
Abstract
E2F activators (E2F1–3) codify a family of transcription factors (TFs) in higher eukaryotes. E2F activators are involved in the cell cycle regulation and synthesis of DNA in mammalian cells, and their overexpression has been detected in many human cancers. However, their clinical significance has not been deeply researched in non-small-cell lung cancer (NSCLC), and bioinformatics analysis has never been reported to explore their clinical role in NSCLC. In the current study, we investigated the expression and prognostic value of E2F activators in NSCLC patients through the “TCGA datasets” and the “Kaplan-Meier plotter” (KM plotter) database. Hazard ratio (HR), 95 % confidence intervals, and log-rank P were calculated. Compared with normal tissue samples, E2F activators were overexpressed in NSCLC tissues, in lung adenocarcinoma (LUAD) tissues, and in lung squamous cell carcinoma (LUSC) tissues. In NSCLC patients, E2F1 expression was significantly correlated with age, sex, and tumor stage. E2F2 expression was found to be significantly correlated with sex and tumor size. We further demonstrated that E2F1 and E2F2 overexpressions were significantly associated with poor prognosis. In LUAD patients, E2F1 expression was significantly correlated with tumor size and tumor stage. E2F2 expression was significantly correlated with lymph node status and tumor stage. E2F1 and E2F2 overexpression showed a significant association with poor prognosis, while E2F3 overexpression was significantly correlated to better prognosis. In LUSC patients, E2F1 was concluded to be significantly correlated with tumor stage. However, E2F activators were not found to be correlated to prognosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lung cancer, also known as bronchopulmonary carcinoma, is one of the common malignancies and the leading cause of cancer-related death worldwide [1]. Two main histological types are included: non-small-cell lung cancer (NSCLC) and small-cell lung cancer (SCLC). NSCLC which contains adenocarcinoma, squamous cell carcinoma, and large cell carcinoma accounts for approximately 85 % of all lung cancers [2]. Despite that the diagnostic and treatment methods have undergone considerable advancements, prognosis of NSCLC is still unfavorable, with an overall 5-year survival rate less than 15 % [2, 3]. Therefore, in order to provide better prognostic prediction and individualized treatments, further investigation on identification of prognostic markers and potential drug targets is eagerly needed.
Similar to many other carcinomas, NSCLC occurrence and development are closely related to abnormal cell cycle regulation [4, 5]. The timing of the cell to proliferate, to enter into reversible quiescence, to differentiate, or to die is controlled by the cell cycle clock apparatus [6]. Deregulation of the cell cycle process is a necessary step in malignant transformation [7].
The E2F activators (E2F1–3), belonging to the E2F family of transcription factors (Table 1) [8–12], play an important role in controlling the cell cycle, proliferation, differentiation, and apoptosis [13–17]. They were thought to determine the timing of the G1/S transition [18, 19]. An experiment done on mice demonstrated that the higher expression of E2F activators leads to the higher expression of E2F target genes and spontaneous cancer formation [17]. Deregulated expression of E2F activators has been observed in several human malignancies and has been found in bladder, breast, ovarian, and prostate cancers; gastrointestinal carcinomas; and lung cancer [20–26]. Although high-level expression of E2F activators and their relationship with clinicopathological features and prognosis have been partly reported in human NSCLC [24–26], to the best of our knowledge, the bioinformatics analysis has never been used to explore the role of E2F activators in NSCLC.
Material and methods
Expression evaluation and analysis
In order to evaluate and analyze E2F activator expression, we used The Cancer Genome Atlas (TCGA) datasets. TCGA is a collaboration between the National Cancer Institute (NCI) and the National Human Genome Research Institute (NHGRI). The tumor and normal tissues from more than 11,000 patients have been profiled, covering 37 types of genetic and clinical data for 33 types of cancer [27]. Comprehensive profiling data have been published on cancers of the breast, ovary, skin, head/neck, lung, and other organs and will soon be available for many other cancer types. With rigorous control by the NCI and individual institutes, the data are of high quality. This makes TCGA a useful source of information for gene expression alteration [28], tumor molecular subtype classification [29, 30], and other applications.
