and heterogeneous and partly responds to treatment with immunotherapy. Younger patients with ptosis and diplopia at disease onset had an increased risk of secondary GMG. The presence of thymoma increases the risk for poor prognosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Myasthenia gravis (MG) is an uncommon autoimmune disorder targeting neuromuscular junctions, most commonly acetylcholine receptors (AChR) [1]. The initial presenting symptom in about half of all cases is limited to eyelid elevators, and extraocular muscles (EOMs) defined as ocular MG (OMG) [2]. Patients with OMG may subsequently progress to generalized MG (GMG) in 20–50% of cases, usually within 2 years of onset [3,4,5,6,7]. EOM involvement in MG is heterogeneous ranging from individual muscle palsy to complete external ophthalmoplegia and can mimic other oculomotor disturbances [8,9,10,11,12,13,14,15,16,17,18]. The previous reports about the ophthalmologic manifestations and outcomes of ocular findings in MG are limited [15,16,17,18].
In this single-center study, we systematically evaluated the different patterns of ocular involvement and factors that influence the outcomes of patients with MG and determined the risk factors for secondary generalization.
Method
Patient population
This retrospective study included 100 consecutive patients (53 males, 47 females), aged 55.7 ± 17.5 (range 15–85) years with an established diagnosis of MG who were evaluated at Istanbul Okmeydani Training and Research Hospital, Department of Neurology, Neuromuscular Disorders Outpatient Clinic between January 2013 and December 2019. Ethics approval for the study was obtained from the local ethics committee. The demographics of the patients, clinical and neuro-ophthalmologic findings, disease duration, electrophysiologic test results [including repetitive nerve stimulation (RNS), and single-fiber electromyography (EMG)], serologic and other laboratory data, computed tomography (CT) scans of the chest, thymectomy status and histopathology, history of myasthenic crisis, treatment, and outcome measures were entered into the database consecutively. All patients underwent chest CT at diagnosis. Congenital myasthenic syndromes (n = 2) were excluded based on a history of symptoms and neurologic findings. Patients with poor clinical documentation and uncertain diagnosis (n = 12) were excluded. No patients had a history of any co-existing medical or neurologic conditions affecting extraocular motility, such as mitochondrial myopathy, muscular dystrophy, thyroid orbitopathy, and prior strabismus surgery.
Definition and classification of myasthenia gravis
The diagnosis of MG was based on the presence of fatigable weakness and at least one (mostly two) of the following: (1) Seropositivity of either of anti-AChR antibody (anti-AChR-Ab) (above > 0.5 nmol/L) or antimuscle-specific kinase antibody (anti-MUSK-Ab) (above > 0.01 nmol/L) with a standard radioimmunoassay; (2) Abnormal results of electrophysiologic tests including more than 10% decreased amplitude of compound muscle action potential with 3 Hz RNS of the facial or accessory nerve and/or increased jitter (if mean jitter exceeded 36 µs and at least three individual potentials had jitter values greater than 55 µs) on volitional single-fiber EMG (SFEMG) of the frontalis or orbicularis oculi muscles [19, 20]; (3) Unequivocal clinical response to acetylcholinesterase inhibitors and/or immunosuppression with appropriate clinical symptoms and exclusion of alternative diagnosis. Seventy (70%) patients were positive for anti-AChR-Ab. Anti-Musk-Ab was available for 14 seronegative patients and positive in three patients. The RNS test was abnormal in 32 (62.7%) of the 51 tested patients. SFEMG was abnormal in 38 (95%) of the 40 tested patients. Of the 27 patients with a negative antibody assay, the diagnosis of MG was based on the abnormal RNS in six patients, abnormal SFEMG in 13, and favorable response to cholinesterase inhibitors, and/or steroids in eight patients.
