
Abstract
Seawater intrusion is a growing pressure in coastal communities worldwide, putting millions of people at risk of excess salinity in drinking water. This study examines the impact of saline water on people's health and labor allocation as potential pathways towards chronic poverty. Using a transdisciplinary approach based on a coupled human-water system framework, we test these linkages combining field data on well water salinity levels and rich household survey data in coastal Tanzania. The results suggest that increased salinity levels lead to more time spent collecting drinking water and an increase in illnesses. Moreover, households in poorer villages with weaker public infrastructure have limited access to alternative sources of drinking water, making them more vulnerable to scarce potable water resources stemming from high salinity. To prevent chronic poverty, communities vulnerable to saline drinking water need better adaptation strategies as well as groundwater monitoring and management.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
More than two billion people around the world are still lacking safely managed drinking water (WHO 2022). Climate change is exacerbating this problem by prolonged droughts and less predictable water availability (UNESCO 2020). Developing countries are facing growing challenges linked to water pollution problems stemming from multiple sources, making the increasingly scarce water unsafe. In particular, many rural parts of Sub-Saharan Africa lack capital for water infrastructure investment and water management institutions are weak (Comte et al. 2016; Nkiaka et al. 2021). Lack of safe drinking water negatively impacts people’s health and labor productivity threatening sustainable development (e.g., Cuevas et al. 2019). Recognizing this need, Sustainable Development Goal 6 (United Nations 2018) aims to ensure access to safe water for all, including addressing water quality problems. However, the need to better understand the linkages between groundwater quality and people’s welfare has been identified as an important knowledge gap hindering progress towards water, poverty, and gender inequality (Katuva et al. 2020).
One growing global drinking water problem affecting coastal areas worldwide is salinization (e.g., Werner et al. 2013; Idowu and Lasisi 2020; Agoubi 2021; Cao et al. 2021). Drinking water wells along the coast are especially susceptible to salt water intrusion, a situation where a salt water wedge moves inland and creates a saline mixing zone that can render the water unpotable (e.g., Greene et al. 2016). The extent of salt water intrusion is influenced by groundwater flux, hydrologic conductivity, and heterogeneity of coastal deposits (Essink et al. 2001; Sappa et al. 2015; Michael et al. 2016). Within a given aquifer, wells closer to the coast and aquifers with low groundwater flows and more permeability are more susceptible to salt water intrusion.
Salt water intrusion is also frequently associated with overpumping. In unconfined aquifers, which are common sources of drinking water in sandy deposits along the coast, overpumping lowers the water table and captures groundwater flow that would otherwise move to the shore (Sappa et al. 2015). Hydrologic drought, which reduces groundwater recharge, can also reduce thickness of the freshwater zone and accelerate salt intrusion (e.g., Taylor et al. 2013; Tully et al. 2019). With possible rises in sea level in eastern Africa of 3–8 mm/year, intrusion is more likely to extend inland where low-lying coastal areas are likely to experience significant inundation (Comte et al. 2016). Higher annual temperature and prolonged droughts are also likely to exacerbate the problem.
This increasingly widespread problem of saline drinking water can become a source of chronic poverty in coastal areas. Groundwater may become unsafe for human consumption and no longer suitable for irrigation purposes as it can reduce soil fertility, adversely impacting agricultural production and food security (Majeed and Muhammad 2019). Excess salinity in drinking water can cause health issues, especially during pregnancy and infancy (e.g., Dasgupta and Wheeler 2016; Damania et al. 2019) such as higher risks of miscarriage, preeclampsia and hypertension, leading to higher maternal and infant mortality. Additional health issues that arise from drinking saline water include headaches, diarrhea and abdominal pain (e.g., Chakraborty et al. 2019), impacting household labor and well-being.
In addition to these impacts, salinization problems can force households to spend longer time collecting water. Collecting water is a labor-intensive task, often for women, in many rural developing economies where stable water infrastructure is lacking (e.g., Graham et al. 2016). Excess salinity can cause wells to be abandoned, creating conditions where households spend more of their time traveling further in search of drinkable water. This can take time away from productive activities, education, or leisure, but also lower labor productivity, resulting in lower income and eventually constraining the households from affording better drinking water. However, there is thus far little evidence showing how saline drinking water is associated with health issues and lowers labor productivity, both of which can become pathways towards chronic poverty.
To address this gap, this study investigates the severity of the saline drinking water problem in coastal Tanzania and examines whether salinization is affecting people’s health as well as the time they spend to collect drinking water. This transdisciplinary study first describes a coupled human-water system as a conceptual framework, and then analyzes field data on well water salinity levels and household data on health and labor allocation. Overall, the study finds that higher salinity levels in well water is associated with more time spent to collect drinking water, especially for women, and a modest increase in illnesses among adult family members. The data also reveal that households in poorer villages with weaker public infrastructure have limited access to alternative sources of drinking water. Combined, these results suggest that these communities have low resilience to scarcity of potable water resources stemming from high salinity. To avoid chronic poverty, communities vulnerable to saline drinking water need appropriate adaptation strategies and better groundwater monitoring and management.
Theoretical framework
This study contributes to the growing field of socio-hydrology (e.g., Sivapalan et al. 2012; Troy et al. 2015; Blair and Buytaert 2016), which seeks to understand the dynamics and coevolution of coupled human-water systems (Sivapalan et al. 2012, 2014). In our context, the human system comprises households possessing various forms of capital including human capital (i.e., labor), a part of which is used to collect water; constructed capital (e.g., water infrastructure), and financial capital. The households’ well-being is represented by health and poverty status. This human system is intricately coupled with the dynamics of water salinization. Systemic conditions creating chronic poverty, such as a lack of water infrastructure and financial capital, also limit communities from effective water management, policies, and other interventions to mitigate or deal with water salinization. These conditions in turn increase salinity, further exacerbating poverty through a lack of potable water and its impact on health, reduced yield in agriculture, and other ways. These bidirectional interactions and feedbacks between humans and water are at the core of socio-hydrology (Blair and Buytaert 2016). Based on this simple framework, we hypothesize that saline drinking water affects people’s welfare (i.e., poverty) through health and labor allocation, and that in turn, chronic poverty constrains the quality of water infrastructure and thus limits the ways in which people can adapt to saline drinking water.
