
Abstract
The aim of this study was to elucidate the effects of an ischemic stroke on the amplitude and latency of the P300 wave and evaluate their changes over a prospective 1-year follow-up period. We recorded the P300 wave using an auditory oddball paradigm in 60 consecutive brain infarct patients at baseline (i.e., within 4 weeks after the stroke), after 3 months, after 12 months and in 30 healthy control subjects. The P300 latencies in stroke patients were significantly longer and the P300 amplitudes were significantly smaller than those of the control group. The latency of P300 showed a highly significant average improvement 12 months after the stroke compared to the baseline. There was no significant change observed for the P300 amplitude during the same period. The P3 latency is initially more increased in the patients with hemispheric brain infarction but shows a better recovery compared to the patients with brainstem infarction. Also, the results of the P300 latency of patients with the left-sided lesions was significantly longer compared to the patients with right-sided lesions on the beginning of the study but not 3 and 12 months after the stroke. The results of our study show the importance of P300 event-related potentials in the detection and follow-up of cognitive changes after ischemic stroke.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Stroke is often associated with cognitive decline which may hinder functional recovery and rehabilitation [1, 2]. Assessment of cognitive status after ischemic stroke represents a possibility for early diagnostics of vascular cognitive impairment and timely introduction of necessary pharmacotherapy treatment and neuropsychological rehabilitation. In clinical practice, cognitive deficits after ischemic stroke usually are monitored and evaluated by neuropsychological tests. However, neuropsychological testing depends on the cooperation of the patient and is often complex and time-consuming. For these reasons, researchers’ attention has been attracted by an objective neurophysiological method—event-related potentials (ERP) which can help in the evaluation of cognitive impairment.
The numerous clinical P300 studies [3–9] strongly suggest that this ERP component may be clinically useful as an index of cognitive function. ERP are reproducible electrophysiological responses to an external stimulus, representing a brain activity associated with various cognitive processes such as selective attention, memory, or decision making [10–12]. The P300 (also known as P3 or P3b) is the late positive wave that occurs with a modal latency of about 300 ms in normal young adults, with larger amplitude over the central-parietal scalp regions [13–15]. It is generated when a subject discriminates between stimulus events which are different from one another along some dimension such as intensity, duration or modality [16, 17]. A rare event that is not task-relevant can produce a positive-going waveform that has been labeled “P3a”. This component distinguished from P300 of a relatively short peak latency of 250–300 ms and a scalp distribution with a midline fronto-central maximum. The relation between P3a and P300 is still a focus of theoretical debate [14].
A prolongation of the P3 latency and reduction of the P300 amplitude indicates a cognitive slowing and could be shown in various diseases and injuries of the brain, including dementia regardless of the etiology [18–22], schizophrenia [23, 24], depression [25, 26], Parkinson’s disease [27, 28], and multiple sclerosis [29–32]. However, the results of a few previous ERP studies performed in patients with ischemic stroke have shown controversial results. Some study reports have shown a prolongation of the P3 latency in the unilateral thalamic infarction [33], thalamic hemorrhages [34], brainstem and hemispheric infarction [35], as well as in the multiple lacunar brain infarction [36]. Some of these studies have shown a delay of the P300 wave without reduction of its amplitude or change in its scalp distribution. On the other hand, there are studies that did not find significant differences of P300 latency in stroke patients but show a decrease of the P300 amplitude [37]. Onofrj et al. [38] demonstrated normal latency, amplitude, and topographic distribution of the P300 in four patients affected by basilar artery thromboembolism which had resulted in the locked-in syndrome
However, these studies did not evaluate, in a prospective study, a recovery of the cognitive impairment caused by stroke and which factors might have an influence on the recovery process. A usefulness of the P300 as a cognitive impairment marker after the ischemic stroke has not been clarified yet. To the best of our knowledge, there is no prospective study that has followed the recovery of latency and amplitude of P300 after ischemic stroke at three time points during the study (baseline, after a 3 and 12 months’ period).
The purpose of this study was to investigate the effects of a stroke on the amplitude and latency of the P300 wave and evaluate their changes over a prospective 1-year follow-up period. Also, we wanted to determine whether certain factors such as localization of the brain lesion or vascular risk factors impact the recovery of the latency and amplitude of the P300 for a period of 1 year after the stroke. The study included 60 patients with clinically first ischemic stroke and 30 healthy age- and sex-matched control subjects. We recorded the P300 to target stimuli using a classic auditory oddball paradigm.
