
Abstract
This study was designed to find the correlation of iron indices with HbA1c levels and microvascular complications among patients with type 2 DM. Results were consistent with our hypothesis that high iron indices (serum iron and serum ferritin) not high enough to cause hemochromatosis but were still associated with poor glycemic control and its complications. The mean age of study group was 58.57 ± 3.17 years; whereas, the mean age of control group was 53.95 ± 4.43. The mean HbA1c of study group was 9.46 ± 1.31; whereas, the mean HbA1c of control group was 6.42 ± 0.28. The duration of diabetes in study group was 9.69 ± 2.69 years; whereas, it is 5.26 ± 2.81 years in control group. The mean serum iron level in study group was 155.08 ± 22.13 μg/dl; whereas, it is 88.81 ± 38.04 μg/dl in control group. The mean serum ferritin level in study group was 284.79 ± 50.06 ng/ml; whereas, it is 181.31 ± 54.08 ng/ml in control group. The mean serum transferrin saturation in study group was 30.25 ± 9.94; whereas, it is 28.92 ± 6.03 in control group. Out of the 100 patients in the study group, 40 patients had nephropathy, 33 patients had retinopathy, and 31 patients had neuropathy. In 100 patients in the control group, 12 patients had nephropathy, 11 patients had retinopathy, and 12 patients had neuropathy. On applying Pearson’s coefficient of correlation, a moderately significant correlation was obtained between serum iron, ferritin, and HbA1c in study group. However, no significant correlation was obtained with transferrin saturation. On applying regression analysis among HbA1c, serum ferritin, and serum iron, it was observed (the sum of squares of the group was 30.5) that variation is not due to chance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
We have come a long way as far as our understanding about pathophysiology of type 2 diabetes is concerned from the core defects of impaired insulin secretion from β cells of pancreas and increasing peripheral insulin resistance to De Fronzo’s famous ominous octet [1] and further to “Dirty Dozen” [2] involving a delayed incretin response from the gut, increased glucagon production from the α cells as well as insulin resistance in the brain and increased glucose reabsorption in the kidneys all playing a crucial role in worsening of hyperglycemia.
The fact that the frequency of diabetes is increased in classic hereditary hemochromatosis gives us the clue that systemic iron overload could contribute to abnormal glucose metabolism [3].
The contribution of iron in the pathogenesis of diabetes is suggested by the following: (1) diverse causes of iron overload have been found to be associated with an increased incidence of type 2 diabetes and (2) improvement in glycemic burden with a reduction in iron load was achieved using either phlebotomy or iron chelation therapy.
It is recognized recently that increased body stores of iron have association with the development of insulin resistance syndrome, glucose intolerance, gestational diabetes, and type 2 DM [4,5,6,7,8]. Reduction in iron stores by repeated blood donations leads to decrease in postprandial hyperinsulinemia and improvement in insulin sensitivity [9]. Phlebotomy leads to fall in serum glucose, cholesterol, triglycerides, and improvement in both beta cell secretion as well as peripheral insulin action in type 2 DM [10, 11]. Epidemiological studies also suggest the same correlation [12, 13]
Recent in vitro studies have shown that H-ferritin mRNA is four- to eightfold higher in rat islets treated with 20 mmol/l glucose than in islets treated with 1 mmol/l glucose [14]. The fact that beta cells are particularly sensitive to oxygen radicals and ferritin has some potential to exhibit antioxidant properties explains increased levels of ferritin in beta cells [15].
Study patients of DM have hyperferritinemia which co-relates with diabetic retinopathy, diabetic nephropathy, and vascular dysfunction [16,17,18]. It is important to realize that raised levels of iron above physiological requirement do not seem to serve any useful purpose in these patients. Although few indirect evidences from the western region do suggest that iron overload influences DM in a negative way, but overall there is paucity of literature especially from our country showing any direct evidence between increased iron load and control of diabetes mellitus. Moreover, finding out such correlation in Indian population carries great clinical significance as anemia has very high prevalence in Indian population, and continuous efforts are being made at physician, community, and government level to prevent and treat anemia which might influence the coexisting diabetic state. Hence, the present comprehensive study was planned to find out the relationship between iron indices (serum iron, serum ferritin, and transferrin saturation) with HbA1c in type 2 DM and to study the influence of body iron stores on diabetic microvascular complications in patients coming to OPD and IPD of our hospital.
Aims and objectives
-
1.
To study the correlation between serum ferritin, serum free iron, and transferrin saturation with HbA1c in patients of type 2 diabetes mellitus
-
2.