Empirically, we illustrate an approach of coupling multiple field data sources to investigate and describe a complex system whose subsystems have processes occurring at different spatial and temporal scales. In this case, the health effect of drinking saline water and the impact on labor to collect water are impacts on conditions and decisions made at the individual and household levels on a daily basis. In contrast, groundwater salinization is a process which occurs at a larger spatial and temporal scale, influenced largely by water extraction by water users in the aquifer, sea level rise, and drought. This study contributes to the growing field of socio-hydrology by illustrating a novel way of understanding this complex system by fostering local knowledge through coupling survey data from households and key informants with field data on water salinity levels. Although the importance of using information from local communities and water users in socio-hydrogeology research has been widely recognized (e.g., Re 2015; Re et al. 2021), studies using such methods have only started to grow recently.
Materials and methods
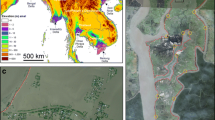
We conduct this study in Tanzania, where nearly half of its 57 million people do not have improved access to safe and clean water (UNICEF 2021). We use coupled data of water samples from drinking water wells with detailed panel household surveys implemented in 2016–2017 from 156 households in 14 subvillages in two districts, Pangani (located in Tanga region) and Rufiji (located in Pwani region), in rural coastal Tanzania (Fig. 1). The study period coincided with a prolonged drought and many wells displayed elevated salinities. Both types of field data were collected three times in 2016–2017 (August 2016, February and May 2017) to account for seasonal variation in rainfall. August is typically during the long dry season, while February is typically the period immediately following the short rain season and May is in the middle of the long rain season. In 2017, some villages did not experience the short rain season, resulting in a prolonged dry season when the second-round survey was conducted (Famine Early Warning Systems Network 2017).

Study site, location of surveyed households and wells, and photos of the most common type of wells in each region. Notes The maps were created using GPS coordinates from field data. The data for mangrove cover is from the Global Distribution of Mangroves USGS dataset (Giri et al. 2011), which can be downloaded from data.unep-wcmc.org/datasets/4. The photos show the most common type of wells in each region—a concrete-lined, permanent well in Pangani and an unlined, shallow, hand-dug well in Rufiji
Study regions
We conducted our study in 14 villages in coastal Tanzania, six of which are located in the Pangani and eight in the Rufiji (Fig. 1). All villages are located in sandy unconfined coastal plain aquifers of Cenozoic origin, which generally have good water quality but are susceptible to salt water intrusion (Sangea et al. 2018). All sample villages are located in rural remote areas characterized by chronic poverty, which is revealed in multidimensional ways (World Bank 2018). Overall, Rufiji has a higher incidence of poverty, and is more severely lacking in public infrastructure compared to Pangani. Access to basic infrastructure for drinking water, sanitation, and electricity are lacking, and the use of petroleum products for cooking, lighting, pumps, or generators is rare (Appendix S2, Table S1).
Data sources
Precipitation data
We obtained insights into the drought status of the two study regions using monthly precipitation data and monthly estimates of the Palmer Drought Severity Index (PDSI, Palmer 1965) from the 35 years (1981–2017) preceding the site investigations. The data (ERA5) from 1981 to 2017 were obtained from the Copernicus Climate Change Service (C3S) (Hersbach et al. 2019; Appendix S1).
Water sampling
We surveyed 70 drinking water wells (30 wells in Pangani, 40 wells in Rufiji) currently in use in the 14 sampled subvillages in each season. We obtained data on GPS coordinates, construction materials, surface area, well depth, depth to water, and the salinity levels (electrical conductivity measurements) at the surface and bottom of the wells (Appendix S3, Table S2.1 and S2.2). Water electrical conductivity ranges from < 500 μS/cm to > 25,000 μS/cm for freshwater and seawater, respectively, and is widely used for assessing salt water intrusion (e.g., Beaujean et al. 2014). We used a YSI Pro30 meter to measure electrical conductivity and temperature of the well water and then compensated for temperature to obtain specific conductance at 25 °C (YSI 2011). Salinity was then obtained as described in Standard Methods for the Examination of Water and Wastewater (APHA 1999). Key informants, who were members of the village water committees identified via the Village Executive Officers, provided information on the dates of construction, approximate number of households using the wells, and if applicable, the approximate date that the water within the well first tasted salty (Appendix S4).
A salinity health threshold, which was compared to our series of electrical conductivity field measurements, was derived from the World Health Organization (WHO)’s recommendation (WHO 2012). Sodium intake is used as a health risk indicator because of the adverse impacts of hypertension, which is one of the strongest risk factors for cardiovascular disease. The WHO recommends that the daily intake of sodium, from all sources, should not exceed 2 g/day (WHO 2012). We assume drinking water to be the only source of sodium intake and use this recommendation in calculating an upper conductivity (parts per thousand; ppt) threshold. This threshold is more conservative compared to another empirical study of saline coastal wells in villages in Bangladesh, which recommended that the daily intake of sodium should not exceed 2.33 g/day (Khan et al. 2011).
Based on previous studies (Besa 2013; Sappa et al. 2015; Mahenge et al. 2018—Appendix S3), we assumed that the salinity in the coastal wells was due to salt water intrusion from the adjacent marine waters and contained the same relative concentrations of sodium to total salt content (0.308 g sodium per gram of seawater salt (Turekian 1968). Thus, 2 g/day of sodium is obtained by ingesting 6.49 g of seawater salt per day. Based on the approach of Khan et al. (2011) and WHO (2012), we assumed that people consume 2 L of drinking water per day, which yields a threshold of 3.25 g of salt/liter (3.25 ppt). To put these higher values in greater context, a study of more than 2100 drinking water sources in the U.S. found that less than 0.1% had sodium concentrations equivalent to a salinity greater than 3.25 ppt (WHO 1979).
Household survey data
Household surveys were designed to elicit information related to drinking water sources and perceptions of water quality and quantity, labor allocation, livelihoods, and a suite of poverty indicators (Appendix S4). The 14 subvillages were selected randomly by applying population proportional to size sampling (United Nations 2008). In each subvillage, ten households were randomly selected from village rosters with replacement households for attrition. The key variables from the survey used in this study include the time that the households spent collecting water, perceptions about how water tastes, primary water source(s), and whether or not a household member experienced health problems that limited the adult member from work (Table S3). We aggregate the well data at the subvillage level and then couple it with the household survey data to compare measurements at the wells and households’ perceptions of water quality. The survey also included an open-ended, contingent valuation question to measure willingness to pay to make their drinking water taste less salty (Appendix S4).
