
Abstract
Cervical cancer is the third most common cancer disease affecting the female population, and a key factor in the development of the disease is the human papillomavirus infection (HPV). The disease is also impacted by epigenetic changes such as DNA methylation, which causes activation or exclusion of certain genes. The aim of our review is to summarize and compare the most common molecular methods for detection of methylated promoter regions in biomarkers occurring in cervical carcinoma and also show the importance of connections of HR-HPV testing with methylation analysis in patients with cervical intraepithelial neoplasia. Insight into genetic and epigenetic alterations associated with cervical cancer development can offer opportunities for the molecular biomarkers that can be useful for screening, diagnosis, and also as new ways of treatment of cervical cancer precursor lesions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The annual mortality from cervical cancer is about 275,000 women worldwide [1]; the highest incidence of the disease is between 35 to 39 and 60 to 65 years of age. The human papillomavirus (HPV) infection is the main etiological factor with more than 100 HPV types [2] identified and divided into two groups. The first group includes so-called “low-risk” (LR) types and the main actors are HPV 6 and 11. The second group consists of HPV types known as “high-risk” (HR) types (HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59) leading to development of cervical cancer. Recently, HPV 68 has been classified as probable high risk, and seven types (HPV 26, 53, 66, 67, 70, 73 82) have been classified as possible high-risk. Only a minority of HR-HPV infections become “transforming” infections, characterized by an altered expression of two viral genes E6 and E7 [3].
The HPV can be detected by very sensitive molecular methods (on the DNA or RNA), such as dot blot (DB) hybridization, Southern blots, fluorescent in situ hybridization (FISH), polymerase chain reaction (PCR), strand displacement amplification (SDA), transcription-mediated amplification (TMA), and others. On the mRNA level, only the active virus expressed in the DNA can be detected. To analyze such an active virus, an amplification test which qualitatively detects the viral mRNA expressing the oncogenes (E6, E7) in patients with HR-HPV was performed [4]. An increased level of E6mRNA and p16 transcripts could mean the potential of cervical dysplasia progression to cancer [5].
The other possible cause and also a promising tool for cervical cancer diagnostics could be the methylation of DNA of specific biomarkers. Methylation was also observed in a number of other gynecological malignancies, including endometrial carcinoma [6, 7], ovarian carcinoma [8], and breast cancer [9]. There are already some soluble cancer biomarkers available such as CADM1, MAL, SOX1, PAX1, CDH1, and DAPK1, but if taken singularly, they do not offer complete reliability due to their intrinsic lack of both sensitivity and specificity. The primary objective is to find the possibility of setting up a panel which could take advantage of the combination of the various methylated biomarkers and HR-HPV testing method with high sensitivity and specificity.
The aim of our review is to summarize and compare the most common molecular methods for detection of methylated promoter regions in biomarkers occurring in cervical carcinoma and also show the importance of the connections of HR-HPV testing with methylation analysis in patients with cervical intraepithelial neoplasia (CIN).
Genetic and epigenetic changes in cervical carcinoma
Although the major cause of cervical cancer is considered to be the HPV infection, recent studies have reported that the infection itself is not sufficient for a malignant transformation; neoplastic cells require other cooperating factors. These are particularly factors in the process causing suppression of general and local immunity: a chronic vaginal infection, smoking, hormonal contraception, a certain kind of sex life, and also a large genetic instability, chromosomal aberrations, and epigenetic changes in DNA sequence [3].
The main issue is that women with advanced CIN (with increased levels of molecular aberrations) have a high short-term risk for cancer progression. Studies of genetic instability refer to chromosome 3; specifically, gain at 3q was particularly frequent in HPV 16 positive squamous cell carcinoma (SCC), and gain at 1p was the most frequent aberration in CIN3. These findings have led to an identification of new oncogenes and tumor suppressor genes such as eyes absent homologue 2 (Eya2) and Mir 375 [10, 11]. Chromosomal amplification of 3q26 and 5p15 is also present in precancerous lesions with high specificity for a differential diagnosis of CIN2+ lesions [12, 13].
Epigenetic changes are stable without alterations of gene expression changes in the actual sequence of DNA and cause a disease in the absence of mutation in the gene. The mechanism of these changes can alter the phenotype without altering the genotype. Such modification of phenotype can be induced by genetic factors and environmental influences, and these changes are inherited mitotically as well as meiotically. Despite this fact, these hereditary signs are reversible, providing thus an opportunity for therapeutic intervention. These changes include two basic methods of switching genes. The first one is a modification of histones and the second one is DNA methylation. Double-stranded DNA is wrapped around the cell histones and due to their modification, the access of protein to a particular gene is stopped, and thus the transcription from DNA to RNA becomes non-functional [14].
