
Abstract
The aim of the present study was to assess the prevalence of depression in a large multiple sclerosis (MS) patient group and to analyse the physical and psycho-socio-economic factors that influence its frequency and severity. In total, 351 consecutive patients with a diagnosis of MS were included in this study. All the patients completed a survey about their demographic characteristics, marital status, presence of children, employment status, educational level, duration of disease, disease course, duration of treatment and type of disease modifying therapies (DMT). Their disability level was evaluated using the Expanded Disability Status Scale (EDSS). Their depression level was evaluated using the Romanian Version (2012) of the Beck Depression Inventory-II (BDI-II). There was a significant positive correlation between the BDI-II score and the actual age of the patients, their disease duration, EDSS and the number of total relapses. From the EDSS functional scores, only the pyramidal score and the sensitive score presented a significant association with BDI-II in the logistic regression analysis. The BDI-II values decreased significantly with increasing education level. In the case of the retired patients, the BDI-II values were significantly higher. The BDI-II scores were also higher in widowers and divorced patients and in patients with children. There was no significant difference in the BDI-II values between different DMT groups. The main physical and psycho-socio-economic determinants of depression in patients with MS are the physical disability, disease duration, number of relapses, marital status, education level, employment status, and the presence of children, but many unsolved questions remain about the interrelations and relative contributions of these factors, which necessitates further research. The DMTs did not significantly influence the depression level.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Multiple sclerosis (MS) is one of the most disabling diseases of the central nervous system and affects 1 in 1000 people in Western countries [1]. Until recently, the severity of MS was measured only by taking into account the physical disability (motor weakness, visual loss, brainstem, cerebellar, sensitive, and autonomic symptoms); however, in the last few years, special attention has been directed towards the neuropsychological and neuropsychiatric manifestations of the disease [2].
The psychiatric symptoms in MS were first noted by Charcot in his lectures at the Salpetriere hospital in the nineteenth century when he described depression, mania, euphoria, hallucinations, and pathological laughing in his patients [3, 4].
Epidemiologic studies have indicated that the lifetime prevalence of major depression in MS patients is between 36 and 54 %, much higher compared to the general population (16.2 %) or even when compared to other chronic neurological conditions with similar levels of physical disability, such as temporal lobe epilepsy and amyotrophic lateral sclerosis [5, 6]. However, recent studies did not find differences in depressive symptomatology between MS and another chronic medical condition, after controlling for physical impairment [7].
Fernández-Jiménez and Arnett analysed the relative importance of factors that predict the quality of life in MS patients using multiple regression metrics in order to solve the colinearity problems. They compared different variables such as the Expanded Disability Status Scale (EDSS), depressive symptomatology, as measured by the Beck Depression Inventory-Fast Screen (BDI-FS), cognitive performance and coping. They concluded that EDSS and BDI-FS are relevant determinants of the quality of life in patients with MS [8].
It was thought originally that depression was a stress reaction following the diagnosis of a chronic, extremely disabling disease with an uncertain prognosis, but recent studies have shown that depression is also present in patients with minor or no physical disability. Due to the research conducted in this area in recent years, it is now known that, in the pathogenesis of depression in patients with MS, several pro-inflammatory cytokines (interferon-γ, tumour necrosis factor-α, interleukin-6) and structural brain changes are involved. Depression also seems to be an independent predictive factor for the quality of life of patients with MS as it may exacerbate fatigue, compromise cognitive functions, decrease compliance with treatment, affect work performance and family and social relationships of patients, and, not least, it is also an important risk factor for suicide [9–11].
Despite the negative impact that depression has on patients with MS, it is often overlooked in routine physical examination, or when diagnosed, it is not properly treated [10]. In Romania, the prevalence of MS is 22.6/100,000 people, therefore around 5000 people are affected by the disease [12].
The objectives of the present study were to assess the prevalence of depression in a large MS patient group and to analyse the physical and psycho-socio-economic factors that influence its frequency and severity.