Regression analyses
The goals of the regression analyses are to identify (1) the relationship of drinking water salinity level on health, and (2) how households change their labor supply for drinking water collection with increasing salinity level. Salinity level should be exogenous to households because households do not cause salinization directly. However, there are a few identification problems. First, people’s health status and labor supply can change for a variety of reasons other than excess salinity levels. Second, the salinity levels measured at each well do not necessarily equate to individuals’ exposure because people can adapt by taking measures (i.e., using water from other sources) to reduce their exposure. Moreover, individuals who have taken measures to reduce exposure to salinity in drinking water may do so because they are wealthier, better informed, have access to healthcare, or just have greater cause for concern about their health. Because of these potential problems, a simple comparison of households who live in subvillages with high salinity levels versus low sanity levels confounds the effect of salinity with these other factors.
To deal with these confounding factors, we use panel data methods (Wooldridge 2010) to estimate the impact of salinity levels on households’ health and labor supply for collecting water, carefully controlling for confounding factors that can potentially bias the coefficient estimates such as access to healthcare. We also compare panel data models with alternative specifications controlling for these confounding factors in different ways.
Specifically, the first key outcome we model is hardships in health. The survey asks ‘In the past 3 months, did member j have health problems that limited the kind or amount of work member j could do?’ We hypothesize that the level of salinity positively correlates with the number of adult members of the household having health problems. To estimate the effect of salinity on health at the household level, we estimate the following equation:
where \({HardshipHealth}_{it}\) is the dependent variable measuring the proportion of adult members in household i having health problems that limit the amount of work they can normally perform in the past three months leading up to the survey in season t. The key explanatory variable of interest is \({Salinity}_{it}\), is the average salinity concentration of all functioning drinking water wells in each subvillage of household i. In our most robust model, we control for all time-invariant household characteristics using household fixed effects (\({\alpha }_{i}\)). As an alternative specification, we estimate Eq. (1) with observable household characteristics (age, education attainment, and sex of the household head). \({\varepsilon }_{it}\) is idiosynchratic error term. The coefficient of interest is \({\gamma }_{1}\), which measures the effect of salinity on the health outcome.
The second key outcome variable is water collection time per capita. For each household member, we ask ‘In the past 7 days, how many minutes did member j spend time fetching water?’ We then aggregate the duration across all members in the household, and divide the total by the household size. We hypothesize that higher levels of salinity in drinking water increases the time the households spend in fetching water. To test this hypothesis, we estimate the following equation:
where \({TimeWater}_{it}\) is the labor (minutes) that household i spend in fetching water per week per capita in season t. Equation (2) is estimated with either a set of observable household characteristics (age, education attainment, and sex of the household head) or household fixed effects. We are interested in the estimated coefficient on Salinityit, which measures the effect of salinity in labor for water collection.
Finally, in addition to the household-level analyses, we leverage data for each individual household member level and estimate Eqs. (1) and (2) to test whether there is differential impact of saline water by sex (Appendix S6). All regression models were estimated as linear regressions using Stata 16 (StataCorp 2019). In all models, the robust standard errors are clustered at the subvillage level to reflect the sampling framework.
Results
Drought status
Our analyses of precipitation data (1981–2017, Appendix S1) in coastal Tanzania show signs of prolonged drought likely to have contributed to excess salinity in well water (Hersbach et al. 2019). During the decade leading up to 2016, both districts experienced prolonged periods of hydrologic drought (Fig. 2a and b). Rufiji had 7 out of 10 years with below-normal annual rainfall; Pangani had 9 out of 10 years below normal—in fact, rainfall was below normal eight years in a row (Fig. 2a). Moreover, the monthly average rainfall in the recent decade was below the 30-year normal in 10 out of 12 months in Rufiji and 9 out of 12 months in Pangani (Fig. 2b). The pattern of rainfall between 1981 and 2010 was periodically punctuated by years with high precipitation (e.g., > 1 SD above the mean) that can generate groundwater recharge, but no high precipitation years occurred in the decade preceding the study. These findings are consistent with PDSI, which also suggest that this period was the most extensive and severe drought during the 116 years of record (Appendix S1).

a Annual mean precipitation for Rufiji and Pangani Districts compared to the 30-year normal, 2007–2016. Note The 30-year normal for each district is calculated as the mean of annual rainfall between 1981 and 2010. b Monthly mean precipitation for Rufiji and Pangani Districts compared to the 30-year normal, 2007–2016. Note The 30-year normal for each month in each district is the mean of monthly rainfall between 1981 and 2010
Well structures and drinking water sources
All villages of both regions are immediately adjacent to the shoreline, on level terrain, and most of the wells are located 50–300 m from the shore. The data reveal wide regional differences in the structure of the drinking water wells, reflecting the extent of water infrastructure development (Fig. 3). The village wells in Pangani are more permanent in nature with 75% lined with either concrete or brick casing and 13% had a hand pump or piped faucet. The water column in the Pangani village wells was less than 5 m and many had less than 3 m of water within the well. Hand pumps have been found to fail for numerous reasons, including limited water column depths as well as poor condition of the hand pump components (MacAllister et al. 2022, Appendix S7). In situations of lower transmissivity, new wells or abandoned ones may respectively increase or reduce salt water intrusion, but the coastal aquifers in both study areas are dominated by coarse sands reducing these effects.

Regional comparison of well structure. Data: Authors’ well survey
In contrast, nearly 80% of the wells in Rufiji District were temporary, open, hand dug pit wells, and approximately half were less than two years old. Pumps were absent from all but one of the wells in the Rufiji region. These distinctions in well construction in the study regions correspond with differences in the depth of water within the wells. The Pangani wells had several meters of waters from the well bottom to the surface of the water; in contrast, the Rufiji wells were much shallower with most containing < 0.5 m of water in the wells. Although none of the wells in the two regions were greater than 10 m deep from the ground surface, we refer to the unlined pit wells of Rufiji that were less than 3 m as “shallow wells”.