All patients were regularly evaluated by the same neurologists (OA and/or LBK) at 2–6-month intervals and new symptoms, neurologic examination findings, treatments, treatment adverse effects, and outcomes were recorded systematically. OMG was defined as the presence of fatigable ptosis and/or diplopia with no limb, bulbar, or respiratory manifestations. Generalized MG (GMG) was defined as any symptoms beyond the extraocular muscles or eyelids including neck or extremity weakness, dysphagia, dysarthria, dyspnea, and dysphonia. The Maximum Myasthenia Gravis Foundation of America (MGFA) postintervention score (MGFA-PIS) was determined for the outcome at the last visit [20]. MGFA-PIS favorable outcomes included categories of complete stable remission, pharmacologic remission, and minimal manifestations for 1 year. Unfavorable outcomes included categories of improved, unchanged, worse, exacerbation, and died of MG. Patients with favorable outcome should not have received intravenous immunoglobulins (IVIG) or plasma exchange for the past 1 year [21].
Treatment protocol
Treatment protocols for patients with MG were planned according to international treatment guidelines [22]. Pyridostigmine was the initial treatment drug for all patients with MG. The average pyridostigmine dosage was 60 mg 2–5 times daily, as required. When the patients remained symptomatic under anticholinesterase treatment, immunosuppressive treatments were introduced. Prednisolone 0.5–1 mg/kg was given with an initial target dosage of 15–20 mg daily and increased as required, followed by gradual dose reduction on alternate-day administration. Azathioprine (2.5–3 mg/kg) was used as the first-line steroid-sparing agent. A few patients with refractory GMG were treated with rituximab. Patients with severe generalized disease whose symptoms could not be controlled with oral medications, bulbar muscle involvement and/or respiratory crises were treated with IVIG or plasma exchange as rescue therapy. Thymectomy was performed to all patients diagnosed with probable thymoma in thorax CT. In the absence of thymoma, thymectomy was recommended to all adult patients with a diagnosis of positive anti-AChR-Abs or seronegative GMG, onset of disease < 50 years, failed response to initial immunosuppressive treatments, intolerable side effects with immunosuppressive treatments, and relapse after immunosuppressive treatments [22].
Statistical analysis
For categorical variables, statistical analysis was performed using Fisher’s exact test or standard Chi-square tests where appropriate. The significance of the differences between groups for continuous variables was tested using a two-sided independent sample t test or the Mann–Whitney U two-sample test after testing for normal distribution of the data. The results were considered statistically significant when p < 0.05. The data analysis was performed using the SPSS statistics package version 21.0 (SPSS Inc, Chicago, IL).
Results
Clinical characteristics of the patients with MG
Overall, the mean age at onset for MG was 49.7 ± 18.5 (range, 12–84) years. Four patients were classified as having juvenile-onset (< 18 years), and 52 patients were classified as late-onset (> 50 years) MG. The male-to-female ratio was 1.1 (53% male) (Table 1). Twenty-eight (28%) patients had additional autoimmune diseases: 18 had thyroid disorders, 10 had allergic asthma, one had Sjogren’s syndrome, one had systemic lupus erythematosus (SLE), and one had polymyalgia rheumatica. Forty-eight (48%) patients had purely ocular symptoms at the onset of disease and 52 patients (52%) presented with generalized symptoms.
The most common presenting ocular symptoms in patients with MG was coexisting ptosis and diplopia in 56 (56%), and ptosis alone in 34 (34%) and diplopia without ptosis in 7(7%) patients. Of all patients, 59% presented with bilateral asymmetric and 27% with unilateral ptosis, whereas only 4% of patients presented with bilateral symmetric ptosis. Bilateral orbicularis oculi muscle weakness was detected in 87.6% (78/89) of all patients. Three patients underwent oculoplastic surgery due to ptosis at the beginning of the disease before the diagnosis of MG.
