
Abstract
Purpose of Review
This review aims to describe the treatment and outcomes in the perioperative management of elderly patients undergoing hepatic surgery for cancer.
Recent Findings
There is a broad perception that elderly patients are more frail and less able to tolerate major resection. They are therefore offered surgery less often than younger patients. Elderly patients can tolerate major hepatectomies with comparable length of surgery, rate of transfusion, and length of hospital stay as younger patients. However, they are more apt to develop significant cardiopulmonary complications and require discharge to an acute care facility. When matched for tumor stage, disease-specific survival is similar to younger patients.
Summary
Contrary to what is sometimes perceived, elderly patients can tolerate major hepatic resection. However, this requires careful patient selection and preoperative evaluation, as elderly patients are more prone to complications, concerns related to quality of life outcomes and perioperative mortality.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatobiliary malignancies are disproportionately represented in an older population. Despite this relative prevalence, older patients have historically been perceived to be less able to tolerate aggressive oncologic therapy, including systemic chemotherapy and hepatic resections. Elderly patients more commonly have decreased liver volume, decreased hepatic perfusion, reduced hepatocyte function, and subsequently increased vulnerability for postoperative hepatic failure. Further, this patient population is prone to having multiple significant medical comorbidities, increased frailty, and poorer nutrition, all qualities which are typically attributed to poor surgical outcomes. These factors contribute to the impression that elderly patients have decreased tolerance for operative intervention and major hepatectomy. As a result, there have been multiple studies that report on decreased rates of chemotherapy and surgical interventions being utilized in this patient population.
In the last several years, however, hepatobiliary surgery has made multiple advances towards less invasive interventions and more efficacious percutaneous ablative therapies. Systemic chemotherapy has made several advances towards greater efficacy. Critical care has also significantly improved for assistance in managing the postoperative complications that may arise after resection. Consequently, there are more treatment options that are available to a broader patient population than what was previously offered.
The purpose of this review is to assess the current literature for hepatobiliary oncologic surgical treatment in the elderly. We will discuss recent data with respect to preoperative medical evaluation, immediate postoperative complications and long-term outcomes.
Current Trends in Practice
While reviewing the literature, it is important to note that when comparing younger versus older patients, there are a number of confounding variables which have potential to cloud a direct, head-to-head comparison between both cohorts. First, a consistent definition of which age threshold identifies an elderly patient is not available. The majority of published literature refer to ages 70–75 years old as a threshold defining elderly versus younger patient populations; however, there are some studies which refer to ages as young as 65 years or as old as 85 years when defining the age group of interest. Moreover, while age 75 and older are typically referred to as the elderly patient population, patients greater than 75 are heterogeneous in the number and severity of comorbidities, their physiologic reserve, and performance status. Indeed, with increasing age from 75 years to 95 years, patients are more apt to have greater severity disease, more numerous comorbidities, and poorer underlying reserve making appropriate patient selection increasingly important. Moreover, with increasing age, the gain in years of any successful treatment also decreases which has to be factored into any risk-benefit calculation. Finally, the underlying hepatic reserve and tumor biology may be different in older from that of younger patients. Younger patients may be more apt to have non-alcoholic fatty liver disease, alcoholic cirrhosis, and chronic hepatitis B and have more aggressive histologies. These differing characteristics complicate the comparison between younger and older patients and their ability to tolerate surgical interventions.
