
Abstract
The inhibitor of growth family member 3 (ING3) is a member of the ING tumor suppressor family. Although its expression has been reported in various types of cancers, the role of ING3 and its prognostic value in prostate cancer (PCa) has not been investigated. ING3 expression and prognostic value was assessed in a cohort of PCa patients (n = 312) treated with transurethral resection of prostate using immumoflourescent automated quantitative analysis (AQUA) system. In vitro studies were carried out in conjunction to investigate its expression in various PCa cell lines. ING3 knockdown was also carried out in DU145 cell lines to assess for any changes in invasion and migration. ING3 expression was highest in benign prostate tissues (mean 3.2 ± 0.54) compared to PCa (mean 2.5 ± 0.26) (p = 0.437), advanced prostate cancer (AdvPCa) (mean 1.5 ± 0.32) (p = 0.004), and castration-resistant prostate cancer (CRPC) (mean 2.28 ± 0.32) (p = 0.285). ING3 expression was inversely correlated to Gleason score (p = 0.039) and ETS-related gene (ERG) expression (p = 0.019). Higher ING3 expression was marginally associated with lethal disease (p = 0.052), and this was more pronounced in patients with ERG-negative status (p = 0.018). Inhibition of ING3 in DU145 PCa cells using small interfering RNA (siRNA) was associated with decreased cell invasion (p = 0.0016) and cell migration compared to control cells. ING3 is significantly associated with PCa disease progression and cancer-specific mortality. To our knowledge, this is the first report suggesting an oncogenic function of ING3, previously well known as a tumor suppressor protein. Further studies should investigate potential-related pathways in association to ING3.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prostate cancer (PCa) is the most common malignancy in men and the second leading cause of cancer-related deaths in Western countries [1]. It is expected that one in six men will develop PCa in their lifetime [2] with estimated 233,000 new cases and 29,480 deaths to have occurred in 2014 in USA [3]. The inhibitor of growth family member 3 (ING3) is a member of the ING family type II of tumor suppressors, which represent novel tumor suppressors comprised of five conserved genes ING1–ING5 [4]. ING proteins were identified in different organisms such as mouse, frog, worms, yeast, and human. Mutations and alterations of INGs have been reported in different types of cancer [5–7].
ING3 encoding a 47 kDa protein with 418 amino acids is located on chromosome 7q31, and it is expressed in various normal human tissues and is suggested to play a role in apoptosis and cell cycle regulation [8, 9].
Recent studies have suggested that ING3 has tumor suppressor functions [5–7]. For instance, deregulation of ING3 expression has been found in human head and neck squamous cell carcinomas, hepatocellular carcinoma (HCC), and melanomas [6, 9, 10]. In another study, overexpression of ING3 in colon cancer cell lines induced apoptosis and inhibited tumor cell growth through mechanisms involving cell cycle regulation [8].
The ETS-related gene (ERG) belongs to the erythroblast transformation specific erythroblast transformation specific (ETS) family of transcription factors, which consists of 29 genes, subdivided into 13 groups [11]. ERG fusion was first described in Ewing’s sarcoma and acute myeloid leukemia [12]. The ERG gene has been reported to have a normal biological function in regulating cellular differentiation, cell growth, and angiogenesis [13].
In clinical cohorts, ERG has been proposed to be associated with specific molecular subtypes of PCa and may be of potential prognostic value, but this is not uniformly noted in all publications, [14–19].
Metastasis is one of the main hallmarks of cancer, and there are different procedures to assess metastatic potential in in vitro studies. One methodology is evaluating epithelial-mesenchymal transition (EMT) which changes the morphology of epithelial cells from firm organized to more spindle-like in order to travel to distant organs. Therefore, demonstrating levels of EMT markers such as E-cadherin, N-cadherin, Twist, and Snail in prostate cancer cell lines where ING3 is manipulated would support the role of ING3 in prostate cancer aggressiveness.
The role and function of ING3 in PCa have not yet been investigated. In this study, we investigated the prognostic value of ING3 in a cohort of prostate cancer patients treated by transurethral resection of prostate (TURP) and characterized the role of ING3 its biological role in vitro using several PCa cell lines.
