
Abstract
Surface electromyography (sEMG) meets extensive applications in the field of prosthesis in the current period. The effectiveness of sEMG in prosthesis applications has been verified by numerous revolutionary developments and extensive research attempts. A large volume of research and literature works have explored and validated the vast use of these signals in prostheses as an assistive technology. The objective of this paper is to conduct a systematic review and offer a detailed overview of the work record in the prosthesis and myoelectric interfaces framework. This review utilized a systematic search strategy to identify published articles discussing the state-of-the-art applications of sEMG in prostheses (including upper limb prosthesis and lower limb prostheses). Relevant studies were identified using electronic databases such as PubMed, IEEE Explore, SCOPUS, ScienceDirect, Google Scholar and Web of Science. Out of 3791 studies retrieved from the databases, 188 articles were found to be potentially relevant (after screening of abstracts and application of inclusion–exclusion criteria) and included in this review. This review presents an investigative analysis of sEMG-based prosthetic applications to assist the readers in making further advancements in this field. It also discusses the fundamental advantages and disadvantages of using sEMG in prosthetic applications. It also includes some important guidelines to follow in order to improve the performance of sEMG-based prosthesis. The findings of this study support the widespread use of sEMG in prosthetics. It is concluded that sEMG-based prosthesis technology, still in its sprouting phase, requires significant explorations for further development. Supplementary investigations are necessary in the direction of making a seamless mechanism of biomechatronics for sEMG-based prosthesis by cohesive efforts of robotic researchers and biomedical engineers.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
In general, the sEMG signal comprises of superimposed motor unit action potentials (MUAPs) which exist in the vicinity and the pick-up range of the surface electrodes. On account of the variations in amplitude and frequency content of sEMG signal with regard to the level of contraction force [1, 2], user control of assistive devices aided by the muscle contractions is possible. In general, assistive devices, commonly known as prostheses, are artificial devices that replace a missing body part and restore the normal functions of the missing body part. The body part may be lost through trauma, a disease, or a congenital disorder. In principle, sEMG signals are acquired from the patient's (i.e., the amputee's) body. After suitable processing of the acquired sEMG data, the processed data is fed as control input to drive motors coupled to the prosthetic device. Usually, the prosthetic device is worn by the amputee, and the amputee's sEMG signals initiate the control mechanism for the device.
With the introduction of the concept of sEMG in the 1940s [3], the first successful attempt towards the development of a myoelectric prosthetic arm as an application of sEMG was made in 1960 [4]. Over the past few decades, research has tended to focus on the applications of sEMG interfaces. Besides establishing their prospective in applications for disabled individuals [5,6,7,8,9,10,11], myoelectric interfaces have also substantiated their promising applications for healthy users [12,13,14,15,16,17]. Furthermore, several patents in the field of mobile technology have been encouraged as a result of the numerous advantages of sEMG interfaces over conventional devices [18, 19].
There has been a growing interest in sEMG-based prosthesis applications over the past decade. Figure 1 shows the trends in publications related to the sEMG-based prosthetic device, its control, and applications for various years. The trends indicate (1) a substantial increase in publications demonstrating ongoing research in this field and (2) the active participation of researchers in the maturation of sEMG-based prosthetic devices.

Trends in the number of publications associated with sEMG and its applications in prosthetic devices. The data (number of publications for each year) has been taken from Google Scholar
In comparison to the conventional and supplementary techniques of man–machine control, it has been suggested that the sEMG interface provides a number of benefits. It has been shown that comparatively less user attention is entailed in sEMG control unlike EEG–based controls or controlling action via movements of the eye. Contrary to visual–based control, the myoelectric control permits the user to gaze about during the controlling task of the device. Also, sEMG signals offer reasonably high signal-to-noise ratio in comparison of other biosignals. When compared to voice control, sEMG control has just a minor delay. Furthermore, sEMG control is robust to and insensitive to changes in ambient sound. For users with motor impairment, sEMG interfaces may assist in the development of interactive interfaces with minimal requirement of user motor skills. Nevertheless, some training is requisite to make the user familiar with the interface. The electrodes employed in sEMG recording offer ease in their placement and may be placed beneath the clothes or even fixed over them [20, 21]. Commercial textile electrodes (including smart shorts) which measure the EMG activity are available whose control commands are delivered via delicate movements or various intensities of muscular contractions [21,22,23]. Conclusively, no marking is made on handicapped users or users with exceptional concessions by the sEMG interface.
The superficial muscles of the human body are the locations of measurement of sEMG signals [24]. In the sEMG interfaces, muscles of the upper limbs [5, 25], the lower limbs [26], the shoulder or the head, face, and neck [27,28,29] have been utilized. Accordingly, by using their contractible muscles (which they are able to contract), users with mobility disabilities can control a number of devices. For instance, using the contractions of the facial muscles, a device can be controlled by a quadriplegic individual [6]. Moreover, sEMG signal can be recorded from the stump skin of the amputees in order to control the prosthesis [5, 25, 30, 31]. Thus, an amputee is allowed to perform a variety of controlling actions (such as grasp posture of prosthesis) merely by the usage of residual muscles. Moreover, some relevant reviews have been reported in the literature which discussed about the imperative issues associated with sEMG signal measurement and processing [8, 32, 33] along with the precarious issues and endorsed practices in view of myoelectric interfaces [34]. Also, researchers have shown keen interest towards sEMG interfaces which is mainly observed due to the pattern recognition-based approach for controlling action embraced in 1993 in interfaces linked to sEMG [35]. One of the major aspects is the massive use of sEMG signals in prostheses as an assistive technology.
Based on the above framework and the above dialogue, this review article presents an all-inclusive discussion of the state-of-the-art applications of sEMG in prostheses. This narrative literature review highlights the recent developments and underscores the challenges associated with sEMG-based prosthesis. Contrary to the existing reviews, this review also suggests some critical directions to follow to improve the performance of sEMG-based prosthesis. This review also provides some guidelines for the acceleration of future developments. Like other existing reviews, this review is also subject to limitations including but not limited to: (1) potential bias, including the influence of the authors' viewpoints, and (2) gaps in literature-searching practices that might have led to the omission of relevant research. We also tried our best to avoid misrepresenting or misinterpreting the source data.
Review Organization: This review is structured as follows. Section 2 describes the methodical search strategy followed for performing this review. Section 3 provides a comprehensive description of the result and applications of sEMG signal in prostheses (including upper limb and lower limb). Section 4 provides discussions and a list of challenges associated with sEMG-based prostheses. Finally, in Sect. 5, the review ends with the concluding remarks and some prospects in sEMG-based prostheses technology for boosting its broad and extensive utilization.
2 Methodology
For this review, a comprehensive literature search was performed from many databases using generic search terms such as “Surface Electromyography”, “sEMG”, “Prosthesis”, etc. The following databases were chosen for the literature search based on the high number of results: IEEE Explore, ScienceDirect, PubMed, Google Scholar, and Web of Science. The following keywords (and their combinations) were adopted for the literature search: Surface Electromyography, Myoelectric control, Prosthesis, Amputees. For the search, we considered publications (1) in journals and conference proceedings later than 1950, and (2) mostly in English, due to the predominance of the English language in scientific literature. Other articles extracted from the references of the papers identified in the electronic search were also included. Indeed, many articles on sEMG (and its applications) existed before 1950. However, we restricted our search to articles from 1950 onwards for the following reasons: (1) to narrow down the number of articles included in the review; and (2) to consider advanced and state-of-the-art in sEMG and exclude obsolete technologies.
A large number of publications on sEMG were retrieved during the initial screening. Hence, to include the searches with the main focus on sEMG-based prosthesis, an inclusion criterion was utilized in the search string. From the selected databases, the search retrieved a total of 3791 publications. Then, the duplicate records were removed. After that, based on the title and abstract, the remaining 2758 publications were screened for their relevance by using the following inclusion and exclusion criteria. Publications focusing on ‘sEMG-based prosthesis’ were included, whereas those works which delivered theoretical concepts on sEMG were excluded. We also excluded those studies available only in the form of abstracts. Besides, if the paper was a workshop summary, we excluded it.
Based on the screening and eligibility, 188 research chronicles were identified that offered explicit applications of sEMG in prosthesis, and were found to be relevant to this review. The review process is shown in Fig. 2 by the PRISMA flow diagram. PRISMA i.e., “preferred reporting items for systematic reviews and meta-analyses” is employed in systematic reviews to refine the quality of reporting.

PRISMA flow diagram illustrating the search and inclusion process. N represents the number of records
For better identification and visualization of the clusters that influence the topic of this review paper, we exploited VOSviewer: a software tool infrastructure that constructs and visualizes bibliometric networks. Figure 3 illustrates the network visualization where items are represented by using their labels and, by default, also by a circle. The network has 54 clusters, each representing a unique color. The item’s weight determines the label's size and its corresponding circle size. The higher the weight of an item, the larger the label and its associated circle. For example, referring to Fig. 3, the item “electromyography” has the highest weight and the largest label and circle sizes.

Network visualization: term co-occurence map showing the network of co-occuring keywords with VOSviewer
3 Results and applications in prosthetic devices
One of the greatest applications scrutinized in the perspective of sEMG interfaces is the EMG prostheses as evident from an immense expanse of research chronicles [36,37,38,39,40,41,42,43,44,45,46]. Established by the Central Prosthetic Research Institute of the USSR in 1960s, the first commercial prosthetic arm was a revolutionary step in the arena of sEMG applications in upper limb prostheses (ULP) [4]. This prosthetic arm included one DOF (open and close) which used strong antagonistic muscle contractions for control action. Regardless of the fact that the realization of high classification accuracies for about twelve classes [25, 47] has been reported in erstwhile sEMG investigations, the contemporary sEMG-based ULP employ the classical threshold-based concepts. On–Off control based on threshold is one of the easiest methods for control which actuates the desired function whenever a preset value of threshold falls below the sEMG amplitude. In addition, different channels positioned over physiologically apt muscles can be allotted different functions. Nonetheless, for controlling one DOF (such as hand opening or closing), as a minimum, two signal sites are needed. Moreover, the series of muscle activity (starting from the threshold and terminating at the value of maximal muscle contraction) may be separated among numerous intervals such that each interval links to a specific prosthetic function [48]. Rate coding (which involves utilization of speed of the muscle contraction) and pulse coding (which utilizes pulses of sEMG activity as the control command) are two more strategies employed in commercial prostheses [48]. After the introduction of the advanced ULP, the markets were flooded with multiple-DOFs based prostheses as shown in [34]. These systems ensure control of DOFs in a sequential and consecutive manner. Unintuitive movements are necessary for the production of two sEMG control signals (one for using both DOFs and the other for switching between two DOFs). For switching between different DOFs, co-contractions are required. One of the major limitations of this approach is the incapability of concurrent control of multiple joints and increased complexity with increasing number of DOFs. Some of the major advancements and pioneering investigations in the field of sEMG-based prostheses have been discussed in the following sub-sections. More specifically, we present the review results for both upper and lower limb prostheses detailed in many aspects, as illustrated in Fig. 4.