Materials and methods
The study included 60 patients (27 men and 33 women, mean age 57.1 ± 7.2 years, range 45–72 years) with acute first-ever brain infarction. Cerebral CT or MRI scan was performed on all patients. Appropriate patients were recruited from the Department for neurological disease at the Rehabilitation centre Novi Sad Serbia. Patients with history of any other neurologic disease, history of traumatic brain injury, aphasia, defects in hearing, communication disorders, previous depression or other psychiatric illnesses as well as alcoholism and/or administration of medications known to influence cognitive functions were excluded. The control group consisted of 30 age- and sex-matched healthy volunteers (12 men and 18 women, mean age 56.2 ± 6.3 years, range 42–72 years). Clinical and demographic features of the patient and control groups are shown in Table 1.
All the patients with first ever stroke without any other cerebral diseases were enrolled consecutively. The patients were neurological and laboratory examined in the acute phase and at 3 and 12 months after the stroke. The mean interval between the stroke onset and the first P300 recording was 10.9 days (SD 4.4). Neurological deficits of the patients were scored with the NIHSS Scale (National Institute of Health Stroke Scale). Independence in their activities of daily living was scored with the Barthel Index. A psychiatric examination was performed on all the patients at baseline, at the 3- and 12-month follow-up visits, and patients’ depression was diagnosed according to the criteria of DSM-IV. Severity of depression was measured by means of the Hamilton Depression Rating Scale (HDRS).
After the 3-month examination two patients died and one patient refused the follow-up. The protocol of the study was approved by the local Ethics Committee, in accordance with the principles of the Declaration of Helsinki. An informed consent was obtained from all patients, before they were enrolled into the study.
ERP measurement
P300 ERPs were recorded using the classic auditory oddball paradigm (Polich, 2000) with 20 % of target and 80 % of non-target stimuli. Tones with the frequency of 2,000 and 1,000 Hz and strength of 90 dB were used as a target and non-target stimuli. Tones were presented to the subject trough binaural phones. The subjects were instructed to react as fast as possible to the target tones (2,000 Hz) by pressing the button on the special handle they were holding in their preferred hand and at the same time to ignore rhythmical non-target tones (1,000 Hz). The subjects were sitting on the chair in the comfortable position in the silent darkened room with their eyes open.
Bioelectrical activity of the brain was recorded using Ag/AgCl electrodes fastened on the scalp of the subject with the colodium. Three active electrodes were positioned at the central line of the scalp frontally (Fz), centrally (Cz), and parietally (Pz) according to the international 10–20 system. Reference electrodes were placed at the mastoids while the ground electrode was positioned at the subject forearm. Impedance of all electrodes in all recordings was under 5 kΩ. During one recording session 200 tones were presented in variable intervals, with 1 s as a minimum, averaging at 2 s to prevent habituation. Tone order is determined by a random number generator individually for each recording. The probability of target tone appearance was 0.15. A 1,000 ms of the cortical electrical activity was recorded after each stimulus appearance. The signal was averaged during the recording. The cortical activity signal averaging was done separately for target and non-target stimuli. At the end of the recordings P300 latency was identified as the largest positive peak at range 250–450 ms occurring after the N1, P2, and N2 ERP components obtained from the “target” stimulus presentation. In cases of bifurcated peaks, the second peak with a central/parietal maximum was selected for P300 latency and amplitude determination [39].
The peak amplitudes (μV) were evaluated as the differences between P300 peak and the mean baseline automatically calculated by a computer.
Statistical analysis
The statistical analyses were carried out using the Wilcoxon rank-sum test (Mann–Whitney) to compare the P300 amplitudes and latencies of the patients with those of the control subjects. The ERP components measured in the different subgroups at the first, second, and third visit were compared by Wilcoxon signed-rank test. Pearson’s correlation coefficients were used to correlate the amplitudes and latencies of the P300 with the scores of the different scales. Point-biserial correlation is used to determine the influence of various risk factors to the values of P300 component. In the interpretation of data, probability values of p < 0.05 (two tailed) were considered statistically significant. The statistical analysis was performed, using R version 3.1.0 [40].
Results
Table 2 presents the P300 latencies and amplitudes of the control group and of all patients at the beginning of the study (baseline) and at the follow-up examinations after 3 months, and after 12 months.