Material and methods
Cell culture and transfections
Human PCa cell lines Vcap, LNCaP, PC3, and DU145 as well as immortalized prostate cell line RWPE-1 were from the American Type Culture Collection (Rockville, MD, USA) and were cultured following the manufacturer’s instructions [20–23].
To study the effect of ERG on ING3 expression, we generated stable clones of RWPE-1 and LNCaP cell lines overexpressing ERG as shown in Supplementary Fig. 1. The PC3-ERG stable cell line was obtained from Dr. Felix Feng, University of Michigan. VCaP cells were transiently transfected with either non-targeting control small interfering RNA (siRNA) or siRNA against ERG custom synthesized (GAUCCACGCUAUGGAGUA) (Sigma, St. Louis, MO, USA) using Lipofectamine RNAiMax reagent (Invitrogen, Carlsbad, CA, USA) according to the manufacturer’s protocol. To assess the functional role of ING3, we transfected DU145 (originally expressing high ING3 levels) with either siRNA against ING3 or non-targeting control siRNA using Lipofectamine RNAiMax reagent (Invitrogen).
qRT-PCR analyses
Total RNA was extracted using miRNeasy® Mini Kit (Qiagen Sciences, Maryland, USA; cat. number 1038703), and reverse transcription was performed using qScript™ cDNA SuperMix (Quanta BioSciences TM, Gaithersburg, MD, USA) by Authorized Thermal Cycle Eppendorf. The primers used for quantitative reverse transcription PCR (qRT-PCR) are listed in Supplementary Table 1. Beta glucuronidase (GUSB) was used as an internal control. Three independent experiments were performed; each one had reactions in triplicates.
Western blot analysis
Western blotting was performed as previously described in [24]. Primary antibodies used in this study are anti-ING3 (2A2) mouse monoclonal (Riabowol’s Lab, Antibody Facility University of Calgary), anti-β-Actin (Cell Signaling Technology, Danvers, MA, USA), anti-ERG (Santa Cruz Biotechnology, Santa Cruz, CA, USA), and anti-glyceraldehyde 3-phosphate dehydrogenase (GAPDH; Santa Cruz Biotechnology). The signals were detected with an enhanced chemiluminescence kit (Pierce ECL Western Blotting Substrate) (Thermo Scientific, Rockford, IL, USA).
Invasion assay
The CytoSelectTM 24-well cell invasion assay basement membrane, Flourometric Format kit (catalogue number CBA-111, Cell Biolabs Inc., San Diego, CA. USA), was used according to the manufacturer protocol to determine the invasion ability of DU145 cells after ING3 knockdown.
Wound-healing assay
A wound was created on a monolayer of confluent cells cultured in 6-well plates by scratching using a p200 pipette tip. The wounded monolayer was then washed twice with fresh cell culture media to remove debris. At that point, cell-free space was compared by images taken by Moticam Pro camera (Hong Kong, China) at different times 0, 16, and 24 h.
Clinical samples
Patients and tissue microarray construction
The study cohort consisted of 312 PCa patients treated with TURP between 2005 and 2008 at University of Calgary, Rockyview General Hospital. A total of two tissue microarray blocks were constructed with an average of two cores (0.6 mm) taken from each patient sample reflecting total Gleason score (GS). After construction, the diagnosis and GS were verified on the initial HE slides. GS was assessed using the 2005 ISUP criteria [25]. All clinical and pathological information were collected with approval of the institutional ethical review board at the University of Calgary. Patients were grouped into three categories:
-
1.
Patients with unsuspected PCa; defined as patients with no previous diagnosis of PCa, found to have PCa with GS ≤7at the time of histological examination.
-
2.
Patients with advanced prostate cancer (AdvPCa); defined as patients with no prior diagnosis of PCa, but for whom the histological findings demonstrate a GS of 8–10.
-
3.
Patients with castration-resistant prostate cancer (CRPC); defined as patients with previous diagnosis of PCa who were treated by LH-RH agonists and progressed requiring channel TURP to relieve obstructive symptoms.
A total of 615 cores from two tissue microarray (TMAs) were available. They included benign prostate tissue (n = 83), localized PCa cores (n = 233), AdvPCa (n = 173), and CRPC cores (n = 126), assembled into two TMAs.