Overall, 21% of patients with MG presented with EOM weakness, all of whom reported diplopia. Nineteen patients had coexisting EOM weakness and ptosis and only two patients had isolated EOM weakness without ptosis. Bilateral EOM weakness was seen in 12 (57.1%) and unilateral EOM weakness was seen in 9 (42.9%) patients. Weakness of a single EOM was detected in five patients (23.8%) and all mimicked sixth-nerve paresis. Bilateral and combined asymmetric horizontal and vertical gaze palsy was observed in six patients (28.6%). Total ophthalmoplegia with near-complete limitation of duction in all gaze directions was observed in two (9.5%) patients (Table 1; Figs. 1 and 2). Eleven out of 21 patients with EOM weakness were positive for anti-AChR-Ab and two patients were positive for anti-Musk-Ab. Anti-AChR-Ab-positive patients were more frequent among patients without ophthalmoparesis (74.7% vs. 52.4%), without reaching statistical significance. The mean anti-AChR-Ab titer was significantly higher in patients without ophthalmoparesis (p = 0.02) (Table 2). Five patients with EOM weakness had an underlying thyroid disorder, all of whom were euthyroid. We found no significant difference regarding age, age of disease onset, sex, disease duration, presentation of symptoms, seropositivity, myasthenic crises, thymectomy status and thymoma, secondary generalization rates, treatments, and long-term remission rates between patients with and without EOM weakness (Table 2). The outcome of EOM weakness was assessed in 15 patients with at least 1-year follow-up. Although all of the patients with EOM weakness responded well to immunosuppressive drug therapy, nine out of 15 (60%) patients responded partially with mild EOM deficits and had recurrent symptoms of diplopia.

A male patient with anti-AChR-Ab-positive MG. Left prominent bilateral asymmetric ptosis is present. The patient had bilateral limitation of extraocular eye movements in all directions

A female patient with anti-Musk-Ab-positive MG. Right prominent bilateral asymmetric ptosis and bilateral orbicularis oculi muscle weakness is present. The patient had marked bilateral limitation of extraocular eye movements in horizontal directions and moderate bilateral limitation with infraduction
The most common presenting symptoms in patients with ocular-onset MG was coexisting ptosis and diplopia in 29 (60.4%), and isolated ptosis in 18 (37.5%) patients. Only one (2%) patient with ocular-onset MG presented solely with diplopia without ptosis. Patients with ocular-onset MG presented more frequently with unilateral ptosis (41.6%) compared with patients with generalized-onset MG (14%) (p = 0.01) (Table 1). The frequency of patients with late-onset MG (> 50 years) was significantly higher among patients with ocular-onset MG (64.6%) compared with patients with generalized-onset MG (40.4%) (p = 0.02, Table 1). Anti-AChR-Abs were detected in 60.4% of the patients with ocular-onset MG and 78.8% of the patients with generalized-onset MG. Three patients with anti-Musk-Ab presented as generalized-onset MG. We found no significant differences regarding the mean age of disease onset, sex, disease duration, seropositivity, anti-AChR-Ab titer, myasthenic crises, electrophysiologic findings, and the use of immunosuppressant treatments between patients who were initially diagnosed as having ocular-onset MG and generalized-onset MG (Table 1). Patients with generalized-onset MG were treated more frequently with thymectomy (44.2%) compared with patients with ocular-onset MG (22.9%) (p = 0.03). Thymoma was more frequently diagnosed in patients with generalized-onset MG (23%) compared with patients with ocular-onset MG (8.3%), without reaching statistical significance.
Prognosis
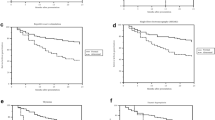
Of the 40 patients with ocular-onset MG with a minimum disease duration of 2 years, 15 (31.3%) patients remained purely ocular, whereas 25 (52.1%) patients progressed to secondary generalized MG (Table 3). The mean age of disease onset in patients with pure ocular MG was significantly higher than patients with secondary generalized MG (p = 0.04). Patients with secondary generalized MG presented more frequently with ptosis and diplopia (72% vs. 28%) compared with patients with pure ocular MG who presented more frequently with isolated ptosis (66.7% vs. 33.3%) (p = 0.02). We observed no significant association between the risk of conversion to generalized MG and sex, disease duration, seropositivity, anti-AChR-Ab titer, electrophysiologic findings, thymectomy status, thymoma, treatments, and neuro-ophthalmologic findings (Table 3). When the generalization occurred, the mean time from the onset of the first symptoms to generalization was 14.5 (range 2–36) months. None of the patients developed the generalized form of the disease 3 years after symptom onset. More than half of the patients (59%) converted to secondary generalized MG within the first year of symptom onset. Although most patients progressed to secondary generalized MG within two years after symptom onset, two patients converted within 3 years.