To study the correlation between serum ferritin, serum free iron, and transferrin saturation with microvascular complications (neuropathy, nephropathy, retinopathy) in patients of type 2 diabetes mellitus
Sample size of 200 was calculated using the epi-info statistical software for cross-sectional comparative study. Taking reference from Mukesh Gohel study [19], using proportion of patients in each group with raised serum iron level, the sample size came out to be 84 in each group at 5% precision, but taking attrition into consideration, we took 100 patients in each group.
One hundred patients of type 2 diabetes mellitus with HbA1c greater than seven constituted study population. One hundred patients of type 2 diabetes mellitus with HbA1c less than seven constituted control population. Study duration was from March 2014 to November 2015.
Blood investigations
-
1.
Glycated hemoglobin (normal range, < 6.5) was estimated by high performance liquid chromatography (HPLC).
-
2.
Serum iron (normal range, 41–130 μg/dl) was estimated by Bathophenthroline disulphonate assay (BPS).
-
3.
Transferrin saturation (normal range, 16–45%) was estimated by photometric color method.
-
4.
Serum ferritin (normal range, males 29–248 μg/dl and females 10–150 μg/dl) was measured by CLIA (chemiluminescence immuno assay).
Tests for Micro vascular complications
Retinopathy was screened by fundus examination.
Nephropathy screening was done by urine for albuminuria. Patients were taken as positive for microalbumin (a ratio of albumin (mcg/l) to creatinine (mg/l) of less than 30 was taken as normal; a ratio of 30–300 signified microalbuminuria) if found in this range on two occasions separated by 3 months.
Neuropathy screening was done by bed side criteria which have been validated by Chawla et al. [20] using the following:
-
A)
NSS (neuropathy symptom score)
-
B)
NDS (neuropathy disability score)
-
A)
Diabetic neuropathy symptom score (NSS): The questions should be answered “yes” (positive, 1 point) if a symptom (as mentioned in the table below) occurred more than two times a week during the last 2 weeks or “no” (negative, no point) if it did not.
Symptoms | No | Yes |
|---|---|---|
Unsteadiness in walking | 0 | 1 |
Burning feet | 0 | 1 |
Numbness or tingling of hands and/or feet | 0 | 1 |
Fatigue, cramping, aching, or nocturnal exacerbations | 0 | 2 |
-
B)
NDS (neuropathy disability score) is calculated as mentioned below.
Neuropathy disability score (NDS)
Vibration perception threshold using 128 Hz tuning fork Normal = can distinguish vibration | Normal = 0 Abnormal = 1 | Right foot | Left foot |
Temp perception on dorsum of foot Using cup full of cold or warm water or thermal tip | Normal = 0 Abnormal = 1 | Right foot | Left foot |
Pin prick Apply prick proximal to big toe nail just enough to deform the skin Trial pair = sharp/blunt Normal can distinguish sharp/not sharp | Normal = 0 Abnormal = 1 | Right foot | Left foot |
Achilles reflex | Present = 0 With reinforcement = 1 Absent = 2 | Right foot | Left foot |
NDS total out of = 10 | Right foot | Left foot |
Statistical analysis
Data was entered into MS Excel and analyzed using the SPSS version 17. Descriptive statistics in the form of mean and standard deviations or proportions were used to characterize the study sample. For qualitative data, chi-square or Fisher’s exact test was used to observe difference between proportions for independent groups. For continuous variables, student’s t test was used to compare the two groups. Pearson correlation coefficients were calculated between the outcome and quantitative independent demographic and clinical factors. p value of less than 0.05 was considered to be statistically significant. Linear regression analysis was done to determine the models contributing to HbA1C/predictors of HbA1C.
Results
The present comparative study evaluated the relationship between iron indices, Hb1Ac levels, and microvascular complications among patients with type 2 diabetes mellitus. This cross-sectional comparative study comprised of 200 patients (100 patients each categorized under the control and study type 2 diabetes). The overall statistics of the study subjects are shown in Tables 1 and 2.
Serum Iron and HbA1c
The present study states that there is a significant positive correlation of serum iron and HbA1c (r = 0.46; p = 0.001*) in the study diabetic group (Table 3). Similar results have been found in a study conducted by Shetty et al. [21] where a positive correlation between free iron and HbA1c was found in uncontrolled type 2 diabetes (r = + 0.513; p < 0.01)
Serum ferritin and HbA1c
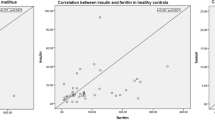
Our study shows that there is a significant positive correlation between serum ferritin levels with HbA1c (r = 0.43; p = 0.001*) which coincides with a study conducted by Sumeet et al. [22] (Fig 1). Their study showed significant positive correlation between serum ferritin with HbA1c (p = 0.04) and also positive correlation between raised ferritin levels in study diabetics. In a study conducted by Sun et al. [23], elevated-circulating ferritin concentrations were associated with higher risk of type 2 diabetes and metabolic syndrome in middle-aged and elderly Chinese independent of obesity, inflammation, adipokines, and other risk factors which support our association of ferritin with HbA1c.