ERG and AR protein expression assessment by immunohistochemistry
ERG immunohistochemistry was carried out as previously described [18]. Briefly, paraffin-embedded sections were placed on slides and incubated with sodium citrate buffer (10 mM pH 6.0) for 40 min. Slides were kept at room temperature to cool down for about 20–30 min. Immunohistochemistry was performed using automated Ventana autostainer. Slides were then incubated with ERG rabbit monoclonal antibody (Epitomics, clone EPR 3864) at 1:50 dilution. Androgen receptor (AR) immunohistochemistry was performed on Leica Bond Max platform (Leica Microsystems, Wetzlar, Germany). Sections were subjected to heat-induced antigen retrieval for 30 min using Leica Epitope Retrieval Solution 2. Slides were then incubated with androgen receptor mouse monoclonal antibody from Santa Cruz clone AR441 (catalogue # sc-7305) for 15 min at a 1:200 dilution. Expression of ERG and AR were assessed based on the intensity of the protein level where 0, 1, 2, and 3 were considered negative, weak, moderate, and strong protein level intensity, respectively.
Assessment of ING3 by immunoflourescent imaging system (AQUA)
ING3 protein expression was assessed by fluorescence immunohistochemical staining using an Aperio Scanscope FL (Aperio Inc., Vista, CA, USA) for the Automated Image Acquisition and Analysis (AQUA). Using this system, ING3 nuclear staining was red and counterstained blue with 4′,6-diamidino-2-phenylindole dihydrochloride (DAPI). The generated score was a percentage of the nuclear area that was positive for ING3 and nuclear staining which was stained blue by DAPI. ING3 positivity was determined based on threshold image levels to remove background. Samples were separated according to the percentage of cells expressing ING3, into two groups (≤0.15 vs. ≥0.15) based on fluorescent immunohistochemical staining of ING3 using AQUA platform. The 0.155 cutoff was determined using the Charité Cutoff Finder: http://molpath.charite.de/cutoff/index.jsp and was found to be the most significant cutoff point [26]. Further analyses were then performed based on this cutoff.
Statistical analysis
Statistical analyses were carried out using the Statistical Package for Social Sciences, version 19.0 (SPSS, Chicago, IL, USA). Graphing was carried out using the GraphPad Prism 6 software package. Two-sided Student’s t test and the Mann–Whitney test were used for statistical comparisons between controls and ERG cells. Correlations between ING3 expression and ERG, GS, tumor volume, and lethal disease were evaluated by the Spearman’s test. The Kaplan–Meier and Cox regression hazard tests were applied for the analysis of follow-up data. Unless otherwise mentioned, the mean for the corresponding number of experiments was plotted together with the SEM. The degrees of significance are indicated as * p < 0.05, ** p < 0.01.
Results
ING3 expression in clinical prostate samples
To explore ING3 expression in prostate cancer, we utilized a cohort of (n = 304) patients who were diagnosed with PCa by TURP and then used the AQUA analysis system to determine the association of ING3 expression and prostate disease progression. Based on the 0.15 cutoff proposed above, our cohort of 304 patients was grouped into 90 patients with low ING3 and 214 with high ING3 expressions (Table 1).
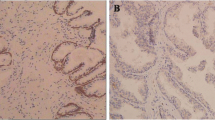
ING3 staining was mainly located at the nuclear compartment, and its expression was decreased with disease progression as shown in Fig. 1. ING3 mean percentage expression was highest in benign prostate tissues (mean 3.2 ± 0.54) compared to PCa (mean 2.5 ± 0.26) (p = 0.437), AdvPCa (mean 1.5 ± 0.23) (p = 0.004), and CRPC (mean 2.28 ± 0.32) (p = 0.285) (Fig. 2a). This was significant when comparing ING3 mean percentage expression in benign prostate tissues (mean 3.2 ± 0.54) with all types of prostate cancer progression combined (PCa/Adv/CRPC) (mean 2.13 ± 0.16) (p = 0.015) (Fig. 2b).