Long-term outcomes were analyzed in 63 patients with a mean disease duration of 8.1 ± 6.4 (range, 3–35) years. Remission and minimal manifestation status were achieved in 50 (79.3%) of all patients. None of the patients died during follow-up (Table 4). Favorable outcomes at the last visit included MM-3 in 36 (57.1%), MM-2 in 11 (17.5%), MM-1 in two (3.2%), and PR in one (1.6%) patient. Poor outcome was associated with the presence of thymoma (p = 0.007). We found no other significant association between prognosis and age of disease onset, sex, disease duration, presentation of symptoms, seropositivity, anti-AChR-Ab titer, electrophysiologic findings, thymectomy status, treatments, and neuro-ophthalmologic findings.
Treatment
Thymectomy was performed in 34 (34%) patients. With respect to the postoperative pathologic reports, thymoma was detected in 17 (50%), normal or atrophic thymus in 10 (29.4%), and hyperplastic thymus in 5 (14.7%) patients who underwent thymectomy. Pathologic reports were inaccessible in 2 (5.9%) patients. All of our patients treated with thymectomy had generalized disease except one who had thymoma-related ocular MG. In terms of medication, pyridostigmine alone was the treatment of choice in 15 patients. In 75 patients, corticosteroids, and in 52 patients, azathioprine was added as the second-line medication. In 45 out of 70 (64.3%) patients who received corticosteroids as the second-line therapy, azathioprine was introduced as add-on therapy due to a lack of efficiency or adverse effects of steroids. Three patients with treatment-refractory MG received rituximab (Table 1).
Discussion
This study shows, in a medium-sized cohort of patients from a single center, that MG-related ophthalmoparesis is observed in nearly one-fifth of patients and may cause long-term functional disability. Patients with unilateral ptosis appear to present more frequently as ocular-onset MG compared with patients with bilateral asymmetric ptosis who present more frequently as generalized-onset MG. Patients with the coexisting ptosis and diplopia at onset more frequently progressed into generalized MG, which has not been previously reported. Patients who developed secondary generalized MG were younger and had an earlier age of disease onset compared with patients with pure OMG. Prognosis was good in nearly 80% of all patients with a clinical follow-up at least 3 years. Poor outcome was associated with the presence of thymoma.
Regarding the clinical features at presentation, the most frequent initial ocular symptoms was coexisting ptosis and diplopia (56%). Ocular manifestation in MG appeared to be more bilateral and asymmetrical (59%), whereas symmetric ptosis (4%) and isolated diplopia (7%) were uncommon findings. Isolated diplopia in patients with MG was reported more frequently in the previous cohorts between 27 and 34% [4, 6].
In our patient cohort, bilateral and multiple EOM weakness was most frequently observed (12%). Such a presentation may suggest a misdiagnosis of central gaze disorder or mitochondrial myopathy. Previous studies reported no consistent pattern of ocular motility disturbances in patients with MG. Elevator muscles (inferior oblique and superior rectus) and medial rectus muscle have been reported as being more frequently involved than other ocular muscles [13, 14, 24, 25]. Unlike other studies, lateral rectus was the only isolated ocular muscle affected in our patient group. Ocular motility weakness mimicking isolated cranial nerve palsies, internuclear ophthalmoplegia, conjugate gaze palsies, one and a half syndrome, complete external ophthalmoplegia, and double elevator palsy have all been described in MG [8, 9, 12,13,14,15].
Bilateral orbicularis oculi weakness was seen in 87.6% of our patient group and would not be expected in other non-MG-related ocular motility disorders [2]. Nearly half of the patients with ocular gaze palsy had anti-AChR-Abs. We had no patients with anti-Musk-Ab-positive MG who presented with isolated ocular disease as reported rarely in the literature [15, 26].