Organization of review results
3.1 Upper limb prosthesis
Upper limb amputation ominously hinders the performance of amputees towards their daily activities. The functions of such lost limbs can be seamlessly re-established by utilizing the signals from residual stump muscles via myoelectric prostheses. Many remarkable attempts have been made by a number of researchers and academicians towards ULP control via sEMG.
3.1.1 Levels of upper limb amputation
Usually, the upper limb amputation can be categorized into various types as exemplified in Table 1 [49]. However, the levels of upper limb loss can be classified as transcarpal, wrist disarticulation, transradial, elbow disarticulation, transhumeral, shoulder disarticulation and forequarter [50, 51]. The sEMG-based prostheses control for amputees with various levels of amputation has been addressed by a huge volume of literature works.
3.1.2 Related work
A comprehensive assessment on the improvements in the arena of sEMG-based control of ULP has been presented in [52]. Also, state-of-the-art evaluations on control of prosthetic hands via myoelectric controlling action [53], the hybrid myoelectric control systems in [54] and bionic prosthetic hands have been put forward in literature. Moreover, some imperative issues associated with control strategy (based on sEMG and pattern recognition) for versatile and multi-purpose myoelectric ULP have also been discussed in [49]. These concerns include sEMG processing and evaluation along with the performance analysis of algorithms for pattern recognition. For the measurement of sEMG signal for clinical applications, a sensor system was developed in [55]. The sEMG signals at various muscles located above the elbow for activities like elbow flexion/extension, abduction/adduction were studied. As a whole, the earlier mentioned effort along with [56], delivered an enhanced knowledge of sEMG analysis and opened new prospects for the design of powerful, flexible and efficient prostheses.
Using Independent Component Analysis, the application of sEMG signal towards the control and governance of myoelectric ULP has been demonstrated [57]. In [57], the patterns corresponding to various hand actions were determined on the basis of two correlations: first correlation between the muscle voluntary contraction and the degree of motor movement, and the second correlation between motor frequencies and the degree of motor movement. In another work considering the amputation below the elbow [58], a body-powered prosthetic hand was developed which was regulated by EMG signals via DSP by means of virtual prosthesis implementation. The recommended system was implemented and tested with acceptable results due to the fast-processing capability of the considered processor. Another pioneer work dealt with advanced robotic hand control via sEMG wherein the effective real-time control of finger force and position of a highly dexterous robotic hand was demonstrated by integrating machine learning and simple downsampling approaches [59]. The impedance control was used to exert force for holding and grasping of objects.
Moreover, a single channel sEMG control of a simple, fast and low-cost advanced prosthetic hand has been demonstrated [60]. It can recognize four gestures specifically the closing of hands, opening of hands, flexion of the wrist and double flexion of the wrist. On the basis of predefined grasp postures, it was verified that these gestures can be utilized for controlling a prosthetic terminal. Real-time gesture recognition and acceptable classification accuracy were observed through experimental investigation [60]. In the context of wireless and mobile platform for sEMG acquisition, a cost-effective mobile apparatus for effective prosthetic control was established which could perform continual operation based on daily activities [61].
For adequate detection of posture and grasp force of amputees via sEMG, an experiment was performed which demonstrated satisfactory feed-forward control of a dexterous prosthesis [62]. Another major contribution towards control of prosthetic movements was made in [63] by analyzing a precise discrimination among discrete and collective finger movements. In this work, the sEMG signals were utilized for posture control of various fingers of hand prosthesis. A multichannel sEMG for synchronized, multi-axis, comparative regulation of prosthetic systems was developed to ensure instantaneous controlling action of activities like rotation of wrist, flexion or extension of wrist, and grasping for able individuals as well as transradial amputee [64].
Also, sEMG based test tool was presented for envisaging realizable function in intentional control via EMG [65]. This method assists in the prosthetic control training and fitting, and measures proportional prosthetic control in upper limb amputees before prosthetic fitting. This tool was developed with the aim of pre-evaluating the activation skills of the trainable voluntary muscle to assist in decision support in advance of prosthetic fitting. Also, long term stability of sEMG (from the forearm muscles) pattern classification for ULP control has been inspected in [66]. Some of the important advancements in ULP design and control based on sEMG have been elucidated in Table 2.
For dexterous control of ULP via sEMG, classification of essential hand movements via forearm muscles has also been reported [67]. Another work provided a database directed towards the investigation of the correlation among sEMG, kinematics and forces of the hand, with the intention of establishing a non-invasive robotic hand prosthesis with regular monitoring and governance action [68]. Other works proposed fuzzy model for simultaneous control of bionic hand wherein the construal and investigation of sEMG of amputees were done [69, 70].
3.1.3 Classification of sEMG signals for ULP
Various approaches for processing and classification of sEMG signals have been elucidated in [76] for prosthetic control applications along with [77]. Some of these classification techniques and their applications in sEMG-based prosthesis control have been presented in Table 3. Besides the classification techniques mentioned in Table 3, other machine learning techniques, such as k-nearest neighbor (k-NN), Naive Bayes (NB), decision tree (DT), etc., have also been utilized in sEMG-based prosthetic devices. For instance, a system on chip (SoC) Raspberry platform exploits a multi-thread algorithm to operate a prosthetic hand device using k-NN and DT machine learning techniques.Footnote 1
Based on the existing literature, it is shown that the classification techniques (mentioned in Table 3) can achieve satisfactory and high classification accuracies of up to 99% [79]. However, the choice of the classifier remains to be one of the potentially unresolved issues that needs to be addressed. While the classification performance might not be heavily reliant on the choice of the classifier, the number of samples greatly influences the classifier's performance. For instance, downsampling might enhance the classifier performance by artificially increasing the number of samples. An increased sample size might reduce the variance of the estimator (even though the samples are not independent), consequently improving the classification accuracy. Besides, to be successful in classifying the sEMG signal, the selection of a feature vector ought to be carefully considered. More simply, a robust classifier can only perform well if the choice of features is good. In addition, there is a bias-variance trade-off and various analytics trade-offs in an end-to-end machine learning-based classification system for sEMG signals. Thus, the choice of the classifier remains debatable, and a well-defined solution to this problem seeks thorough investigation and exhaustive experiments.
3.1.4 Advancements in ULP for different amputees
For the evaluation of ULP control based on sEMG and pattern recognition, an investigation was carried out in [91] on transradial amputees for 2-DOF electric prosthesis control in the completion of everyday activities. The foremost intentions were to evaluate the outcomes of a transradial amputee via the control strategy for 2-DOF prosthesis and to analyze the skill acquisition pace in users with transradial amputations. For analyzing the effects of user adaptation over the performance of myoelectric control in dexterous and intuitive activities, real-time experiments were performed on able-bodied individuals as well as disabled individuals (with transradial amputation) [92]. It was shown that significant improvements in performance occur due to user experience. In another work [93], the signal acquisition and investigation for recognizing numerous movements of the hand pertaining to their use in prostheses was investigated. Along with the indispensable movements for grasping action, five movements for the wrist-hand mobility were also analyzed. Also, sEMG data acquisition and handling for smart identification of prosthetic action was presented in [94] for realizing the exact and proficient controlling action of the restoration apparatus or smart prosthesis in sports. Nine actions were used for extracting sEMG signals, and these are abbreviated as rest (Re), closing of hand (HC), opening of hand (HO), pronation (PR), extension of wrist (WE), flexion of wrist (WF), thumbs up (TU), contact of thumb with index finger (TI), contact of thumb with middle finger (TM).
Moreover, algorithms such as Adaptive threshold method for processing of sEMG signals have been used which assist in the design of more accurate and competent controllers for users with upper limb amputation [95]. Shared control of EMG-controlled prosthetic hand [96], recognition and categorization of simple and intricate movements associated with finger flexion via sEMG [97] along with the neural network aided pattern examination and classification [98] have also been reported. Also, classification of movements of the fingers for sEMG-based control of prosthesis has been presented [99]. Upper Extremity Limb Function Discrimination via sEMG analysis proved useful in the generation of control signals for prosthetic devices [100]. Another work employed an investigation of the configuration of electrodes for Targeted Muscle Reinnervation (TMR) centered on the Neural Machine Interface platform [101]. The investigational results provided significant strategies for real-world placement of the EMG electrodes so as to stimulate promising clinical uses of TMR and sEMG-pattern recognition in multifunctional prostheses control. Also, nonlinear feature extraction as well as classification techniques have been recommended and evaluated for identification of numerous sEMG-based hand manipulations [102].
Many feature extraction techniques are available for extracting features from the acquired sEMG signals. In general, sEMG feature extraction can be categorized into three methods: (1) time domain, (2) frequency domain, and (2) time–frequency domain. The most common features used for sEMG pattern recognition are time domain features. The reason is that time domain features are easy and quick to calculate as they do not require any transformation. Time domain features assume the data as a stationary signal, i.e., the time domain features are computed based on the amplitude of input signals. Thus, they are advantageous when the signals are recorded in low-noise environments. Any interference acquired through the recording becomes the disadvantage of the time-domain features. Common time domain features include Mean Absolute Value, Mean Absolute Value Slope, Zero Crossings, Slope Sign Changes, Waveform Length, Root Mean Square, Histogram, etc.
Frequency domain features are usually obtained by transforming the raw sEMG signal from the time domain to the frequency domain. In principle, most of the frequency domain features are normally based on the signal's power spectral density (PSD). Frequency domain features include mean frequency, median frequency, peak frequency, mean power, total power, the 1st, 2nd, and 3rd spectral moments, frequency ratio, power spectrum ratio, the variance of central frequency, etc. Compared to time domain features, frequency domain features are computationally expensive in terms of resources and time. However, they are sometimes approximations of the time domain features. They are only beneficial if the feature space quality in class separability is better than that obtained with the time domain features.