Fluorescent immunohistochemical staining of ING3 in prostate samples. Representative samples of TMA cores showing fluorescent immunohistochemical staining of ING3 using AQUA platform of two prostate tissue samples. Benign core (A–D) and cancer core (E–H). Immunofluorescence, using AQUA system, is shown for the localization of ING3 (red; B, F) and cytokeratin (green; C, G). DAPI was used as a nuclear stain (D, H). Merged images for all three stains (A, E). (Image provided by Mr. Brant Pohorelic)

ING3 expression in clinical samples. Mean expression of the percentage of cells which expressed nuclear ING3 protein levels in correlation with disease progression between benign and each type of prostate cancer progression (PCa, AdvPCa, and CRPC) separately (a) and between benign and all combined progression of prostate cancer samples (b). The overall survival analysis of patients with tumors expressing low ING3 levels (below median, <0.15) compared to patients with high levels of ING3 in all prostate cancer samples (c) and in ERG-negative samples (d). Significant differences in the overall survival between both groups were determined by Kaplan–Meier survival analysis. Error bars represent 95 % CI of mean percentage of cells expressing ING3 based on AQUA analysis. (BN benign, PCa localized prostate cancer, AdvPCa advanced prostate cancer, CRPC castration-resistant prostate cancer). The primary antibody used is anti-ING3 (2A2)
ING3 and Gleason score in clinical samples
To investigate the correlation between ING3 expression and Gleason score, PCa clinical samples were grouped into three categories GS < 7, GS 7 (3 + 4), and GS 7 (4 + 3). Our results showed that higher ING3 expression was significantly and inversely associated with GS (4 + 3) compared to GS (3 + 4) or GS < 7 (p < 0.041) (Supplementary Fig. 2).
ING3 and patients’ outcome
Patients with lower expression of ING3 showed marginally significant better cancer-specific mortality outcome compared to patients with higher ING3 expression (n = 304; p < 0.052) (Fig. 2c). This significance was more pronounced in the group of patients with ERG-negative tumors (p = 0.018) (Fig. 2d). Using Cox regression analysis, ING3 mean percentage expression was still significant in predicting lethal outcome when considering GS and tumor volume (p < 0.027) (Table 2).
ING3 expression in the prostate cancer cell lines
Examining ING3 messenger RNA (mRNA) levels using qRT-PCR showed upregulation of ING3 expression in both VCaP and LNCaP PCa cell lines compared to RWPE-1 (p < 0.007 and p < 0.0003), respectively. ING3 mRNA expression in PC3 and DU145 cells was significantly downregulated compared to RWPE-1, p < 0.0007 and p < 0.0003, respectively (Supplementary Fig. 3). However, ING3 protein levels were detectable at relatively comparable levels in all PCa cell lines (LNCaP, VCaP, and DU145 cell lines as well as in the immortalized prostate cell line RWPE-1) with the exception of PC3 cell line that expresses ING3 at low levels (Fig. 3).

ING3 expression in prostate cell lines. Of total protein cell lysate from all prostate cell lines, 40 μg was used to determine the protein level of ING3. Western blot performed on all prostate cancer cell lines was compared to the immortalized prostate cell line RWPE-1. ING3 (2A2) antibody was utilized in Western blot experiments. HEK293 cell lines were used as positive control for ING3 expression, and GAPDH was used as an internal control
ING3 increases cell invasion and migration in prostate cancer cell lines
To assess the biological role of ING3 in PCa, we performed cell invasion and migration assays in DU145 cells (originally expressing higher levels of ING3) after ING3 knockdown using siRNA. The effectiveness of ING3 knockdown is shown in Supplementary Fig. 4. Invasion assessed after 48 h demonstrated a significant decrease in ING3 knocked down cells compared to the control cells (Fig. 4a). Similarly, the migration ability assessed after 24 h was decreased in ING3 knocked down cells compared to the control (Fig. 4b).