Scatter graph depicting strength between serum ferritin and HbA1c in control diabetics
Microvascular complications
In the present study, there is a significant positive correlation between serum iron, serum ferritin levels, and microvascular complications; nephropathy, retinopathy, and neuropathy (p = 0.001) (Tables 4, 5, 6, 7, and 8). HbA1c and duration of diabetes also correlated well with microvascular complications (p = 0.001) which were significantly higher in the study diabetes group in comparison to the control diabetes group (Table 9). Correlation with HbA1c and duration is a well-known fact, and our study also showed the same consistent results. Dymock et al. [10] reported influence of the increase body iron stores on diabetic nephropathy and vascular dysfunction. In a study by Canturk et al. [16], patients of diabetes had hyperferritinemia, and they found correlation between ferritin levels and diabetic retinopathy. These findings are in accordance with our study.
Transferrin saturation and HbA1c
We also observed the relationship of transferrin saturation with HbA1c; however, we found weak negative correlation in the study diabetic group which was insignificant (r = − 0.05; p = 0.6) consistent with a study conducted by Montonen et al. [3]. But in study conducted by Thomas et al [24], they observed that higher transferrin saturation was observed in diabetics compared to healthy individuals.
Fernandez-Real et al. [25] documented in general population increased body iron stores associated with increased occurrence of glucose intolerance, type 2 diabetes, and gestational diabetes which is consistent with our study.
Elevated iron and diabetes
In the last few decades, the impact of transition metals, and iron in particular, on human physiology has been explored. Iron, being a first-line prooxidant, seems to regulate the clinical manifestations of various systemic diseases, including diabetes and atherosclerotic vascular diseases. Iron regulation of the cell oxidative stress can explain, to some extent, its close association with abnormalities in insulin sensitivity.
The mechanisms by which elevated iron stores may induce diabetes include oxidative damage to pancreatic beta cells, impairment of hepatic insulin secretion by the liver, and interference with insulin’s ability to suppress hepatic glucose production.
Elevated ferritin and diabetes
Oxidative stress and chronic inflammation are being postulated as mechanisms involved in the pathophysiology of diabetes and its complications. Being an inflammatory biomarker and a reflector of iron stores, higher ferritin levels in correspondence to higher iron levels in our study might have been associated with the positive correlation observed in our study with both poor glycemic control and long-term microvascular complications.
Transferrin saturation and diabetes
Based on previous studies, it was speculated that Se transferrin levels may increase as a compensatory mechanism for a reduction in free iron levels that may occur secondary to oxidative stress, and thus, it may serve as a biomarker of some other factor that is causally related to diabetes, and possibly not related to iron load. In the present study, we did not find any association between Se transferrin and diabetes incidence. Interestingly, Se transferrin seemed to be associated with diabetes risk in individuals with HbA1c values in the control group, but not in those with higher HbA1c values.
Limitations
-
1.
Sample size of the study is small, thereby preventing us from drawing strong conclusions.
-
2.
Diabetes mellitus is a state of chronic inflammation. Though ferritin is a marker of chronic inflammation, the causal relationship between raised ferritin and the study diabetes group is a matter of debate and requires further exploration in establishing the authenticity of causal hypothesis.
Summary and conclusion
In the present cross-sectional, comparative study, we have found significant positive correlation between iron indices (serum iron, serum ferritin) and HbA1c levels in the study group with type 2 diabetes mellitus. We also found that iron indices (i.e., serum iron, serum ferritin, and transferrin saturation) have significant correlation with microvascular complications in them. However, we did not observe any significant correlation between transferrin saturation and HbA1c levels in the present study (p = 0.62).
We conclude that serum ferritin and serum iron may be used as surrogate markers of poor glycemic control and microvascular complications in association with HbA1c. Though, the causal association of iron indices is evident by the regression analysis in our study, further larger trials need to be undertaken to establish this causal relationship.
References
De Fronzo RA. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58(4):773–95.
Kalra S, Chawla R, Madhu SV. The dirty dozen of diabetes. IJEM. 2013;17(3):367–9.
Montonen J, Boeing H, Steffen A, Lehmann R, Fritsche H-G, Joost M, et al. Body iron stores and risk of type 2 diabetes: results from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam study. Diabetologia. 2012;55:2613–21.
Fernandez-Real JM, Lopez-Bermejo A, Ricart W. Cross talk between iron metabolism and diabetes. Diabetes. 2002;51:2348–54.