Time–frequency domain features provide signal information in both time and frequency domains. The signal is non-stationary, with different frequency components varying with time. Thus, time–frequency domain features are more advantageous than time and frequency domain features alone. These features are richer in information and, therefore, guarantee a more satisfactory performance of the classifier. However, the drawback is that these features require more resources and time for their computation. The features from the time–frequency domain include, but are not limited to, short-time Fourier Transform, wavelet transform, and wavelet packet transform. A detailed discussion of sEMG feature extraction methods is beyond the scope of this review. We refer interested readers to work by existing extensive reviews on sEMG feature extraction for in-depth study.Footnote 2
Some of the research works utilized PCA (Principal Component Analysis) for processing sEMG to control the prosthetic device. These works have been summarized in Table 4. PCA is an unsupervised feature extraction scheme commonly used in sEMG-based prosthetic applications. It reduces the dimensionality of the sEMG data to make it appropriate for various myoelectric applications. The strong preference for the PCA algorithm for sEMG data preprocessing over other algorithms is due to the following reasons: (1) In essence, the PCA recognizes a typical temporal pattern across large datasets of sEMG signals, and describes a low-dimensional space wherein the original signals can be expressed as vectors and then classified. Thus, the PCA is beneficial in processing the sEMG activity of individual muscles recorded during several variants of one motor action (or even different motor behaviors), and then characterizing the temporal patterns linked with various components of the motor action. (2) PCA-based sEMG data decomposition fosters unraveling the intrinsic coordinative structures in the correlated patterns of variation among joints or body segments. Such structures (e.g., walking and gait) might yield helpful information on body control mechanisms and consequently assist in correlating walking patterns with injuries. (3) PCA can assist in identifying spatial–temporal neuromuscular synergies underlying the motor behavior, when the sEMG activity is recorded via multi-electrode systems from many muscles throughout the body during one or more motor actions. (4) Principal Components that explain a considerable proportion of the data variation is usually linked to the control signal outputs of spinal pattern generators. On the other hand, the remaining principal components are likely to be associated with the system-related random noise. Thus, the analysis of the sEMG activity becomes more manageable, and higher performance accuracy can be achieved. In summary, PCA captures features from sEMG signals that can provide insight into the activation state of motor neurons and the nature of the premotor control signals. Such rich features may improve the existing technologies in clinical, neurophysiological, and rehabilitation domains.
3.1.5 Other works
A prototype of concurrent hand prostheses driven by sEMG signals using PID controlled DC motor was presented wherein the signal acquisition was performed over the biceps and triceps brachii muscles [108]. In another work, the utilization of pattern recognition for torque estimation of the torque and its realistic enactment for controlling a unique two DOF wrist exoskeleton was done [109]. Also, another investigative analysis presented the concept of synergy matrices with the intention of extracting fluid wrist movement intents by sEMG, thereby permitting users with wrist amputations to efficiently make use of wrist prostheses [110]. Another work proposed a technique to classify the movements of the fingers to achieve dexterous control of hand prostheses via the sEMG signals recorded from the forearm [111]. Moreover, a two-part inspection was performed to investigate the application of forearm sEMG signals for instantaneous supervision of a robotic arm [112].
In another work, a Knit band sensor has been presented for myoelectric control of hand prostheses based on sEMG signals [113]. Moreover, the control of multi-purpose transradial prostheses by means of pattern recognition has been investigated [31]. Self-regulating pattern recognition scheme for sEMG-based ULP control [114], extraction of real-time and relational data associated with neural control for prostheses with multiple DOF via sEMG signals [115] and sEMG-based estimation of clench force for neural prosthesis hand [116], have also been reported. Moreover, constant hand prosthesis control via non-linear incremental learning has been presented in [117]. A novel approach for extracting sEMG features centered on muscle active region had been anticipated wherein an experiment was designed for classifying four hand movements via a number of sEMG features [118].
Another work recommended the commencement in the investigation and exploration of prosthetic bimanual manipulation via sEMG in unilateral and bilateral amputees with upper limb amputation [119]. Also, the design concerns associated with wireless acquisition of sEMG signals from multiple channels in the control of hand prostheses have been explored in [120]. Additionally, a novel sEMG sensor has been projected for the disabled for prosthetic limb control (hand prostheses) in day-to-day activities [121]. Notably, apart from upper limb prostheses, the viability of using neck and face surface sEMG with the intention of controlling the commencement, compensation, and pitch of an Electrolarynx controlled by EMG signals has been investigated [122]. For the prosthetic voice control, eight individuals who had undergone total laryngectomy were considered.
For the ULP control, the evolving opportunities and challenges associated with the abstraction of neural evidence from sEMG were discussed in [123] where the classical myoelectric control was eloquently described. Two sEMG channels are employed for controlling one DOF at once. For instance, the flexors of forearm and the extensors of the forearm may be utilized as two channels. At a given time, either the flexion as well as extension of the wrist; or opening and closing of hand can be controlled by the two channels. For each channel, a threshold is chosen so that whenever the threshold is surpassed, the activation of the corresponding DOF occurs. If both thresholds are surpassed simultaneously, switching of the mode of the controller to the other DOF takes place. Though this method offers restricted functionality, it proves to be very important for control of prostheses.
3.1.6 Integration of sEMG-based ULPs with IMUs
In general, sEMG-based ULP devices are made position aware (POS) using inertial measurement units (IMUs) to monitor various movements of the upper limbs. Some of the recent works that have reported integration of sEMG based ULPs with IMUs are tabulated in Table 5. In prosthesis control in biomedical research, sEMG remains the gold standard for providing gesture-specific information, exceeding the performance of IMUs alone. However, the integration of IMUs for kinematic quantification with sEMG for muscle activity analysis offers manifold advantages: (1) Using these two sensor modalities (IMU and sEMG) provides statistically significant improvements over individual modality in terms of accurate and consistent classification results. (2) Combining these two sensing modalities can significantly enhance the gesture-based control of upper-limb and lower-limb prosthetics. (3) Statistical features from IMU data can be advantageous in predicting motor function scores for assessing the quality of movement. (4) IMUs can be used for computing joint torques through inverse dynamics and integrated with sEMG activity to objectively assess patients' spasticity after stroke.
3.2 Lower limb prosthesis
Most of the lower limb amputations belong to the categories of transtibial (below-knee) or transfemoral (above-knee) type. Accordingly, prosthetic devices encompassing knee joints and feet are the most common lower-limb prosthetic components that are envisioned to substitute the biomechanical purpose of the foot in addition to ankle joint. Recently, robotic prostheses are finding immense applications among users with lower limb amputations.
3.2.1 Basic concepts and preliminaries
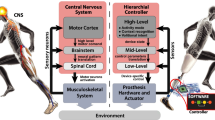
The indispensable constituents of robotic leg prosthesis [130] have been presented in Table 6. Also, the generalized framework for active lower limb prostheses/orthoses (P/O) control [131] has been illustrated in Fig. 5. This sketch reveals the physical interface and signal-level feedback paths involved in the real-time application of powered assistive devices.

Generalized supervisory structure for active lower limb prostheses and orthoses
3.2.2 Related work
A systematic and narrative evaluation on design concerns and clarifications associated with active lower limb prostheses (LLP) has been presented [132]. Users with lower limb amputation have used novel LLP designs with enhanced stability and reduced energy requirements in level-ground walking [133]. The upgraded function of artificial legs through advanced computerized control and efficient prostheses have enabled the users to perform versatile activities. In [134], the fabrication of a cost-effective prosthetic leg via EMG signals was proposed for amputees with lower limb amputation. The sEMG signal procurement and processing for prosthetic legs was demonstrated in [135]. Also, an active above knee prosthesis was presented and described which was designed to compensate the movements of transfemoral amputees [136]. The use of sEMG-pattern recognition-based phase dependent strategy was used for identification of user locomotion modes [137]. For successful recording of high quality sEMG signals to be acquired from the interior of the sockets of lower limb (transfemoral) amputees, four exemplary integrated socket–sensor designs were used [138]. The employment of EMG signals towards robotic ankle systems control in LLP (including knee-ankle prostheses and ankle–foot prostheses) has been explored in [139] and the summary of the control algorithms has been elucidated in Table 7.
3.2.3 Notable advancements
Table 8 summarizes some of the notable works on lower limb prosthesis.
In [155], the authors shed light on the potential of sEMG control for enabling new functionalities in robotic LLP and discuss the pitfalls and prospects for future research for both human motor control and clinical practice. For incessant recognition of the locomotion mode for prosthetic legs on the basis of neuromuscular–mechanical fusion, an investigation was performed on patients with transfemoral amputations [156]. The findings of [157] assisted in the design of the state-of-the art lower limb assistive devices of the future including prostheses. In a recent work [158], the authors proposed the sEMG-based real-time motion pattern recognition to assist hemiplegia patient in walking. Another study focused on the proposal of an effective algorithm to identify the terrain type over which the person who uses prosthetic leg moves [159]. In [160], the authors presented a sEMG-based online adaptive prediction of human motion intention. In another notable work [161], a standard machine learning approach was presented sEMG-based intention-detection systems of lower limb to intelligently boost human–robot interaction systems and detect subject’s walking direction prior-to or during walking. Further, a neural network-based control algorithm was proposed for sEMG-based control of ankle prosthesis [162]. In [163], the authors proposed a novel machine learning-driven neuromusculoskeletal model able to predict lower limb joint torque using sEMG sensors of LLP. Another work demonstrated the development and evaluation of an adaptive intent recognition algorithm for sEMG-based leg prosthesis [164]. However, attributable to some difficulties encountered in the sEMG field, the contemporary trends emphasize the cybernetic era of prostheses in the impending years [165].
3.2.4 Integration of sEMG-based LLPs with IMUs
Like ULPs, various sEMG-based LLPs have been integrated with IMUs to make them position aware and keep track of the movements of the lower limbs. Table 9 presents a list of some of the works that focus on coupling sEMG with IMUs for LLP control.
4 Discussions on common Pitfalls and Challenges
Reviews on the challenges, complications and implications of robotic implantations and biological interfaces of prosthetic devices have been offered in the collected works [173]. As compared to the existing control methods, the sEMG interface delivers numerous advantages to user. The indirect and close communication, individuality of handy supervisory devices, and no requirement of straight eye contact or profound user attentiveness are some of the advantages offered by sEMG interfaces which make them apt for prostheses control. However, the sEMG interfaces suffer from a number of challenges [174,175,176,177,178,179,180].