Current attitudes towards elderly patients were assessed in a web-based survey of the Society of Surgical Oncology and the European Society of Surgical Oncology in 2016. Ghignone et al. reported that, of those surveyed, there was a strong consensus that elderly patients were associated with increased morbidity, mortality, postoperative complication, and greater likelihood of prolonged hospital stay [1]. There is also evidence to suggest that elderly patients do not receive the same degree of aggressive treatment as younger patients. In a retrospective review, Benedetto et al. describe that the majority of those patients diagnosed with colorectal metastases to the liver are elderly, but that curative surgery is offered less frequently to these patients in the context of synchronous hepatic metastases. These patients are also less likely to be offered systemic chemotherapy. The study authors attribute this difference to concerns regarding the elderly patient’s concomitant medical comorbidities, greater likelihood of poorer cardiopulmonary reserve, and malnutrition. Further, aging-related changes to the liver including smaller volume, reduction in hepatocyte function, and decreased ability to regenerate give greater concern for the patient’s ability to tolerate a major hepatectomy [2]. However survey results may also reveal an undeserved perceived bias by the surgeon.
The observation that elderly patients are not offered surgical resection as often as younger patients is disputed in several other retrospective studies. For example, in a single-center review of practice patterns, Horgan et al. retrospectively reviewed the care delivered to 913 patients treated from 1987 to 2013 for biliary tract cancer at a tertiary referral center in Canada. Of these patients, they found no difference in the rate of undergoing surgical resection between young and elderly (greater than 70 years of age) patients, nor offering of adjuvant chemotherapy. However, they did find a significant difference in the rate at which second-line chemotherapy was offered to patients [3]. In another retrospective cohort study examining 531 patients diagnosed with biliary tract cancer, Lee et al. determined that older patients had a greater frequency of poorer performance status, lower serum albumin, and greater number and severity in comorbidities. Tumor stage, location, and histology were similar to those identified in younger patient cohorts. On multivariate analysis, higher severity of comorbidity was associated with mortality, though age was not. Study authors noted that elderly patients appeared to be treated at a similar frequency to that of younger patients but as this was a referral center, some self-selection of patients treated there would appear likely. However, patients did undergo less adjuvant chemotherapy and radiation. The etiology for this difference in care was unclear, although study authors hypothesize that this difference may be attributable to the patients’ poorer clinical condition or refusal to endure further treatment [4].
While curative resection may be offered at a similar rate, adjuvant chemotherapy and subsequent resection for recurrent or metastatic disease may not be utilized in elderly patients at the same frequency as younger patients. In a multi-institutional analysis published in 2011, a retrospective review examined the characteristics of 856 patients who underwent hepatic resection from 2002 to 2009 between three major tertiary care referral centers. Indications included metastatic colorectal cancer, hepatocellular carcinoma, cholangiocarcinoma, non-colorectal hepatic metastases as well as 128 patients who underwent hepatectomy for benign disorders. The elderly patient cohort (greater than 75 years of age) underwent fewer major hepatectomies when compared to the younger patient cohort. They were also less likely to be treated with chemotherapy than younger patients and less likely to be treated with resection for synchronous or metachronous lesions [5]. With this in mind, on subsequent multivariate analysis, the authors identified that male sex, malignant diagnosis, simultaneous non-hepatic procedures, increasing American Society of Anesthesiologists (ASA) score and increasing age were all associated with mortality. Further, each 10-year increase in age increased the odds ratio of mortality (OR 1.4).
Without being able to determine the true denominator in a stage-specific manner and careful provider and patient factor evaluations, it is difficult to definitively determine if differences in treatments are related to real or perceived risk differences in morbidity/mortality of the treatment.
Preoperative Assessment
A survey of SSO and ESSO surgeons indicated that there was a general concern of greater comorbidity, poorer physiologic tolerance, and greater frailty in elderly patients among surveyed surgeons. Despite this, there was no general agreement of the best appropriate way to assess and risk-stratify patients preoperatively. Current common surrogates include use of the ASA score, nutritional status, or performance status. Few respondents used any sort of frailty or geriatric assessment tool in routine clinical practice. Further, few providers routinely involved consultation from geriatricians in their preoperative assessment of a surgical candidate [1]. Thus, there remains a significant need for a useful tool for adequate preoperative assessment of the elderly patient undergoing major abdominal surgery and prediction of postoperative morbidity and mortality.