Three datasets named TCGA_LUNG_exp_HiSeqV2-2015-02-24, TCGA_LUAD_exp_HiSeqV2-2015-02-24, and TCGA_LUSC_exp_HiSeqV2-2015-02-24 were downloaded at the website of the UCSC cancer browser (https://genome-cancer.ucsc.edu/). These datasets contain a list of cancer-related characteristic information of 1013 NSCLC tissue samples, which include 108 paired NSCLC tissue samples, 57 pairs of lung adenocarcinoma (LUAD) tissues, and 51 pairs of lung squamous cell carcinoma (LUSC) tissues, respectively. The values of E2F activator expression of the tissue samples were obtained from the file “genomicMatrix.” Then, files named “clinical_data” in datasets were used to analyze the association between the E2F activator expression and some certain clinical characteristics.
Prognosis analysis
An online database named Kaplan-Meier plotter (KM plotter) [31] was used to assess the correlation of E2F activator expression to overall survival (OS). Presently, the database has breast cancer [32], gastric cancer, ovarian cancer [33], and lung cancer [31] data. The gene expression data and overall survival information of NSCLC patients in the database are downloaded from Cancer Biomedical Informatics Grid (caBIG, http://cabig.cancer.gov/, microarray samples are published in the caArray project), the Gene Expression Omnibus (GEO, http://www.ncbi.nlm.nih.gov/geo/), and TCGA (http://cancergenome.nih.gov) [31]. The database was established using gene expression data and survival information of 1926 NSCLC patients downloaded from GEO, EGA, and TCGA. Briefly, three E2F activator submembers (E2F1, E2F2, E2F3) were entered into the database (http://kmplot.com/analysis/index.php?p=service&cancer=lung) to get Kaplan-Meier survival plots. Hazard ratio (and 95 % confidence intervals) and log-rank P were calculated and displayed on the main plots.
Statistical analysis
Three TCGA datasets and one online database mentioned above were used to extract data, analyze correlations, and evaluate different prognosis. Student’s t test and χ 2 test were performed to analyze the data using SPSS software version 22.0. P < 0.05 was considered statistically significant. The data graphs were made by GraphPad Prism 6.02 software.
Results
Analysis in TCGA datasets validates high-level expression of E2F activators in lung cancer, LUAD, and LUSC tissues
When we focused on the 108 paired NSCLC tissues (57 LUAD tissues and 51 LUSC tissues) from the three TCGA datasets, we firstly found that E2F1 was on average 1.19-fold overexpressed in lung cancer tissues (1.14-fold change in LUAD and 1.25-fold change in LUSC, all P values <0.0001) (Fig. 1a). Then, we explored the expression level of E2F2 and E2F3 in lung cancer tissues. The results demonstrated that E2F2 was on average 1.56-fold overexpressed in lung cancer tissues (1.48-fold change in LUAD and 1.64-fold change in LUSC, all P values <0.0001) (Fig. 1b) and E2F3 was on average 1.17-fold overexpressed in lung cancer tissues (1.19-fold change in LUAD and 1.16-fold change in LUSC, all P values <0.0001) (Fig. 1c).

