
Abstract
From January 2011 to December 2015, 70 consecutive patients underwent either laparoscopic surgery (LS) or robotic surgery (RS) total mesorectal excision (TME) for malignancy. Data were prospectically recorded in a dedicated local database including ASA score, age, operative time, conversion rate, re-operation rate, early complications, length of stay, and pathological results. We enrolled 70 consecutive patients, 35 treated with LS (18 M, 17 F), 35 treated with RS (23 M, 12 F). Median total operative time was 225 min in LS group (IQR 194–255) and 252.5 min for RS group (IQR 214–300). Median first flatus time was 2 days for LS group (IQR 1–3) and 1 day for RS group (IQR 1–2). Stool discharge time (median) was 4 days for LS group (IQR 2–5) and 2 days for RS group (IQR 1–3). Length of stay (median) was 8 days in LS group (IQR 7–10) and 7 days in RS group (IQR 5–8). It was not found any statistically significant difference between the two groups when we analyzed the number nodes harvested the postoperative complications. The 30 day mortality was 0% in both two groups. The conversion rate for LS group was 23% (8/35 pts) and that for RS group was 0% (0/35). The RS may overcome technical limitations of LS. In our experience, it is a feasible and safe technique, it achieves better clinical outcomes due to the lower conversion rate compared to LS, although with higher costs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Minimally invasive techniques have revolutionized general surgery, especially in the field of gastrointestinal surgery. The first hemicolectomy was performed laparoscopically in 1990 [1]. Since then, despite early skepticism towards this technique, laparoscopic technique for malignancy has been gradually performed. Since 2002, a series of randomized clinical trials compared the laparoscopic and the open technique, whose results definitely eliminated any doubts concerning the oncological adequacy of laparoscopic technique [2,3,4,5,6,7]. The advantages of minimally invasive approach in colorectal cancer surgery have been demonstrated in both pathophysiological (decreased inflammatory response → decreased immune response → decreased postoperative morbidity/comorbidity) and oncological aspects (similar results in terms of survival and outcome) [4,5,6,7,8,9].
Many advantages over traditional techniques have been reported, including less pain, quicker return to daily activities, minimal scarring, reduced recovery time, and less injury to tissue. Oncologic surgery is feasible with at least the same long-term results as the traditional open approach [10, 11].
The laparoscopic approach for colorectal disease, however, has both technical and “anatomical” disadvantages: long learning curve, presence of a large surgical field that requires a skilled camera assistant surgeon, constant dialog between the operator and the assistant, loss of three-dimensional vision, reduced ergonomics during specific phases of the procedure (need to take uncomfortable positions), poor dexterity of the laparoscopic instruments and decreased range of motion due to the rigidity of the insertion of the trocars site, amplification of physiological tremor, and the fulcrum effect [1, 12,13,14].
Compared with laparoscopy, surgery with robotic systems is known to have several advantages, including a more ergonomic position, a stable camera platform, a stereoscopic view under the surgeon’s direct control, elimination of tremors, and improved dexterity because of instruments with seven degrees of freedom that mimic hand movements. Robotic arms follow the slightest movement of the surgeon’s hands; it also can scale down hand movements when the tiniest dissections are needed and it eliminates hand tremors, which further enhances technology’s precision and control during surgical procedures [12, 15, 16].
Many works have been published regarding open and laparoscopic surgery [17, 18]; in the last few years, a lot of papers regarding robotic surgery have been published and we aim to contribute, with our experience gained in a single operative unit of general surgery, to the treatment of rectal cancer.
Materials and methods
We report our cumulative experience with TME for malignancy in a 5-year period, in relation to surgical technique evolved from LS into RS.
From January 2011 to December 2015, 70 patients underwent TME with LS or RS (since March 2012) with the DaVinci® System (Intuitive Surgical Inc., Sunnyvale, CA, USA).