Materials and methods
In total, 351 consecutive patients with a diagnosis of clinically isolated syndrome (CIS), relapsing remitting multiple sclerosis (RRMS) and secondary progressive multiple sclerosis (SPMS), according to McDonald’s diagnostic criteria 2010 [13], who attended the Regional MS Centre, Targu Mures, Romania, were included in this cross-sectional study that took place between September 2014 and February 2015. The study was performed in accordance with the principles stated in the Declaration of Helsinki and was approved by the local ethics committee. All the patients signed informed consent to participate in the study. All the patients included in this study were over 18 years old and were on treatment with the disease modifying therapies (DMT): Avonex, Betaferon, Copaxone, Rebif or Tysabri. The exclusion criteria were: (1) use of anti-depressant medications in the last 2 months; (2) corticosteroid treatment in the last 30 days; (3) were attending the MS Centre because of an MS relapse; (4) patients included in clinical trials with experimental therapies.
All the patients completed a survey that included questions on their demographic characteristics, such as age and sex, marital status, presence of children, employment status, educational level, duration of disease, disease course, duration of treatment, and type of DMT.
Patients’ disability level was evaluated using the physician-reported EDSS, which is a unified scale to evaluate the level of neurological impairment in MS patients in eight functional systems [14].
Depression level was evaluated using the Romanian version (2012) of the BDI-II, which is an instrument that consists of 21 questions. A score between 11 and 16 indicates a mild mood disorder, 17–20 indicates borderline depression, 21–30 indicates mild depression, 31–40 indicates severe depression, and a score above 40 indicates extremely severe depression [15].
Statistical analysis
For all the statistical calculations, Graph Pad 3.6 State Software, San Diego, California, USA, was utilised. To assess the normality of the continuous variables (e.g. age, disease duration, BDI-II score, EDSS, etc.), the Shapiro–Wilk test was applied. The Student’s t test was used to assess the differences between the means of the continuous variables (expressed as mean ± SD), while the differences between the non-parametric variables (expressed as median, range) were compared using the Mann–Whitney test. The differences among the other variables were estimated using the Kruskal–Wallis test, an analysis which is appropriate for more than two groups. By using Dunn’s multiple comparison tests, we found the groups between which there was a statistical significance. To assess the associations between the distributions of categorical variables, we used contingency tables and the Chi-squared test. The correlation between the quantitative variables was assessed using correlation or Spearman’s rho, when appropriate. We calculated the odds ratio (OR) to demonstrate the probability or susceptibility to depression. A multivariate analysis was carried out using linear regression. We used the BDI-II as the dependent variable. We included as independent variables the education level, employment status, marital status, the presence of children, etc. We interpreted all the tests against a p = 0.05 significance threshold and the statistical significance was considered for p values below the significance threshold.
Results
The demographic data, social and familial background, main clinical and DMT data of the whole patient group and separate to BDI-II score groups are shown in Table 1.
The mean age of the whole patient group was 42.9 ± 9.6 years. The mean BDI-II score of the whole patient group was 11.8 ± 10.3, while the median was 9 (min–max: 0–55). The histogram of these data is shown in Fig. 1.

The histogram of BDI sores
There was a significant positive correlation between the BDI-II score and the age of the patients (Fig. 2).

Correlation between the BDI score and the current age of the patients
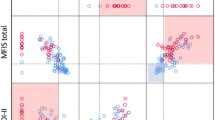
The BDI-II values were significantly higher in the patient group with an age >45 years (median 13.0, min 0, max 55) versus the group with an age ≤45 years (median 6.0, min 0, max 47), p = 0.0001, Mann–Whitney test. There was also a positive correlation between the BDI-II score and the age of the patients at the onset of the disease (r = 0.18, p = 0.0004). There was no significant difference between the male and female patient group regarding the BDI-II score. The mean disease duration in the whole patient group was 11.26 ± 6.81 years, while the mean disease duration before treatment was 4.6 ± 5.45 years and the mean disease duration on treatment was 6.63 ± 3.91 years. A significant positive correlation was found between the disease duration and the BDI-II scores (r = 0.18, p = 0006). The correlation was also significant between BDI-II and disease duration before and on treatment (r = 0.14, p = 0.007, r = 0.12, p = 0.02). The mean EDSS value was 2.96 ± 2.05. There was a significant correlation between the EDSS and BDI-II score (r = 0.45, p < 0.0001) (Fig. 3). From the EDSS functional scores, only the pyramidal score and sensitive score presented a significant association with BDI-II in the logistic regression analysis (OR 1.39, CI 95 % 1.04–1.87, p = 0.024, OR 1.35, CI 95 % 1.03–1.77, p = 0.027, where BDI-II was the dependent variable, and the functional scores—visual, brainstem, pyramidal, cerebellar, sensitive, bowel and bladder, cerebral and ambulation were the independent variables).