E2F activators are highly expressed in NSCLC, LUAD, and LUSC tissues. a E2F1 is on average 1.19-fold overexpressed in lung cancer tissues, 1.14-fold changed in LUAD, and 1.25-fold changed in LUSC (all P values <0.0001). b E2F2 is on average 1.56-fold overexpressed in lung cancer tissues, 1.48-fold changed in LUAD, and 1.64-fold changed in LUSC (all P values <0.0001). c E2F3 is on average 1.17-fold overexpressed in lung cancer tissues, 1.19-fold changed in LUAD, and 1.16-fold changed in LUSC (all P values <0.0001)
E2F activator expression shows significant correlation with some certain clinical characteristics in NSCLC and subtypes
After further analyzing the file clinical_data in the three TCGA datasets, 725 patients (337 LUAD patients and 388 LUSC patients, respectively) with full-scale clinical data (age, gender, TNM stage, pathologic stage, survival information) were extracted from the 1013 patients mentioned above. Among the 725 patients, median age at the time of diagnosis was 66 years (ranging from 38 to 87 years) and 36.6 % of the patients were female. For NSCLC patients, we chose the median expression value of each E2F activator as the cutoff value, and then the patients were divided into two groups: high expression and low expression. For LUAD and LUSC patients, we used the same grouping method. Firstly, we explored the relationship between E2F activator expression and clinicopathological features in NSCLC patients and we found that E2F1 expression was significantly correlated with age (P = 0.049838), sex (P = 0.007762), and tumor stage (P = 0.023432) (Table 2). E2F2 expression was found to be significantly correlated with sex (P = 0.000003) and tumor size (P = 0.008569) (Table 3). But E2F3 expression showed no correlation with all the clinical characteristics as previously mentioned (Table 4). Then, we explored the relationship between E2F activator expression and clinicopathological features in LUAD patients and we concluded that E2F1 expression was significantly correlated with tumor size (P = 0.047061) and tumor stage (P = 0.043911) (Table 5). E2F2 expression was significantly correlated with lymph node status (P = 0.016263) and tumor stage (P = 0.007615) (Table 6). However, no significant correlation was observed between E2F3 and any clinical characteristic (Table 7). For LUSC patients, E2F1 was concluded to be significantly correlated with tumor stage (P = 0.004436) (Table 8). E2F2 and E2F3 were not correlated with the clinical characteristics as previously mentioned (Tables 9 and 10).
Different prognostic value of E2F activators in NSCLC and subtypes
We next examined the prognostic value of E2F activator expression. All E2F activator Kaplan-Meier survival information can be found in www.kmplot.com.
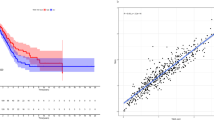
We first determined the predictive value of the expression of E2F1 in www.kmplot.com. The desired Affymetrix ID is valid: 204947_at (E2F1). Survival curves are plotted for all patients (n = 1928) (Fig. 2a), for LUAD patients (n = 866) (Fig. 2b), and for LUSC patients (n = 675) (Fig. 2c). E2F1 high expression was found to be correlated to worsen OS in all NSCLC patients followed for 200 months, hazard ratio (HR) 1.46 (1.28–1.66), P = 5e−09. E2F1 high expression was also found to be correlated to worsen OS in LUAD patients, HR 1.74 (1.37–2.21), P = 3.6e−06. However, E2F1 high expression was not found to be correlated to OS in LUSC patients, HR 1.15 (0.91–1.46), P = 0.25.

The predictive value of the expression of E2F1 in www.kmplot.com. The desired Affymetrix ID is valid: 204947_at (E2F1). E2F1 high expression is significantly associated to worsen OS in all NSCLC patients (n = 1928) (P = 5e−09) (a), as well as in LUAD patients (n = 866) (P = 3.6e−06) (b). E2F1 high expression is not associated with OS in LUSC patients (n = 675) (P = 0.25) (c)
We then determined the predictive value of E2F2 expression in www.kmplot.com. The Affymetrix ID is valid: 228361_at (E2F2). E2F2 high expression was found to be correlated to worsen OS in all NSCLC patients, HR 1.84 (1.56–2.18), P = 4.7e−13 (Fig. 3a), as well as in LUAD patients, HR 2.23 (1.73–2.87), P = 1.6e−10 (Fig. 3b), but not in LUSC patients, HR 1.01 (0.74–1.38), P = 0.93 (Fig. 3c).

The predictive value of the expression of E2F2 in www.kmplot.com. The desired Affymetrix ID is valid: 228361_at (E2F2). E2F2 high expression is significantly correlated to worsen OS in all NSCLC patients (n = 1928) (P = 4.7e−13) (a), as well as in LUAD patients (n = 866) (P = 1.6e−10) (b), but not in LUSC patients (n = 675) (P = 0.93) (c)
Figure 4 shows the predictive value of E2F3 expression in www.kmplot.com. The Affymetrix ID is valid: 203693_s_at (E2F3). E2F3 high expression was not found to be correlated to OS in all NSCLC patients, HR 0.93 (0.82–1.06), P = 0.27 (Fig. 4a), and in LUSC patients, HR 1.06 (0.84–1.34), P = 0.63 (Fig. 4c). But E2F3 high expression was found to be correlated to better OS in LUAD patients, HR 0.62 (0.49–0.79), P = 8.4e–05 (Fig. 4b).