Patients data including ASA score (American Society of Anesthesiologists’), age, BMI, previous abdominal surgery, comorbidity, tumor distance to anal verge, preoperative radio-chemotherapy operative time, conversion rate, re-operation rate, early complications, length of stay, and pathological results were prospectically recorded in a database.
We reviewed the prospectively collected records of patients with mid or low rectal cancer. The inclusion criteria were as follows: histologically proven adenocarcinoma located ≤ 15 cm from the anal verge; no evidence of distant metastasis at the time of surgery.
Tumor location was defined as the distance between the distal margin of the tumor and the anal verge as measured using a flexible colonoscopy.
All patients with a primary rectal cancer within 15 cm from the anal verge who were seen by a cancer surgeon and who were determined to be a candidate for laparoscopic or robotic-assisted resection were included. These patients underwent laparoscopic or robotic-assisted, and total mesorectal excision with primary anastomosis with or without diverting loop ileostomy. Neoadjuvant chemoradiotherapy was applied if necessary.
The Da Vinci® Robotic System (Intuitive Surgical Inc., Sunnyvale, CA, USA) was introduced in the Department of General Surgery, San Pio X Hospital in Milan, in January 2012 with the purpose of a multidisciplinary adoption (General Surgery, Urology, ORL, Gynecology). After being informed in detail about the procedure, patients were recruited for robot-assisted TME, instead of a traditional laparoscopic TME, according to patients’ wish. An informed consent was obtained. There were not any exclusion criteria for robotic surgery. All the patients underwent “fast track surgery” protocol according to ERAS guidelines, including bowel preparation during the 4 days before surgery. Before induction of general anesthesia, an epidural catheter for postoperative analgesia was positioned in selected cases and a urinary catheter was positioned in all patients. Standard DVT with Enoxaparin and antimicrobial with Cefazolin and Metronidazole prophylaxis was adopted.
Robotic surgery technique [15]
Surgery starts with the introduction of a trocar for the camera, three robotic trocars, and additional trocar for the assistant.
The previous laparotomies do not exclude by rule mini-invasive surgery because adhesions can be treated laparoscopically by the assistant surgeons before docking.
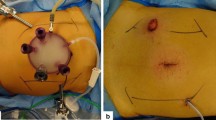
We usually perform a totally single docking technique; without repositioning the arms, such schemes have been modified to achieve an optimal positioning that has allowed us to perform left colectomy, R-LAR, and Miles procedures without conflicts. The trocars’ position is different between robotic and laparoscopic techniques, because the robotic trocar must have a minimum distance between them of at least 8–10 cm to avoid the conflict between the arms (Fig. 1). With the single docking technique, it is very important to ensure that the trocar is not aligned with each other on the same axis in relation to the three anatomic target (the splenic flexure, mesenteric vessels, and pelvis); if this was to occur, the conflict of arms would not allow the continuation of the procedure; in that case, the only remedy is to move the trocar during surgery or make more docking. It is a goaded to simulate the correct accesses positioning during the various phases of the operation, before their insertion. The robotic instruments used are the mono-polar scissors, bipolar forceps, the grasper (Prograsp or Cadiere), the robotic 30° scope oriented from top to bottom in the periumbilical 10–12 mm trocar, laparoscopic forceps, clips, and the linear stapler all inserted into the trocar in the right flank. The use of energy devices in robotic surgery is not necessary as in laparoscopic technique.

Robotic trocars placement
The patient is tilted into a deep Trendelenburg position with the left side maximally elevated. The patient cart is brought to the operating table following an oblique imaginary line joining the trocar of the camera, the left ASIS, and the camera arm aligned with the support of the cart plant. The robotic arms are then docked. The operative steps are the same than in laparoscopic technique as follows. We start the surgery with the opening of the colo-epiploic ligament from the middle third of the transverse colon to the left corner. The splenic flexure is taken down by spleno-colic ligament dissection with exposure of the pancreatic tail and Gerota fascia, and an initial detachment of the descending colon. A gauze is then inserted on the pancreas’ tail which will serve as a marker addressing the subsequent dissection from medial to lateral.
