
Abstract
Background
Small-dense (sd)LDL-cholesterol (C) is a potent risk factor for atherosclerotic cardiovascular disease (ASCVD) beyond LDL-C, and 35 mg/dL has been proposed as a cut-off value for high-sdLDL-C. sdLDL-C levels are strongly regulated by triglycerides (TG) and LDL-C levels. LDL-C has detailed targets for the prevention of ASCVD, while TG is only defined as abnormal at ≥ 150 mg/dL. We investigated the effect of hypertriglyceridemia on the prevalence of high-sdLDL-C in patients with type 2 diabetes and explored the optimal TG levels that would suppress high-sdLDL-C.
Methods
Fasting plasma was obtained from 1569 patients with type 2 diabetes who were enrolled in the regional cohort study. sdLDL-C concentrations were measured by the homogeneous assay established by us. High-sdLDL-C was defined as ≤ 35 mg/dL according to the Hisayama Study. Hypertriglyceridemia was defined as ≥ 150 mg/dL.
Results
All lipid parameters except HDL-C were higher in the high-sdLDL-C group than in the normal-sdLDL-C group. The receiver operating characteristic (ROC) curves revealed that high sdLDL-C was identified sensitively by TG and LDL-C, with cut-off values of 115 mg/dL for TG and 110 mg/dL for LDL-C. The presence of hypertriglyceridemia increased the prevalence of high-sdLDL-C sixfold more than the normotriglyceridemic counterpart, regardless of statin use. This substantial influence of hypertriglyceridemia was found even within the control target of LDL-C levels (70–120 mg/dL) for diabetic subjects.
Conclusions
The TG cut-off for high-sdLDL-C was well below 150 mg/dL in a diabetic population. Amelioration of hypertriglyceridemia is needed even when LDL-C targets for diabetes are achieved.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Several large cohort studies have revealed that small dense (sd) low-density lipoprotein (LDL)-cholesterol(C) is a potent risk factor for atherosclerotic cardiovascular disease (ASCVD) beyond LDL-C [1,2,3]. In the Hisayama study [3], the risk of coronary heart disease (CHD) almost doubled in subjects with sdLDL cholesterol of ≥ 32.9 mg/dL, regardless of LDL-C levels, as compared with subjects with sdLDL cholesterol of < 32.9 mg/dL. Therefore, a cut-off value of 35 mg/dL for sdLDL-C was proposed [3]. The sdLDL-C concentration is strongly regulated by triglyceride (TG) and LDL-C concentrations [4, 5]. Indeed, a simple formula for calculating sdLDL-C concentration using TG and LDL-C has been proposed by Sampson et al. [6]. Thus, it is easily understood that combined hyperlipidemia (hypertriglyceridemia and hypercholesterolemia) exhibits the highest sdLDL-C levels among the various dyslipidemic phenotypes [4]. The Japanese Atherosclerosis Society (JAS) guidelines for prevention of atherosclerotic cardiovascular diseases state that LDL-C should be 120 mg/dL or less if diabetes is present, 100 mg/dL or less if diabetes-related complications are present, and 70 mg/dL or less if CHD or atherothrombotic stroke is present (second prevention) [7]. Unlike LDL-C, which has detailed management goals, the goal for TG is only stated as less than 150 mg/dL fasting and 175 mg/dL nonfasting, and the presence of diabetes is not considered [7]. Statins, potent LDL-C-lowering drugs, are widely used in diabetic patients, and LDL-C targets are easily achieved. On the other hand, TG, which is specifically elevated in diabetes, is often overlooked. The main reason for overlooking TG is the lack of clear evidence of a preventive effect of the TG-lowering drugs, fibrates [8, 9] and omega-3 fatty acids [10], on ASCVD events. However, it should be noted that TG is causally related to atherosclerosis and TG is an established risk factor for ASCVD in the general population [11, 12] and diabetic population [13].