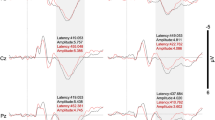
The P300 latencies of the stroke patients were significantly longer than those of the control subjects at the beginning at all recording sites, Fz, Cz, and Pz (p < 0.01). The P300 amplitudes were significantly slightly smaller than those of the control subjects, the difference being statistically signifcant at (Fz p = 0.032, Cz p = 0.021, and Pz p = 0.030).
In addition, we compared the latencies and amplitudes of P300 measured 3 and 12 months after stroke with the value at the baseline. The P300 latency continuously decreased over the observation period, with a significant difference after 3 months at (Fz p = 0.024, Cz p = 0.048, Pz p = 0.04), and after 12 months (p < 0.01) compared to baseline. On the other hand, the amplitude P3 showed no significant changes over time.
Impact of lesion location
Table 3 presents the data for the inter-group comparison of P300 latencies and amplitudes between patients with a hemispheric brain infarction and patients with a brainstem infarction. Comparing the P300 latencies in baseline patients with a hemispheric brain infarction showed a significantly longer P300 latency than those in patients with a brainstem infarction (p < 0.01). The recovery of the patients with a hemispheric brain infarction was faster so that after 3 and 12 months no significant difference between the groups could be proved. There were no significant differences between these two groups with respect to P300 amplitude during the study period.
We conducted the inter-group comparison of P300 latencies and amplitudes between the patients with left- and right-sided lesions and found a significantly longer P3 latencies at the baseline in the left-side lesions patients (Fz p = 0.047, Cz p = 0.032). Only patients with one infarction in either hemisphere were included into the analysis. There was no significant difference between these groups after 3 and 12 months. There were no significant differences between these two groups with respect to P300 amplitude during the study period.
No significant correlations were found between the P300 values and the scores of the NIHS and the Barthel Index. In the normals the latency of the P300 correlated significantly with the reaction time at Pz site (r = 0.54, p < 0.01). In the patients significant correlations were found between the P300 latencies and reaction time 12 months after the stroke (Pz r = 0.33, p < 0.05). A significant correlation between the P300 latencies and reaction time was found for group with left hemispheric stroke at 12 months (Pz, r = 0.35, p < 0.05). In the patients with right hemispheric stroke a significant correlations were found between the P300 latencies and reaction time at 3 months (Pz r = 0.42, p < 0.05) and 12 months (Pz r = 0.41, p < 0.05) after the stroke. We also calculated the coefficient of variation of reaction time from 60 reaction time data obtained at each test time. Correlation between P300 latency and the coefficient of variation of reaction time was significant for left hemispheric stroke patients at 12 months (r = 0.39, p < 0.05) while for the right hemispheric stroke patients we have found significant correlation at 3 months (r = 0.51, p < 0.05) and 12 months (r = 0.49, p < 0.05). The P300 amplitude and reaction time were significantly negatively correlated at baseline (Pz r = −0.48, p < 0.01), 3 months (Pz r = −0.31, p < 0.05), and 12 months (Pz r = −0.29, p < 0.05) after the stroke.
The P300 latencies correlated significantly with the scores of the Hamilton Depression Rating Scale at the 12-month (Pz, r = 0.27, p < 0.05) follow-up visits. No significant correlation was found between the P300 amplitude and the scores of the Hamilton Depression Rating Scale. From all analyzed risk factors (hypertension, obesitas, diabetes, hipelilidemia, nicotine) we have found a significant correlation between the values of P300 latency and the hypertension at baseline (Fz r pb = 0.44, p < 0.01, Pz r pb = 0.64, p < 0.01).
Discussion
Cognitive decline is a frequent sequelae of ischemic brain infarction that most frequently manifests as deficits in attention, memory, information processing speed, language, conceptual thinking, in particular episodic and working memory and executive functions [41, 42]. The presence of cognitive impairment in patients with stroke has important functional consequences, independent of the effects of physical impairment [41, 43].
We have used P3 component for the purpose of cognitive deficit evaluation after ischemic stroke, because its latency is considered to reflect the basic time of central information processing. The aim of this prospective study was to elucidate the effects of ischemic stroke on the P300 latencies and amplitudes, as well as their potential changing over the time of follow-up.
In comparison with the previous studies of ERP at brain infarction [33, 35, 36], we prospectively assessed P300 latencies and amplitudes over a period of 12 months after the stroke and evaluated which factors might have an influence on these changes. The results of our study suggest that brain infarction increases the latency of the P300 ERP and decreases the amplitude of P3.