Correlation between the BDI scores and EDSS
In a multivariate regression model including BDI-II as the dependent variable and the age at disease onset, disease duration and current EDSS as independent variables, the BDI-II was significantly influenced by the age at disease onset (p = 0.003) and current EDSS (p < 0.0001), but was not influenced by disease duration (p = 0.25).
Moderate, severe and extreme depression were found more frequently in the SPMS group (p = 0.0001) compared with the RRMS and CIS groups. Moderate depression was found in 12.8 % of SPMS patients, 9.3 % of RRMS patients and 0 % in the CIS group, while severe and extreme depression was found in 17.0, 3.2 and 0.0 % of patients in the same groups, respectively. Another significant correlation was found between the severity of depression and the number of total relapses (r = 0.36, p < 0.0001) and the number of the relapses in the last year (r = 0.109, p = 0.04). In a logistic regression model, BDI-II was influenced significantly only by the number of total relapses. The OR for clinically significant depression (BDI-II ≥ 17) was 1.08 (95 % CI 1.02–1.13, p = 0.0022) for the number of total relapses and 1.07 (95 % CI 0.75–1.52, p = 0.7) for the number of relapses in the last year.
Taking into account the education level, the BDI-II values decreased significantly with increasing education level (p = 0.0001) (Fig. 4). The employment status of the patients had a significant influence on the depression level, e.g. in the case of retired patients (both age-based retired patients and those receiving a disability pension), the BDI-II values were significantly higher (p = 0.0001) (Fig. 4). The marital status of the patient also had a significant effect on the depression level. The BDI-II scores were higher in widowers and divorced people, while the lowest BDI-II values were found in the single patient group (p = 0.004) (Fig. 4). In the patient group with children, the BDI-II values were significantly higher (p = 0.02) (Fig. 4).

The relationship between BDI scores, education level, employment status, marital status and presence of children (Kruskal–Wallis tests). ES elementary school, AS apprentice school, HS high school, TVHS technical and vocational high school, U university, M/PhD master or PhD
In a logistic regression model, after the adjustment for age (including only for patients >30 years old), the OR for clinically significant depression was 3.45 (95 % CI 1.8–6.3, p = 0.0001) among the retired patients group and 2.68 (95 % CI 1.4–4.8, p = 0.001) for patients with a low education level (<12 years of school), while the association was not significant for marital status and for the presence of children. There was no significant difference in BDI-II values between the different DMT groups.
Discussion
The frequency of depression in MS patients is high, but varies significantly according to the studied population and the research methods used. Some researchers have studied the lifetime prevalence, while others have looked at the current point in the disease course.
The majority of the published literature data include only a relatively small cohort of MS patients. There are only a few studies with population-based data. Patten et al. [16] examined 115,071 patients older than 18 years, 322 of them with MS, using the Composite International Diagnostic Interview Short Form for Major Depression. The 12-month prevalence of depression was 25.7 % in the MS group, and only 8.9 % in those patients without MS [16]. Chwastiac et al. used a mail-based survey that included 1374 MS patients and achieved a 54 % response rate, and found that 29.1 % of the MS patients had moderate and severe depression levels according to the Centre for Epidemiological Studies’ Depression Scale [1]. Sadovnick et al. examined 221 MS patients from an MS clinic. They found that 34.4 % of them had a current lifetime diagnosis of depression and the cumulative risk for developing depression by the age of 59 was 50.3 % [11]. Minden et al. [17] found that 54 % of MS patients developed major depression at least once during the disease course. In our MS patient group, 27.05 % of the patients (95/351) had clinically significant depression.
The explanation for this high prevalence of depression in MS patients is debatable and it is difficult to conclude that it is only secondary to the burden of a disabling neurological disease, since there are other more disabling disorders, such as amyotrophic lateral sclerosis, with significantly lower depression rates [6, 18].
We found a strong association between depression and the severity of MS as indicated by EDSS. Of the eight functional systems of the EDSS, the pyramidal and sensitive scores had the strongest association with depression level. In a logistic regression analysis, the OR for clinically significant depression for pyramidal symptoms was 1.39 (95 % CI 1.04–1.87, p = 0.024) and 1.35 for sensitive symptoms (95 % CI 1.03–1.77, p = 0.027).