It is well known that the atherogenicity of TG is mainly due to TG-rich lipoprotein (TRL) remnants, preponderance of sdLDL particles, and low high-density lipoprotein (HDL)-C [13]. In this study, we focused on the relationship between TG and sdLDL-C and examined how the presence of hypertriglyceridemia, apart from LDL-C, is associated with the prevalence of high-sdLDL-C. The results of this study may draw attention to the underestimation of hypertriglyceridemia and suggest the need for stricter TG control in diabetic patients.
Methods
Patients with type 2 diabetes (n = 1569) were examined who were participants of the regional diabetes cohort (ViNA cohort) [14]. Most patients with type 2 diabetes were treated with oral hypoglycemic agents (81%) or in combination with insulin (21%).
The hypoglycemic agents are shown in Table 1. Dyslipidemic subjects were treated with statins (53%), ezetimibe (7%), fibrates (7%), or omega-3 fatty acids (4%) alone or in combination. Collectively, 60% of subjects were treated with any lipid-lowering drugs. Patients with severe hypertriglyceridemia (TG ≥ 1000 mg/dL, n = 3) were excluded to avoid wild relationship between TG and other lipid parameters. According to the Japanese Atherosclerosis Society (JAS) guidelines for prevention of atherosclerotic cardiovascular diseases, the target LDL-C level is 120 mg/dl or less in the presence of diabetes (primary prevention), 100 mg/dL or less in the presence of diabetes-related complications (primary prevention), and 70 mg/dL or less in the presence of CHD or atherothrombotic stroke (secondary prevention). According to the guideline, LDL ranges were defined as L1 ≤ 69 mg/dL, L2: 70–99 mg/dL, L3: 100–119 mg/dL, L4: 120–139 mg/dL, L5 ≥ 140 mg/dL, respectively. Plasma samples were taken in the morning after overnight fasting. sdLDL-C was measured directly in plasma by our established homogeneous method [15]. LDL-C, HDL-C, and apolipoprotein B, CIII, and E were measured by commercially available test kits. nonHDL-C was calculated by subtracting HDL-C from total-C. TG-rich lipoprotein (TRL)-C was calculated by subtracting nonHDL-C from total-C.
The study complied with the principal of the Declaration of Helsinki. The study was explained in detail to all subjects who agreed to participate, and written informed consents were obtained from all subjects. This study was approved by the Ebina General Hospital Ethics Committee (no115,2019).
Statistics
Continuous variables were expressed as mean ± standard deviation (SD). Categorical variables were expressed as percentage of subjects. Significance between groups was evaluated by chi-square test or unpaired t test. p-value less than 0.05 was considered statistically significant. Receiver operator characteristic (ROC) analysis was carried out to explore the area under the curve (AUC) and optimal TG or LDL-C values to identify high-sdLDL-C. The optimal cut-off value was defined as the concentration at which the sensitivity and specificity were closest to the AUC. Analyses were performed using JMP software version 15 (SAS Institute, Cary, NC, USA).
Results
Table 1 shows a comparison of clinical characteristics and measurements between the normal-sdLDL-C group (< 35 mg/dL, n = 1056) and the high-sdLDL-C group (≥ 35 mg/dL, n = 513). The high-sdLDL-C group was younger, more male, had a higher BMI, and had poor glycemic control than the normal-sdLDL-C group. Most patients with type 2 diabetes were treated with oral hypoglycemic agents (81%) or in combination with insulin (21%). The hypoglycemic agents are shown in Table 1. The prevalence of diabetic retinopathy was slightly lower in the high-sdLDL-C group, but eGFR was comparable between groups. The prevalence of coronary artery disease and cerebrovascular disease was similar between groups. Fasting plasma TG concentrations were twice higher in the high-sdLDL-C group than in the normal-sdLDL-C group. Similar differences were observed for TRL-C, apoCIII, and apoE, which are strongly related to TG. LDL-C, non-HDL-C, and apoB were higher and HDL-C was lower in the high-sdLDL-C group. More than half of the subjects were treated with statins, but there were no significant differences in statin use between the sdLDL-C subgroups. This was also true for all lipid-lowering drugs. The high SdLDL-C group was less likely to use insulin and more likely to use SGLT2 inhibitors. Use of other antidiabetic agents was similar between groups.