Effect of ING3 expression on cancer cell invasion and migration. a DU145 cells were transfected with siRNA, non-targeting (siControl) and siRNA ING3. 5 × 104 cells per ml were left to transfer through membrane for 24 and 48 h in triplicate; then, the mean ± SEM was calculated. ING3 knocked down cells invaded through membrane in significantly less numbers (**p < 0.01). b Monolayer of DU145 cells. Cells transiently transfected with non-targeting siRNA (upper panel). DU145 cells transiently transfected with siRNA ING3 (lower panel). Cells were then subjected to a wound-healing assay, and images were taken after 0, 16, and 24 h to assess migration
ERG affects ING3 expression in PCa cell lines
To study the influence of ERG on ING3 expression, we used RWPE-1, LNCaP, and PC3 cell lines stably expressing ERG. VCaP cells, which harbor TMPRSS2-ERG gene fusion, were used as a positive control for ERG expression. ING3 mRNA expression was downregulated in all the cell lines stably expressing ERG; RWPE-1-ERG, LNCaP-ERG, and PC3-ERG compared to their control cell lines expressing either GFP or luciferase (p < 0.001, p < 0.0001, p < 0.0003, respectively) (Fig. 5a). At the protein level, ING3 did not show significant changes in RWPE1-ERG or LNCaP-ERG cells; however, there was a significant reduction in PC3-ERG in comparison to the control PC3-Luc (Fig. 5b).

ING3 expression in prostate cancer cell lines stably overexpressing ERG. a Relative expression of ING3 mRNA in RWPE-1 (**p = 0.001), LNCaP (**p = 0.0001), and PC3 (**p = 0.0003) where ERG is overexpressed in those cell lines compared to their controls (RWEP-GFP, LNCaP-GFP, and PC3-Luc). GUSB was used as an internal control. The figure represents experiments repeated three times (n = 3). The ING3 and GUSB primers that were used are described in Supplementary Table 1. b Total cell protein lysates from cells stably overexpressing ERG by Western blot. ING3 protein (upper panel). ERG exogenous expression in RWPE1-ERG, LNCaP-ERG, and PC3-ERG (middle panel). GAPDH was used as loading control (lower panel). ING3 2A2 antibody was used in the Western blot
Discussion
The inhibitor of growth family member 3 (ING3) is a member of the ING tumor suppressor family, which represents a novel tumor suppressor family of proteins encoded by five-conserved genes. ING3 is ubiquitously expressed in normal human tissues and regulates gene transcription, cell cycle control, and apoptosis [27]. Deregulated ING3 expression has been found in human head and neck squamous cell carcinomas, melanomas, and hepatocellular carcinoma [5–7]. However, no previous studies have examined ING3 expression levels and its function in prostate cancer or investigated its relation to TMPRSS2-ERG gene rearrangements.
A study by Lu et al. [10] investigated expression of ING3 in HCC and showed lower levels of ING3 in cancer samples compared with normal liver tissues using both cell lines and human samples of HCC. Moreover, in the same study, wound-healing assays on hepatocellular cell lines transfected with ING3 showed a significant reduction of migration in those cells. These studies suggest a tumor suppressor role of ING3 in this type of malignancy. In contrast to these studies, our results demonstrated that lower ING3 levels in PCa is associated with a better survival rate compared to higher levels of ING3. In addition, our observation in wound-healing and invasion assays on DU145 cell line transfected with siRNA ING3 showed that there was a reduction of invasion and migration. These findings present for the first time support a potential oncogenic role of ING3 in PCa. To our knowledge, only one study has suggested a tumor potentiating role of another member of the ING family (ING2) in colon cancer, where its expression levels were found to be upregulated in this type of malignancy; however, this was not supported by further functional studies [28]. In other studies, ING2 was reported to play a tumor suppressor role in hepatocellular carcinoma, head and neck squamous cell carcinoma, and melanoma [29–31]. ING3, similar to ING2, showed downregulation in those three types of cancer in addition to colon cancer. The contradictory roles of the same member of the ING family suggest that ING proteins’ biological role is cell type-specific.
Our qRT-PCR results indicated a negative correlation between ERG and ING3 where ERG overexpressing cell lines showed a significant decrease in ING3 expression in comparison to their controls at the mRNA level. These findings are in agreement with our clinical data where ERG-positive samples showed a decrease in the percentage of cells that have nuclear expression of ING3. It was interesting to observe that PC3-ERG cell lines had lower levels of ING3 in comparison to their PC3-Luc control cells, which was not the case in RWPE1-ERG and LNCaP-ERG cells when compared to their controls. In addition to the cell type differences, other factors such as PTEN deletion and the presence of AR may have a role in this discrepancy among the cells regarding the effect of ERG on ING3 expression. This might suggest a role of AR in regulating ING3 expression, as PC3 cells are AR negative while RWPE-1 and LNCaP are AR positive. Therefore, the excess amount of ERG could have acted as a negative feedback for the expression of AR [32]. The differences between ING3 protein and mRNA levels in the ERG expressing cell lines might also be attributed to posttranslational modifications, which warrants further investigation to explain the discrepancies between mRNA and protein levels.