Some other important challenges have been listed below:
-
The power-weight ratio of multifunctional prostheses is a significant challenge in their design. Due to the heaviness and bulkiness of the actuation and control system [181] associated with the state-of-the-art non-prosthetic mechanical hands with 20 DOF, they cannot be used as prostheses in realistic applications. The realization of greater number of DOFs require sensor placement at highly complex sites which is difficult and burdensome [182].
-
Relevant to the fabrication and assemblage of interfaces linked with sEMG signals, the maintenance of high classification accuracy poses a major challenge for long-term use.
-
Due to the muscular contractions performed under several conditions, variations in signal properties may occur which may make them unrecognizable for the classifier. The variations in EMG signal due to the influence of limb orientation [183] as well as socket loading effects, fluctuations in muscle contraction [184] and electrode shifts [178] (due to donning, doffing, usage) may affect the performance of the classifier.
Researchers and technical minds working in the arena of ULP aim towards the development of simultaneous, autonomous, and proportional control of multiple DOFs with adequate enactment along with proximate standard governing intricacy and response time [185]. Other prime challenges encountered in the prostheses design are the electromechanical application, utilization of sEMG control signals and the synergy amongst robotic and clinical groups [186].
4.1 Limitations
There are some limitations to this review. We excluded an in-depth discussion of many of the main topics that were brought up in the text. For instance, a discussion of the following topics (in substantiative depth) was excluded from this review: pattern recognition approaches, sEMG features and their extraction modes; types of EMG features used to drive the classification algorithms, etc. Moreover, one conducted a literature search in some well-known electronic databases. However, this review might be missing additional relevant studies, as was the "gray" literature.
5 Conclusions and outlook for future research
This review presented an overview of the state-of-the-art applications of sEMG in prostheses and an exploratory analysis of the essential elements in sEMG-based prosthesis research [187, 188]. Moreover, the challenges and future trends associated with sEMG interfaces were also discussed. Some of the essential aspects of sEMG-based prosthesis applications were also highlighted. In a nutshell, this review offers a platform to researchers for facilitating the design and applications of sEMG-based prosthetic devices. Owing to the provision of an entirely new mode of communication, sEMG interface opens the prospective gateway to widespread human–device collaboration. This review points out that sEMG plays a noteworthy role in prostheses on account of its practicability and non-invasiveness. It is believed that in the forthcoming years, our entire limbs can be replaced with prosthetics which has the ability to accurately imitate the biological functions and requires minimal maintenance. However, further explorations are necessary in the direction of making a seamless mechanism of bio mechatronics for sEMG-based prosthesis by cohesive efforts of robotic researchers and biomedical engineers. These robotic researchers and biomedical engineers are required to work together holistically and synergistically to create marvels in the domain of sEMG-based prostheses control. As a final note, we believe that the critical recommendations and our perspective would spark a dialogue among researcher—about further advancements for excellent sEMG-based prosthesis applications—and, therefore, help in improving the quality of life of amputees.
6 Ethics approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Notes
Triwiyanto, T., Caesarendra, W., Purnomo, M.H., Sułowicz, M., Wisana, I.D.G.H., Titisari, D., Lamidi, L. and Rismayani, R., 2022. Embedded machine learning using a multi-thread algorithm on a Raspberry Pi platform to improve prosthetic hand performance. Micromachines, 13(2), p.191.
Burhan, N., & Ghazali, R. (2016, October). Feature extraction of surface electromyography (sEMG) and signal processing technique in wavelet transform: A review. In 2016 IEEE International Conference on Automatic Control and Intelligent Systems (I2CACIS) (pp. 141–146). IEEE.
References
Hoozemans MJM, van Dieën JH. Prediction of handgrip forces using surface EMG of forearm muscles. J Electromyogr Kinesiol. 2005;15(4):358–66. https://doi.org/10.1016/j.jelekin.2004.09.001.
Bilodeau M, Schindler-Ivens S, Williams DM, Chandran R, Sharma SS. EMG frequency content changes with increasing force and during fatigue in the quadriceps femoris muscle of men and women. J Electromyogr Kinesiol. 2003;13(1):83–92. https://doi.org/10.1016/S1050-6411(02)00050-0.
Reiter R. Eine neue elektrokunsthand. Grenzgeb Med. 1948;1(4):133–5.
Kobrinski AE, et al. Problems of bioelectric control. IFAC Proc Vol. 1960;1(1):629–33. https://doi.org/10.1016/s1474-6670(17)70141-3.
Ajiboye AB, Weir RFF. A heuristic fuzzy logic approach to EMG pattern recognition for multifunctional prosthesis control. IEEE Trans Neural Syst Rehabil Eng. 2005;13(3):280–91. https://doi.org/10.1109/TNSRE.2005.847357.
Huang CN, Chen CH, Chung HY. Application of facial electromyography in computer mouse access for people with disabilities. Disabil Rehabil. 2006;28(4):231–7. https://doi.org/10.1080/09638280500158349.
Ferris DP, Lewis CL. “Robotic lower limb exoskeletons using proportional myoelectric control,” In: Proceedings of the 31st Annual International Conference of the IEEE Engineering in Medicine and Biology Society: Engineering the Future of Biomedicine, EMBC 2009, 2009, pp. 2119–2124. https://doi.org/10.1109/IEMBS.2009.5333984.
Micera S, Carpaneto J, Raspopovic S. Control of hand prostheses using peripheral information. IEEE Rev Biomed Eng. 2010;3:48–68. https://doi.org/10.1109/RBME.2010.2085429.
Moon I, Lee M, Chu J, Mun M. Wearable EMG-based HCI for electric-powered wheelchair users with motor disabilities. Proc IEEE Int Conf Robot Autom. 2005;2005:2649–54. https://doi.org/10.1109/ROBOT.2005.1570513.
Stepp CE. Surface electromyography for speech and swallowing systems: measurement, analysis, and interpretation. J Speech Lang Hear Res. 2012;55(4):1232–46. https://doi.org/10.1044/1092-4388(2011/11-0214).
Xing S, Zhang X. EMG-driven computer game for post-stroke rehabilitation, in 2010 IEEE Conference on Robotics, Automation and Mechatronics, RAM 2010, 2010, pp. 32–36. https://doi.org/10.1109/RAMECH.2010.5513218
Costanza E, Inverso SA, Allen R. “Toward subtle intimate interfaces for mobile devices using an EMG controller,” in Proceedings of the SIGCHI conference on Human factors in computing systems - CHI ’05, 2005, p. 481. https://doi.org/10.1145/1054972.1055039
Costanza E, Inverso SA, Allen R, Maes P. “Intimate interfaces in action: Assessing the usability and subtlety of emg-based motionless gestures,” in Conference on Human Factors in Computing Systems - Proceedings, 2007, pp. 819–828. https://doi.org/10.1145/1240624.1240747
Costanza E, Perdomo A, Inverso SA, Allen RK. “EMG as a subtle input interface for mobile computing,” Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), vol. 3160, pp. 426–430, 2004, https://doi.org/10.1007/978-3-540-28637-0_50
Jorgensen C, Dusan S. Speech interfaces based upon surface electromyography. Speech Commun. 2010;52(4):354–66. https://doi.org/10.1016/j.specom.2009.11.003.
Saponas TS, Tan DS, Morris D, Balakrishnan R. “Demonstrating the feasibility of using forearm electromyography for muscle-computer interfaces,” in Conference on Human Factors in Computing Systems - Proceedings, 2008, pp. 515–524. https://doi.org/10.1145/1357054.1357138.
Saponas TS, Tan DS, Morris D, Turner J, Landay JA. Making muscle-computer interfaces more practical. Conf Human Factors Comput Syst Proc. 2010;2:851–4. https://doi.org/10.1145/1753326.1753451.
Jung JY, Park YK, Lee JW. “Wearable mobile phone using EMG and controlling method thereof,” 2009 Accessed: May 09, 2020. [Online]. Available: https://patents.google.com/patent/US7596393B2/en
Tan D, Saponas T, Morris D, Turner J. “Wearable electromyography-based controllers for human-computer interface,” 2012, https://doi.org/10.1145/1060000/1055039.
Farina D, Lorrain T, Negro F, Jiang N. “High-density EMG E-textile systems for the control of active prostheses,” in 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC’10, 2010, pp. 3591–3593. https://doi.org/10.1109/IEMBS.2010.5627455.
Finni T, Hu M, Kettunen P, Vilavuo T, Cheng S. Measurement of EMG activity with textile electrodes embedded into clothing. Physiol Meas. 2007;28(11):1405–19. https://doi.org/10.1088/0967-3334/28/11/007.
Kim S, Lee S, Jeong W. EMG measurement with textile-based electrodes in different electrode sizes and clothing pressures for smart clothing design optimization. Polymers. 2020. https://doi.org/10.3390/POLYM12102406.
McGuigan PM, Colyer SL. Textile electrodes embedded in clothing: a practical alternative to traditional surface electromyography when assessing muscle excitation during functional movements. J Sports Sci Med. 2018;17(1):101–9.
Barbero M, Merletti R, Rainoldi A. Atlas of muscle innervation zones: understanding surface electromyography and its applications. 2012. Accessed: May 09, 2020. [Online]. Available: https://books.google.co.in/books?hl=en&lr=&id=rWF-8HE9kf8C&oi=fnd&pg=PR3&dq=M.+Barbero,+R.+Merletti,+A.+Rainoldi,+Atlas+of+Muscle+Innervation+Zones,Springer-Verlag+Italia,+Milan,+Italy,+2012,+ISBN+978-88-470-2462-5.&ots=FCUrd-wU3J&sig=PkYuEBZrHs3g_GP60U3NA3FQ7xQ
Tenore FVG, Ramos A, Fahmy A, Acharya S, Etienne-Cummings R, Thakor NV. Decoding of individuated finger movements using surface electromyography. IEEE Trans Biomed Eng. 2009;56(5):1427–34. https://doi.org/10.1109/TBME.2008.2005485.
He H, Kiguchi K. “A study on EMG-based control of exoskeleton robots for human lower-limb motion assist,” in Proceedings of the IEEE/EMBS Region 8 International Conference on Information Technology Applications in Biomedicine, ITAB, 2007, pp. 292–295. doi: https://doi.org/10.1109/ITAB.2007.4407405
Jou SC, Maier-Hein L, Schultz T, Waibel A. “Articulatory feature classification using surface electromyography,” in ICASSP, IEEE International Conference on Acoustics, Speech and Signal ProcessingProceedings, 2006, vol. 1. https://doi.org/10.1109/icassp.2006.1660093
Sugie N, Tsunoda K. A speech prosthesis employing a speech synthesizer—vowel discrimination from perioral muscle activities and vowel production. IEEE Trans Biomed Eng. 1985. https://doi.org/10.1109/TBME.1985.325564.