The Treitz’s ligament is identified, the posterior parietal peritoneum is opened, and the inferior mesenteric vein (IMV) is detected, dissected, and closed with hemostatic clips near the splenorenal mesenteric confluence; we proceed in the dissection of the medial side of the space underlying the IMV detaching the Toldt’s fascia from the Gerota’s fascia and cranially to the lower border of the pancreas rejoining the epiploon cavity identified by the gauze previously placed; the IMV is then sectioned. The incision of peritoneum is carried down by the IMV window to the promontory; the dissection of the preaortic space allows for the hypogastric branch identification and the IMA dissection approximately 1–1.5 cm from its origin. We routinely perform flush IMV and IMA ligation mainly to optimize mesenteric nodal dissection, and to achieve better colon mobilization and splenic flexure takedown. The IMA is closed with hemostatic clips and sectioned. The detachment of the Toldt’s fascia by gonadal vessels and ureter proceeds downward and laterally to complete the mobilization of the descending and sigmoid colon.
After the colon mobilization, the mesorectal plane is exposed. The holy plane between the mesorectal fascia and the presacral is dissected. The left and right branches of the inferior hypogastric plexus are identified and saved. Mesorectal dissection is performed posteriorly and on the right side (270°) down to the elevators muscles; the left lateral dissection is completed tractioning the rectum to the right side of the pelvis. The opening of the anterior peritoneal reflection is performed and the dissection of the recto vaginal septum, in women, or of the seminal vesicles and Denonvilliers’ fascia in men is completed.
Once the circumferential dissection of the rectum is completed, the linear stapler is introduced for rectal section which is not always easy, especially in cases of narrow pelvis. The last step of the intervention, before the extraction of the surgical specimen, is the preparation of the descending mesocolon: starting from the IMA stump.
A Pfannenstiel mini-laparotomy is executed and a wall protector is inserted; the specimen is extracted and cut; the anvil of the circular stapler is inserted into the proximal colon stump, which is then reduced in the abdomen. The mini-laparotomy is sutured. In cases of Miles procedure, the specimen is extracted from the perineal wound.
The pneumoperitoneum is created and a robot-assisted Knight–Griffen colorectal anastomosis is performed. When necessary, it is possible to put some stitches on the suture line. The operation is completed with the placement of a pelvic drainage, the identification of the last ileal loop for the ileostomy, which is always performed for ultra-low TMEs and in patients who underwent neo adjuvant therapy.
Statistical analysis
Numeric variables were summarized by their median and Inter-Quartile Range (IQR: first quartile–third quartile), categorical variables were summarized by absolute frequencies and percentages.
Differences among means were evaluated by non-parametric ANOVA or Mann–Whitney test. The Odds Ratios between groups were fitted by logistic regressions. P values were computed by permutation methods, to avoid any asymptotic approximation or distributional assumption, and adjusted for False Discovery Rate (p-adj), when appropriate. P values < 0.05 were considered significant. All analyses were computed in R environment (ver. 3.2.2).
Results
We enrolled 70 consecutive patients, 35 treated with LS (18 M, 17 F), 35 treated with RS (23 M, 12 F).
The median age for each group was 66 years (LS) and 70 years (RS).
We analyzed preoperative parameters like median BMI, number of comorbidity, number of patient with previous abdominal surgery, tumor distance to anal verge, ASA score, T stage, and type of surgery in both of two groups, and no statistical difference appeared (Table 1).
Distribution according to ASA Score (American Society of Anesthesiologists’) was as follows:
All patients underwent TME for malignancy diagnosed at endoscopic biopsy.
In LS group, rectal anterior resection (L-RAR) was performed in 28 (80%) patients, whereas Hartmann’s operation was performed in one patient (3%) and Miles’ operation was performed in six patients (17%).
In RS group, rectal anterior resection (R-RAR) was performed in 30 (86%) patients, whereas Hartmann’s operation was not performed in any patient (0%) and Miles’ operation was performed in five patients (14%).