In conclusion, this study is the first to report the expression of ING3 in prostate cancer and the association of this expression with ERG gene fusion. One of the main novelties of our study is that it is the first to investigate the expression levels of ING3 in relation to disease progression and clinical outcome of prostate cancer patients. In addition, this is the first study to demonstrate direct evidence about the oncogenic role of ING3, a protein that has been only known as a tumor suppressor. Further studies to elucidate the detailed mechanistic pathways involved in the functional role of ING3 and its therapeutic usage in prostate cancer are warranted.
Abbreviations
- ING3:
-
Inhibitor of growth member 3
- CRPC:
-
Castration-resistant prostate cancer
- GS:
-
Gleason score
- PCa:
-
Prostate cancer
- ERG:
-
ETS-related gene
- PCK:
-
Cytokeratin
- DAPI:
-
4′,6-Diamidino-2-phenylindole dihydrochloride
References
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30. doi:10.3322/caac.21166.
Society AC (2013) Prostate cancer overview American Cancer Society, Inc. http://www.cancer.org/cancer/prostatecancer/overviewguide/prostate-cancer-overview-key-statistics
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. doi:10.3322/caac.21208.
He GH, Helbing CC, Wagner MJ, Sensen CW, Riabowol K. Phylogenetic analysis of the ING family of PHD finger proteins. Mol Biol Evol. 2005;22(1):104–16. doi:10.1093/molbev/msh256.
Gunduz M, Beder LB, Gunduz E, Nagatsuka H, Fukushima K, Pehlivan D, et al. Downregulation of ING3 mRNA expression predicts poor prognosis in head and neck cancer. Cancer Sci. 2008;99(3):531–8. doi:10.1111/j.1349-7006.2007.00708.x.
Wang Y, Dai DL, Martinka M, Li G. Prognostic significance of nuclear ING3 expression in human cutaneous melanoma. Clin Cancer Res. 2007;13(14):4111–6. doi:10.1158/1078-0432.CCR-07-0408.
Yang HY, Liu HL, Tian LT, Song RP, Song X, Yin DL, et al. Expression and prognostic value of ING3 in human primary hepatocellular carcinoma. Exper Biol Med. 2012;237(4):352–61. doi:10.1258/ebm.2011.011346.
Nagashima M, Shiseki M, Pedeux RM, Okamura S, Kitahama-Shiseki M, Miura K, et al. A novel PHD-finger motif protein, p47ING3, modulates p53-mediated transcription, cell cycle control, and apoptosis. Oncogene. 2003;22(3):343–50. doi:10.1038/sj.onc.1206115.
Gunduz M, Ouchida M, Fukushima K, Ito S, Jitsumori Y, Nakashima T, et al. Allelic loss and reduced expression of the ING3, a candidate tumor suppressor gene at 7q31, in human head and neck cancers. Oncogene. 2002;21(28):4462–70. doi:10.1038/sj.onc.1205540.
Lu M, Chen F, Wang Q, Wang K, Pan Q, Zhang X. Downregulation of inhibitor of growth 3 is correlated with tumorigenesis and progression of hepatocellular carcinoma. Oncol lett. 2012;4(1):47–52. doi:10.3892/ol.2012.685.
Laudet V, Hanni C, Stehelin D, Duterque-Coquillaud M. Molecular phylogeny of the ETS gene family. Oncogene. 1999;18(6):1351–9. doi:10.1038/sj.onc.1202444.
Ichikawa H, Shimizu K, Hayashi Y, Ohki M. An RNA-binding protein gene, TLS/FUS, is fused to ERG in human myeloid leukemia with t(16;21) chromosomal translocation. Cancer Res. 1994;54(11):2865–8.
Birdsey GM, Dryden NH, Amsellem V, Gebhardt F, Sahnan K, Haskard DO, et al. Transcription factor Erg regulates angiogenesis and endothelial apoptosis through VE-cadherin. Blood. 2008;111(7):3498–506. doi:10.1182/blood-2007-08-105346.