Wand M, Schultz T. “Analysis of phone confusion in EMG-based speech recognition,” in ICASSP, IEEE International Conference on Acoustics, Speech and Signal Processing—Proceedings, 2011, pp. 757–760. https://doi.org/10.1109/ICASSP.2011.5946514
Sebelius FCP, Rosén BN, Lundborg GN. Refined myoelectric control in below-elbow amputees using artificial neural networks and a data glove. J Hand Surg. 2005;30(4):780–9. https://doi.org/10.1016/j.jhsa.2005.01.002.
Li G, Schultz AE, Kuiken TA. Quantifying pattern recognition-based myoelectric control of multifunctional transradial prostheses. IEEE Trans Neural Syst Rehabil Eng. 2010;18(2):185–92. https://doi.org/10.1109/TNSRE.2009.2039619.
Oskoei MA, Hu H. Myoelectric control systems—a survey. Biomed Signal Process Control. 2007. https://doi.org/10.1016/j.bspc.2007.07.009.
Merletti R, Aventaggiato M, Botter A, Holobar A, Marateb H, Vieira TMM. Advances in surface EMG: recent progress in detection and processing techniques. Crit Rev Biomed Eng. 2010;38(4):305–45. https://doi.org/10.1615/CritRevBiomedEng.v38.i4.10.
Hakonen M, Piitulainen H, Visala A. Current state of digital signal processing in myoelectric interfaces and related applications. Biomed Signal Process Control. 2015. https://doi.org/10.1016/j.bspc.2015.02.009.
Hudgins B, Parker P, Scott RN. A new strategy for multifunction myoelectric control. IEEE Trans Biomed Eng. 1993;40(1):82–94. https://doi.org/10.1109/10.204774.
Farrell TR, Weir RF. The optimal controller delay for myoelectric prostheses. IEEE Trans Neural Syst Rehabil Eng. 2007;15(1):111–8. https://doi.org/10.1109/TNSRE.2007.891391.
Boostani R, Moradi M. Evaluation of the forearm EMG signal features for the control of a prosthetic hand. Physiol Meas. 2003. https://doi.org/10.1088/0967-3334/24/2/307.
Huang Y, Englehart KB, Hudgins B, Chan ADC. A gaussian mixture model based classification scheme for myoelectric control of powered upper limb prostheses. IEEE Trans Biomed Eng. 2005;52(11):1801–11. https://doi.org/10.1109/TBME.2005.856295.
Chan FHY, Yang YS, Lam FK, Zhang YT, Parker PA. Fuzzy EMG classification for prosthesis control. IEEE Trans Rehabil Eng. 2000;8(3):305–11. https://doi.org/10.1109/86.867872.
Fontana J. “Classification of EMG signals to control a prosthetic hand using time-frequesncy representations and Support Vector Machines,” Doctoral Dissertations, 2010, Accessed: May 10, 2020. [Online]. Available: https://digitalcommons.latech.edu/dissertations/401
Khezri M, Jahed M, Sadati N. “Neuro-fuzzy surface EMG pattern recognition for multifunctional hand prosthesis control,” in IEEE International Symposium on Industrial Electronics, 2007, pp. 269–274. https://doi.org/10.1109/ISIE.2007.4374610.
Chan ADC, Englehart KB. Continuous myoelectric control for powered prostheses using hidden Markov models. IEEE Trans Biomed Eng. 2005;52(1):121–4. https://doi.org/10.1109/TBME.2004.836492.
Carrozza MC et al. “On the development of a novel adaptive prosthetic hand with compliant joints: Experimental platform and EMG control,” in 2005 IEEE/RSJ International Conference on Intelligent Robots and Systems, IROS, 2005, pp. 3951–3956. https://doi.org/10.1109/IROS.2005.1545585.
Boschmann A, Platzner M, Robrecht M, Hahn M, Winkler M. “Development of a pattern recognition-based myoelectric transhumeral prosthesis with multifunctional simultaneous control using a model-driven approach for mechatronic systems. ,” in Proceedings of the MyoElectric Controls/Powered Prosthetics Symposium Fredericton, New Brunswick, Canada., Aug, 2011
Herle S, Raica P, Lazea G, Robotin R, Marcu C, Tamas L. “Classification of surface electromyographic signals for control of upper limb virtual prosthesis using time-domain features,” in 2008 IEEE International Conference on Automation, Quality and Testing, Robotics, AQTR 2008 - THETA 16th Edition—Proceedings, 2008, vol. 3, pp. 160–165. https://doi.org/10.1109/AQTR.2008.4588902.
Karlik B, Tokhi MO, Alci M. A fuzzy clustering neural network architecture for multifunction upper-limb prosthesis. IEEE Trans Biomed Eng. 2003;50(11):1255–61. https://doi.org/10.1109/TBME.2003.818469.
Tenore F, Ramos A, Fahmy V, Acharya S, Etienne-Cummings R, Thakor NV. “Towards the control of individual fingers of a prosthetic hand using surface EMG signals,” in Annual International Conference of the IEEE Engineering in Medicine and Biology–Proceedings, 2007, pp. 6145–6148.https://doi.org/10.1109/IEMBS.2007.4353752.
McMillan G. “The technology and applications of biopotential-based control,” RTO educational notes, 1998
Li G. “Electromyography pattern-recognition-based control of powered multifunctional upper-limb prostheses.” Adv Appl Electromyograph INTECH. 2011. https://doi.org/10.5772/22876.
Cordella F, et al. Literature review on needs of upper limb prosthesis users. Front Neurosci. 2016. https://doi.org/10.3389/fnins.2016.00209.
Mohd Zaini MH, Ahmad, “Su SA. Surgical and non-surgical prosthetic hands control: a review,” in 2011 IEEE Symposium on Industrial Electronics and Applications, ISIEA 2011, 2011, pp. 634–637, https://doi.org/10.1109/ISIEA.2011.6108792
Das N, Nagpal N, Bankura SS. A review on the advancements in the field of upper limb prosthesis. J Med Eng Technol. 2018. https://doi.org/10.1080/03091902.2019.1576793.
Geethanjali P. Myoelectric control of prosthetic hands: state-of-the-art review. Med Devices Evidence Res. 2016. https://doi.org/10.2147/MDER.S91102.
Madusanka DGK, Wijayasingha LNS, Gopura RARC, Amarasinghe YWR, Mann GK. “A review on hybrid myoelectric control systems for upper limb prosthesis,” in MERCon 2015 - Moratuwa Engineering Research Conference, May 2015, pp. 136–141. https://doi.org/10.1109/MERCon.2015.7112334
Veer K. Development of sensor system with measurement of surface electromyogram signal for clinical use. Optik (Stuttg). 2016;127(1):352–6. https://doi.org/10.1016/j.ijleo.2015.10.072.
Veer K. A flexible approach for segregating physiological signals. Measurement. 2016;87:21–6. https://doi.org/10.1016/j.measurement.2016.03.017.
Lazaro JB, Abuan DD, Linsangan NB, Panganiban AG. Surface electromyography signal for control of myoelectric prosthesis of the upper-limb using independent component analysis. J Autom Control Eng. 2014. https://doi.org/10.12720/joace.2.1.94-98.
Salem FHA, Mohamed KS, Mohamed SBK, el Gehani AA. “The development of body-powered prosthetic hand controlled by EMG signals using DSP processor with virtual prosthesis implementation,” in International Conference on Electrical and Computer Engineering, 2013, https://doi.org/10.1155/2013/598945
Castellini C, van der Smagt P. Surface EMG in advanced hand prosthetics. Biol Cybern. 2009;100(1):35–47. https://doi.org/10.1007/s00422-008-0278-1.
Tavakoli M, Benussi C, Lourenco JL. Single channel surface EMG control of advanced prosthetic hands: A simple, low cost and efficient approach. Expert Syst Appl. 2017;79:322–32. https://doi.org/10.1016/j.eswa.2017.03.012.
Brunelli D, Tadesse AM, Vodermayer B, Nowak M, Castellini C. “Low-cost wearable multichannel surface EMG acquisition for prosthetic hand control,” in Proceedings - 2015 6th IEEE International Workshop on Advances in Sensors and Interfaces, IWASI 2015, 2015, pp. 94–99. https://doi.org/10.1109/IWASI.2015.7184964.
Castellini C, Gruppioni E, Davalli A, Sandini G. Fine detection of grasp force and posture by amputees via surface electromyography. J Physiol Paris. 2009;103(3–5):255–62. https://doi.org/10.1016/j.jphysparis.2009.08.008.
Khushaba RN, Kodagoda S, Takruri M, Dissanayake G. Toward improved control of prosthetic fingers using surface electromyogram (EMG) signals. Expert Syst Appl. 2012;39(12):10731–8. https://doi.org/10.1016/j.eswa.2012.02.192.
Yatsenko D, McDonnall D, Shane Guillory K. “Simultaneous, proportional, multi-axis prosthesis control using multichannel surface EMG,” in Annual International Conference of the IEEE Engineering in Medicine and Biology–Proceedings, 2007, pp. 6133–6136. https://doi.org/10.1109/IEMBS.2007.4353749
Sturma A, et al. A surface EMG test tool to measure proportional prosthetic control. Biomed Tech. 2015;60(3):207–13. https://doi.org/10.1515/bmt-2014-0022.
Amsuss S, Paredes LP, Rudigkeit N, Graimann B, Herrmann MJ, Farina D. “Long term stability of surface EMG pattern classification for prosthetic control,” in Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, 2013, pp. 3622–3625. https://doi.org/10.1109/EMBC.2013.6610327.
Waris MA, Jamil M, Gilani SO. Classification of functional motions of hand for upper limb prosthesis with surface electromyography. Int J Biol Biomed Eng. 2020;8:15–20.
Atzori M, et al. Electromyography data for non-invasive naturally-controlled robotic hand prostheses. Sci Data. 2014;1(1):1–13. https://doi.org/10.1038/sdata.2014.53.