The literature regarding the association between depression and disability is controversial. Chwastiak et al. found a positive relationship between the disability level and depression. Patients with intermediate and severe disability according to EDSS were found to be three and six times as likely to have clinically significant depression compared with patients with minimal disability [1]. According to Smith et al., physical disability is an independent significant predictor of depression. Miletic et al. found a significant correlation between BDI and EDSS [19, 20]. Williams found no association between overall disability and depression, but falls and bowel dysfunction were positively associated with increased levels of depression [20]. Zephir et al. and Bakhsi et al. found no association between depression and disability [22, 23].
According to Chwastiak et al., the prevalence of severe depression decreases in patients with a longer duration of MS due to the adaptation to illness over time, but in our sample we obtained a significant positive correlation between the BDI-II score and the duration of MS [1]. In a study published in 2003, Patten et al. found that the prevalence of major depression was higher in younger patients (<45 years old), probably due to the development of coping strategies in older patients. In our study, the level of depression was significantly higher in older patients (>45 years old) [16]. This might be explained by disability progression over time, which will decrease the level of independence and will have a negative impact on social life and working ability, as well as possibly by the deficiencies in our social support system compared with Western societies. However, younger patients in our society have stronger social support, mainly from their parents.
The level of depression in the general population is 1.7–2.0 times higher in females compared to males, so we expected to obtain a similar result in our sample, but no significant difference between these two groups regarding BDI-II score was found [24]. There are controversial literature data about gender in MS-associated depression. Patten et al. found that women with MS presented a significantly higher prevalence of depression compared with males. Of the 99 female patients in their study, 28 % had major depression, but only 8 % of the male patients had major depression [25]. Galeazzi et al. and Korostil et al. published similar findings [26, 27]. Beal et al. explain the higher prevalence of depression in females by the fact that women have weaker social support and higher social expectations of the illness [28]. Several studies in accordance with our data found no significant difference in depression between genders. They suggested that this lack of association is due to hormonal and biological factors [1, 29].
In our study group, high levels of depression were associated with lower education. The same results were obtained by Bamer et al. and by Aşiret et al. A higher level of education can contribute to a better understanding of the disease, its symptoms and evolution, can improve the capacity to cope with the stress caused by the diagnosis of a disease with a high disability potential and can help dealing with the problems rather than avoiding them. Education also assumes better skills for interpersonal communication, thus facilitating a good level of support [30, 31].
Other determinants of depressive symptoms in our sample seem to be employment status, marital status, and having children. In retired patients (both age-based retired patients and those receiving a disability pension), we found significantly higher BDI-II scores. Given the current condition for pensioners in our country, this fact might be explained by a low economic condition. Regarding marital status, depressive symptoms were found more frequently in divorced patients and widowers. We expected this result because this group of patients has additional risk factors for developing depressive symptoms, such as loss of a spouse or going through a divorce, but we did not expect that the lowest depression levels would occur in the single patients group compared to married patients or those living with a partner. These results were maintained even after adjustments for age.
In the patients group that have children, we found significantly higher BDI-II scores compared to MS patients without children, probably due to the unpredictable disease evolution, high risk of severe disability and uncertainty about the future [31].
We found little data in the literature regarding depression, or regarding the type of clinical course (RRMS vs SPMS). The higher prevalence of clinically significant depression in our SPMS patients is probably due to the higher disability level and the longer disease duration in this group. Möller et al. and Minden et al. found no significant difference regarding depression between these patient groups [17, 32].
We found no literature data regarding the association between the total number of relapses, the number of relapses in the last year before evaluation and the depression level. However, there exist some data about the depression level during and post MS relapse. Moore et al. found high rates of possible depression during relapses [33].
We found no significant difference between the different DMTs. Literature data regarding these aspects are debatable. There is no strong evidence supporting the view that some of the DMTs predispose patients towards depression or exacerbate the pre-existing depression level. Zephir et al. and Patten et al. analysed the influence of interferon beta 1a treatment on depression in MS. They found no evidence of increased depression levels in association with this DMT [22, 34]. Patten et al. analysed the level of depression in two different DMT groups (interferon beta 1a and Copaxone). They found no significant difference regarding depression levels between these groups. The same authors concluded that ‘depression is not a side effect of interferon beta 1a′ when used in the treatment of patients with SPMS [35].