There is no standard screening tool for evaluating the elderly surgical patient. A European, multi-center prospective cohort study compared 12 screening tools to evaluate for major complications within the immediate perioperative period (30 days). Huisman et al. evaluated 328 patients, aged 70 and older, of which 18.6% experienced major complications. The most common operations were for colorectal cancer and breast cancer. Of note, the “Timed Up and Go” test evaluated basic functional mobility, coordination, and muscle strength by having patients stand up from a sitting position, walk 3 m, turn around, and return to a seated position [6]. Patients that take longer than 12 s to perform these tasks are not only at a greater risk for falling but also are at significant risk of developing a major complication (OR 3.1) [7]. ASA class (ASA >3, OR 2.8) and nutritional risk screening (if impaired, OR 3.3) were also predictors of major complications. ASA class is routinely used to evaluate preoperative patients and can be used for routine geriatric preoperative assessment. While nutritional risk screening is not routinely performed, serum albumin is commonly used as a surrogate test although it is widely viewed to be a poor predictive tool.
In more recent years, the use of cross-sectional imaging as an adjunct for predicting poor operative outcomes has been popular in trauma and acute care surgery. These tools have recently been evaluated for application in evaluating oncologic patients. In a Japanese trial, sarcopenia (as assessed from preoperative cross-sectional imaging) was associated with poorer overall survival and recurrence-free survival in the elderly. In a retrospective evaluation of all patients treated for hepatocellular carcinoma from 2004 to 2013, the area and Hounsfield units associated with the psoas, erector spinae, quadratus lumborum, transversus abdominis, external and internal oblique, and rectus abdominis were quantified for a total evaluated measure for skeletal muscle mass. On subgroup analysis, overall survival was significantly poorer in elderly patients (greater than 70 years old) with sarcopenia compared to those without (p = 0.002). Further, disease-free survival rates were also significantly associated with poorer prognosis in older patients with sarcopenia (p = 0.030). Notably, this distinction was not observed in younger patients. Multivariate analysis also suggested that patients with sarcopenia, more advanced Child-Turcotte-Pugh class, greater number of tumors, and poorly differentiated histology were also associated with poorer overall survival. Of these factors, only sarcopenia was found to also be significantly associated with disease-free survival on multivariate analysis. This study was limited in that it was a single-center trial and generally accepted definitions for sarcopenia have not yet been determined. However, sarcopenia has been significantly associated with poorer postoperative outcome and overall survival in colorectal cancer, melanoma, cirrhosis, and liver transplantation, suggesting that further validation of this finding, as part of a comprehensive preoperative assessment, may be warranted in the prospective evaluation of a geriatric surgical patient [8].
Portal Vein Embolization
For some patients, underlying hepatic disease or extent of planned resection may prompt concern about the size of the functional liver remnant following resection. Patients with hepatocellular carcinoma may have concomitant chronic hepatitis B, hepatitis C, and underlying cirrhosis. For younger patients, portal vein embolization is routinely used to enable hypertrophy of the remaining liver segments preoperatively. There is recent evidence that elderly patients are similarly able to tolerate portal vein embolization. Russolillo et al. prospectively evaluated 60 patients over the age of 70, who were matched with younger patients based on sex, diabetes, cirrhosis, exposure to chemotherapy and bevacizumab, and jaundice. When comparing both groups, median functional liver remnant volume and volumetric increase were similar. Both groups had similar rates of mortality (5.5 vs. 6.7%, ns) and major morbidity (25.9 vs. 22%, ns) following portal vein embolization. However, the rate of liver dysfunction/failure were higher in older patients (35.1 vs. 16.9%, p = 0.0001) [9]. Thus, early data suggests that while most elderly patients are likely to tolerate portal vein embolization preoperatively, there is a higher risk of developing post-embolization acute hepatic failure and fewer older patients do eventually undergo surgery.