Tabakov M, Fonal K, Abd-Alhameed RA, Qahwaji R. “Fuzzy bionic hand control in real-time based on electromyography signal analysis,” in Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), 2016, vol. 9875 LNCS, pp. 292–302. https://doi.org/10.1007/978-3-319-45243-2_27.
Tabakov M, Fonal K, Abd-Alhameed RA, Qahwaji R. “Bionic hand control in real-time based on electromyography signal analysis,” in Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), vol. 10840 LNCS, Springer Verlag, 2018, pp. 21–38. https://doi.org/10.1007/978-3-319-90287-6_2
Wang N, Lao K, Zhang X. Design and myoelectric control of an anthropomorphic prosthetic hand. J Bionic Eng. 2017;14(1):47–59. https://doi.org/10.1016/S1672-6529(16)60377-3.
Sudarsan LS, Sekaran EC. Design and development of EMG controlled prosthetics limb. Proc Eng. 2012;38:3547–51. https://doi.org/10.1016/j.proeng.2012.06.409.
Andrade NA, Borges GA, Nascimento FADO, Romariz ARS, da Rocha AF. “A new biomechanical hand prosthesis controlled by surface electromyographic signals,” in Annual International Conference of the IEEE Engineering in Medicine and Biology–Proceedings, 2007, pp. 6141–6144. https://doi.org/10.1109/IEMBS.2007.4353751
Xu K, Guo W, Hua L, Sheng X, Zhu X. “A prosthetic arm based on EMG pattern recognition,” in 2016 IEEE International Conference on Robotics and Biomimetics, ROBIO 2016, 2016, pp. 1179–1184. https://doi.org/10.1109/ROBIO.2016.7866485.
Aranceta-Garza A, Lakany H, Conway BA. “An investigation into thumb rotation using high density surface electromyography of extrinsic hand muscles,” in Proceedings - 2013 IEEE International Conference on Systems, Man, and Cybernetics, SMC 2013, 2013, pp. 3751–3755. https://doi.org/10.1109/SMC.2013.639.
Chowdhury R, Reaz M, Ali M, Bakar A, Chellappan K, Chang T. Surface electromyography signal processing and classification techniques. Sensors. 2013;13(9):12431–66. https://doi.org/10.3390/s130912431.
Reaz MBI, Hussain MS, Mohd-Yasin F. Techniques of EMG signal analysis: detection, processing, classification and applications. Biol Proced Online. 2006;8(1):11–35. https://doi.org/10.1251/bpo115.
Du YC, Lin CH, Shyu LY, Chen T. Portable hand motion classifier for multi-channel surface electromyography recognition using grey relational analysis. Expert Syst Appl. 2010;37(6):4283–91. https://doi.org/10.1016/j.eswa.2009.11.072.
Alkan A, Günay M. Identification of EMG signals using discriminant analysis and SVM classifier. Expert Syst Appl. 2012;39(1):44–7. https://doi.org/10.1016/j.eswa.2011.06.043.
Moura KOA, Favieiro GW, Balbinot A. “Support vectors machine classification of surface electromyography for non-invasive naturally controlled hand prostheses,” in Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Oct. 2016, pp. 788–791. https://doi.org/10.1109/EMBC.2016.7590819
Veer K. A technique for classification and decomposition of muscle signal for control of myoelectric prostheses based on wavelet statistical classifier. Measurement. 2015;60:283–91. https://doi.org/10.1016/j.measurement.2014.10.023.
Veer K, Sharma T. A novel feature extraction for robust EMG pattern recognition. J Med Eng Technol. 2016;40(4):149–54. https://doi.org/10.3109/03091902.2016.1153739.
Wang R, Huang C, Li B. Neural network-based surface electromyography motion pattern classifier for the control of prostheses. Ann Int Conf IEEE Eng Med Biolo Proc. 1997;3:1275–7. https://doi.org/10.1109/iembs.1997.756607.
Sidek SN, Jalaludin NA, Shamsudin AU. Surface electromyography (sEMG)-based thumb-tip angle and force estimation using Artificial Neural Network for prosthetic thumb. Proc Eng. 2012;41:650–6. https://doi.org/10.1016/j.proeng.2012.07.225.
Bu N, Fukuda O, Tsuji T. EMG-based motion discrimination using a novel recurrent neural network. J Intell Inf Syst. 2003;21(2):113–26. https://doi.org/10.1023/A:1024706431807.
Hargrove LJ, Scheme EJ, Englehart KB, Hudgins BS. Multiple binary classifications via linear discriminant analysis for improved controllability of a powered prosthesis. IEEE Trans Neural Syst Rehabil Eng. 2010;18(1):49–57. https://doi.org/10.1109/TNSRE.2009.2039590.
Atzori M, Cognolato M, Müller H. Deep learning with convolutional neural networks applied to electromyography data: a resource for the classification of movements for prosthetic hands. Front Neurorobot. 2016. https://doi.org/10.3389/fnbot.2016.00009.
Young AJ, Smith LH, Rouse EJ, Hargrove LJ. Classification of simultaneous movements using surface EMG pattern recognition. IEEE Trans Biomed Eng. 2013;60(5):1250–8. https://doi.org/10.1109/TBME.2012.2232293.
Favieiro GW, Balbinot A. “Adaptive neuro-fuzzy logic analysis based on myoelectric signals for multifunction prosthesis control,” in Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, 2011, pp. 7888–7891. https://doi.org/10.1109/IEMBS.2011.6091945
Mane SM, Kambli RA, Kazi FS, Singh NM. Hand motion recognition from single channel surface EMG using wavelet & artificial neural network. Proc Comput Sci. 2015;49(1):58–65. https://doi.org/10.1016/j.procs.2015.04.227.
Resnik L, Huang HH, Winslow A, Crouch DL, Zhang F, Wolk N. Evaluation of EMG pattern recognition for upper limb prosthesis control: a case study in comparison with direct myoelectric control. J Neuroeng Rehabil. 2018;15(1):1–13. https://doi.org/10.1186/s12984-018-0361-3.
Krasoulis A, Vijayakumar S, Nazarpour K. Effect of user practice on prosthetic finger control with an intuitive myoelectric decoder. Front Neurosci. 2019;13:891. https://doi.org/10.3389/fnins.2019.00891.
Gini G, Arvetti M, Somlai I, Folgheraiter M. Acquisition and analysis of EMG signals to recognize multiple hand movements for prosthetic applications. Appl Bionics Biomech. 2012;9(2):145–55. https://doi.org/10.3233/ABB-2011-0024.
Li C, Li G, Jiang G, Chen D, Liu H. Surface EMG data aggregation processing for intelligent prosthetic action recognition. Neural Comput Appl. 2018. https://doi.org/10.1007/s00521-018-3909-z.
Kaur A, Agarwal R, Kumar A. Adaptive threshold method for peak detection of surface electromyography signal from around shoulder muscles. J Appl Stat. 2018;45(4):714–26. https://doi.org/10.1080/02664763.2017.1293624.
Cipriani C, Zaccone F, Micera S, Carrozza MC. On the shared control of an EMG-controlled prosthetic hand: Analysis of user-prosthesis interaction. IEEE Trans Rob. 2008;24(1):170–84. https://doi.org/10.1109/TRO.2007.910708.
Naik GR, Baker KG, Nguyen HT. Dependence independence measure for posterior and anterior EMG sensors used in simple and complex finger flexion movements: Evaluation using SDICA. IEEE J Biomed Health Inform. 2015;19(5):1689–96. https://doi.org/10.1109/JBHI.2014.2340397.
Hiraiwa A, Shimohara K, Tokunaga Y. EMG pattern analysis and classification by neural network. Proc IEEE Int Conf Syst Man Cybern. 1989;3:1113–5. https://doi.org/10.1109/icsmc.1989.71472.
Zhang Z, Yu X, Qian J. Classification of finger movements for prosthesis control with surface electromyography. Sens Mater. 2020;32(4):1523–32. https://doi.org/10.18494/SAM.2020.2652.
Doerschuk PC, Gustafson DE, Willsky AS. Upper extremity limb function discrimination using EMG signal analysis. IEEE Trans Biomed Eng. 1983. https://doi.org/10.1109/TBME.1983.325162.
Huang H, Zhou P, Li G, Kuiken TA. An analysis of EMG electrode configuration for targeted muscle reinnervation based neural machine interface. IEEE Trans Neural Syst Rehabil Eng. 2008;16(1):37–45. https://doi.org/10.1109/TNSRE.2007.910282.
Ju Z, Ouyang G, Wilamowska-Korsak M, Liu H. Surface EMG based hand manipulation identification via nonlinear feature extraction and classification. IEEE Sens J. 2013;13(9):3302–11. https://doi.org/10.1109/JSEN.2013.2259051.
Naik GR, Selvan SE, Gobbo M, Acharyya A, Nguyen HT. Principal component analysis applied to surface electromyography: a comprehensive review. IEEE Access. 2016. https://doi.org/10.1109/ACCESS.2016.2593013.
Matrone GC, Cipriani C, Secco EL, Magenes G, Carrozza MC. Principal components analysis based control of a multi-dof underactuated prosthetic hand. J Neuroeng Rehabil. 2010;7(1):16. https://doi.org/10.1186/1743-0003-7-16.
Matrone GC, Cipriani C, Carrozza MC, Magenes G. Real-time myoelectric control of a multi-fingered hand prosthesis using principal components analysis. J Neuroeng Rehabil. 2012;9(1):40. https://doi.org/10.1186/1743-0003-9-40.
Segil JL, Weir RFF. Design and validation of a morphing myoelectric hand posture controller based on principal component analysis of human grasping. IEEE Trans Neural Syst Rehabil Eng. 2014;22(2):249–57. https://doi.org/10.1109/TNSRE.2013.2260172.
Hargrove LJ, Li G, Englehart KB, Hudgins BS. Principal components analysis preprocessing for improved classification accuracies in pattern-recognition-based myoelectric control. IEEE Trans Biomed Eng. 2009;56(5):1407–14. https://doi.org/10.1109/TBME.2008.2008171.
Raj R, Ramakrishna R, Sivanandan KS. A real time surface electromyography signal driven prosthetic hand model using PID controlled DC motor. Biomed Eng Lett. 2016;6(4):276–86. https://doi.org/10.1007/s13534-016-0240-4.
Khokhar ZO, Xiao ZG, Menon C. Surface EMG pattern recognition for real-time control of a wrist exoskeleton. Biomed Eng Online. 2010;9(1):1–17. https://doi.org/10.1186/1475-925X-9-41.