The conversion rate for LS group was 23% (8/35 pts) and that for RS group was 0% lesion (one case), pelvic involvement (one case), no tumor identification (one case), and hypercapnia (one case). According to the Clavien–Dindo Classification [19] (Tables 2, 3), we considered the complications of grade I and II like minor complications; instead, the adverse events of grade III and IV are considered like major complications. No death (grade V) occurred nor in robotic neither in laparoscopic group.
The perioperative complications in LS group were: four anastomotic leakage requiring one revisional surgery, one percutaneous drainage and two conservative treatment, three anastomotic bleeding (one endoscopic and two conservative treatment), one duodenal ulcer perforation treated with surgery, and two patients had mechanical postoperative ileus (one required surgery, one conservative treatment), and one patient had multiorgan failure and required recovery in Intensive-Care Unit.
We performed three reoperations: one percutaneous drainage, one endoscopic treatment, and one patient which had an MOF; according to Clavien–Dindo Classification grade III and IV, there were six major complications in the laparoscopic group.
The 30 day mortality rate was 0% in the LS group.
The perioperative complications in RS group were: one anastomotic leakage requiring revisional surgery, two anastomotic bleeding (one endoscopic and one conservative treatment), one pelvic bleeding treated with surgery, two patients had mechanical postoperative ileus (one required surgery, one endoscopic treatment), and one patient had multiorgan failure and required recovery in Intensive-Care Unit.
We performed three reoperations, six endoscopic treatments, and one patient had an MOF; according to Clavien–Dindo Classification grade III and IV, there were six major complications in the robotic group. The 30 day mortality rate was 0% in the RS group.
Median total operative time was 225 min in LS group (IQR 194–255) and 252.5 min for RS group (IQR 214–300).
We considered the median operative time of the first 17 and the last 18 patients, according to the date of operation, treated with LS and RS to evaluate the learning curve. The results in LS were 220 min (IQR 175–252.5) for the first 17 and 225 min (IQR 210–257.5) for the last 18 patients, while the results in RS were 272.5 min for the first 17 (IQR 220–310) and 222.5 min (IQR 197.5–255) for the last 18 patients.
Median first flatus time was 2 days for LS group (IQR 1–3) and 1 day for RS group (IQR 1–2).
Stool discharge time (median) was 4 days for LS group (IQR 2–5) and 2 days for RS group (IQR 1–3).
Length of stay (median) was 8 days in LS group (IQR 7–10) and 7 days in RS group (IQR 5–8).
The median number of nodes harvested was 20 in LS group (IQR 10.75–23.5) and 16 in RS group (IQR 13–19.5) (Table 2).
Discussion
The first robotic colectomies were reported by Weber et al. [1]. Since then, a wide range of colorectal operations have been performed, including right and left colectomies, sigmoid resections, rectal anterior resections, abdominoperineal resections, and total colectomies. These operations were performed mainly on benign diseases [20]. Colorectal robotic surgery also seems to be feasible for malignant disease [15, 21, 22] with comparable results, in terms of oncologic radicality and surgical accuracy and in terms of short-term outcomes, compared to the standard laparoscopy.
The experience of our Department of Surgery is reported in this study. The goal was to evaluate the feasibility and the safety of robotic TME for cancer.
The layout for trocars placement, previously described by authors skilled in robotic surgery, was applied with some adjustments due to patient conformation to avoid arms collisions and achieve a single docking procedure.
We compared 70 consecutive patients treated with two different techniques (LS 35 pts and RS 35 pts) to evaluate whether the robotic approach to rectal surgery was as successful as the laparoscopic surgery. The LS and RS groups of patients, even if not randomly selected, were similar in terms of demographic and clinical characteristics (Table 1).
All the patients suffered from rectal cancer.
No statistically significative differences (p = 0.588) were found between the two groups in the number of harvested nodes.
The median operative time was significative lower in LS group (225 min) than RS group (252.5 min).