In most of the patients under immunosuppressive therapy, EOM weakness rapidly remitted. However, despite immunotherapy, 60% of patients had recurrent symptoms of diplopia with mild EOM weakness during follow-up. Our patients did not have as severe persistent EOM weakness, but intermittent diplopia continued without full recovery. Former studies described a subset of patients who developed treatment-resistant ophthalmoplegia, and their non-ocular muscles responded to standard myasthenic therapies [17, 18, 24]. More aggressive immunotherapy with higher prednisone doses within 3 months is suggested for the resolution of myasthenic ophthalmoparesis [18]. Previous studies showed ocular muscle atrophy in patients with anti-AChR-Ab-positive GMG whose ocular symptoms responded poorly to treatment [27]. Few reports on EOM histopathology in MG-associated ophthalmoplegia revealed nonspecific fibrofatty changes and mitochondrial alterations in EOM muscles secondary to functional denervation and poor contractility [28, 29]. Gene polymorphisms in some of the differentially expressed genes in the EOMs may be related to an increased susceptibility of EOM in MG [30]. In a treatment-resistant ophthalmoplegic subphenotype of patients with MG with African genetic ancestry, potential gene variants, dysregulating myogenesis, and gangliosphingolipid biosynthesis pathways contributing to the synaptopathy at the extraocular neuromuscular junction were defined [17, 31]. Hashimoto’s thyroiditis might rarely cause ophthalmopathy in the euthyroid state with a good response to steroids and should be considered in the differential diagnosis of patients [32]. Ptosis and diplopia in MG may interfere with daily activities and result in significant disability. For patients who remain diplopic despite medical therapy, prism therapy, or strabismus surgery may be an effective alternative [2].
In our database, ocular symptoms led to a diagnosis of MG in 48% of patients, which was similar to those reported in earlier studies [6, 7]. Later age of disease onset was more frequently observed in our patient group with ocular-onset MG (64.6%), as previously mentioned [33, 34]. Antibodies against the acetylcholine receptor confirm the immunopathologic features of the disease and are present in 60.4% of the ocular-onset MG and 78.8% of the generalized-onset MG. Previous studies reported the presence of anti-AChR-Abs in patients with OMG between 30 and 83% [4,5,6,7, 23, 33, 34]. During the course of the disease, 52.1% of patients with ocular-onset MG evolved to secondary generalized MG over a mean follow-up of 14.5 months. Previous studies reported a longer transformation time of up to 5 years [6]. Patients who developed secondary generalized MG were younger and had an earlier age of disease onset compared with patients with pure OMG. Lower rates of secondary generalization in older patients have been reported in previous studies [33, 34]. The reported rate of conversion to GMG is quite variable in earlier studies between 9.4% and 85%, possibly due to different durations of follow-up periods, different inclusion criteria, and the possible effect of immunosuppressive treatment [4,5,6,7, 10, 23, 33, 35]. In our cohort, patients with more than one ocular symptom (ptosis and diplopia) at onset more frequently progressed into generalized MG. Wang et al. reported that single onset symptoms of OMG such as ptosis or diplopia predicted early conversion to GMG than co-occurrence of ptosis and diplopia [36]. Consistent with some studies, but in contrast with others, no predictive factors for progression to secondary generalized MG were found regarding sex, rate of seropositivity, titer of anti-AChR-Abs, and abnormal electrodiagnostic test results [4,5,6, 10, 35,36,37].
Nearly two-thirds of our patients with pure ocular MG required treatment with immunosuppressive drugs for the control of their symptoms. Prior studies have shown a higher incidence of remission and lower risk of progression to GMG in individuals treated with corticosteroids [10, 38]. Our patient group was too small for this subgroup analysis. Nearly 80% of our patient group had favorable outcomes, which corroborates with previous studies [23, 39]. The presence of pathologically confirmed thymoma was the only factor that was associated with unfavorable outcomes, as previously mentioned [40].