The distinct well construction methods in the two regions reflect the differences in the severity of drought and the ways in which communities have adapted. Based on long-term PDSI records, the Rufiji area experienced prolonged periods of severe drought more frequently than Pangani. The Pangani area experienced mild and severe drought for only 21 and 5% of the period of record, respectively, with no severe droughts between 1917 and 1996. In contrast, the Rufiji area was classified as experiencing mild or severe drought in 66 and 25% of the 116 years of record, respectively. The majority of the Pangani wells extend deeper into the groundwater, reflecting an investment predicted on long-term use while most in Rufiji were temporary, subject to frequent flooding due to the low-lying topography. However, they are also well suited to take advantage of the shallow freshwater lens that can develop above saline groundwater in coastal aquifers. We frequently observed abandoned dug wells in Rufiji during our fieldwork (Appendix S7). The household survey data confirmed these regional differences in the sources of drinking water and further reflected differences in poverty and seasonal variation (Fig. S1, Appendix S5).
Water salinity levels and comparison with household perceptions
The water salinity levels varied significantly between the two regions, in part reflecting the depth of water within the wells (Fig. 4). In August 2016, 21% of the wells sampled in Pangani and 8% in Rufiji exceeded the salinity threshold of 3.25 ppt, with levels in several of those wells exceeding 6.4 ppt. Similarly, in February 2017, 24% of the wells in Pangani exceeded the salinity health threshold, with a couple registering levels exceeding 12.8 ppt (comparable to a mixture composed of approximately one third seawater.) In contrast, only 4% of the wells in Rufiji exceeded the salinity health threshold. In May 2017, 26% of the wells in the Pangani region exceeded the salinity threshold while all the samples from Rufiji were below the threshold. Among the high salinity wells in Pangani, 11.1% had salinity between 6.4 and 12.8 ppt and 22.2% of the wells had salinity > 12.8 ppt.

Salinity levels of drinking water wells in Pangani and Rufiji Districts in August 2016, February and May 2017. Notes The red line indicates the threshold level of 3.25 ppt. Percentages indicate the proportion of wells exceeding this threshold. This computation excludes wells unmeasurable due to flooding or drying up
The variation in water salinity levels between the two study regions can be explained in part by the stark differences in well structure. The very shallow wells in Rufiji intercept just the top of the groundwater and are constructed to access the shallow freshwater lens that floats above saline groundwater. In contrast, Pangani is dominated by permanent deeper wells that frequently extend several meters into the groundwater and can thus intercept more saline groundwater. Therefore, it is not surprising that Rufiji wells are less saline even though Rufiji experienced more prolonged periods of drought. However, as pointed out by Michael et al. (2016), differences in the heterogeneity of the aquifer media can play a major role in the salinity patterns between the regions.
The perception of water quality from the household survey data underscores the severity of the saline drinking water (Fig. S2). In the August survey, over 60% of the sample households indicated they experienced saltiness in their primary source of drinking water. Nearly 50% of the households in Pangani and 30% in Rufiji said their water “always” tasted salty in the past four weeks, and poorer households are more likely. Households indicated few adaptation strategies (Figs. S3, S4): find or dig another well (80%), find water-logged areas (15%), and buy unbottled or bottled water (5%).
Impact of salinity on health and labor productivity
Descriptive statistics
According to our data, 21% of the adults in Pangani and 17% in Rufiji had health problems that limited them from working (Fig. 4, Table S2). On average, the proportion of adult household members with health issues limiting them from working are 0.63 adults per household (std = 0.98) in Pangani and 0.58 adults per household (std = 0.97) in the Rufiji. There was some seasonal variation, with May being the worst in Pangani while February was the worst in Rufiji.
The average water collection time per week, normalized by household size, was 131 min (std = 481) in Pangani and 77 min (std = 100) in Rufiji (Fig. 5). These differences in part reflect the differences in the well structure: fewer, permanent, fixed wells in Pangani as compared to a greater number of temporary shallow wells in Rufiji; the shallow wells in Rufiji are closer to people’s homes on average than compared to the permanent wells in Pangani. The task of collecting drinking water is primarily performed by female adults in their 20 and 30 s, the age range associated with the most productive in income-generating activities and hence having a high opportunity cost of time (Fig. S5). On average, females spend more time collecting water compared to males, which is consistent with the findings in previous studies (Sorenson et al. 2011; Graham et al. 2016; Das 2017; UN Women 2018; Ngarava et al. 2019), but the differences vary across seasons (Fig. S6). Both females and males contribute to water collection during the driest season (August), but females contribute more during the wetter seasons (February and May) (Table S4, S5.1). The distribution by age (Table S5.1) suggests that children contribute only a small share of labor, which differs from other settings where water is collected mostly by children (e.g., Pickering and Davis 2012; Geere and Cortobius 2017; Levison et al. 2018). The likelihood of illnesses were statistically the same between sex (Table S5.2).

Adults with health issues preventing them from work (A) and labor time to collect water (B). A Proportion of adults in the household with health issues preventing them from work in the past four weeks (per capita), by study region and survey round. B Natural log of household labor supply to collect water, by study region and survey round
Regression analyses results
We find that higher salinity level in well water is associated with more adults with health problems preventing them from working (Table 1, Panel A). Based on Model (4), which is the most robust (Appendix S6), a one standard deviation increase in salinity level (+ 1.29 ppt) is associated with a 3.3 percentage point increase in proportion of adult household members having a health problem. For an average household, a two standard deviation (+ 2.58 ppt) increase in salinity would increase the expected mean of proportion of household members with an illness from 15 to 19%. This magnitude suggests that the problem of saline drinking water has a moderate effect on the available adult household labor, undermining productive activities of the households.
We find consistent evidence that higher salinity is associated with longer time to collect water (Table 1, Panel B). Based on model (4), a one standard deviation increase in salinity level is associated with on average a 13-min increase in weekly labor to collect water per capita. This is substantial given that the mean weekly labor to collect water is 99 min (SD = 323), suggesting that a one standard deviation increase in salinity level is equivalent to about a + 13% increase in water collection time. For a household with five household members, a two standard deviation (+ 2.58 ppt) increase in salinity would increase the expected mean of total labor to collect water by one hour and 24 min (84 min). This additional time required for water collection reduces the amount of water that can be collected per hour of labor. It also takes time away from productive livelihood activities, time for education, as well as leisure, rest, and personal care. At an annual level, this would add up to nearly two weeks’ worth of labor, assuming a 40-h work week.