Figure 1 shows the ROC curves for the identification of high-sdLDL-C with TG or LDL-C concentrations. TG or LDL-C significantly identified high-sdLDL-C, and their combination was more sensitive. The AUC was 0.829 for TG value, 0 0.746 for LDL-C, and 0.898 for both (p < 0.0001). The cut-off values for high-sdLDL-C detection were TG = 115 mg/dL and LDL-C = 110 mg/dL. ROC curve analysis showed that HDL-C significantly identified high sdLDL-C (AUC = 0.61, p < 0.01), but this association was lost when TG and LDL-C were entered into a multivariate logistic analysis (data not shown).

Receiver operator characteristic (ROC) curves for the determination of TG or LDL-C cut-off values for prevalence of high-sdLDL-C (≥ 35 mg/dL). A = TG as varible; B = LDL-C as variable, and C = TG and LDL-C as variables. AUC = area under the curve. n = 1569
Figure 2 shows the prevalence of high-sdLDL-C without/with hypertriglyceridemia. The prevalence of high-sdLDL-C was 10% in normotriglyceridemic group and 64% in the hypertriglyceridemic group, indicating that high-sdLDL-C frequency was sixfold higher in the hypertriglyceridemic group. These results were the same when subjects were divided into statin use and non-statin use.

Prevalence of high-sdLDL-C in normotriglyceridemia and hypertriglyceridemia. High-sdLDL-C (≥ 35 mg/dL); normotriglyceridemia ≤ 150 mg/dL; hypertriglyceridemia ≥ 150 mg/dL. A = total subjects n = 1569 (1148 normotriglyceridemia and 421 hypertriglyceridemia). B = subjects with non-statin use n = 725 (542 normotriglyceridemia and 183 hypertriglyceridemia). C = subjects with statin use n = 844 (606 normotriglyceridemia and 238 hypertriglyceridemia)
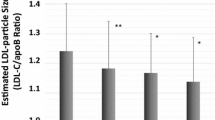
Figure 3 shows the prevalence of high-sdLDL-C stratified by LDL-C range in the normotriglyceridemic and hypertriglyceridemic groups. In the normotriglyceridemic group, the prevalence of high-sdLDL-C were 0, 6, 20, 37, and 63% for L1, L2, L3, L4, and L5, respectively, indicating that the percentage gradually increased with increasing LDL-C but remained below 50% with the exception of L5. On the other hand, in the hypertriglyceridemic group, the prevalence of high-sdLDL-C was markedly increased in all LDL-C ranges: 35, 57, 80, 87 and 100% for L1, L2, L3, L4 and L5, respectively. Thus, a high prevalence (≥ 50%) of high-sdLDL-C was observed even at optimal LDL-C levels (< 120 mg/dL) for primary prevention for patients with diabetes and its complications; the prevalence of high-sdLDL-C in L2, L3 and L4 was 9.5-, 4.0- and 2.3-fold higher in the hypertriglyceridemic group than in the normotriglyceridemic group.

Prevalence of high-sdLDL-C in normotriglyceridemia and hypertriglyceridemia stratified by LDL-range. The LDL-C ranges are L1 < 69 mg/dL, L2: 70–99 mg/dL, L3: 100–119 mg/dL, L4: 120–139 mg/dL, L5 > 140 mg/dL Number of subjects in L1, L2, and L3; L1, L2, L3, L4, and L5 are 108, 469, 328, 164, 79 (total n = 1148) in the normotriglyceridemic group and 40, 134, 131, 87, 29 (total n = 421) in the hypertriglyceridemic group
Discussion
While the importance of lowering LDL-C to prevent the development of ASCVD in diabetes is well recognized, the importance of managing TG, which is particularly elevated in type 2 diabetes, is often neglected. The Framingham study has shown that sdLDL-C is the most sensitive lipid biomarker for predicting ASCVD [1]. The Hisayama study also showed that sdLDL-C concentration was a sensitive predictor of future CHD events in Japanese community, and suggested 35 mg/dL as a cut-off value [3]. In this study, we attempted to determine the appropriate TG level for diabetic patients using sdLDL-C, a highly sensitive biomarker for ASCVD. The results showed that hypertriglyceridemia was associated with a sixfold higher prevalence of high-sdLDL-C compared to normotriglyceridemia. Furthermore, the effect of hypertriglyceridemia on high-sdLDL-C was more remarkably observed in the lower LDL-C levels. The ROC curve analysis showed that the cut-off value of TG for identifying high-sdLDL-C was 115 mg/dL, which is within the range of normotriglyceridemia and well below hypertriglyceridemic level. These results may raise the question of whether a TG cut-off of 150 mg/dL is really sufficient to prevent ASCVD in terms of cardiovascular biomarkers.