In many works, operative time in LS for malignancy is reported to be shorter than RS. RS has a high variable total operative time in different series (range 204–441 min) [15, 23,24,25,26,27,28] and the median operative time, in a recent meta-analysis, was found to be the same for both RS and LS for rectal cancer [29]. A recent retrospective multicenter analysis on data of 425 patients who underwent robotic total mesorectal excision for rectal lesions has shown a mean operative time of 240 min; that time differs only on 12 min from our data [30].
Our data are aligned with the most recent papers on the topic and we can affirm that the shorter operative time is the main advantage of LS compared to RS; nevertheless, in a growing number of articles, the operative time is the same for both RS and LS [31]; this is probably related to the faster learning curve of the RS compared with LS [32].
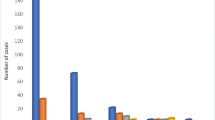
We observed that the total operative time in RS decreases significantly during the learning curve of the surgeon and the team (Fig. 2): we analyzed the operative median time of the first 17 patients of the laparoscopic and robotic group with the last 18 patients of the same groups. Comparing the two subpopulation of LS, we did not find any statistical difference in time of median operating time (215 min and 225 min) between the two groups; conversely, comparing the two subpopulation in RS, we recognized a significant statistical difference (p < 0.05) in the median operative time between the first 17 and the last 18 patients (272.5 min and 225.5 min) who underwent surgery. Moreover, comparing the group of the last patients who underwent RS with the LS, we did not find any statistical difference. This result confirm our hypothesis about the different operative time of RS comparing with LS: however, we found that, after an adequate learning curve, there was no difference among RS and LS.

Learning curve for robotic surgery
We observed that the recover of the bowel function and the length of stay are significantly reduced in RS than LS groups (respectively, p < 0.001 and p < 0.002).
The median first flatus time was 1 day for RS group and 2 days for LS group (p < 0.001).
The rapid recovery of the first flatus time with minimally invasive procedures, especially with robotic techniques, agrees with the results found in the literature [27, 28, 33].
Rapid bowel recovery after surgery allows for shorter length of stay; in fact, in RS, patients are dismissed 7 days after surgery compared to 8 days in LS. The better outcome for RS is statistically significant (p < 0.002).
The increased operative time is justified either in terms of clinical benefit to the patient or costs of hospitalization. The early resumption of intestinal function can be attributed to less trauma due to the absence of conversion to laparoscopic or open surgery, due to robotic instruments that act on a fulcrum located in the abdominal wall thickness and by the lower traction of colon which is guaranteed by the presence of a fixed and stable field, with robotic instruments able to perform the most delicate and fragmented traction during surgery. In no case in the RS group was it necessary to place additional laparoscopic or robotic trocars to overcome conflicts of instruments or robotic arms, reducing abdominal wall trauma.
A substantial difference was observed in the conversion rate if we compare the two groups of minimally invasive surgery.
In the literature, between the various patient series, we found a significant variability of the conversion rate from laparoscopy to open surgery. Recent papers attest this value between 10 and 31% [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34].
In our experience, the conversion rate in LS group was 23% (8/35) compared to 0% (0/35) in the RS group (p < 0.001).
In all cases treated with robotics, the procedures were performed totally robotically.
The best result in favor of RS group, in terms of conversion, was statistically significant (p < 0.001).
The robotic technique allows us to carry out easily all the cases of difficult TME without need of conversion to open surgery, even if with longer operative time.
In a recent paper, 776,007 patients were analyzed, of which nearly 1000 underwent laparoscopic TME; compared with patients who had a complete laparoscopic operations, patients who had conversion to open surgery (about 31%) had a higher mortality, higher overall morbidity, longer length of hospitalization, and increased hospital charges [34].
Between January 20, 2004, and May 4, 2010, 1044 patients with rectal cancer enrolled in the COLOR II trial and were randomized to either laparoscopic or open surgery. Of 693 patients who had laparoscopic surgery, 114 (16%) were converted to open surgery [17].