The individual-level analyses reveal some differences in these effects by sex. Females are more likely to have illness preventing them from working (Table 2, Panel A, Models (1) and (2)). In our preferred specification with individual fixed effects, we still find that salinity is associated with higher likelihood of having illness preventing adults from working, but there is no differential effect by sex (Models (3 and (4)). In comparison, we find evidence that higher salinity is associated with more time spent collecting water for females (Model 3). Based on the computed implied effect, a 1% increase in salinity level is associated with 25 more minutes per week for females. This is a stark contrast to the impact on males’ labor for collecting water, which is 12 min per week on average (Panel B, Model (4)). This finding is crucial as females already spend more time collecting water (Panel B, Models (1) and (2)).
Willingness to pay (WTP) to treat saline drinking water
The survey revealed that over 70% of the households were willing to pay some amount to treat saline drinking water. The average willingness to pay in Pangani was US$1.63 per month (or US$2.48 using Purchasing Power Parity, PPP) and US$1.37 (US$2.08 in PPP) per month in Rufiji. Using the mean income per capita estimates from the Tanzania National Bureau of Statistics (2021) for each district, the WTP estimate is equivalent to about 3% of their monthly income. Compared to a recent study from Bangladesh (Das et al. 2019), these willingness-to-pay estimates are comparable in absolute terms and slightly higher in share of income. Using a revealed preference approach, Das et al. (2019) found that households were willing to pay about US$1.67 US per month (or 1% of income) to reduce salinity concentration to a permissible level.
Using these willingness-to-pay estimates, we consider the financial affordability of a small-scale rainwater harvest system. In Makabe, a coastal village near Dar es Salaam, Tanzania, a complete rainwater collection system for a 15 m2 roof area was estimated to cost approximately $260 in 2011 (Mwakapalila 2011). Using a conservative willingness-to-pay estimate of $1 per household per month, it would take just 22 households to invest in a rainwater collection system. Additionally, water treatment costs about US$0.016 per 1000 L while maintenance costs about $0.10 per 1000 L (Jing et al. 2017). Assuming a household with five members consumes 7.5 L of drinking water per day (or 2738 L per year), the annual operational cost amounts to US$0.32 per household per year, which is much within the sample households’ willingness to pay to treat saline drinking water. The potential labor savings from taking less time to fetch water would be an additional benefit of such a small-scale system.
Discussion
Although drinking saline water can be a potential source of chronic poverty, there has been no empirical evidence showing this linkage. Our study finds that higher salinity levels in well water is associated with more time required to collect drinking water, and with more illnesses among adults preventing them from working.
We found a disproportionately larger impact on females’ labor, which could further reinforce gender inequality given the burden females already bear for household tasks such as water collection and caring for family members with illnesses caused by water supply and sanitation issues (Graham et al. 2016; Nkiaka et al. 2021). This, in turn, can also diminish the amount of time that females have to engage in other income generating activities. A recent review article (Ho et al. 2021) highlights the results of eight empirical studies, which found that women were either late to work or missed it completely due to water collection obligations. We did not find a differential impact on females’ health, which is in contrast to a cohort study conducted in Bangladesh by Scheelbeek et al. (2017). Although our study did not have data on specific health conditions, health assessment data through anthropometry and blood pressure measurements (e.g., Nahian et al. 2018) could improve future studies on excess water salinity and health impacts. However, other studies (Geere et al. 2010; Ho et al. 2021) have documented the adverse physical health effects (e.g., headaches, neck/spinal pain, fractured bones, etc.) of frequently carrying heavy loads of water. These physical health consequences could also negatively impact females’ abilities to perform other important livelihood and household tasks, especially if they are required to travel greater distances with these heavy water loads as sources of potable water become scarcer.
There are a few limitations to the empirical approach. This study employed a multi-stage sampling approach to ensure that results were representative of the area and generalizable. However, disadvantages of this approach may include difficulties in linking households with specific wells, and incomplete information about how many households utilize specific wells. We therefore complemented these surveys with interviews with key informants who provided details on each well (Appendix S4). An alternative approach may be to interview water collectors at the point of the wells. Although it may be costly, such an approach would allow collection of detailed information about the usage of the well and perceptions about the water of the specific well. Fostering direct engagement with experts and water users with local knowledge by administering interviews during the in-situ measurements is a useful way of understanding coupled systems in socio-hydrogeology. Additionally, such an approach could also allow to collect gender-disaggregated data and thus have more information on the gendered-impact of groundwater salinization.
The findings from this research call for practical, long-term solutions to tackle the saline drinking water problem and meet water consumption needs. The saline well water is suitable for basic hygiene, but low salinity water is required to meet recommended daily consumption (cooking and drinking). The World Health Organization recommends water supplies for daily consumption should exceed 7.5 L per capita per day for people engaged in manual labor in hot (> 32 °C) conditions, with daily collection times of 5–30 min (Howard et al. 2003). Our study demonstrated that numerous wells had elevated salinity levels, and dry season (August 2016) collection times exceeded 60 min/day in approximately 75% of all households in both regions (Fig. 4b), suggesting the need for additional water sources. Using a value of five members per household (Table S3) and 30–100 households per well (Tables S2.2 and S2.3), a water supply that supplies the most basic consumption requirements could be addressed by either the creation of multiple community water systems that can generate 1000–4000 l/day in close proximity to households or distributed approaches where smaller, individualized water sources are a ubiquitous feature of the villages. However, any efforts that increase groundwater withdrawals in close proximity to the coast (where the villages are located) could exacerbate the risk of salt water intrusion adding further value to considerations of alternative methods.
Our study suggests that households are willing to pay for treating saline water, and that collectively, they may be able to afford a simple technology such as a small-scale rainwater harvesting system combined with household cisterns. These systems typically consist of an impermeable rooftop collection area (zinc, concrete, tile, or galvanized iron) that feeds into a collection tank. More than a million rainwater harvesting cisterns have been constructed in semi-arid portions of Brazil (Gomes et al. 2014) using 16 m3 storage tanks. Storage tanks are constructed of local materials (e.g., brick, mortar, stucco) while systems in Nigeria (Shittu et al. 2012) and Bangladesh (Biswas and Mandal 2014) rely on smaller plastic tanks (2–3 m3) that augment or supply the most basic needs. With 1000 mm/year of rainfall and a collection efficiency of 0.8–0.9 (Mwakapalila 2011; Biswas and Mandal 2014), even modest rooftop collection areas (e.g., 15 m2) should provide sufficient water to sustain household water consumption needs during the annual droughts that characterize the regions. Construction techniques for rainwater harvesting systems are relatively simple, and in several areas costs were offset by the development of trained village residents and cooperative efforts (Gera 1996).