Demichelis F, Fall K, Perner S, Andren O, Schmidt F, Setlur SR, et al. TMPRSS2:ERG gene fusion associated with lethal prostate cancer in a watchful waiting cohort. Oncogene. 2007;26(31):4596–9. doi:10.1038/sj.onc.1210237.
Teng LH, Wang C, Dolph M, Donnelly B, Bismar TA. ERG protein expression is of limited prognostic value in men with localized prostate cancer. ISRN Urology. 2013;2013:786545. doi:10.1155/2013/786545.
Nagle RB, Algotar AM, Cortez CC, Smith K, Jones C, Sathyanarayana UG, et al. ERG overexpression and PTEN status predict capsular penetration in prostate carcinoma. Prostate. 2013;73(11):1233–40. doi:10.1002/pros.22675.
Hoogland AM, Jenster G, van Weerden WM, Trapman J, van der Kwast T, Roobol MJ, et al. ERG immunohistochemistry is not predictive for PSA recurrence, local recurrence or overall survival after radical prostatectomy for prostate cancer. Mod Pathol. 2012;25(3):471–9. doi:10.1038/modpathol.2011.176.
Bismar TA, Dolph M, Teng LH, Liu S, Donnelly B. ERG protein expression reflects hormonal treatment response and is associated with Gleason score and prostate cancer specific mortality. Eur J Cancer. 2012;48(4):538–46. doi:10.1016/j.ejca.2012.01.001.
Minner S, Enodien M, Sirma H, Luebke AM, Krohn A, Mayer PS, et al. ERG status is unrelated to PSA recurrence in radically operated prostate cancer in the absence of antihormonal therapy. Clin Cancer Res. 2011;17(18):5878–88. 1078–0432.CCR-11-1251.
Korenchuk S, Lehr JE LMC, Lee YG, Whitney S, Vessella R, Lin DL, et al. VCaP, a cell-based model system of human prostate cancer. In vivo. 2001;15(2):163–8.
Nupponen NN, Hyytinen ER, Kallioniemi AH, Visakorpi T. Genetic alterations in prostate cancer cell lines detected by comparative genomic hybridization. Cancer Genet Cytogenet. 1998;101(1):53–7.
Chen TR. Chromosome identity of human prostate cancer cell lines, PC-3 and PPC-1. Cytogenet Cell Genet. 1993;62(2–3):183–4.
Zhu X, Kumar R, Mandal M, Sharma N, Sharma HW, Dhingra U, et al. Cell cycle-dependent modulation of telomerase activity in tumor cells. Proc Natl Acad Sci U S A. 1996;93(12):6091–5.
Mahmood T, Yang PC. Western blot: technique, theory, and trouble shooting. N Am J Med Sci. 2012;4(9):429–34. doi:10.4103/1947-2714.100998.
Epstein JI, Allsbrook Jr WC, Amin MB, Egevad LL. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am J Surg Pathol. 2005;29(9):1228–42.
Budczies J, Klauschen F, Sinn BV, Gyorffy B, Schmitt WD, Darb-Esfahani S, et al. Cutoff Finder: a comprehensive and straightforward web application enabling rapid biomarker cutoff optimization. PLoS One. 2012;7(12):e51862. doi:10.1371/journal.pone.0051862.
Shah S, Smith H, Feng X, Rancourt DE, Riabowol K. ING function in apoptosis in diverse model systems. Biochem Cell Biol. 2009;87(1):117–25. doi:10.1139/O08-107.
Kumamoto K, Fujita K, Kurotani R, Saito M, Unoki M, Hagiwara N, et al. ING2 is upregulated in colon cancer and increases invasion by enhanced MMP13 expression. Int J Cancer. 2009;125(6):1306–15. doi:10.1002/ijc.24437.
Zhang HK, Pan K, Wang H, Weng DS, Song HF, Zhou J, et al. Decreased expression of ING2 gene and its clinicopathological significance in hepatocellular carcinoma. Cancer Lett. 2008;261(2):183–92. doi:10.1016/j.canlet.2007.11.019.