The interpretation of our data is hampered by its retrospective design, and measurement errors by the authors were possible because neuro-ophthalmologic examinations with Maddox rod or prism evaluations are not performed routinely. Hence, the number of patients with ophthalmoparesis may be underestimated among patients with symptoms of diplopia. We did not systematically assess the degree of ophthalmoparesis. However, patients were assessed by the same neurologists in a standardized pattern and information on clinical examination, treatments, and outcomes were well documented. Our results regarding the clinical features and prognosis are in accordance with previous studies. Sample sizes in some subgroup analyses were too small, which could result in missing potential factors that influence outcomes. Not all of the patients with negative anti-AChR-Ab test results were tested for anti-Musk-Ab. Some patients might have presented to clinics after their ocular symptoms had already progressed and generalized. Especially in older patients who might report nonspecific fatigue, mild generalized-onset MG could be misclassified as ocular onset MG or vice versa, which might impede the categorization of the disease into subgroups as ocular or generalize-onset MG [37].
In conclusion, our study confirms that myasthenic ophthalmoparesis is usually bilateral and heterogeneous and partly responds to immunotherapy. Bilateral ptosis is associated with generalized onset MG. Diplopia and ptosis at the onset of disease might suggest conversion to secondary generalized MG. Younger patients with an earlier disease onset convert to secondary generalized MG frequently. The presence of thymoma increases the risk for poor prognosis.
References
Gilhus NE, Verschuuren JJ (2015) Myasthenia gravis: subgroup classification and therapeutic strategies. Lancet Neurol 14:1023–1036. https://doi.org/10.1016/S1474-4422(15)00145-3
Smith SV, Lee AG (2017) Update on ocular myasthenia gravis. Neurol Clin 35:115–123. https://doi.org/10.1016/j.ncl.2016.08.008
Benatar M, Sanders DB, Wolfe GI, McDermott MP, Tawil R (2012) Design of the efficacy of prednisone in the treatment of ocular myasthenia (EPITOME) trial. Ann N Y Acad Sci 1275:17–22. https://doi.org/10.1111/j.1749-6632.2012.06780.x
Nagia L, Lemos J, Abusamra K, Cornblath WT, Eggenberger ER (2015) Prognosis of ocular myasthenia gravis: retrospective multicenter analysis. Ophthalmology 122:1517–1521. https://doi.org/10.1016/j.ophtha.2015.03.010
Teo KY, Tow SL, Haaland B, Gosavi TD, Jing-Liang L, Yew Long LO, Milea D (2018) Low conversion rate of ocular to generalized myasthenia gravis in Singapore. Muscle Nerve 57:756–760. https://doi.org/10.1002/mus.25983
Hendricks TM, Bhatti MT, Hodge DO, Chen JJ (2019) Incidence, epidemiology, and transformation of ocular myasthenia gravis: a population-based study. Am J Ophthalmol 205:99–105. https://doi.org/10.1016/j.ajo.2019.04.017
Li F, Hotter B, Swierzy M, Ismail M, Meisel A, Rückert JC (2018) Generalization after ocular onset in myasthenia gravis: a case series in Germany. J Neurol 265:2773–2782. https://doi.org/10.1007/s00415-018-9056-8
Bandini F, Faga D, Simonetti S (2001) Ocular myasthenia mimicking a one-and-a-half syndrome. J Neuroophthalmol 21:210–211. https://doi.org/10.1097/00041327-200109000-00010
Das JC, Chaudhuri Z, Bhomaj S, Sharma P, Aggarwal M (2002) Ocular myasthenia presenting as progressive external ophthalmoplegia. J Pediatr Ophthalmol Strabismus 39:52–54