The predictive value of the expression of E2F3 in www.kmplot.com. The desired Affymetrix ID is valid: 203693_s_at (E2F3). E2F3 expression shows no association with OS in NSCLC patients (n = 1928) (P = 0.27) (a). E2F3 high expression is significantly correlated to better OS in LUAD patients (n = 866) (P = 0.63) (b), but not in LUSC patients (n = 675) (P = 8.4e−05) (c)
Discussion
NSCLC is a highly malignant and aggressive tumor type and showed a poor 5-year survival rate [2, 3, 34]. E2F activator overexpression has been reported in many cancers in recent years, and such overexpression may promote carcinogenesis [22, 23]. Though the role of E2F activators in tumorigenesis and prognosis in several cancers has been partially researched and confirmed [23–25], the method of further bioinformatics analysis has never been reported in NSCLC. In the present study, we mainly explored the relationship between E2F activators and the clinical characteristics of NSCLC as well as the relationship between E2F activators and the OS of NSCLC. We hope that all these works will be helpful to make the previous research results abundant, design the treatment, and estimate the prognosis of NSCLC patients.
E2F1, among E2F activators, is the best studied in NSCLC [24, 35, 36]. It was reported that the overexpression of E2F1 contributes to the development of NSCLC, and this role is enhanced by the deregulated pRb-p53-MDM2 circuitry [6]. Moreover, in lung cancer, some miRNAs exert their function by regulating E2F1 [36, 37]. Furthermore, a recent experimental study showed that during the progression of NSCLC, E2F1 overexpression could produce more aggressive tumors with a high proliferation rate and chemoresistance [24]. But Volm et al. demonstrated that E2F1 showed no correlation at all with LUSC patients [38]. In our study, TCGA datasets revealed higher expression of E2F1 in NSCLC, LUAD, and LUSC tissues. Also, we demonstrated that E2F1 expression was significantly correlated with age, sex, and tumor stage in all NSCLC patients; correlated with tumor size and tumor stage in LUAD patients; and correlated with tumor stage in LUSC patients. Then, by using the KM plotter, we determined the prognostic value of E2F1 in NSCLC patients. E2F1 high expression was significantly associated to worsen OS in all NSCLC patients followed for 200 months, as well as in LUAD patients. However, E2F1 high expression was not found to be correlated to OS in LUSC patients.
The E2F2 gene is located on 1p36 [39]. It was reported that in different cancer types, E2F2 may act as either a tumor suppressor or an activator [40]. Many studies revealed that E2F2 overexpression is related to larger tumor size and advanced clinical stage in ovarian cancer [41, 42] and hepatocellular carcinoma [43]. Chen et al. indicated that E2F2 acted as a tumor activator in NSCLC and was an independent indicator for OS in NSCLC patients [25]. In our report, higher expression of E2F2 in NSCLC, LUAD, and LUSC tissues was demonstrated. Besides, E2F2 expression was found to be significantly correlated with sex and tumor size in all NSCLC patients, while E2F2 expression was significantly correlated with lymph node status and tumor stage. However, E2F2 expression showed no correlation with the clinical characteristics in LUSC patients. Furthermore, E2F2 high expression was found to be significantly correlated to worsen OS in all NSCLC patients, as well as in LUAD patients, but not in LUSC patients.
E2F3 encodes two different proteins, E2F3a and E2F3b [44, 45]. E2F3a, as well as E2F1 and E2F2, is inhibited by pRB in quiescent cells and recruits coactivators to E2f-responsive genes in G1, and its promoter is E2f-responsive. E2F3b, like E2F4 and E2F5, acts as a transcriptional repressor [46]. E2F3 overexpression is proved to be an oncogenic event during human bladder cancer [47, 48] and prostate cancer [49] development. Overexpression of E2F3 was also observed in LUAD and LUSC lung cancer patients [26]. In this report, we demonstrated the higher expression of E2F3 in NSCLC, LUAD, and LUSC tissues. But no significant correlation was observed between E2F3 and any clinical characteristic in all NSCLC patients, in LUAD patients, and in LUSC patients. We also observed that E2F3 high expression was significantly correlated to better OS in LUAD patients, but not in all NSCLC and LUSC patients. We consider that E2F3b may be responsible for the better OS in LUAD patients; however, there is no information about E2F3b that can be found in “TCGA datasets” and the “Kaplan-Meier plotter.” More research is needed to better understand the role E2F3 played in NSCLC patients.