The most common and significant epigenetic modifications in the mammalian genome is DNA methylation. Methylation is a covalent chemical modification, in which the group is attached to the fifth methylated cytosine ring carbon (5Mc), thus preventing access of proteins. Most DNA methylation of cytosine occurs at guanine nucleotide in areas called CpG islands. These islands, present in an unmethylated state and located at the 5′end (the promoter region and the first exon), are 500-bp long and have at least 55 % CG dinucleotides. Whereas an unmethylated promoter could lead to gene expression, the promoter methylation may cause canceling the transcription of genes [15]. The process of transmission of methylated DNA is catalyzed by a methyltransferase (DNMT1, DNMT2, DNMT3, DNMT3B)-CH3. The source is S-adenosyl-l-methionine (SAM), which is converted to S-adenosyl-l-homocysteine (SAH). These changes in DNA methylation occur mainly during embryonic development in the mother’s body, but the change may also occur in adulthood. One of the most important features of DNA methylation changes is their specificity for tissue and tumor types. Tumors from different tissues exhibit a unique formula of DNA methylation changes. Another essential feature of these changes is the fact that they are already present in early stages of the development of the disease; before the actual clinical manifestations of carcinogenesis start, making screening and early diagnosis of the disease is very important.
Methylation markers
Testing and screening of cervical smears for HR-HPV-positive samples showed a sensitivity increase in cervical screening [16], but this is also associated with low specificity, especially in the young population. For this reason, there is a need for additional markers to increase the positive predictive value of the screening of populations with cervical neoplasia. Methylation of the promoter region of tumor suppressor genes (TSG) is regarded to be one of the first causes of carcinogenesis. An aberrant methylation has been described in a number of candidate TSG, which occur in CIN lesions and cervical cancer [17]. Herfs et al. reported in 2012 that a discrete population of cuboidal epithelial cells—localized in the squamo-columnar junction (SCJ)—is a cellular representative (a probable precursor) of most cervical cancers [18]. Methylation biomarkers such as cell adhesion molecule 1 (CADM1), cadherin 1 (CDH1), death-associated protein kinase 1 (DAPK1), erythrocyte membrane protein band 4.1-like 3 (EPB41L3) family with sequence similarity 19, chemokine (CC motif)-like, member A4 (FAM19A4) myelin and lymphocyte protein (MAL), paired box 1 (PAX1), PR domain-containing 14 (PRDM14), and telomerase reverse transcriptase (TERT) are among the most common methylating genes for samples with invasive squamous cell carcinoma (SCC) and adenocarcinoma. From the transforming genes in CIN lesions, the average methylation frequency was highest for the CADM1 gene, a gene that followed CDH1, DAPK1, and TERT [19].
For now, this appears to be the most reliable panel consisting of the genes CADM1 and MAL. Up to now, only one large study (n = 236) took place where these two methylation markers (CADM1, MAL) were tested in patients positive for HR-HPV and also with CIN3. The real-time PCR showed clinical sensitivity values amounted to 84 % and the clinical specificity values of 53 % [20]. Eijsink et al. [21] in their study reached the value of the clinical sensitivity of 84 % for HR-HPV-positive patient with a diagnosis of CIN3 clinical value and specificity of 69 %. In recent studies, it was also established that the methylation of the promoter region of genes MAL and CADM1 were increased in female patients with a diagnosis of CIN3 and also a long presence of the HR-HPV infection. The highest values of methylation were achieved when the patient was already diagnosed with cervical cancer [22].
Bisulfite methods for diagnostic of potential methylated gene region
Accurate determination of DNA methylation and its degree is not only a very important step in the diagnosis but may also be used in anticancer therapy.
Using methylation-specific primers, this converts non-methylated cytosines to uracils (thymine by the PCR product), and thus modifies the DNA sequence. Methylated cytosines remain unchanged. The principle of this method is based on a different reaction of bisulfite (NaHSO3) with cytosine (C) and methylated cytosine (mC). Cytosine forms a bisulfite anion product that is subsequently hydrolytically deaminated to uracil. After the alkaline desulfonation, SO3 ion is removed from the uracil group and there remains a final uracil (U). This modification is currently used in several methods that can be divided into two groups, based on methylation-specific (MSP-PCR, real-time PCR-MS method, and MethyLight) or nonspecific (HRM, MS-SSCP, bisulfite sequencing, and COBRA) PCR.
Methylation-specific PCR (MSP) with the specific primers is the most commonly used method. Its principle lies in differences between methylated and unmethylated alleles following bisulfite modification. The method is used in two separate reactions when methylated and unmethylated molecules are amplified, and the products are analyzed by agarose gel electrophoresis. This technique is specific and sensitive, but it cannot assess quantitative results [23].