Kupersmith MJ, Ying G (2005) Ocular motor dysfunction and ptosis in ocular myasthenia gravis: effects of treatment. Br J Ophthalmol 89:1330–1334. https://doi.org/10.1136/bjo.2004.063404
Benatar M, Kaminski HJ, Quality Standards Subcommittee of the American Academy of Neurology (2007) Evidence report: the medical treatment of ocular myasthenia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 68:2144–2149. https://doi.org/10.1212/01.wnl.0000263481.14289.90
Argyriou AA, Karanasios P, Potsios C, Makridou A, Doukas V, Koukopoulou I, Makris N (2009) Myasthenia gravis initially presenting with pseudo-internuclear ophthalmoplegia. Neurol Sci 30:387–388. https://doi.org/10.1007/s10072-009-0106-y
Cleary M, Williams GJ, Metcalfe RA (2008) The pattern of extra-ocular muscle involvement in ocular myasthenia. Strabismus 16:11–18. https://doi.org/10.1080/15569520701830992
Almog Y, Ben-David M, Nemet AY (2016) Inferior oblique muscle paresis as a sign of myasthenia gravis. J Clin Neurosci 25:50–53. https://doi.org/10.1016/j.jocn.2015.08.026
Evoli A, Alboini PE, Iorio R, Damato V, Bartoccioni E (2017) Pattern of ocular involvement in myasthenia gravis with MuSK antibodies. J Neurol Neurosurg Psychiatry 88:761–763. https://doi.org/10.1136/jnnp-2017-315782
Al-Haidar M, Benatar M, Kaminski HJ (2018) Ocular Myasthenia. Neurol Clin 36:241–251. https://doi.org/10.1016/j.ncl.2018.01.003
Heckmann JM, Nel M (2018) A unique subphenotype of myasthenia gravis. Ann N Y Acad Sci 1412:14–20. https://doi.org/10.1111/nyas.13471
Europa TA, Nel M, Heckmann JM (2018) Myasthenic ophthalmoparesis: time to resolution after initiating immune therapies. Muscle Nerve 58:542–549. https://doi.org/10.1002/mus.26172
Stålberg E (2012) Jitter analysis with concentric needle electrodes. Ann N Y Acad Sci 1274:77–85. https://doi.org/10.1111/j.1749-6632.2012.06775.x
Sirin NG, Orhan EK, Durmus H, Oflazer P, Parman Y, Oge AE, Deymeer F, Baslo MB (2017) Jitter measurement using a concentric Needle in 133 patients with myasthenia gravis: a retrospective analysis. Neurol Sci Neurophysiol 34:207–214. https://doi.org/10.24165/jns.10168.17
Jaretzki A 3rd, Barohn RJ, Ernstoff RM, Kaminski HJ, Keesey JC, Penn AS, Sanders DB (2000) Myasthenia gravis: recommendations for clinical research standards. Task Force of the Medical Scientific Advisory Board of the Myasthenia Gravis Foundation of America. Neurology 55:16–23. https://doi.org/10.1212/wnl.55.1.16
Sanders DB, Wolfe GI, Benatar M, Evoli A, Gilhus NE, Illa I, Kuntz N, Massey JM, Melms A, Murai H, Nicolle M, Palace J, Richman DP, Verschuuren J, Narayanaswami P (2016) International consensus guidance for management of myasthenia gravis: executive summary. Neurology 87:419–425. https://doi.org/10.1212/WNL.0000000000002790
Beekman R, Kuks JB, Oosterhuis HJ (1997) Myasthenia gravis: diagnosis and follow-up of 100 consecutive patients. J Neurol 244:112–118. https://doi.org/10.1007/s004150050059
Kim JH, Hwang JM, Hwang YS, Kim KJ, Chae J (2003) Childhood ocular myasthenia gravis. Ophthalmology 110:1458–1462. https://doi.org/10.1016/S0161-6420(03)00460-3
Oosterhuis HJ (1982) The ocular signs and symptoms of myasthenia gravis. Doc Ophthalmol 52:363–378
Bennett DL, Mills KR, Riordan-Eva P, Barnes PR, Rose MR (2006) Anti-MuSK antibodies in a case of ocular myasthenia gravis. J Neurol Neurosurg Psychiatry 77:564–565. https://doi.org/10.1136/jnnp.2005.075812
Okamoto K, Ito J, Tokiguchi S, Furusawa T (1996) Atrophy of bilateral extraocular muscles. CT and clinical features of seven patients. J Neuroophthalmol 16:286–288