Li X, Kikuchi K, Takano Y. ING genes work as tumor suppressor genes in the carcinogenesis of head and neck squamous cell carcinoma. J Oncol. 2011;2011:963614. doi:10.1155/2011/963614.
Lu F, Dai DL, Martinka M, Ho V, Li G. Nuclear ING2 expression is reduced in human cutaneous melanomas. Br J Cancer. 2006;95(1):80–6. doi:10.1038/sj.bjc.6603205.
Yu J, Yu J, Mani RS, Cao Q, Brenner CJ, Cao X, et al. An integrated network of androgen receptor, polycomb, and TMPRSS2-ERG gene fusions in prostate cancer progression. Cancer Cell. 2010;17(5):443–54. doi:10.1016/j.ccr.2010.03.018.
Acknowledgments
The authors acknowledge the Antibody Facility at University of Calgary especially Ms. Donna Boland for ING3 antibody and Mr. Brant Pohorelic for AQUA images. Amal Almami is a graduate student sponsored by King Abdullah Scholarship, Saudi Arabia, and supported by Saudi Cultural Bureau in Canada. This work was supported in part by the Prostate Cancer Foundation Young Investigator Award (T.A.B). This work was also supported by Prostate Cancer Canada and is proudly funded by the Movember Foundation-Grant # B2013-01.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Fig. 1
Overexpression of ERG in prostate cell lines. ERG was cloned from VCaP cell lines and then stably transfected in RWPE-1, LNCaP and PC3 cell lines. Transfection was confirmed with qRT-PCR and Western blot, by comparing the transfected cells to its control. A) Relative expression of ERG mRNA levels in ERG overexpressed RWPE1-ERG (P = 0.013), LNCaP-ERG (P = 0.0005), and PC-ERG (P = 0.001) cell lines to it controls (RWPE1-GFP, LNCaP-GFP and PC3-Luc). GUSB was used as internal control. The ERG and GUSB primers that were used are shown in in Supplementary Table 1. The figure represents experiments run in triplicates (n = 3). (B) represents protein levels of ERG in RWPE-1, LNCaP and PC3, respectively, depicting overexpression of ERG compared to their controls. GAPDH were used as loading controls for Western blot. Bars indicate quantification of three separate Western blots experiments. P values < 0.05 were considered significant. (GIF 83 kb)
Supplementary Fig. 2
Correlation between ING3 percentage level and Gleason score. The percentage of ING3 positive nuclear cells based on AQUA analysis in relation to Gleason score. Representative percentage of cells with ING3 expression in tissue samples with more specific Gleason Scores. GS <7 gray, GS7 (3 + 4) narrow strikes and GS7 (4 + 3) broad dark strikes. Chi-square statistical test using SPSS software and the value of P <0.05 was considered statistically significant. (GIF 47 kb)
Supplementary Fig. 3
ING3 mRNA expression in prostate cell lines. Quantitative Real time PCR experiments of ING3 mRNA expression in four prostate cancer cell lines LNCaP (P = 0.00017), VCaP (P = 0.008), PC3 (P = 0.0007) and DU145 (P = 0.0003) relative to the expression of ING3 in RWPE-1 cells. GUSB was used as an internal control. The ING3 and GUSB primers that were used are shown in Supplementary Table 1. The figure represents experiments repeated three times (n = 3). (GIF 40 kb)
Supplementary Fig. 4
Successful knockdown of ING3 in DU-145 cells. ING3 was knocked down in DU145 cell lines compared to DU145 cells transfected with scrambled siRNA. The mRNA levels of ING3 in DU145 cells transfected with siRNA ING3 down-regulated relative to cells transfected with control siRNA quantified by qRT-PCR. GUSB was used as an internal control. Student t-test used to calculate the P value where ** p < 0.01 was considered significant. The figure represents three times independent experiments (n = 3). ING3 and GUSB used primers are described in Supplementary Table 1. (GIF 14 kb)
Supplementary Table 1
(DOCX 18 kb)
Rights and permissions
About this article

Cite this article
Almami, A., Hegazy, S.A., Nabbi, A. et al. ING3 is associated with increased cell invasion and lethal outcome in ERG-negative prostate cancer patients. Tumor Biol. 37, 9731–9738 (2016). https://doi.org/10.1007/s13277-016-4802-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-016-4802-y