Intraoperative and Immediate Postoperative Considerations
There are numerous studies affirming the safety and efficacy of hepatic resection in the elderly. The majority of patients experience similar operative times, intraoperative blood loss, and transfusion requirement as younger patients despite having a greater number of comorbidities and more severe cardiopulmonary disease.
Nachmany et al. [10] evaluated 174 patients undergoing liver resection for colorectal metastases between 2010 and 2015, comparing an elderly population (age ≥70, n = 54) to a younger cohort (age <70, n = 120). Elderly patients had an increased prevalence of ischemic heart disease (18.5 vs. 6.6%, p = 0.0002), COPD (9.2 vs. 4.1%, p = 0.01), and diabetes mellitus (30 vs. 14%, p = 0.02) when compared to younger cohorts. Hepatectomy operative times were slightly shorter in elderly patients but intraoperative blood loss and transfusion requirements were similar. Postoperatively, overall complication rates were similar between both groups, although they did find that elderly patients had a higher rate of major complications (11.1 vs 2.5%, p = 0.0001). Study investigators found no difference in length of hospital stay or 3-year overall survival.
These findings have been generally reproduced in other studies. Benedetto et al. performed a single-institution, case-control study evaluating hepatic resection for colorectal liver metastases in older adults compared to a younger cohort. Thirty-two patients aged 70 and older were matched 1:1 with younger patients by sex, primary tumor site, presence of liver metastases at time of diagnoses, number of metastases, maximum tumor size, type of hepatic resection, and timing of resection. While not perfectly matched (younger patients had a greater depth of tumor and greater regional nodal involvement), both groups underwent resections with similar operative times, transfusion needs, and type of surgical resections. They did not have significant differences in length of hospital stay, frequency of post-op complications, or recurrence during the study follow-up period. A 5-year disease-free survival was not significantly different between both groups (16.4 vs. 19.5% in younger patients). While overall survival was different between both groups, this was felt to be attributable to greater incidence of cardiovascular disease among the elderly cohort patients [2].
These observations were similarly seen in patients with hepatocellular carcinoma. In a study evaluating 299 Japanese patients with hepatocellular carcinoma, Sato et al. [11] examined patients who underwent curative resection at their institution between January 2000 and December 2010. Of these, 34 patients were considered elderly (age greater than 75). All patients underwent formal hepatectomy and adjuvant hepatic arterial infusion chemotherapy with 5-FU and cisplatin. In the immediate perioperative period, there was no difference in the proportion of patients undergoing major hepatectomy, length of operative time, intraoperative blood loss, or transfusion requirements. Postoperative complications were more common in the elderly, especially with rates of postoperative arrhythmia and delirium. This was attributed by the study authors to cardiovascular complications rather than directly to liver-related complications. This study found no difference in disease-free survival at 1-, 3-, and 5-year follow-ups between both groups. Just as importantly, there were no differences in recurrence rate, use of adjuvant therapy, or incidence of repeat resection between both groups.
An Australian meta-analysis by Phan et al. [12] evaluated 27 studies comparing hepatectomies in elderly (>70 years of age) versus younger patients. When comparing a total of 4769 elderly patients to 15,855 patients younger than 70 years, Child-Pugh class A status, presence of cirrhosis, proportion of minor vs. major resections, length of stay, number of transfusions, average tumor size, and positive margin status were similar between the two cohorts. Elderly patients were more likely to be diabetic (24.2 vs. 13.2%, p < 0.00001). While assessing postoperative complications, in-hospital mortality was similar between both groups, but 30-day mortality was two times higher in the elderly cohort (4.9 vs. 2.4%, RR 1.79, 95% CI 1.32–2.42). Recurrence rates and need for return to the operating room was similar between both groups. Elderly patients had a significantly higher risk of developing pneumonia, renal failure, stroke, and infection, though there was no difference in the rate of liver failure. Data on overall survival, when pooled, demonstrated a significant but marginally higher rate of survival in young patients versus the elderly (HR 1.10, 95% CI 1.01–1.19, p = 0.02). However, pooled analysis of disease-free survival showed no difference between both cohorts.