There are other types of technology available for treating saline drinking water. However, many poorer communities may not have sufficient resources to afford larger and more efficient technologies such as photovoltaic reverse osmosis, which is gaining momentum in some parts of the world due to its output capacities and relatively low power (Greenlee et al. 2009). In reverse osmosis, the saline water source is pushed under pressure through a membrane that retains most of the salts, creating two outputs—a low salinity water supply suitable for drinking and a concentrated brine that requires disposal. Reverse osmosis systems work efficiently at the salinity concentrations found in wells of the two study regions, which are 10–30% of the salinity of seawater (Abraham and Luthra 2011). However, such systems may only be possible with robust external assistance.
Another potential barrier to the adoption of affordable technology in Tanzania and other rural coastal communities in Sub-Saharan Africa may be lack of accurate, affordable, and timely information about water quality. Local knowledge represents a largely untapped knowledge-base that can improve water quality management (Ongley 2000). With regard to risks from salinity, studies suggest that if people can taste saltiness in their water, the salinity level is well beyond safe levels. In our sample, nearly 40% of the households had never tasted saltiness in their drinking water in the past. In contrast, based on surveys in Pangani Town, where mechanized pumping wells are implicated in promoting salt water intrusion, 96% of respondents found the well water to be saline (Mahenge et al. 2018). At the village level, educational campaigns on the risks of saline drinking water could be combined with simple surveys at regular intervals that track the presence or absence of saltiness in wells. These monitoring programs need to arm local residents with approaches that simplify data management and provide education materials to residents and decision-makers in educational campaigns that also include viable, affordable water treatment alternatives (e.g., cisterns).
Conclusion
Water salinization is likely to accelerate this century with climate change through increasing drought and sea level rise, influencing the livelihoods of impoverished communities in Asia, Sub-Saharan Africa and elsewhere. Although the poorest countries in the world are facing increasing risk of water salinization, there has been no empirical evidence that increasing saline water is associated with pathways to chronic poverty. This study illustrated the severity of the saline drinking water problem and the vulnerability of the rural coastal communities with few alternative options for drinking water. We found that higher salinity in well water was associated with worse health outcomes and more labor supply to collect their everyday water, especially among females. These findings offer two potential mechanisms involving health and household labor through which higher salinity levels can lead to chronic poverty. Communities’ willingness to invest in treating saline drinking water can only be leveraged with more innovations in affordable and sustainable solutions and better monitoring of groundwater quality.
References
Abraham, T., and A. Luthra. 2011. Socio-economic and technical assessment of photovoltaic powered membrane desalination processes for India. Desalination 268: 238–248.
Agoubi, B. 2021. A review: Saltwater intrusion in North Africa’s coastal areas—Current state and future challenges. Environmental Science and Pollution Research 28: 17029–17043.
APHA. 1999. 2520 Salinity. Standard methods for the examination of water and wastewater, 20 edn.
Beaujean, J., F. Nguyen, A. Kemna, A. Antonsson, and P. Engesgaard. 2014. Calibration of seawater intrusion models: Inverse parameter estimation using surface electrical resistivity tomography and borehole data. Water Resources Research 50: 6828–6849.
Besa, M.C. 2013. Using climate information to support adaptation planning and policy-making: A practical case study in Bagamoyo District, coastal Tanzania. Stockholm Environment Institute.
Biswas, B.K., and B.H. Mandal. 2014. Construction and evaluation of rainwater harvesting system for domestic use in a remote and rural area of Khulna, Bangladesh. International Scholarly Research Notices 2014: 1–6.
Blair, P., and W. Buytaert. 2016. Socio-hydrological modelling: A review asking “why, what and how?” Hydrology and Earth System Sciences 20: 443–478.
Cao, T., D. Han, and X. Song. 2021. Past, present, and future of global seawater intrusion research: A bibliometric analysis. Journal of Hydrology 603: 126844.
Chakraborty, R., K.M. Khan, D.T. Dibaba, M.A. Khan, A. Ahmed, and M.Z. Islam. 2019. Health implications of drinking water salinity in coastal areas of Bangladesh. International Journal of Environmental Research and Public Health 16: 3746.
Comte, J.C., R. Cassidy, J. Obando, N. Robins, K. Ibrahim, S. Melchioly, I. Mjemah, H. Shauri, et al. 2016. Challenges in groundwater resource management in coastal aquifers of East Africa. Journal of Hydrology: Regional Studies 5: 179–199.
Cuevas, J., I.N. Daliakopoulos, F. del Moral, J.J. Hueso, and I.K. Tsanis. 2019. A review of soil-improving cropping systems for soil salinization. Agronomy 9: 295.
Damania, R., S. Desbureaux, A.-S. Rodella, J. Russ, and E. Zaveri. 2019. Quality unknown: The invisible water crisis. Washington, DC: World Bank.
Das, M.B. 2017. The rising tide: A new look at water and gender. Washington, DC: World Bank.
Das, D.K., M.S. Islam, S. Hadiujjaman, C.B. Dutta, and M.M. Morshed. 2019. Health cost of salinity contamination in drinking water: Evidence from Bangladesh. Environmental Economics and Policy Studies 21: 371–397.
Dasgupta, S., M. Huq, and D. Wheeler. 2016. Drinking water salinity and infant mortality in Coastal Bangladesh. Water Economics and Policy 2: 1650003.
Essink, G.H.P.O. 2001. Improving fresh groundwater supply—Problems and solutions. Ocean & Coastal Management 44: 429–449.
Famine Early Warning Systems Network. 2017. Drought conditions exacerbated by above-average surface temperatures over Eastern Horn. https://fews.net/sites/default/files/documents/reports/EA_Seasonal%20Monitor_2017_01_31_Final.pdf. Accessed 23 April 2023.
Geere, J.-A., and M. Cortobius. 2017. Who carries the weight of water? Fetching water in rural and urban areas and the implications for water security. Water Alternatives 10: 513–540.