LDL-C is another strong determinant of sdLDL-C [4,5,6]. ROC analysis showed that LDL-C alone can identify sdLDL-C with high sensitivity and specificity (AUC = 0.746), but the combination with TG further increased sensitivity and specificity (AUC = 0.898), suggesting an additive effect of TG on sdLDL-C. In normotriglyceridemia, the prevalence of high sdLDL-C decreased by half as LDL-C decreased, whereas in hypertriglyceridemia the prevalence of high sdLDL-C decreased only slightly (7–23%) as LDL-C decreased. These results suggest that in the presence of hypertriglyceridemia, enhanced LDL-C lowering is not very effective in suppressing high sdLDL-C, and that a slight reduction in LDL-C can effectively suppress this once hypertriglyceridemia is resolved. The LDL-C cut-off value to discriminate high-sdLDL-C was 110 mg/dL, which corresponds to the control target for primary prevention in diabetic patients. For LDL-C that has reached the control target, no further lowering is considered necessary. To effectively control sdLDL-C for primary prevention of ASCVD, treatment of hypertriglyceridemia may be a better strategy than increasing statin intensity.
The Pemafibrate to Reduce Cardiovascular Outcomes by Reducing Triglycerides in Patients with Diabetes (PROMINENT) trial was recently published [9], which was designed to determine whether pemafibrate, a TG-lowering drug, can reduce the incidence of ASCVD in hypertriglyceridemic diabetic patients whose LDL-C was controlled below 70 mg/dL with high-intensive statins. Unexpectedly, this study failed to demonstrate the preventive effects of pemafibrate on ASCVD. As a possible reason for negative study, we reported the hypothesis that calculated sdLDL-C levels [6] were not reduced by pemafibrate treatment [16]. Possibly, very low LDL-C levels with intensive statin pretreatment may attenuate the suppressive effect of TG lowering on sdLDL-C [16]. On the other hand, the present study suggests that hypertriglyceridemia increases sdLDL-C when LDL-C levels are above the secondary prevention level of < 70 mg/dL. Therefore, even after achieving LDL-C targets for primary prevention (70–120 mg/dL), efforts should be made to control hypertriglyceridemia to reduce sdLDL-C. Further clinical trials are needed to determine whether TG lowering can reduce ASCVD in hypertriglyceridemic diabetic patients whose LDL-C is within control targets for primary prevention.
Conclusion
Hypertriglyceridemia was substantially associated with a high prevalence of high-sdLDL-C, even when LDL-C is within target ranges for primary prevention of diabetes. Thus, amelioration of hypertriglyceridemia is important to prevent ASCVD in patients with diabetes.
Data Availability
The datasets used and analyzed in the current study are available from the corresponding author on reasonable request.
References
Ikezaki H, Lim E, Cupples LA, Liu CT, et al. Small dense low-density lipoprotein cholesterol is the most atherogenic lipoprotein parameter in the prospective Framingham Offspring Study. J Am Heart Assoc. 2021;10(5):e019140.
Hoogeveen RC, Gaubatz JW, Sun W, et al. Small dense low-density lipoprotein-cholesterol concentrations predict risk for coronary heart disease: the Atherosclerosis Risk in Communities (ARIC) study. Arterioscler Thromb Vasc Biol. 2014;34:1069–77.