Our results indicated that higher expression of E2F1 and E2F2 may play an important role in the malignancy of NSCLC especially in LUAD. E2F1 and E2F2 might be a useful marker for poor prognosis and a potential therapeutic target in LUAD patients. On the other hand, high E2F1 and E2F2 expression could also serve as a molecular marker to identify high-risk subgroups in LUAD patients. But in LUSC patients, no significant clinical significance was observed.
References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30.
Ramalingam SS, Owonikoko TK, Khuri FR. Lung cancer: new biological insights and recent therapeutic advances. CA Cancer J Clin. 2011;61:91–112.
Subramaniam S, Thakur RK, Yadav VK, Nanda R, Chowdhury S, Agrawal A. Lung cancer biomarkers: state of the art. J Carcinog. 2013;12:3.
Cooper WA, Lam DC, O’Toole SA, Minna JD. Molecular biology of lung cancer. J Thorac Dis. 2013;5(Suppl 5):S479–90.
Niklinski J, Niklinska W, Laudanski J, Chyczewska E, Chyczewski L. Prognostic molecular markers in non-small cell lung cancer. Lung Cancer. 2001;34(Suppl 2):S53–8.
Gorgoulis VG, Zacharatos P, Mariatos G, Kotsinas A, Bouda M, Kletsas D, Asimacopoulos PJ, Agnantis N, Kittas C, Papavassiliou AG. Transcription factor E2F-1 acts as a growth-promoting factor and is associated with adverse prognosis in non-small cell lung carcinomas. J Pathol. 2002;198:142–56.
Abreu VA, Howard MS. Tumor-suppressor genes, cell cycle regulatory checkpoints, and the skin. N Am J Med Sci. 2015;7:176–88.
Attwooll C, Lazzerini DE, Helin K. The e2f family: specific functions and overlapping interests. EMBO J. 2004;23:4709–16.
Trimarchi JM, Lees JA. Sibling rivalry in the e2f family. Nat Rev Mol Cell Biol. 2002;3:11–20.
DeGregori J, Johnson DG. Distinct and overlapping roles for e2f family members in transcription, proliferation and apoptosis. CURR MOL MED. 2006;6:739–48.
Iaquinta PJ, Lees JA. Life and death decisions by the e2f transcription factors. Curr Opin Cell Biol. 2007;19:649–57.
Dimova DK, Dyson NJ. The e2f transcriptional network: old acquaintances with new faces. Oncogene. 2005;24:2810–26.
Li J, Ran C, Li E, Gordon F, Comstock G, Siddiqui H, Cleghorn W, Chen HZ, Kornacker K, Liu CG, Pandit SK, Khanizadeh M, Weinstein M, Leone G, de Bruin A. Synergistic function of e2f7 and e2f8 is essential for cell survival and embryonic development. Dev Cell. 2008;14:62–75.
Westendorp B, Mokry M, Groot KM, Holstege FC, Cuppen E, de Bruin A. E2f7 represses a network of oscillating cell cycle genes to control s-phase progression. Nucleic Acids Res. 2012;40:3511–23.
Nakayama KI, Nakayama K. Ubiquitin ligases: cell-cycle control and cancer. Nat Rev Cancer. 2006;6:369–81.
Peart MJ, Poyurovsky MV, Kass EM, Urist M, Verschuren EW, Summers MK, Jackson PK, Prives C. Apc/c(cdc20) targets e2f1 for degradation in prometaphase. Cell Cycle. 2010;9:3956–64.
Chen H, Tsai S, Leone G. Emerging roles of e2fs in cancer: an exit from cell cycle control. Nat Rev Cancer. 2009;9:785–97.
Wu L, Timmers C, Maiti B, Saavedra HI, Sang L, Chong GT, Nuckolls F, Giangrande P, Wright FA, Field SJ, Greenberg ME, Orkin S, Nevins JR, Robinson ML, Leone G. The e2f1-3 transcription factors are essential for cellular proliferation. Nature. 2001;414:457–62.