During the study period a significant average improvement of P3 latency after 12 months compared to the baseline has been observed. These findings suggest that the endogenous cognitive processing such as decision making and secondary stimulus evaluation improves after the stroke. This implies that P300 latency may be used as a marker of cognitive recovery after the stroke. On the other hand, we have not observed a significant change of P300 amplitude during the study period.
The results of several studies on the subject of the influence of ischemic stroke on P300 component are controversial. Gummow [37] has found that P300 amplitudes decrease in patients with brain infarction located in the middle cerebral artery territory, without increase of latencies.
In several studies [35, 36] authors suggest that brain infarction increases latency without influence on the amplitude while other studies [44] claim that the increase in latency is evident only in the patients with dementia. We assume that these differences might occur due to the different time points of P300 measurements after the stroke. Furthermore, the differences could also occur due to different experimental methodologies (e.g. auditory or visual stimulation, target stimuli counting or pressing the button). The assessment of a cognitive status in the acute phase is of a great importance having in mind that the P300 latency shows a capacity for recovery.
The results show that lesion localization has an impact on the values of P300 latency. Our comparison of patients with a hemispheric brain infarction and patients with a brainstem infarction revealed a significant prolongation of P300 latency in patients with a hemispheric brain infarction at baseline in the weeks after the stroke. Over the time, both groups showed a continuous improvement of P3 latency. However, patients with a hemispheric brain infarction had a faster P300 latency recovery and thus after 12 months the difference between these two groups could not be proved.
Some authors [45, 46] find that the longer P300 latencies in patients with cortical compared to patients with subcortical dementia may be caused by the cortical localization of the greater number of P300 potential generators and the impairment in structures of the declarative memory.
At the beginning of the study, we have observed significantly longer P300 latencies in patients with the lesions in the left hemisphere compared to the patients with the right localized lesions. Therefore, we conclude that stroke might cause a higher cognitive impairment in patients with left-sided lesions than in patients with right-sided lesions.
However, some patients with left hemispheric infarction show a better cognitive recovery from stroke than patients with right hemispheric infarction. Therefore, a significant difference between groups at 12 months has not been observed. There are a lot of controversial reports concerning the question how the lesion side affects P300 components. Korpelainen [35] did not find significant difference of P300 components among left- and right-side lesions. Some authors evaluated that left hemispheric infarction shows a better recovery from stroke with respect to several neuropsychological functions except aphasia [47–50].
The results also demonstrate a significant correlation between the P300 latency and the severity of post-stroke depression. The correlation between vascular risk factors and cognitive impairment has shown that hypertension has negative effect on the cognitive recovery. The explanation for this correlation is a significant direct impact of the hypertension on tiny blood vessels of the brain. Hypertension could lead to an ischemic subcortical structures damaging, where the subcortical ischemic disease particularly has an effect on the frontal-subcortical circuitry responsible for the cognitive and affective status regulation [51].
Conclusion
Results of our study show the importance of P300 ERP in the evaluation of patients with ischemic stroke, because of its sensitivity in the detection of subtle cognitive disturbances. The P3 latency stands out as a marker for cognitive function recovery after the stroke.
References
Dombovy ML, Sandok BA, Basford JA (1986) Rehabilitation after stroke: a review. Stroke 17:363–369