Geere, J.A., P.R. Hunter, and P. Jagals. 2010. Domestic water carrying and its implications for health: A review and mixed methods pilot study in Limpopo Province, South Africa. Environmental Health 9: 52.
Gera, R. 1996. Rainwater harvesting and empowerment of women. In 22nd WEDC international conf. New Delhi, India. https://www.ircwash.org/sites/default/files/Gera-1996-Rainwater.pdf. Accessed 17 Oct 2021.
Giri, C., E. Ochieng, L.L. Tieszen, Z. Zhu, A. Singh, T. Loveland, J. Masek, and N. Duke. 2011. Status and distribution of mangrove forests of the world using earth observation satellite data. Global Ecology and Biogeography 20: 154–159.
Gomes, U.A., L. Heller, S. Cairncross, L. Domenèch, and J.L. Pena. 2014. Subsidizing the sustainability of rural water supply: The experience of the Brazilian rural rainwater-harvesting programme. Water International 39: 606–619.
Graham, J.P., M. Hirai, and S.-S. Kim. 2016. An analysis of water collection labor among women and children in 24 Sub-Saharan African countries. PLoS ONE 11: e0155981.
Greene, R., W. Timms, P. Rengasamy, M. Arshad, and R. Cresswell. 2016. Soil and aquifer salinization: Toward an integrated approach for salinity management of groundwater. In Integrated groundwater management: Concepts, approaches and challenges, ed. A.J. Jakeman, O. Barreteau, R.J. Hunt, J.D. Rinaudo, A. Ross, M. Arshad, and S. Hamilton, 377–412. Cham: Springer.
Greenlee, L.F., D.F. Lawler, B.D. Freeman, B. Marrot, and P. Moulin. 2009. Reverse osmosis desalination: Water sources, technology, and today’s challenges. Water Research 43: 2317–2348.
Hersbach, H., B. Bell, P. Berrisford, G. Biavati, A. Horányi, J. Muñoz Sabater, J. Nicolas, C. Peubey, et al. 2019. ERA5 monthly averaged data on single levels from 1979 to present. Copernicus Climate Change Service (C3S) Climate Data Store (CDS). https://doi.org/10.24381/cds.f17050d7. Accessed 14 Nov 2020.
Ho, E.W., S. Strohmeier-Breuning, M. Rossanese, D. Charron, D. Pennise, and J.P. Graham. 2021. Diverse health, gender and economic impacts from domestic transport of water and solid fuel: A systematic review. International Journal of Environmental Research and Public Health 18: 10355.
Howard, G., J. Bartam, A. Williams, A. Overbo, D. Fuente, and J.A. Geere. 2003. Domestic water quantity, service level and health. Geneva: World Health Organization.
Idowu, T.E., and K.H. Lasisi. 2020. Seawater intrusion in the coastal aquifers of East and Horn of Africa: A review from a regional perspective. Scientific African 8: e00402.
Jing, X., S.H. Zhang, J.J. Zhang, Y.J. Wang, and Y.Q. Wang. 2017. Assessing efficiency and economic viability of rainwater harvesting systems for meeting non-potable water demands in four climatic zones of China. Resources, Conservation and Recycling 126: 74–85.
Katuva, J., R. Hope, T. Foster, J. Koehler, and P. Thomson. 2020. Groundwater and welfare: A conceptual framework applied to coastal Kenya. Groundwater for Sustainable Development 10: 100314.
Khan, A.E., A. Ireson, S. Kovats, S.K. Mojumder, A. Khusru, A. Rahman, and P. Vineis. 2011. Drinking water salinity and maternal health in coastal Bangladesh: Implications of climate change. Environmental Health Perspectives 119: 1328–1332.
Levison, D., D.S. Degraff, and E.W. Dungumaro. 2018. Implications of environmental chores for schooling: Children’s time fetching water and firewood in Tanzania. The European Journal of Development Research 30: 217–234.
MacAllister, D.J., D. Nedaw, S. Kebede, T. Mkandawire, P. Makuluni, C. Shaba, J. Okullo, M. Owor, R. Carter, J. Chilton, and V. Casey. 2022. Contribution of physical factors to handpump borehole functionality in Africa. Science of the Total Environment 851: 158343.
Mahenge, A.S., R.R.A.M. Mato, and S. Charles. 2018. Investigation of the causes and variations of salinity in drinking water wells in Pangani Town, Tanzania. Journal of Scientific and Engineering Research 5: 357–373.
Majeed, A., and Z. Muhammad. 2019. Salinity: A major agricultural problem—Causes, impacts on crop productivity and management strategies. In Plant abiotic stress tolerance. Cham: Springer.
Michael, H.A., K.C. Scott, M. Koneshloo, X. Yu, M.R. Khan, and K. Li. 2016. Geologic influence on groundwater salinity drives large seawater circulation through the continental shelf. Geophysical Research Letters 43: 10–782.
Mwakapalila, B.H. 2011. Rooftop rainwater harvesting: A sustainable solution to water shortage problem in makabe. Master’s Thesis. Open University of Tanzania, Dar es Salaam, Tanzania.
Nahian, M.A., A. Ahmed, A.N. Lázár, C.W. Hutton, M. Salehin, and P.K. Streatfield. 2018. Drinking water salinity associated health crisis in coastal Bangladesh. Elementa: Science of the Anthropocene 6: 1–14.
Ngarava, S., L. Zhou, and N. Monde. 2019. Gendered water insecurity: A structural equation approach for female headed households in South Africa. Water 11: 2491.
Nkiaka, E., R.G. Bryant, M. Okumah, and F.F. Gomo. 2021. Water security in Sub-Saharan Africa: Understanding the status of sustainable development goal 6. Wires Water. https://doi.org/10.1002/wat2.1552.
Ongley, E.D. 2000. Water quality management: design, financing and sustainability considerations-II. In Invited presentation at the World Bank’s Water Week Conference: Towards a strategy for managing water quality management, 3–4 April 2000. Washington, D.C.
Palmer, W.C. 1965. Meteorological Drought. U.S. Department of Commerce, Weather Bureau Research Paper 45.
Pickering, A.J., and J. Davis. 2012. Freshwater availability and water fetching distance affect child health in sub-Saharan Africa. Environmental Science & Technology 46: 2391–2397.