DeGregori J, Leone G, Miron A, Jakoi L, Nevins JR. Distinct roles for e2f proteins in cell growth control and apoptosis. Proc Natl Acad Sci U S A. 1997;94:7245–50.
Santos M, Martinez-Fernandez M, Duenas M, Garcia-Escudero R, Alfaya B, Villacampa F, Saiz-Ladera C, Costa C, Oteo M, Duarte J, Martinez V, Gomez-Rodriguez MJ, Martin ML, Fernandez M, Viatour P, Morcillo MA, Sage J, Castellano D, Rodriguez-Peralto JL, de la Rosa F, Paramio JM. In vivo disruption of an rb-e2f-ezh2 signaling loop causes bladder cancer. Cancer Res. 2014;74:6565–77.
Rennhack J, Andrechek E. Conserved e2f mediated metastasis in mouse models of breast cancer and her2 positive patients. Oncoscience. 2015;2:867–71.
Shackney SE, Chowdhury SA, Schwartz R. A novel subset of human tumors that simultaneously overexpress multiple e2f-responsive genes found in breast, ovarian, and prostate cancers. Cancer Inform. 2014;13:89–100.
Suzuki T, Yasui W, Yokozaki H, Naka K, Ishikawa T, Tahara E. Expression of the e2f family in human gastrointestinal carcinomas. Int J Cancer. 1999;81:535–8.
Huang CL, Liu D, Nakano J, Yokomise H, Ueno M, Kadota K, Wada H. E2f1 overexpression correlates with thymidylate synthase and survivin gene expressions and tumor proliferation in non small-cell lung cancer. Clin Cancer Res. 2007;13:6938–46.
Chen L, Yu JH, Lu ZH, Zhang W. E2f2 induction in related to cell proliferation and poor prognosis in non-small cell lung carcinoma. Int J Clin Exp Pathol. 2015;8:10545–54.
Cooper CS, Nicholson AG, Foster C, Dodson A, Edwards S, Fletcher A, Roe T, Clark J, Joshi A, Norman A, Feber A, Lin D, Gao Y, Shipley J, Cheng SJ. Nuclear overexpression of the e2f3 transcription factor in human lung cancer. Lung Cancer. 2006;54:155–62.
Tomczak K, Czerwinska P, Wiznerowicz M. The cancer genome atlas (tcga): an immeasurable source of knowledge. Contemp Oncol (Pozn). 2015;19:A68–77.
Guo Y, Sheng Q, Li J, Ye F, Samuels DC, Shyr Y. Large scale comparison of gene expression levels by microarrays and rnaseq using tcga data. PLoS One. 2013;8:e71462.
Muzny DM, Bainbridge MN, Chang K, Dinh HH, Drummond JA, Fowler G et al. Comprehensive molecular characterization of human colon and rectal cancer. Nature. 2012;487(7407):330–337.
Koboldt DC, Fulton RS, McLellan MD, Schmidt H, Kalicki-Veizer J, McMichael JF et al. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61–70.
Gyorffy B, Surowiak P, Budczies J, Lanczky A. Online survival analysis software to assess the prognostic value of biomarkers using transcriptomic data in non-small-cell lung cancer. PLoS One. 2013;8:e82241.
Gyorffy B, Lanczky A, Eklund AC, Denkert C, Budczies J, Li Q, Szallasi Z. An online survival analysis tool to rapidly assess the effect of 22,277 genes on breast cancer prognosis using microarray data of 1,809 patients. Breast Cancer Res Treat. 2010;123:725–31.
Gyorffy B, Lanczky A, Szallasi Z. Implementing an online tool for genome-wide validation of survival-associated biomarkers in ovarian-cancer using microarray data from 1287 patients. Endocr Relat Cancer. 2012;19:197–208.
Xu MM, Mao GX, Liu J, Li JC, Huang H, Liu YF, Liu JH. Low expression of the FoxO4 gene may contribute to the phenomenon of EMT in non-small cell lung cancer. Asian Pac J Cancer Prev. 2014;15:4013–8.