This result emphasizes the importance of the low conversion rate which is allowed by the robotic surgery and means reduced need for medical and surgical short- and long-term cares, with an earlier resumption of normal social and work activities like shown in three recent meta-analysis [35,36,37].
The laparoscopic surgery for rectal cancer is technically demanding for the anatomical conformation of the pelvis, especially for narrow pelvis in male patients and for the loss of correct visual and often for the position of the surgeons on the operative field. The robotic surgery exceeds these limitations and offers an effective solution for patients and surgeon.
In our laparoscopic group, the major cause of conversion to open surgery is due to a difficult TME in male’s narrow pelvis (four cases). The R.O.L.A.R.R. randomized clinical trial reports a higher, but not statistically significant, conversion rate in laparoscopic than robotic technique (12.2% vs 8.1%, p = 0.16); in the obese and male patients subpopulation, the conversion rate is significant higher in laparoscopy than robotics (p < 0.01) [38].
We do not found a statistically significative difference between the two mini-invasive techniques (LS and RS) regarding postoperative complications.
The 30 day mortality was 0% for LS and RS groups.
The statistical analysis did not show significant differences between the groups in terms of anastomotic bleeding and anastomotic leakage.
Conclusions
In our experience, the two techniques obtain the same pathological outcomes.
It seems that the operative time is the main advantage shown by the LS group; however, we found that, after an adequate learning curve, the two techniques achieved the same operative time.
RS group obtained the best results in terms of postoperative outcomes, such as the more rapid recovery of the intestinal functionality and a lower postoperative length of stay. The RS group had a 0% conversion rate and this fact is of considerable importance, because we know from the literature that patients who had conversion to open surgery had a higher mortality, higher overall morbidity, longer length of hospitalization, and increased hospital charges.
The RS may exceed the limitation of traditional laparoscopic surgery. In our experience, it is a feasible and safe technique; it achieves better clinical outcomes and obtains the same pathological results compared to LS and OS, although with higher costs. RS permits to perform difficult dissections with greater precision and safety with all the advantages guaranteed by the minimally invasive access.
The authors assume that robotic TME for rectal cancer could find its specific indication to perform nerve sparing TME routinely to reach better functional outcomes and to treat male patients after neoadjuvant chemoradiation therapy.
Further studies are needed.
References
Weber PA, Merola S, Wasielewski A, Ballantyne GH (2002) Tele-robotic assisted laparoscopic right and sigmoid colectomies for benign disease. Dis Colon Rectum 45:1689–1694
Lacy AM, García-Valdecasas JC, Delgado S, Castells A, Taurá P, Piqué JM, Visa J (2002) Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomized trial. Lancet 359:2224–2229
Jayne DG, Guillou PJ, Thorpe H, Quirke P, Copeland J, Smith Adrian MH, Heath RM, Brown JM (2007) Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC trial group. J Clin Oncol 25:3061–3068
Poulin EC, Mamazza J, Schlachta CM, Gregoire R, Roy N (1999) Laparoscopic resection does not adversely affect early survival curves in patients undergoing surgery for colorectal adenocarcinoma. Ann Surg 229(4):487–492