Higashioka M, Sakata S, Honda T, et al. Small dense low-density lipoprotein cholesterol and the risk of coronary heart disease in a Japanese community. J Atheroscler Thromb. 2020;27:669–82.
Hirano T, Ito Y, Koba S, et al. Clinical significance of small dense low-density lipoprotein cholesterol levels determined by the simple precipitation method. Arterioscler Thromb Vasc Biol. 2004;24:558–63.
Hayashi T, Koba S, Ito Y, et al. Method for estimating high sdLDL-C by measuring triglyceride and apolipoprotein B levels. Lipids Health Dis. 2017;16:21.
Sampson M, Wolska A, Warnick R, et al. A new equation based on the standard lipid panel for calculating small dense low-density lipoprotein-cholesterol and its use as a risk-enhancer test. Clin Chem. 2021;67:987–97.
Japanese Atherosclerosis Society (JAS) guidelines for prevention of atherosclerotic cardiovascular diseases 2022 Edit, Japanese Atherosclerosis Society (in Japanese).
Ginsberg HN, Elam MB, Lovato LC, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. 2010;362:1563–74.
Das Pradhan A, Glynn RJ, Fruchart J-C, et al. Triglyceride lowering with pemafibrate to reduce cardiovascular risk. N Engl J Med. 2022;387:1923–34.
Nicholls SJ, Lincoff AM, Garcia M, et al. Effect of high-dose omega-3 fatty acids vs corn oil on major adverse cardiovascular events in patients at high cardiovascular risk: the STRENGTH randomized clinical trial. JAMA. 2020;324(22):2268–80.
Nordestgaard BG. Triglyceride-rich lipoproteins and atherosclerotic cardiovascular disease: new insights from epidemiology, genetics, and biology. Circ Res. 2016;118:547–63.
Ginsberg HN, Packard CJ, Chapman MJ, et al. Triglyceride-rich lipoproteins and their remnants: metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies—a consensus statement from the European Atherosclerosis Society. Eur Heart J. 2021;42:4791–806.
Sone H, Tanaka S, Tanaka S, Iimuro S, et al. Serum level of triglycerides is a potent risk factor comparable to LDL cholesterol for coronary heart disease in Japanese patients with type 2 diabetes: subanalysis of the Japan Diabetes Complications Study (JDCS). Japan Diabetes Complications Study Group. J Clin Endocrinol Metab. 2011;96:3448–56.
Hirano T, Satoh N, Kodera R, et al. Dyslipidemia in diabetic kidney disease classified by proteinuria and renal dysfunction: a cross-sectional study from a regional diabetes cohort. J Diabetes Investig. 2022;13:657–67.
Ito Y, Fujimura M, Ohta M, et al. Development of a homogeneous assay for measurement of small dense LDL cholesterol. Clin Chem. 2011;57:57–65.
Hirano T. No change in small low-density lipoprotein cholesterol levels with pemafibrate might explain the negative results of the PROMINENT trial. J Diabetes Investig. 2023. https://doi.org/10.1111/jdi.13983. (Online ahead of print).
Acknowledgements
I would like to thank Dr. Yasuki Ito of Denka Co., Ltd. for supplying sdLDL-C test kit to Ebina General Hospital. I would like to thank to Drs. Takeshi Hirashima, Ema Aoki, and Natsuko Suzuki, and Mrs Miyuki Tokudome of Ebina General Hospital for performing ViNA cohort.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Tsutomu Hirano receives advisor fee from Denka Co, and lecture fee from Kowa Co.
Ethical consideration
This study was approved by the Ethics Committee of Ebina General Hospital.
Informed consent
The study was detailed to all subjects who consented to participate, and a written informed consent form was obtained from all participants prior to the study. Approval date of Registry and the Registration No. of the study/trial. Approval date: 11-September-2019, no 115, 2019.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Hirano, T. Hypertriglyceridemia contributes significantly to high prevalence of small dense LDL-cholesterol in patients with type 2 diabetes, even when LDL-C targets are achieved. Diabetol Int 14, 288–293 (2023). https://doi.org/10.1007/s13340-023-00634-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13340-023-00634-0