Gratton SM, Herro A, Bermudez-Magner JA, Guy J (2014) Atrophy and fibrosis of extra-ocular muscles in anti-acetylcholine receptor antibody myasthenia gravis. Open J Ophthalmol 4:117. https://doi.org/10.4236/ojoph.2014.44019
Rautenbach RM, Pillay K, Murray ADN, Heckmann JM (2017) Extraocular muscle findings in myasthenia gravis associated treatment-resistant ophthalmoplegia: a case report. J Neuroophthalmol 37:414–417. https://doi.org/10.1097/WNO.0000000000000534
Liu R, Xu H, Wang G, Li J, Gou L, Zhang L, Miao J, Li Z (2013) Extraocular muscle characteristics related to myasthenia gravis susceptibility. PLoS ONE 8:e55611. https://doi.org/10.1371/journal.pone.0055611
Nel M, Jalali Sefid Dashti M, Gamieldien J, Heckmann JM (2017) Exome sequencing identifies targets in the treatment-resistant ophthalmoplegic subphenotype of myasthenia gravis. Neuromuscul Disord 27:816–825. https://doi.org/10.1016/j.nmd.2017.06.009
Tateno F, Sakakibara R, Kishi M, Ogawa E (2011) Hashimoto’s ophthalmopathy. Am J Med Sci 342:83–85. https://doi.org/10.1097/MAJ.0b013e318219bcf6
Allen JA, Scala S, Jones HR (2010) Ocular myasthenia gravis in a senior population: diagnosis, therapy, and prognosis. Muscle Nerve 41:379–384. https://doi.org/10.1002/mus.21555
Cortés-Vicente E, Álvarez-Velasco R, Segovia S, Paradas C, Casasnovas C, Guerrero-Sola A, Pardo J, Ramos-Fransi A, Sevilla T, López de Munain A, Gómez MT, Jericó I, Gutiérrez-Gutiérrez G, Pelayo-Negro AL, Martín MA, Mendoza MD, Morís G, Rojas-Garcia R, Díaz-Manera J, Querol L, Gallardo E, Vélez B, Albertí MA, Galán L, García-Sobrino T, Martínez-Piñeiro A, Lozano-Veintimilla A, Fernández-Torrón R, Cano-Abascal Á, Illa I (2020) Clinical and therapeutic features of myasthenia gravis in adults based on age at onset. Neurology 94(11):e1171–e1180
Aguirre F, Villa AM (2018) Prognosis of ocular myasthenia gravis in an Argentinian population. Eur Neurol 79:113–117. https://doi.org/10.1159/000487132
Wang L, Zhang Y, He M (2017) Clinical predictors for the prognosis of myasthenia gravis. BMC Neurol 17(1):77. https://doi.org/10.1186/s12883-017-0857-7
Hong YH, Kwon SB, Kim BJ, Kim BJ, Kim SH, Kim JK, Park KS, Park KJ, Sung JJ, Sohn EH, Lee YB, Jeong D, Joo IS, Choi BO, Choi YC; Korean Research Group for Neuromuscular Diseases (2008) Prognosis of ocular myasthenia in Korea: a retrospective multicenter analysis of 202 patients. J Neurol Sci 273:10–14. https://doi.org/10.1016/j.jns.2008.05.023
Monsul NT, Patwa HS, Knorr AM, Lesser RL, Goldstein JM (2004) The effect of prednisone on the progression from ocular to generalized myasthenia gravis. J Neurol Sci 217:131–133. https://doi.org/10.1016/j.jns.2003.08.017
Yildiz Celik S, Durmus H, Yilmaz V, Saruhan Direskeneli G, Gulsen Parman Y, Serdaroglu Oflazer P, Deymeer F (2020) Late-onset generalized myasthenia gravis: clinical features, treatment, and outcome. Acta Neurol Belg 120:133–140. https://doi.org/10.1007/s13760-019-01252-x
Romi F (2011) Thymoma in myasthenia gravis: from diagnosis to treatment. Autoimmune Dis 2011:474512. https://doi.org/10.4061/2011/474512
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author(s) declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Akan, O., Baysal-Kirac, L. Ophthalmologic manifestations in myasthenia gravis: presentation and prognosis. Acta Neurol Belg 121, 1131–1140 (2021). https://doi.org/10.1007/s13760-020-01556-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13760-020-01556-3