Dmochowski K, Finegood DT, Francombe W, Tyler B, Zinman B. Factors determining glucose tolerance in patients with thalassemia major. J Clin Endocrinol Metab. 1993;77:478–83.
Cavallo-Perin P, Pacini G, Cerutti F, Bessone A, Condo C, Sacchetti L, et al. Insulin resistance and hyperinsulinemia in homozygous ß-thalassemia. Metabolism. 1995;44:281–6.
Wrede CE, Buettner R, Bollheimer LC, Scholmerich J, Palitzsch KD, Hellerbrand C. Association between serum ferritin and the insulin resistance syndrome in a representative population. Eur J Endocrinol. 2006;154:333–40.
Suvarna J, Ingle H, Deshmukh CT. Insulin resistance and beta cell function in chronically transfused patients of thalassemia major. Ind Pediatr. 2006;43:393–400.
Ascherio A, Rimm EB. Blood donation and risk of coronary heart disease in men. Circulation. 2001;103:52–7.
Dymock IW, Cassar J, Pyke DA, Oakley WG. Observations on the pathogenesis, complications and treatment of diabetes in 115 cases of haemochromatosis. Am J Med. 1972;52:203–10.
Facchini FS. Effect of phlebotomy on plasma glucose and insulin concentrations. Diabetes Care. 1998;21:219.
Rajpathak S, Ma J, Manson J, Willett WC. Hu FB. Iron intake and the risk of type 2diabetes in women: a prospective cohort study. Diabetes Care. 2006;29:1370–612.
Jiang R, Ma J, Ascherio A, Stampfer MJ, Willett WC. Hu FB. Dietary iron intake and blood donations in relation to risk of type 2 diabetes in men: a prospective cohort study. Am J Clin Nutr. 2004;79:70.
MacDonald MJ, Cook JD, Epstein ML, Flowers CH. Large amount of (apo) ferritin in the pancreatic insulin cell and its stimulation by glucose. FASEB J. 1994;8:777–81.
Rahier JR, Loozen S, Goebbels RM, Abrahem M. The hemochromatotic human pancreas: a quantitative immunohistochemical and ultrastructural study. Diabetologia. 1987;30:5–12.
Canturk Z, Cetinarslan B, Tarkun I. Serum ferritin levels in poorly-and well-controlled diabetes mellitus. Endocr Res. 2003;29:299–306.
Loebstein R, Lehotay DC, Luo X, Bartfay W, Tyler B, Sher GD. Diabetic nephropathy in hypertransfused patients with beta-thalassemia. The role of oxidative stress. Diabetes Care. 1998;21:1306–9.
Mascitelli L, Pezzetta F. High iron stores and impaired endothelial function in prediabetic subjects. Am J Cardiol. 2006;97:1550.
Mukesh Gohel HB, Sirajwala AC. Serum free iron concentration in patients with type 2 diabetes mellitus with good and poor control and its correlation with glycemic control. Int J Diab Res. 2013;2(2):33–8.
Chawla A, Bhasin G, Chawla R. Validation of neuropathy symptoms score (NSS) and neuropathy disability score (NDS) in the clinical diagnosis of peripheral neuropathy in middle aged people with diabetes. Internet J Family Prac. 2013;12:1.
Shetty JK, Prakash M, Ibrahim MS. Department of Biochemistry, Kasturba Medical College, Manipal-576104, Karnataka, India. Indian J Clin Biochem. 2008;23(1):67–70.
Sumeet S, Tandon VR, Sharma S, Kudiyar RP. Serum.ferritin and Type 2 Diabetes Mellitus. JK Sci J Med Educ Res. 2007;4:9.
Sun L, Franco OH, Hu FB, Cai L, Yu Z, Li H, et al. Ferritin concentrations, metabolic syndrome, and type 2 diabetes in middle-aged and elderly chinese. Clin Endocrinol Metab. 2008;93(12):4690–6. https://doi.org/10.1210/jc.2008-1159.
Thomas MC, Maclsaac RJ, Tsalamandris C, Jerums G. Elevated Iron Indices in Patients with Diabetes. Diabet Med. 2004;21(7):798–802.
Fernandez-Real JM, Lopez-Bermejo A, Ricart W. Cross talk between iron metabolism and diabetes. Diabetes. 2002;51:2.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chawla, R., Bhoopathi, A. & Punyani, H. Ferritin and serum iron as surrogate markers of poor glycemic control and microvascular complications in type 2 diabetes mellitus. Int J Diabetes Dev Ctries 39, 362–368 (2019). https://doi.org/10.1007/s13410-018-0687-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13410-018-0687-1