Published data also supports the ability to do laparoscopic resections in elderly patients. A prospective, case-control study comparing laparoscopic versus open liver resection evaluated the safety and efficacy of laparoscopic resection in elderly patients [13]. Patients were matched for age, sex, comorbid illness, Child-Pugh class, ASA grade, tumor size, and extent of resection. No significant differences were found in the patients’ preoperative baseline, median tumor size, tumor location, extent of hepatectomy, or operation time. Those patients who underwent laparoscopic resection had significantly less application of the Pringle maneuver (10.0 vs. 70.0%, p < 0.001), lower blood loss, lower total hospitalization cost (US$9147.50 vs. US$10,867.10, p = 0.008), and shorter hospital stay (5 vs. 10 days, p < 0.001). Postoperative complication rates were similar between both groups. This study was limited in that only one patient underwent a major hepatectomy.
In conclusion, elderly patients are able to safely tolerate major and minor hepatic resections with comparable intraoperative outcomes to younger patients. Patients also do not have a higher likelihood of return to the operating room. Elderly patients have comparable length of ICU stay and total hospitalization as younger patients. However, they are at significantly higher risk of developing postoperative complications including pneumonia, renal failure, stroke, infection, cardiac arrhythmia, and delirium.
Long-term Outcomes from Operative Intervention
The challenge in reviewing survival data lies in the mixed grade and cancer histologies examined, reliance on single-center trials, and extracting a patient’s concomitant comorbidities and non-cancer related mortality from overall survival data. Further, the heterogeneity in the elderly and young cohorts examined complicates tumor-specific survival data, including the size of lesions, number of lesions, well-differentiated versus poorly differentiated histology, lymph node involvement, and recurrence after resection.
Cucchetti et al. [14••] evaluated 919 patients undergoing hepatic resection for either cirrhosis or hepatocellular carcinoma. Median duration of follow-up was 5.5 years. In their analysis, separating patients by age into quartiles by years less than 60, 60–66, 67–70, and older than 70 years of age, they found no significant difference in 30-day or 90-day mortality in association with age.
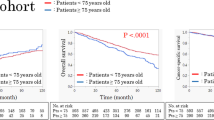
In a population-based, retrospective cohort study of colorectal liver metastases logged with the Ontario Cancer Registry, cases from 2002 to 2009 were examined for patients who underwent hepatic resection with complete follow-up through 2012 [15]. 1310 patients were identified and assessed for 90-day mortality and 5-year cancer-specific survival. When comparing patients less than 65 years old with those between 65 and 74 and greater than 75 years of age, there was an apparent trend in increasing 90-day mortality (2 vs. 5 vs. 8%, p < 0.001). 5-year cancer-specific survival prognosis also worsened with age (49 vs. 44 vs. 28% respectively, p < 0.001).
These conclusions were mirrored in a report by Mastoraki et al. [16]. In their cohort of elderly patients, they noted a higher prevalence of diabetes mellitus, coronary artery disease, chronic cerebrovascular disease, non-alcoholic fatty liver disease, insulin-resistance and chronic liver diseases. However, when comparing their elderly versus young patient cohorts, they found no significant difference in perioperative morbidity or overall survival. In their multivariate analysis, predictors of poor long-term survival were presence of extra-hepatic disease, high CEA levels (>200 ng/mL), and presence of 3 or more liver metastases. These are all factors specific to tumor burden, rather than comorbidities specific to the patient.