Hung JJ, Hsueh CT, Chen KH, Hsu WH, Wu YC. Clinical significance of E2F1 protein expression in non-small cell lung cancer. Exp Hematol Oncol. 2012;1:18.
Tai MC, Kajino T, Nakatochi M, Arima C, Shimada Y, Suzuki M, Miyoshi H, Yatabe Y, Yanagisawa K, Takahashi T. Mir-342-3p regulates MYC transcriptional activity via direct repression of E2F1 in human lung cancer. Carcinogenesis. 2015;36:1464–73.
Gu Y, Cheng Y, Song Y, Zhang Z, Deng M, Wang C, Zheng G, He Z. MicroRNA-493 suppresses tumor growth, invasion and metastasis of lung cancer by regulating E2F1. PLoS One. 2014;9:e102602.
Volm M, Koomagi R, Rittgen W. Clinical implications of cyclins, cyclin-dependent kinases, RB and E2F1 in squamous-cell lung carcinoma. Int J Cancer. 1998;79:294–9.
Ivey-Hoyle M, Conroy R, Huber HE, Goodhart PJ, Oliff A, Heimbrook DC. Cloning and characterization of E2F-2, a novel protein with the biochemical properties of transcription factor E2F. Mol Cell Biol. 1993;13:7802–12.
DeGregori J. The genetics of the E2F family of transcription factors: shared functions and unique roles. Biochim Biophys Acta. 2002;1602:131–50.
Reimer D, Sadr S, Wiedemair A, Goebel G, Concin N, Hofstetter G, Marth C, Zeimet AG. Expression of the E2F family of transcription factors and its clinical relevance in ovarian cancer. Ann N Y Acad Sci. 2006;1091:270–81.
Reimer D, Sadr S, Wiedemair A, Stadlmann S, Concin N, Hofstetter G, Muller-Holzner E, Marth C, Zeimet AG. Clinical relevance of E2F family members in ovarian cancer—an evaluation in a training set of 77 patients. Clin Cancer Res. 2007;13:144–51.
Zhan L, Huang C, Meng XM, Song Y, Wu XQ, Miu CG, Zhan XS, Li J. Promising roles of mammalian E2Fs in hepatocellular carcinoma. Cell Signal. 2014;26:1075–81.
He Y, Armanious MK, Thomas MJ, Cress WD. Identification of E2F-3B, an alternative form of E2f-3 lacking a conserved n-terminal region. Oncogene. 2000;19:3422–33.
Leone G, Nuckolls F, Ishida S, Adams M, Sears R, Jakoi L, Miron A, Nevins JR. Identification of a novel E2F3 product suggests a mechanism for determining specificity of repression by RB proteins. Mol Cell Biol. 2000;20:3626–32.
Adams MR, Sears R, Nuckolls F, Leone G, Nevins JR. Complex transcriptional regulatory mechanisms control expression of the E2F3 locus. Mol Cell Biol. 2000;20:3633–9.
Feber A, Clark J, Goodwin G, Dodson AR, Smith PH, Fletcher A, Edwards S, Flohr P, Falconer A, Roe T, Kovacs G, Dennis N, Fisher C, Wooster R, Huddart R, Foster CS, Cooper CS. Amplification and overexpression of E2F3 in human bladder cancer. Oncogene. 2004;23:1627–30.
Oeggerli M, Tomovska S, Schraml P, Calvano-Forte D, Schafroth S, Simon R, Gasser T, Mihatsch MJ, Sauter G. E2F3 amplification and overexpression is associated with invasive tumor growth and rapid tumor cell proliferation in urinary bladder cancer. Oncogene. 2004;23:5616–23.
Foster CS, Falconer A, Dodson AR, Norman AR, Dennis N, Fletcher A, Southgate C, Dowe A, Dearnaley D, Jhavar S, Eeles R, Feber A, Cooper CS. Transcription factor E2F3 overexpressed in prostate cancer independently predicts clinical outcome. Oncogene. 2004;23:5871–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Gao, Z., Shi, R., Yuan, K. et al. Expression and prognostic value of E2F activators in NSCLC and subtypes: a research based on bioinformatics analysis. Tumor Biol. 37, 14979–14987 (2016). https://doi.org/10.1007/s13277-016-5389-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-016-5389-z