Choi C, Kim J. Synergy matrices to estimate fluid wrist movements by surface electromyography. Med Eng Phys. 2011;33(8):916–23. https://doi.org/10.1016/j.medengphy.2011.02.006.
Al-Timemy AH, Bugmann G, Escudero J, Outram N. Classification of finger movements for the dexterous hand prosthesis control with surface electromyography. IEEE J Biomed Health Inform. 2013;17(3):608–18. https://doi.org/10.1109/JBHI.2013.2249590.
Shenoy P, Miller KJ, Crawford B, Rao RPN. Online electromyographic control of a robotic prosthesis. IEEE Trans Biomed Eng. 2008;55(3):1128–35. https://doi.org/10.1109/TBME.2007.909536.
Lee S, Kim MO, Kang T, Park J, Choi Y. Knit Band sensor for myoelectric control of surface EMG-based prosthetic hand. IEEE Sens J. 2018;18(20):8578–86. https://doi.org/10.1109/JSEN.2018.2865623.
Amsuss S, Goebel PM, Jiang N, Graimann B, Paredes L, Farina D. Self-correcting pattern recognition system of surface EMG signals for upper limb prosthesis control. IEEE Trans Biomed Eng. 2014;61(4):1167–76. https://doi.org/10.1109/TBME.2013.2296274.
Jiang N, Englehart KB, Parker PA. Extracting simultaneous and proportional neural control information for multiple-dof prostheses from the surface electromyographic signal. IEEE Trans Biomed Eng. 2009;56(4):1070–80. https://doi.org/10.1109/TBME.2008.2007967.
Mostafa SS, Ahmad M, Awal MA. “Clench force estimation by surface electromyography for neural prosthesis hand,” in 2012 International Conference on Informatics, Electronics and Vision, ICIEV 2012, 2012, pp. 505–510. doi: https://doi.org/10.1109/ICIEV.2012.6317489
Gijsberts A, et al. Stable myoelectric control of a hand prosthesis using non-linear incremental learning. Front Neurorobot. 2014. https://doi.org/10.3389/fnbot.2014.00008.
Li G, Li J, Ju Z, Sun Y, Kong J. A novel feature extraction method for machine learning based on surface electromyography from healthy brain. Neural Comput Appl. 2019;31(12):9013–22. https://doi.org/10.1007/s00521-019-04147-3.
Strazzulla I, Nowak M, Controzzi M, Cipriani C, Castellini C. Online bimanual manipulation using surface electromyography and incremental learning. IEEE Trans Neural Syst Rehabil Eng. 2017;25(3):227–34. https://doi.org/10.1109/TNSRE.2016.2554884.
Brunelli D, Farella E, Giovanelli D, Milosevic B, Minakov I. Design considerations for wireless acquisition of multichannel sEMG signals in prosthetic hand control. IEEE Sens J. 2016. https://doi.org/10.1109/jsen.2016.2596712.
Jiang YL, Sakoda S, Togane M, Morishita S, Yokoi H. “One-handed wearable sEMG sensor for myoelectric control of prosthetic hands,” in Lecture Notes in Electrical Engineering, 2017, vol. 399, pp. 105–109https://doi.org/10.1007/978-981-10-2404-7_9
Stepp CE, Heaton JT, Rolland RG, Hillman RE. Neck and face surface electromyography for prosthetic voice control after total laryngectomy. IEEE Trans Neural Syst Rehabil Eng. 2009;17(2):146–55. https://doi.org/10.1109/TNSRE.2009.2017805.
Farina D, et al. The extraction of neural information from the surface EMG for the control of upper-limb prostheses: emerging avenues and challenges. IEEE Trans Neural Syst Rehabil Eng. 2014;22(4):797–809. https://doi.org/10.1109/TNSRE.2014.2305111.
Shahzad W, Ayaz Y, Khan MJ, Naseer N, Khan M. Enhanced Performance for multi-forearm movement decoding using hybrid IMU–sEMG interface. Front Neurorobot. 2019. https://doi.org/10.3389/FNBOT.2019.00043.
Chang W, Dai L, Sheng S, Tan JTC, Zhu C, Duan F. “A hierarchical hand motions recognition method based on IMU and sEMG sensors,” 2015 IEEE International Conference on Robotics and Biomimetics, IEEE-ROBIO 2015, pp. 1024–1029, 2015, https://doi.org/10.1109/ROBIO.2015.7418906
Krasoulis A, Vijayakumar S, Nazarpour K. Multi-grip classification-based prosthesis control with Two EMG-IMU sensors. IEEE Trans Neural Syst Rehabil Eng. 2020;28(2):508–18. https://doi.org/10.1109/TNSRE.2019.2959243.
Lauretti C, Davalli A, Sacchetti R, Guglielmelli E, Zollo L. “Fusion of M-IMU and EMG signals for the control of trans-humeral prostheses,” Proceedings of the IEEE RAS and EMBS International Conference on Biomedical Robotics and Biomechatronics, vol. 2016, pp. 1123–1128, 2016, doi: https://doi.org/10.1109/BIOROB.2016.7523782
Ganesan Y, Gobee S, Durairajah V. Development of an upper limb exoskeleton for rehabilitation with feedback from EMG and IMU sensor. Proc Comput Sci. 2015;76:53–9. https://doi.org/10.1016/J.PROCS.2015.12.275.
Bennett DA, Goldfarb M. IMU-based wrist rotation control of a transradial myoelectric prosthesis. IEEE Trans Neural Syst Rehabil Eng. 2018;26(2):419–27. https://doi.org/10.1109/TNSRE.2017.2682642.
Goldfarb M, Lawson BE, Shultz AH. Realizing the promise of robotic leg prostheses. Sci Transl Med. 2013. https://doi.org/10.1126/scitranslmed.3007312.
Tucker MR, et al. Control strategies for active lower extremity prosthetics and orthotics: a review. J NeuroEng Rehabil. 2015. https://doi.org/10.1186/1743-0003-12-1.
Windrich M, Grimmer M, Christ O, Rinderknecht S, Beckerle P. Active lower limb prosthetics: a systematic review of design issues and solutions. BioMed Eng. 2016. https://doi.org/10.1186/s12938-016-0284-9.
Johansson JL, Sherrill DM, Riley PO, Bonato P, Herr H. A clinical comparison of variable-damping and mechanically passive prosthetic knee devices. Am J Phys Med Rehabil. 2005;84(8):563–75. https://doi.org/10.1097/01.phm.0000174665.74933.0b.
Singh LH, Singh T, Singh LD, Singh T, Madde S, Rathod S. “Development of low cost prosthetic limb using EMG signals for amputees,” in 11th International Conference on Industrial and Information Systems, ICIIS 2016 - Conference Proceedings, pp. 742–745. doi: https://doi.org/10.1109/ICIINFS.2016.8263036.
Cadena F, Sanipatin J, Verdezoto G, Cervantes H, Ortiz D, Ojeda D. “Acquisition and Conditioning of Electromyographic Signals for Prosthetic Legs,” in Proceedings–2015 Asia-Pacific Conference on Computer-Aided System Engineering, APCASE 2015, 2015, pp. 360–365. https://doi.org/10.1109/APCASE.2015.70.
Geng Y, Xu X, Chen L, Yang P. “Design and analysis of active transfemoral prosthesis,” in IECON Proceedings (Industrial Electronics Conference), 2010, pp. 1495–1499. https://doi.org/10.1109/IECON.2010.5675461.
Huang H, Kuiken TA, Lipschutz RD. A strategy for identifying locomotion modes using surface electromyography. IEEE Trans Biomed Eng. 2009;56(1):65–73. https://doi.org/10.1109/TBME.2008.2003293.
Hefferman GM, Zhang F, Nunnery MJ, Huang H. Integration of surface electromyographic sensors with the transfemoral amputee socket: a comparison of four differing configurations. Prosthet Orthot Int. 2015;39(2):166–73. https://doi.org/10.1177/0309364613516484.
Jiménez-Fabián R, Verlinden O. Review of control algorithms for robotic ankle systems in lower-limb orthoses, prostheses, and exoskeletons. Med Eng Phys. 2012. https://doi.org/10.1016/j.medengphy.2011.11.018.
Au SK, Bonato P, Herr H. “An EMG-position controlled system for an active ankle-foot prosthesis: An initial experimental study,” in Proceedings of the 2005 IEEE 9th International Conference on Rehabilitation Robotics, 2005, vol. 2005, pp. 375–379. https://doi.org/10.1109/ICORR.2005.1501123
Au S, Berniker M, Herr H. Powered ankle-foot prosthesis to assist level-ground and stair-descent gaits. Neural Netw. 2008;21(4):654–66. https://doi.org/10.1016/j.neunet.2008.03.006.
Kawamoto H, Sankai Y. “Power assist system HAL-3 for gait disorder person,” in Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics), 2002, vol. 2398, pp. 196–203https://doi.org/10.1007/3-540-45491-8_43
Kawamoto H, Lee S, Kanbe S, Sankai Y. Power assist method for HAL-3 using EMG-based feedback controller. Proc IEEE Int Conf Syst Man Cybern. 2003;2:1648–53. https://doi.org/10.1109/icsmc.2003.1244649.
Kawamoto H, Kanbe S, Sankai Y. “Power assist method for HAL-3 estimating operator’s intention based on motion information,” in Proceedings - IEEE International Workshop on Robot and Human Interactive Communication, 2003, pp. 67–72. https://doi.org/10.1109/ROMAN.2003.1251800
Kawamoto H. et al., “Voluntary motion support control of Robot Suit HAL triggered by bioelectrical signal for hemiplegia,” in 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC’10, 2010, pp. 462–466. https://doi.org/10.1109/IEMBS.2010.5626191.
Lee S, Sankai Y. Power assist control for walking aid with HAL-3 based on EMG and impedance adjustment around knee joint. IEEE Int Conf Intell Robots Syst. 2002;2:1499–504. https://doi.org/10.1109/irds.2002.1043967.
Ha KH, Varol HA, Goldfarb M. Volitional control of a prosthetic knee using surface electromyography. IEEE Trans Biomed Eng. 2011;58(1):144–51. https://doi.org/10.1109/TBME.2010.2070840.
Jin D, Yang J, Zhang R, Wang R, Zhang J. Terrain identification for prosthetic knees based on electromyographic signal features. Tsinghua Sci Technol. 2006;11:74–9.