Zinn S, Dudley TK, Bosworth HB, Hoenig HM, Duncan PW, Horner RD (2004) The effect of poststroke cognitive impairment on rehabilitation process and functional outcome. Arch Phys Med Rehabil 85:1084–1090
Yamaguchi S, Knight RT (1991) P300 generation by novel somatosensory stimuli. Electroencephalogr Clin Neurophysiol 78:50–55
Bennys K, Portet F, Touchon J, Rondouin G (2007) Diagnostic value of event-related evoked potentials N200 and P300 subcomponents in early diagnosis of Alzheimer’s disease and mild cognitive impairment. J Clin Neurophysiol 24:405–412
Golob EJ, Irimajiri R, Starr A (2007) Auditory cortical activity in amnestic mild cognitive impairment: relationship to subtype and conversion to dementia. Brain 130:740–752
Frodl T, Hampel H, Juckel G, Bürger K, Padberg F, Engel RR, Möller HJ, Hegerl U (2002) Value of event-related P300 subcomponents in the clinical diagnosis of mild cognitive impairment and Alzheimer’s disease. Psychophysiology 39(2):175–181
Golob EJ, Johnson JK, Starr A (2002) Auditory event-related potentials during target detection are abnormal in mild cognitive impairment. Clin Neurophysiol 113:151–161
Irimajiri R, Golob EJ, Starr A (2005) Auditory brain-stem, middle- and long-latency evoked potentials in mild cognitive impairment. Clin Neurophysiol 116:1918–1929
Polich J (1999) P300 in clinical applications. In: Niedermayer E, de la Silva L, Urban F (eds) Electroencephalography: basic principles, clinical applications and related fields. Schwartzenberger, Baltimore-Munich, pp 1073–1091
Friedman D, Johnson R (2000) Event-related potential (ERP) studies of memory encoding and retrieval: a selective review. Microsc Res Tech 51:6–28
Braverman ER, Blum K (2003) P300 (latency) event-related potential: an accurate predictor of memory impairment. Clin Electroencephalogr 34:124–139
Patel SH, Azzam PN (2005) Characterization of N200 and P300: selected studies of the event-related potential. Int J Med Sci 2:147–154
Polich J, Herbst KL (2000) P300 as a clinical assay: rationale, evaluation, and findings. Int J Psychophysiol 38:3–19
Polich J (2007) Updating P300: an integrative theory of P3a and P3b. Clin Neurophysiol 118(10):2128–2148
Portin R, Kovala T, Polo-Kantola P, Revonsuo A, Muller K, Matikainen E (2000) Does P3 reflect attentional or memory performances, or cognition more generally? Scand J Psychol 41:31–40
Picton TW (1992) The P300 wave of the human event-related potential. J Clin Neurophysiol 9(4):456–479
Polich J (1998) P300 clinical utility and control of variability. J Clin Neurophysiol 15:14–33
Goodin D, Squires K, Starr A (1978) Long latency event-related components of the auditory evoked potential in dementia. Brain 101:635–648
Goodin D, Aminoff M (1986) Electrophysiological differences between subtypes of dementia. Brain 109:1103–1113
Goodin D, Aminoff M (1987) Electrophysiological differences between demented and nondemented patients with Parkinson’s disease. Ann Neurol 21:90–94
Neshige R, Barrett G, Shibasaki H (1988) Auditory long latency event-related potentials in Alzheimer’s disease and multi-infarct dementia. J Neurol Neurosurg Psychiatry 51:1120–1125
Ito J (1994) Somatosensory event-related potentials (ERPs) in patients with different types of dementia. J Neurol Sci 121:139–146
Blackwood DH, St Clair DM, Muir WJ, Duffy JC (1991) Auditory P300 and eye tracking dysfunction in schizophrenic pedigrees. Arch Gen Psychiatry 48:899–909
Weir N, Fiaschi K, Machin D (1998) The distribution and latency of the auditory P300 in schizophrenia and depression. Schizophr Res 31:151–158
Karaaslan F, Gonul AS, Oguz A, Erdinc E, Esel E (2003) P300 changes in major depressive disorders with and without psychotic features. J Affect Disord 73:283–287
Vandoolaeghe E, van Hunsel F, Nuyten D, Maes M (1998) Auditory event-related potentialsin major depression: prolonged P300 latency and increased P200 amplitude. J Affect Disord 48:105–113
Hansch EC, Syndulko K, Cohen SN, Goldberg ZI, Potvin AR, Tourtellotte WW (1982) Cognition in Parkinson disease: an event-related potential perspective. Ann Neurol 11:599–607
Tachibana H, Toda K, Sugita M (1992) Actively and passively evoked P3 latency of event-related potentials in Parkinson’s disease. J Neurol Sci 111(2):134–142
Polich J, Romine JS, Sipe JC, Aung M, Dalessio DJ (1992) P300 in multiple sclerosis: a preliminary report. Int J Psychophysiol 12:155–163
Honig LS, Ramsay RE, Sheremata WA (1992) Event-related potential P300 in multiple sclerosis. Relation to magnetic resonance imaging and cognitive impairment. Arch Neurol 49:44–50