Hasegawa H, Kabeshima Y, Watanabe M, Yamamoto S, Kitajima M (2003) Randomized controlled trial of laparoscopic versus open colectomy for advanced colorectal cancer. Surg Endosc 17:636–640. https://doi.org/10.1007/s00464-002-8516-4
Kaiser AM, Kang JC, Chan LS, Vukasin P, Beart RW Jr (2004) Laparoscopic-assisted vs open colectomy for colon cancer: a prospective randomized trial. J Laparoendosc Adv Surg Tech A 14(6):329–334
Champault GG, Barrat C, Raselli R, Elizalde A, Catheline J-M (2002) Laparoscopic versus open surgery for colorectal carcinoma. Surg Laparosc Endosc Percutan Tech 12(2):88–95
Delgado S, Lacy AM, Filella X, Castells A, García-Valdecasas JC, Pique JM, Momblán D, Visa J (2001) Acute phase response in laparoscopic and open colectomy in colon cancer. Randomized study. Dis Colon Rectum 44(5):638–646
Jian-Kun H, Zhou Z-G, Chen Z-X, Wang L-L, Yong-Yang Yu, Liu J, Zhang B, Li L, Shu Y, Chen J-P (2003) Comparative evaluation of immune response after laparoscopical and open total mesorectal excisions with anal sphincter preservation in patients with rectal cancer. World J Gastroenterol 9(12):2690–2694
Weeks JC, Nelson H, Gelber S, Sargent D, Schroeder G, Clinical Outcomes of Surgical Therapy (COST) Study Group (2002) Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: a randomized trial. JAMA 287:321–328
Nelson H, Sargent D, Wieand HS, The Clinical Outcomes of Surgical Therapy Study Group et al (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 350:2050–2059
Cadiere GB, Himpens J, Germay O et al (2001) Feasibility of robotic laparoscopic surgery: 146 cases. World J Surg 25:1467–1477
Baik SH, Ko YT, Kang CM, Lee WJ, Kim NK, Sohn SK, Chi HS, Cho CH (2008) Robotic tumor-specific mesorectal excision of rectal cancer: short-term outcome of a pilot randomized trial. Surg Endosc 22(7):1601–1608. https://doi.org/10.1007/s00464-008-9752-z (Epub 2008 Feb 13)
Ballantyne GH (2002) Robotic surgery, telerobotic surgery, telepresence, and telementoring. Review of early clinical results. Surg Endosc. 16(10):1389–1402 (Epub 2002 Jul 29)
D’Annibale A, Pernazza G, Pende V, Monsellato I (2010) Minimally invasive robot—assisted ColoTMEs robot surgery, Book edited by: Seung Hyuk Baik, January 2010, INTECH
Giulianotti PC, Coratti A, Angelini M et al (2003) Robotics in general surgery: personal experience in a large community hospital. Arch Surg 138:777–784
Van der Pas MH, Deijen CL, Abis GS, de Lange-de Klerk ES, Haglind E, Fürst A, Lacy AM, Cuesta MA, Bonjer HJ, COLOR II study group (2016) Conversions in laparoscopic surgery for rectal cancer. Surg Endosc 31:2263–2270
Allaix ME, Furnée EJ, Mistrangelo M, Arezzo A, Morino M (2016) Conversion of laparoscopic coloTME for cancer: what is the impact on short-term outcomes and survival? World J Gastroenterol 22(37):8304–8313
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213
Woeste G, Bechstein WO, Wullstein C (2005) Does telerobotic assistance improve laparoscopic colorectal surgery? Int J Colorectal Dis 20:253–257
Delaney CP, Lynch AC, Senagore AJ, Fazio VW (2003) Comparison of robotically performed and traditional laparoscopic colorectal surgery. Dis Colon Rectum 46(12):1633–1639
Rockall TA, Darzi A (2003) Robot-assisted laparoscopic colorectal surgery. Surg Clin North Am 83:1463–1468
Kim YS, Kim MJ, Park SC, Sohn DK, Kim DY, Chang HJ, Nam BH, Oh JH (2016) Robotic versus laparoscopic surgery for rectal cancer after preoperative chemoradiotherapy: case-matched study of short-term outcomes. Cancer Res Treat. 48(1):225–231
Park EJ, Cho MS, Baek SJ, Hur H, Min BS, Baik SH, Lee KY, Kim NK (2015) Long-term oncologic outcomes of robotic low anterior resection for rectal cancer: a comparative study with laparoscopic surgery. Ann Surg 261(1):129–137