The impact that major surgery has on the elderly patient should also include discharge destination and impact on daily activities. In a retrospective review of a prospectively maintained database, Shutt et al. [17] reviewed the postoperative outcomes for 180 elderly patients (greater than 70) undergoing major and minor hepatectomies from 2003 to 2013. Of note, while the majority of these patients underwent hepatectomy for neoplastic disease, approximately 10% underwent resection for benign hepatobiliary conditions. Multivariate analysis did identify increased morbidity with age greater than 75 years. Further, older patients were more apt to require discharge home with home health or to a non-home discharge facility (i.e. acute rehab, subacute rehab, skilled nursing). Subgroup analysis did demonstrate that the risk of 90-day mortality, postoperative complications, and discharge to a skilled facility increased with age (cohorts greater than 70, 70–79, and greater than 80 years of age). As such, the study authors recommend that discussion of the risk of loss of preoperative independence be included into the informed consent process when discussing resection in this patient population, and “not assume that postoperative quantity of life is more important to the patient than quality of life” [17].
This question was also addressed by Balentine et al. [18••] when evaluating NSQIP data from 2011 to 2012 for very elderly patients (ager greater than 85) undergoing pancreatectomy, hepatectomy, or colorectal resection. This study evaluated 55,238 patients undergoing major abdominal surgery and specifically examined their risk for discharge to post-acute care facilities versus home. They determined that older age was a significant predictor for discharge to post-acute care facilities. Further, on subgroup analysis, even those patients who were functionally independent and did not incur postoperative complications had a 27 times greater likelihood of being discharged to a post-acute care facility, at a rate of 30% compared to younger patients. For patients who were functionally independent prior to surgery but did incur postoperative complications, they had a 66% rate of being discharged to a post-acute care facility. This was 11 times greater than younger patients who also endured postoperative complications. Based on these findings, the authors suggested that elderly patients were significantly more likely to be discharged to a post-acute care facility and that discharge planning needs be more extensively discussed preoperatively for elderly patients.
In conclusion, elderly patients do not have similar overall survival rates as younger patients, though this is likely attributable to underlying cardiopulmonary disease and natural life expectancy. There remains some disagreement as to whether elderly patients experience the same disease-specific survival as younger patients, and conclusions depend on the cohort and histology that is examined. However, two large trials suggest that geriatric patients undergoing major abdominal surgery are more likely to require home health or discharge to a post-acute care facility. Thus, these potential consequences should be discussed with the patient during preoperative counseling and informed consent. Further, additional steps could be taken to optimize patient health and conditioning prior to surgery to facilitate greater likelihood of discharge home.
Conclusion
Appropriately selected, elderly patients are able to safely tolerate hepatic resection for oncologic indications. While there is greater risk for postoperative complications given the greater prevalence of medical comorbidities, patients are able to tolerate operative intervention with comparable operative time, blood loss, transfusion needs, ICU requirements and in-hospital length of stay. Further study is warranted with regards to neoadjuvant therapies. Although tolerated in younger patients with good results, these therapies could result in excessive decline in performance status or morbidity preventing more definitive surgical therapy in the elderly. Current data suggests that while disease-free survival remains comparable to that of younger patients, overall survival may be worse. This is further complicated by the evidence that elderly patients have greater risk of being discharged to post-acute facilities after hospitalization even when they do not develop post-op complications.
Tumor biology is a major determinate of cancer-specific survival of patients regardless of age. With modern intraoperative and postoperative care, most elderly patients can survive the immediate postoperative period. Careful patient evaluation and risk assessment followed by a thorough surgeon-patient discussion is required to help determine the best treatment for an individual patient. The surgical maxim of “nothing reveals a patient’s age as quickly as a postoperative complication” is still true and a patient who has lost his/her independence may not feel improved by surgery. Moreover, competing causes of death are a real concern as a patient ages and the years potentially gained by any therapy are lower compared to younger patients. Therefore, tolerance of risk of complications and adverse outcomes becomes equally important to potential for cure in the elderly. With improvements in systemic therapies and in particular other less invasive regional therapies such as stereotactic radiation, percutaneous ablation and intra-arterial therapies, there are more choices to balance benefit and risk. Age alone should not be a contradiction to surgical intervention.