Re, V. 2015. Incorporating the social dimension into hydrogeochemical investigations for rural development: The Bir Al-Nas approach for socio-hydrogeology. Hydrogeology Journal 23: 1293–1304.
Re, V., P. Hynds, T. Frommen, and S. Limaye. 2021. Socio-hydrogeology: uncovering the hidden connections within the Human-Groundwater Cycle, EGU General Assembly 2021, online, 19–30 Apr 2021, EGU21-493.
Sangea, H., K. Upton, B.É. Ó Dochartaigh, and I. Bellwood-Howard. 2018. Africa Groundwater Atlas: Hydrogeology of Tanzania. British Geological Survey. http://earthwise.bgs.ac.uk/index.php/Hydrogeology_of_Tanzania. Accessed 4 Feb 2022
Sappa, G., S. Ergul, F. Ferranti, L. Ngalya Sweya, and G. Luciani. 2015. Effects of seasonal change and seawater intrusion on water quality for drinking and irrigation purposes, in coastal aquifers of Dar es Salaam, Tanzania. Journal of African Earth Sciences 105: 64–84.
Scheelbeek, P.F.D., M.A.H. Chowdhury, A. Haines, D.S. Alam, M.A. Hoque, A.P. Butler, A.E. Khan, S.K. Mojumder, et al. 2017. Drinking water salinity and raised blood pressure: Evidence from a Cohort Study in Coastal Bangladesh. Environmental Health Perspectives 125: 057007.
Shittu, O.I., O.T. Okareh, and A.O. Coker. 2012. Design and construction of rainwater harvesting system for domestic water supply in Ibadan, Nigeria. Journal of Research in Environmental Science and Toxicology 1: 153–160.
Sivapalan, M., M. Konar, and V. Srinivasan. 2014. Socio-hydrology: Use-inspired water sustainability science for the Anthropocene Earth’s Future. Earth’s Future 2: 225–230.
Sivapalan, M., H.H.G. Savenije, and G. Blöschl. 2012. Sociohydrology: A new science of people and water. Hydrological Processes 26: 1270–1276. https://doi.org/10.1002/hyp.8426.
Sorenson, S.B., C. Morssink, and P. Abril. 2011. Safe access to safe water in low income countries: Water fetching in current times. Social Science and Medicine 72: 1522–1526.
StataCorp. 2019. Stata statistical software: Release 16. College Station, TX: StataCorp LLC.
Tanzania National Bureau of Statistics. 2021. 2020 Tanzania in figures. https://www.nbs.go.tz/nbs/takwimu/references/2020_Tanzania_in_Figure_English.pdf. Accessed 2 Feb 2023.
Taylor, R.G., B. Scanlon, P. Döll, M. Rodell, R. Van Beek, Y. Wada, L. Longuevergne, M. Leblanc, et al. 2013. Ground water and climate change. Nature Climate Change 3: 322–329.
Troy, T.J., M. Konar, V. Srinivasan, and S. Thompson. 2015. Moving sociohydrology forward: A synthesis across studies. Hydrology and Earth System Sciences 19: 3667–3679.
Tully, K., K. Gedan, R. Epanchin-Niell, A. Strong, E.S. Bernhardt, T. BenDor, M. Mitchell, J. Kominoski, et al. 2019. The invisible flood: The chemistry, ecology, and social implications of coastal saltwater intrusion. BioScience 69: 368–378.
Turekian, K.K. 1968. Oceans. Foundations of earth science series. Englewood Cliffs, NJ: Prentice-Hall.
UN Women. 2018. Turning promises into action: Gender equality in the 2030 agenda for sustainable development: Fact sheet—Sub-Saharan Africa. Geneva: UN Women.
UNESCO, UN-Water. 2020. United Nations World Water Development Report 2020: Water and Climate Change, Paris, UNESCO.
UNICEF. 2021. Water, sanitation and hygiene. https://www.unicef.org/tanzania/what-we-do/wash. Accessed 01 Nov 2021.
United Nations. 2008. Designing household survey samples: Practical guidelines. Department of Economic and Social Affairs, New York, Pp.240.
United Nations. 2018. Sustainable development Goal 6 synthesis report 2018 on water and sanitation. New York, USA.
Werner, A.D., M. Bakker, V.E.A. Post, A. Vandenbohede, C. Lu, B. Ataie-Ashtiani, C.T. Simmons, and D.A. Barry. 2013. Seawater intrusion processes, investigation and management: Recent advances and future challenges. Advances in Water Resources 51: 3–26.
WHO. 1979. Sodium, chlorides and conductivity in drinking-water. Report on a WHO Working Group.
WHO. 2012. Guideline: Sodium intake for adults and children. Geneva: World Health Organization.
WHO. 2022. Progress on household drinking water, sanitation and hygiene 2000–2020: Five years into the SDGs.
Wooldridge, J.M. 2010. Econometric analysis of cross section and panel data, 2nd ed., 1096. Cambridge: The MIT Press.
World Bank. 2018. Poverty and shared prosperity 2018: Piecing together the poverty puzzle. Washington, DC: World Bank.
YSI. 2011. YSI Pro30 handheld conductivity meter manual 606082A. www.YSI.com. Accessed 14 July 2021.
Acknowledgements
We thank Prof. Robert Rohli for his suggestions on the climate data sources. We also thank Lindsey West, Gumbo Majubwa, Juma Nziajose, Shafii Mohamedi, Mbwana, Boniventure Mchomvu, Temu Pastory, Glory Benny, Edmond Alavaisha, Baraka Nyangoko, Augustino Ibrahim, Verynice Temu, Omari Kigumi, Rosa Malyaga, Jamillah Kileo, Kilindimo, Rehema Mariki, Zahrie Ernst, and all of the key informant interview participants that led us around their respective villages for all of their assistance with coordination and data collection.
Funding
Funding was provided by National Science Foundation (Grant No. 1518471), University of Rhode Island’s Coastal Institute and Ministry of Education of Thailand.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wongsirikajorn, M., McNally, C.G., Gold, A.J. et al. High salinity in drinking water creating pathways towards chronic poverty: A case study of coastal communities in Tanzania. Ambio 52, 1661–1675 (2023). https://doi.org/10.1007/s13280-023-01879-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13280-023-01879-4