Ellger T, Bethke F, Frese A, Lüttmann RJ, Buchheister A, Ringelstein EB, Evers S (2002) Event related potentials in different subtypes of multiple sclerosis—a cross-sectional study. J Neurol Sci 205:35–40
Piras MR, Magnano I, Canu EDG, Paulus KS, Satta WM, Soddu A, Conti M, Achene A, Solinas G, Aiello I (2003) Longitudinal study of cognitive dysfunction in multiple sclerosis: neuropsychological, neuroradiological, and neurophysiological findings. J Neurol Neurosurg Psychiatry 74:878–885
Trinka E, Unterrainer J, Staffen W, Löscher NW, Ladurner G (2000) Delayed visual P3 in unilateral thalamic stroke. Eur J Neurol 7:517–522
Onofrj M, Curatola L, Malatesta G, Colamartino P, Bazzano S, Fulgente T, Ferracci F (1992) Delayed P3 event-related potentials (ERPs) in thalamic hemorrhage. Electroencephalogr Clin Neurophysiol 83:52–61
Korpelainen JT, Kauhanen ML, Tolonen U, Brusin E, Mononen H, Hiltunen P, Sotaniemi KA, Suominen K, MyllylaÈ VV (2000) Auditory P300 event related potential in minor ischemic stroke. Acta Neurol Scand 101:202–208
Tachibana H, Toda K, Sugita M (1992) Event-related potentials in patients with multiple lacunar infarcts. Gerontology 38:322–329
Gummow LJ, Dustman RE, Keaney RP (1986) Cerebrovascular accident alters P300 event-related potential characteristics. Electroencephalogr Clin Neurophysiol 63:128–137
Onofrj M, Thomas A, Paci C, Scesi M, Tombari R (1997) Event related potentials recorded in patients with locked-in syndrome. J Neurol Neurosurg Psychiatry 63:759–764
Goodin D, Desmedt J, Maurer K, Nuwer MR (1994) IFCN recommended standards for longlatency auditory event-related potentials. Report of an IFCN committee. International Federation of Clinical Neurophysiology. Electroencephalogr Clin Neurophysiol 91(1):18–20
R Core Team (2014) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Version 3.1.0. http://www.R-project.org/. Accessed 4 oct 2014
Tatemichi TK, Desmond DW, Stern Y, Paik M, Bagiella E (1994) Cognitive impairment after stroke: frequency, patterns, and relationship to functional abilities. J Neurol Neurosurg Psychiatry 57:202–207
Ballard C, Rowan E, Stephens S, Kalaria R, Kenny RA (2003) Prospective follow-up study between 3 and 15 months after stroke: improvements and decline in cognitive function among dementia-free stroke survivors >75 years of age. Stroke 34(10):2440–2444
Oksala NK, Jokinen H, Melkas S, Oksala A, Pohjasvaara T, Hietanen M, Vataja R, Kaste M, Karhunen PJ, Erkinjuntti T (2009) Cognitive impairment predicts poststroke death in long-term follow-up. J Neurol Neurosurg Psychiatry 80(11):1230–1235
Ladurner G, Schimke H, Wranek U, Klimesch W (1992) The value of P300 in the diagnosis of cognitive impairment in stroke. Arch Gerontol Geriatr 10(1):1–8
Iragui V, Kutas M, Salmon DP (1996) Event related potentials during semantic categorization in normal aging and senile dementia of the Alzheimer’s type. Electroencephalogr Clin Neurophysiol 100(5):392–406
Yamaguchi S, Tsuchiya H, Yamagata S, Toyoda G, Kobayashi S (2000) Event-related brain potentials in response to novel sounds in dementia. Clin Neurophysiol 111(2):195–203
Sunderland A, Tinson D, Bradley L (1994) Differences in recovery fromconstructional apraxia after right and left hemisphere stroke? Clin Exp Neuropsychol 16:916–920
Robertson IH, Ridgeway V, Greenfield E, Parr A (1997) Motor recovery after stroke depends on intact sustained attention: a 2-year follow-up study. Neuropsychology 11:290–295
Desmond DW, Moroney JT, Sano M, Stern Y (1996) Recovery of cognitive function after stroke. Stroke 27:1798–1803
Siekierka-Kleiser EM, Kleiser R, Wohlschläger AM, Freund HJ, Seitz RJ (2006) Quantitative assessment of recovery from motor hemineglect in acute stroke patients. Cerebrovasc Dis 21:307–314
O’Brien JT, Erkinjuntti T, Reisberg B, Roman G, Sawada T, Pantoni L, Bowler JV, Ballard C, DeCarli C, Gorelick PB, Rockwood K, Burns A, Gauthier S, DeKosky ST (2003) Vascular cognitive impairment. Lancet Neurol 2(2):89–98
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dejanović, M., Ivetić, V., Nestorović, V. et al. The role of P300 event-related potentials in the cognitive recovery after the stroke. Acta Neurol Belg 115, 589–595 (2015). https://doi.org/10.1007/s13760-015-0428-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13760-015-0428-x