References
Papers of particular interest, published recently, have been highlighted as: •• Of major importance
Ghignone F. The assessment and management of older cancer patients: a SIOG surgical task force survey on surgeons’ attitudes. Eur J Surg Oncol. 2016;42(2):297–302.
Benedetto, Fabrizio et al. Liver resection for colorectal metastases in older adults: a paired matched analysis. J Am Geriatr Soc 59.12 (2011): 2282–2290. Web. 14 Jan. 2017.
Horgan A, et al. Patterns of care and treatment outcomes in older patients with biliary tract cancer. Oncotarget. 2015;6(42):44995–5005.
Lee B, et al. Older adults with biliary tract cancer: treatment and prognosis. J Am Geriatrics Society. 2012;60(10):1862–71.
Reddy SK. Major liver resection in elderly patients: a multi-institutional analysis. JACS. 2011;212(5):787–95.
CDC gov. STEADI materials for health care providers—older adult fall prevention, CDC Injury Center. Np; 2017. Web. 14 Jan 2017.
Huisman MG, et al. Screening for predictors of adverse outcome in onco-geriatric surgical patients: a multi-center prospective cohort study. EJSO. 2015;41(7):844–51.
Harimoto N, et al. Sarcopenia is a poor prognostic factor following hepatic resection in patients aged 70 years and older with hepatocellular carcinoma. Hepatol Res. 2016;46:1247–55.
Russolillo N, et al. The influence of aging on hepatic regeneration and early outcome after portal vein occlusion: a case-control study. Ann Surg Oncol. 2015;22:4046–51.
Nachmany I, et al. Resection of colorectal liver metastases in the elderly—is it justified? J Surg Oncol. 2016;113:485–8.
Sato S. Hepatic resection for hepatocellular carcinoma in the elderly: selecting hepatectomy procedures based on patient age. Anticancer Res. 2015;35:6855–60.
Phan K, et al. Hepatic resection for malignant liver tumors in the elderly: a systematic review and meta-analysis. ANZ J Surg. 2015;85:815–22.
Wang XT, et al. Pure laparoscopic versus open liver resection for primary liver carcinoma in elderly patients: a single-center, case-matched study. Medicine. 2015;94(43):1–7.
•• Cucchetti A. Effect of age on survival in patients undergoing resection of hepatocellular carcinoma. Br J Surg. 2016;103(2):e93–9. This study offers a characterization of the difference in postoperative mortality and survival rates for elderly patients as compared to younger patients. It further classifies these differences by stratifying elderly patients into multiple age groups.
Booth CM, et al. Management and outcome of colorectal cancer liver metastases in elderly patients: a population-based study. JAMA Oncol. 2015;1(8):1111–9.
Mastoraki A, et al. Outcomes following major hepatic resection in the elderly patients. Clinics and Research in Hepatology and Gastroenterology. 2014;38:462–6.
Shutt TA. Permanent loss of preoperative independence in elderly patients undergoing hepatectomy: key factor in the informed consent process. J Gastorintest Surg. 2016;20:936–44.
•• Balentine CJ, et al. Postacute care after major abdominal surgery in elderly patients: intersection of age, functional status, and postoperative complications. JAMA Surg. 2016;151(8):759–66. This study evaluates the rate of postoperative complications and post-discharge destination for elderly patients after major abdominal surgery. It highlights that while elderly patients may tolerate surgery similar to younger patients in the immediate postoperative period, the rates of perioperative complications can be significantly higher and elderly patients tend to be discharged to acute rehabilitation facilities more frequently.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Jeffrey Sussman and Winifred Lo declare no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Surgical Care for the Geriatric Patient
Rights and permissions
About this article

Cite this article
Lo, W., Sussman, J.J. Hepatobiliary Oncologic Surgery in the Elderly. Curr Geri Rep 6, 127–132 (2017). https://doi.org/10.1007/s13670-017-0212-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13670-017-0212-2