Conclusions
The prevalence of clinically significant depression in MS is high. MS physicians should be aware of this disabling comorbidity for early diagnosis and adequate treatment. The main physical and psycho-socio-economic determinants of depression in our MS cohort are the physical disability, disease duration, number of relapses, marital status, education level, employment status and the presence of children, but many unsolved questions remain about the interrelation and the relative contribution of these factors, and that need further research. We found the DMTs did not significantly influence the depression level.
References
Chwastiak L, Ehde DM, Gibbons LE, Sullivan M, Bowen JD, Kraft GH (2002) Depressive symptoms and severity of illness in multiple sclerosis: epidemiologic study of a large community sample. Am J Psychiatry 159(11):1862–1868
Anhoque CF, Domingues SC, Carvalho T, Teixeira AL, Domingues RB (2011) Anxiety and depressive symptoms in clinically isolated syndrome and multiple sclerosis. Arq Neuropsiquiatr 69(6):882–886
Siegert RJ, Abernethy DA (2005) Depression in multiple sclerosis: a review. J Neurol Neurosurg Psychiatry 76(4):469–475
Charcot JM (1879) Lectures on the disease of the nervous system. Henry C Lea, Philadelphia
Minden SL, Feinstein A, Kalb RC, Miller D, Mohr DC, Patten SB, Bever C Jr, Schiffer RB, Gronseth GS, Narayanaswami P (2014) Guideline Development Subcommittee of the American Academy of NeurologyEvidence-based guideline: assessment and management of psychiatric disorders in individuals with MS: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 82(2):174–181. doi:10.1212/WNL.0000000000000013
Schiffer RB, Babigian HM (1984) Behavioral disorders in multiple sclerosis, temporal lobe epilepsy, and amyotrophic lateral sclerosis. An epidemiologic study. Arch Neurol 41(10):1067–1069
Fernández-Jiménez E, Pérez-San-Gregorio MA, Martín-Rodríguez A, Pérez-Bernal J, Gómez-Bravo MA (2015) Comparison of the affective symptomatology between liver transplant recipients and patients with multiple sclerosis considering their functional impairment. Transplant Proc 47(1):104–106. doi:10.1016/j.transproceed.2014.11.015
Fernández-Jiménez E, Arnett PA (2014) Impact of neurological impairment, depression, cognitive function and coping on quality of life of people with multiple sclerosis: a relative importance analysis. Mult Scler. doi:10.1177/1352458514562439
Siracusano A, Niolu C, Sachetti L, Ribolsi M (2012) Depression and anxiety. In: Nocentini U, Caltagirone C, Tedeschi G (eds) Neuropsychiatric dysfunction in multiple sclerosis. Springer, Berlin
Feinstein A (2011) Multiple sclerosis and depression. Mult Scler J 17(11):1276–1281. doi:10.1177/1352458511417835
Sadovnick AD, Remick RA, Allen J, Swartz E, Yee IM, Eisen K, Farquhar R, Hashimoto SA, Hooge J, Kastrukoff LF, Morrison W, Nelson J, Oger J, Paty DW (1996) Depression and multiple sclerosis. Neurology 46(3):628–632
Kingwell E, Marriott JJ, Jetté N, Pringsheim T, Makhani N, Morrow SA, Fisk JD, Evans C, Béland SG, Kulaga S, Dykeman J, Wolfson C, Koch MW, Marrie RA (2013) Incidence and prevalence of multiple sclerosis in Europe: a systematic review. BMC Neurol 26(13):128. doi:10.1186/1471-2377-13-128
Polman CH, Reingold S, Banwell B et al (2011) Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol 69:292–302
Kurtzke JF (1983) Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 33(11):1444–1452
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:561–571
Patten SB, Beck CA, Williams JV, Barbui C, Metz LM (2003) Major depression in multiple sclerosis: a population-based perspective. Neurology. 61(11):1524–1527
Minden SL, Orav J, Reich P (1987) Depression in multiple sclerosis. Gen Hosp Psychiatry 9(6):426–434
Rabkin JG, Albert SM, Del Bene ML, O’Sullivan I, Tider T, Rowland LP, Mitsumoto H (2005) Prevalence of depressive disorders and change over time in late-stage ALS. Neurology 65(1):62–67