Yoo BE, Cho JS, Shin JW, Lee DW, Kwak JM, Kim J, Kim SH (2015) Robotic versus laparoscopic intersphincteric resection for low rectal cancer: comparison of the operative, oncological, and functional outcomes. Ann Surg Oncol 22(4):1219–1225
Gorgun E, Ozben V, Costedio M, Stocchi L, Kalady M, Remzi F (2016) Robotic versus conventional laparoscopic rectal cancer surgery in obese patients. Colorectal Dis 18:1063–1071
Cho MS, Baek SJ, Hur H, Min BS, Baik SH, Lee KY, Kim NK (2015) Short and long-term outcomes of robotic versus laparoscopic total mesorectal excision for rectal cancer: a case-matched retrospective study. Medicine (Baltimore). 94(11):e522
Xiong B, Ma L, Huang W, Zhao Q, Cheng Y, Liu J (2015) Robotic versus laparoscopic total mesorectal excision for rectal cancer: a meta-analysis of eight studies. J Gastrointest Surg 19(3):516–526
Pai A, Melich G, Marecik SJ, Park JJ, Prasad LM (2015) Current status of robotic surgery for rectal cancer: a bird’s eye view. J Minim Access Surg 11(1):29–34
Hellan M, Ouellette J, Lagares-Garcia JA, Rauh SM, Kennedy HL, Nicholson JD, Nesbitt D, Johnson CS, Pigazzi A (2015) Robotic rectal cancer resection: a retrospective multicenter analysis. Ann Surg Oncol 22:2151–2158
Sun Y, Xu H, Li Z, Han J, Song W, Wang J, Xu Z (2016) Robotic versus laparoscopic low anterior resection for rectal cancer: a meta-analysis. World J Surg Oncol. 14(1):61
Melich G, Hong YK, Kim J, Hur H, Baik SH, Kim NK, Sender Liberman A, Min BS (2015) Simultaneous development of laparoscopy and robotics provides acceptable perioperative outcomes and shows robotics to have a faster learning curve and to be overall faster in rectal cancer surgery: analysis of novice MIS surgeon learning curves. Surg Endosc 29(3):558–568
Lee SH, Lim S, Kim JH, Lee KY (2015) Robotic versus conventional laparoscopic surgery for rectal cancer: systematic review and meta-analysis. Ann Surg Treat Res 89(4):190–201
Moghadamyeghaneh Z, Masoomi H, Mills SD, Carmichael JC, Pigazzi A, Nguyen NT, Stamos MJ (2014) Outcomes of conversion of laparoscopic colorectal surgery to open surgery. JSLS 18(4):e2014.00230 10
Speicher PJ, Englum BR, Ganapathi AM, Nussbaum DP, Mantyh CR, Migaly J (2015) Robotic low anterior resection for rectal cancer: a national perspective on short-term oncologic outcomes. Ann Surg 262(6):1040–1045
Wang Y, Zhao GH, Yang H, Lin J (2016) A pooled analysis of robotic versus laparoscopic surgery for total mesorectal excision for rectal cancer. Surg Laparosc Endosc Percutan Technol 26:259–264
Yang Y, Wang F, Zhang P, Shi C, Zou Y, Qin H, Ma Y (2012) Robot-assisted versus conventional laparoscopic surgery for colorectal disease, focusing on rectal cancer: a meta-analysis. Ann Surg Oncol 19(12):3727–3736
Jane D, Pigazzi A, Marshall H, Croft J, Corrigan N et al (2017) Effect of robotic assisted vs conventional laparoscopic surgery on risk of conversion to open laparotomy among patients undergoing resection for rectal cancer. JAMA 318(16):1569–1580
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Research involving human participants and/or animals
We declare that the study has been conducted according to GCP and ethical standard with no adoption of human or animal source of experimental investigation. This is a retrospective study.
Informed consent
Informed consent was obtained by all patients as per local protocol.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mégevand, J.L., Lillo, E., Amboldi, M. et al. TME for rectal cancer: consecutive 70 patients treated with laparoscopic and robotic technique—cumulative experience in a single centre. Updates Surg 71, 331–338 (2019). https://doi.org/10.1007/s13304-019-00655-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13304-019-00655-y