Atri R, et al. Smart data-driven optimization of powered prosthetic ankles using surface electromyography. Sensors. 2018;18(8):2705. https://doi.org/10.3390/s18082705.
Garikayi T, van den Heever D, Matope S. Analysis of surface electromyography signal features on osteomyoplastic transtibial amputees for pattern recognition control architectures. Biomed Signal Process Control. 2018;40:10–22. https://doi.org/10.1016/j.bspc.2017.09.007.
Chen B, Wang Q, Wang L. “Promise of using surface EMG signals to volitionally control ankle joint position for powered transtibial prostheses,” in 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC 2014, Nov. 2014, pp. 2545–2548. https://doi.org/10.1109/EMBC.2014.6944141
Seyedali M, Czerniecki JM, Morgenroth DC, Hahn ME. Co-contraction patterns of trans-tibial amputee ankle and knee musculature during gait. J Neuroeng Rehabil. 2012;9(1):1–9. https://doi.org/10.1186/1743-0003-9-29.
Chen L, Yang P, Zu L, Guo X. “Movement recognition by electromyography signal for transfemoral prosthesis control,” in 2009 4th IEEE Conference on Industrial Electronics and Applications, ICIEA 2009, 2009, pp. 1127–1132. https://doi.org/10.1109/ICIEA.2009.5138333
Young AJ, Kuiken TA, Hargrove LJ. Analysis of using EMG and mechanical sensors to enhance intent recognition in powered lower limb prostheses. J Neural Eng. 2014. https://doi.org/10.1088/1741-2560/11/5/056021.
Fleming A, Stafford N, Huang S, Hu X, Ferris DP, Huang HH. Myoelectric control of robotic lower limb prostheses: a review of electromyography interfaces, control paradigms, challenges and future directions. J Neural Eng. 2021. https://doi.org/10.1088/1741-2552/AC1176.
Huang H, Zhang F, Hargrove LJ, Dou Z, Rogers DR, Englehart KB. Continuous locomotion-mode identification for prosthetic legs based on neuromuscular–mechanical fusion. IEEE Trans Biomed Eng. 2011. https://doi.org/10.1109/TBME.2011.2161671.
Sawicki GS, Ferris DP. Mechanics and energetics of level walking with powered ankle exoskeletons. J Exp Biol. 2008;205(21):3413–22. https://doi.org/10.1242/jeb.009241.
Wang X, Yang S, Cao Y, Ding Y, Zhang Z. “The real time motion pattern recognition of lower limb based on sEMG signals,” in Proceedings of 2020 IEEE International Conference on Information Technology, Big Data and Artificial Intelligence, ICIBA 2020, pp. 407–411, Nov. 2020, https://doi.org/10.1109/ICIBA50161.2020.9277504
Kust SY, Markova MV. “An algorithm for determination of terrain type in the lower limb prosthesis control,” in Proceedings - 2021 Ural Symposium on Biomedical Engineering, Radioelectronics and Information Technology, USBEREIT 2021, pp. 145–148, 2021, https://doi.org/10.1109/USBEREIT51232.2021.9455119.
Ding Z, Yang C, Wang Z, Yin X, Jiang F. Online adaptive prediction of human motion intention based on sEMG. Sensors. 2021. https://doi.org/10.3390/S21082882.
Khiabani H, Ahmadi M. “A classical machine learning approach for emg-based lower limb intention detection for human-robot interaction systems,”in 2021 IEEE International Conference on Autonomous Systems (ICAS), pp. 1–5, 2021, https://doi.org/10.1109/ICAS49788.2021.9551190
Keleş AD, Yucesoy CA. Development of a neural network based control algorithm for powered ankle prosthesis. J Biomech. 2020. https://doi.org/10.1016/J.JBIOMECH.2020.110087.
Cimolato A, Milandri G, Mattos LS, de Momi E, Laffranchi M, de Michieli L. “Hybrid machine learning-neuromusculoskeletal modeling for control of lower limb prosthetics,” in Proceedings of the IEEE RAS and EMBS International Conference on Biomedical Robotics and Biomechatronics, vol. 2020, pp. 557–563, 2020, https://doi.org/10.1109/BIOROB49111.2020.9224448.
Spanias JA, Simon AM, Finucane SB, Perreault EJ, Hargrove LJ. Online adaptive neural control of a robotic lower limb prosthesis. J Neural Eng. 2018. https://doi.org/10.1088/1741-2552/AA92A8.
Torrealba RR, Fernández-López G, Grieco JC. Towards the development of knee prostheses: review of current researches. Kybernetes. 2008;37(9–10):1561–76. https://doi.org/10.1108/03684920810907869.
Bai O, Atri R, Marquez JS, Fei DY. “Characterization of lower limb activity during gait using wearable, multi-channel surface EMG and IMU sensors,” in 2017 International Electrical Engineering Congress, iEECON 2017, 2017, https://doi.org/10.1109/IEECON.2017.8075872.
Su BY, Wang J, Liu SQ, Sheng M, Jiang J, Xiang K. A cnn-based method for intent recognition using inertial measurement units and intelligent lower limb prosthesis. IEEE Trans Neural Syst Rehabil Eng. 2019;27(5):1032–42. https://doi.org/10.1109/TNSRE.2019.2909585.
Ryu J, Lee BH, Maeng J, Kim DH. sEMG-signal and IMU sensor-based gait sub-phase detection and prediction using a user-adaptive classifier. Med Eng Phys. 2019;69:50–7. https://doi.org/10.1016/J.MEDENGPHY.2019.05.006.
Lu Y, Wang H, Hu F, Zhou B, Xi H. Effective recognition of human lower limb jump locomotion phases based on multi-sensor information fusion and machine learning. Med Biol Eng Comput. 2021. https://doi.org/10.1007/S11517-021-02335-9.
Xu D, Wang Q. On-board Training Strategy for IMU-Based Real-Time Locomotion Recognition of Transtibial Amputees With Robotic Prostheses. Front Neurorobot. 2020. https://doi.org/10.3389/FNBOT.2020.00047.
Negi S, Sharma S, Sharma N. FSR and IMU sensors-based human gait phase detection and its correlation with EMG signal for different terrain walk. Sens Rev. 2021;41(3):235–45. https://doi.org/10.1108/SR-10-2020-0249.
Peng F, Zhang C, Xu B, Li J, Wang Z, Su H. Locomotion prediction for lower limb prostheses in complex environments via sEMG and inertial sensors. Complexity. 2020. https://doi.org/10.1155/2020/8810663.
Lai JCK, Schoen MP, Gracia AP, Naidu DS, Leung SW. Prosthetic devices: challenges and implications of robotic implants and biological interfaces. Proc Inst Mech Eng H. 2007;221(2):173–83. https://doi.org/10.1243/09544119JEIM210.
Parajuli N, et al. Real-time EMG based pattern recognition control for hand prostheses: a review on existing methods, challenges and future implementation. Sensors. 2019;19(20):4596. https://doi.org/10.3390/s19204596.
González-Fernández M. Development of upper limb prostheses: current progress and areas for growth. Arch Phys Med Rehabil. 2014. https://doi.org/10.1016/j.apmr.2013.11.021.
Pasquina PF, Perry BN, Miller ME, Ling GSF, Tsao JW. Recent advances in bioelectric prostheses. Neurol Clin Pract. 2015;5(2):164–70. https://doi.org/10.1212/CPJ.0000000000000132.
Samuel OW, et al. Intelligent EMG pattern recognition control method for upper-limb multifunctional prostheses: advances, current challenges, and future prospects. IEEE Access. 2019;7:10150–65. https://doi.org/10.1109/ACCESS.2019.2891350.
Hargrove L, Englehart K, Hudgins B. “The effect of electrode displacements on pattern recognition based myoelectric control,” in Annual International Conference of the IEEE Engineering in Medicine and Biology–Proceedings, 2006, pp. 2203–2206. https://doi.org/10.1109/IEMBS.2006.260681
Samuel OW, et al. Resolving the adverse impact of mobility on myoelectric pattern recognition in upper-limb multifunctional prostheses. Comput Biol Med. 2017;90:76–87. https://doi.org/10.1016/j.compbiomed.2017.09.013.
Scheme E, Englehart K. Electromyogram pattern recognition for control of powered upper-limb prostheses: State of the art and challenges for clinical use. J Rehabil Res Dev. 2011;48(6):643–60. https://doi.org/10.1682/JRRD.2010.09.0177.
Butterfass J, Grebenstein M, Liu H, Hirzinger G. DLR-Hand II: Next generation of a dextrous robot hand. Proc IEEE Int Conf Robotics Autom. 2001;1:109–14. https://doi.org/10.1109/robot.2001.932538.
Zahak M. “Signal Acquisition using surface emg and circuit design considerations for robotic prosthesis,” in Computational Intelligence in Electromyography Analysis - A Perspective on Current Applications and Future Challenges, InTech,https://doi.org/10.5772/52556
Scheme E, Fougner A, Stavdahl AD, Chan C, Englehart K. “Examining the adverse effects of limb position on pattern recognition based myoelectric control,” in 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC’10, 2010, pp. 6337–6340. https://doi.org/10.1109/IEMBS.2010.5627638
Tkach D, Huang H, Kuiken TA. Study of stability of time-domain features for electromyographic pattern recognition. J Neuroeng Rehabil. 2010;7(1):1–13. https://doi.org/10.1186/1743-0003-7-21.
Edeer D, Martin C. “Upper limb prostheses: a review of the literature: with a focus on myoelectric hands,” in WorkSafeBC, Evidence-Based Practice Group, 2011
Dellon B, Matsuoka Y. Prosthetics, exoskeletons, and rehabilitation [grand challenges of robotics]. IEEE Robot Autom Mag. 2007;14(1):30–4. https://doi.org/10.1109/MRA.2007.339622.
Castellini C, et al. Proceedings of the first workshop on peripheral machine interfaces: Going beyond traditional surface electromyography. Front Neurorobot. 2014;8:22. https://doi.org/10.3389/fnbot.2014.00022.
Yadav D, Yadav S, Veer K. A comprehensive assessment of brain computer interfaces: recent trends and challenges. J Neurosci Methods. 2020;346:108918. https://doi.org/10.1016/j.jneumeth.2020.108918.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by DY. The first draft of the manuscript was written by DY and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yadav, D., Veer, K. Recent trends and challenges of surface electromyography in prosthetic applications. Biomed. Eng. Lett. 13, 353–373 (2023). https://doi.org/10.1007/s13534-023-00281-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13534-023-00281-z