Miletic S, Toncev G, Jevdjic J et al (2011) Fatigue and depression in multiple sclerosis: correlation with quality of life. Arch Biol Sci Belgrade 63(3):617–622
Smith MM, Arnett PA (2013) Perfectionism and physical disability predict depression in multiple sclerosis. J Psychosom Res 75(2):187–189. doi:10.1016/j.jpsychores.2013.06.001 Epub 2013 Jun 28
Williams RM, Turner AP, Hatzakis M Jr, Bowen JD, Rodriquez AA, Haselkorn JK (2005) Prevalence and correlates of depression among veterans with multiple sclerosis. Neurology 64(1):75–80
Zephir H, De Seze J, Stojkovic T, Delisse B, Ferriby D, Cabaret M, Vermersch P (2003) Multiple sclerosis and depression: influence of interferon beta therapy. Mult Scler J 9(3):284–288
Bakshi R, Czarnecki D, Shaikh ZA, Priore RL, Janardhan V, Kaliszky Z, Kinkel PR (2000) Brain MRI lesions and atrophy are related to depression in multiple sclerosis. NeuroReport 11(6):1153–1158
Kessler RC, McGonagle KA, Nelson CB, Hughes M, Swartz M, Blazer DG (1994) Sex and depression in the National Comorbidity Survey. II: cohort effects. J Affect Disord 30(1):15–26
Patten SB, Metz LM, Reimer MA (2000) Biopsychosocial correlates of lifetime major depression in a multiple sclerosis population. Mult Scler J 6(2):115–120
Galeazzi GM, Ferrari S, Giaroli G, Mackinnon A, Merelli E, Motti L, Rigatelli M (2005) Psychiatric disorders and depression in multiple sclerosis outpatients: impact of disability and interferon beta therapy. Neurol Sci 26(4):255–262
Korostil M, Feinstein A (2007) Anxiety disorders and their clinical correlates in multiple sclerosis patients. Mult Scler J 13(1):67–72
Beal CC, Stuifbergen A (2007) Loneliness in women with multiple sclerosis. Rehabil Nurs 32(4):165–171
Beiske AG, Svensson E, Sandanger I, Czujko B, Pedersen ED, Aarseth JH, Myhr KM (2008) Depression and anxiety amongst multiple sclerosis patients. Eur J Neurol 15(3):239–245. doi:10.1111/j.1468-1331.2007.02041.x Epub 2008 Jan 22
Bamer AM, Cetin K, Johnson KL, Gibbons LE, Ehde DM (2008) Validation study of prevalence and correlates of depressive symptomatology in multiple sclerosis. Gen Hosp Psychiatry 30(4):311–317. doi:10.1016/j.genhosppsych.2008.04.006
Aşiret GD, Özdemir L, Maraşlıoğlu N (2014) Hopelessness, depression and life satisfaction among the patients with multiple sclerosis. TJN 20(1):1–6. doi:10.4274/Tnd.24471
Möller A, Wiedemann G, Rohde U, Backmund H, Sonntag A (1994) Correlates of cognitive impairment and depressive mood disorder in multiple sclerosis. Acta Psychiatr Scand 89(2):117–121
Moore P, Hirst C, Harding KE, Clarkson H, Pickersgill TP, Robertson NP (2012) Multiple sclerosis relapses and depression. J Psychosom Res 73(4):272–276. doi:10.1016/j.jpsychores.2012.08.004
Patten SB, Metz LM (2001) Interferon beta-1 a and depression in relapsing-remitting multiple sclerosis: an analysis of depression data from the PRISMS clinical trial. Mult Scler J 7(4):243–248
Patten SB, Metz LM, SPECTRIMS Study Group (2002) Interferon beta1a and depression in secondary progressive MS: data from the SPECTRIMS Trial. Neurology 59(5):744–746
Acknowledgments
This study was supported by the internal research Grant of The University of Medicine and Pharmacy Targu Mures, Grant Number 18/2015.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
This study was approved by the local ethical committee.
Informed consent
All the patients signed informed consent to participate in the study.
Rights and permissions
About this article

Cite this article
Maier, S., Buruian, M., Maier, A. et al. The determinants of depression in a Romanian cohort of multiple sclerosis patients. Acta Neurol Belg 116, 135–143 (2016). https://doi.org/10.1007/s13760-015-0547-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13760-015-0547-4