Quantitative methylation-specific PCR or MethyLight (QM-MSP) is a modification, based on fluorescence detection using real-time technology. The primers are designed in such a way that the complementary sequence of primers does not contain CpG dinucleotides; hence, the DNA regions would be amplified regardless of the methylation status of the template. The principle of the method is to determine the relative level of methylated DNA of the promoter region of each sample as the ratio of the target gene to the internal reference gene that is amplified in the treated DNA, irrespective of methylation state [24]. Wentzensen et al. [19] using the QM-MSP described the most methylated genes in cervical carcinoma (CDH1 (58 %), DAPK1 (57 %), CADM1 (55 %), and the TERT (55 %)), whereas the highest percentage of methylation in samples diagnosed with CIN2/CIN3/HSIL was for the CADM1 gene (33 %).
The abovementioned methods represent a methylation-specific PCR. Among nonspecific methylation PCR methods, we can include the method of high-resolution melting (HRM), methylation-sensitive single-strand conformation polymorphism (MS-SSCP), the method of combined bisulfite restriction analysis (COBRA), the MIRA method, and bisulfite sequencing.
HRM is a post PCR method which is used for a melting curve analysis of samples to reveal mutations in epigenetic changes in double stranded (dsDNA). The advantages of this method include relatively low cost, speed, and accuracy in the identification of genotypes [25]. Both HRM and MethyLight have similar analytical sensitivities and can detect as little as 0.1–1.0 % of methylated DNA in a background of unmethylated DNA [26].
MS-SSCP: quantification of DNA methylation is based on a different migration of single-stranded DNA on a non-denaturing polyacrylamide gel. An advantage of bisulfite sequencing is that it is one of the most complex methods of DNA methylation analysis that significantly saves time. A disadvantage of this method is the need for cloning PCR products into plasmid vectors, which are then sequenced [27]. Using bisulfite sequencing of the promoter region in length of 93 bp, methylation of the CADM1 gene in squamocellular carcinoma and in samples from patients with severe cervical dysplasia was demonstrated, and thus, this gene was functionally incorporated into cervical carcinogenesis [28].
COBRA uses primers specific for bisulfite modification of DNA followed by a technique such as restriction digestion. It serves for determining the percentage of methylation on the basis of the ratios of undigested and digested PCR products [29].
MIRA is a method that is not based on the same principles as the abovementioned methods but instead analyzes hypermethylated genes using a microarray analysis. This method has been described by Rauch and Pfeifer [30] and later used with slight variations in the identification of DNA methylation in the SOX9 gene of cervical cancer [3]. The MIRA method is based on a restriction endonuclease or antibodies in conversion of genomic DNA with sodium bisulfite, but with the ability of protein binding to methylated DNA (MBD protein) that specifically recognizes methylated CpG dinucleotides.
The above-described methods are efficient and of high performance, but they do not allow a numerous sample analysis at the same time. Currently, a gold standard for identification of new genes and methylation is next generation DNA sequencing (NGS). This enables analysis of a large number of samples and quantitative evaluation of results. Pyrosequencing is a quantitative sequencing method that ensures obtaining DNA sequences using real-time sequencing for DNA synthesis as well as quantitative evaluation of results. A principle of this method is luminometric detection of pyrophosphate (PPi), which is liberated during polymerization of DNA. The effect was first described in 1985 [31]. However, only in 2005 was NGS introduced to wide scientific public. Pyrosequencing enables optimal quantitative evaluation of methylation of each analyzed CpG dinucleotide sequence. This is of considerable importance for assessing the degree of methylation of specific genes in the tumor process. [32].
Conclusion
In this review article, we have focused on epigenetic alterations and on an overview of available molecular diagnostic methods. Molecular biomarkers, based on DNA methylation in cervical cancer, can be easily detected in both histological and cytological cervical specimens. Nowadays, other cellular gene alterations (DNA mutations or DNA copy-number aberrations) are less attractive as molecular triage markers [33], and studies indicate that a methylation marker panel is needed to reach high sensitivity for transforming CIN lesions. High methylation levels of two-marker panels CADM1 and MAL were detected in cervical scrapings of women with advanced transforming CIN lesions [34]. Nowadays, there are also examined new biomarker panels including various combinations of the markers (SOX1, PAX1, LMX1A, and NKX6-1). Another promising panel consists of four markers (JAM3, EPB41L3, TERT, and C13ORF18) [20].
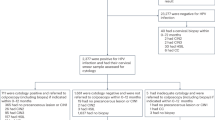
Women from European countries, treated for CIN2 and CIN3, are monitored by cervical cytology 6, 12, and 24 months after treatment. If there are three consecutive negative test results, women return to screening at an interval of 3–5 years. A promising tool for management of CIN2/CIN3 should be the use of a combination of HR-HPV testing and methylation marker analysis, because combination of cytology with HR-HPV testing is not sufficient [35]. Women with methylation-negative tests are not in need of an immediate colposcopy because of a very low short-term progression risk for cancer and should just repeat the test after 12–18 months. On the other hand, HPV-positive women with high short-term progression risk for cancer and also with a positive methylation test should be sent for colposcopy immediately [36].
References
Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer. GLOBOCAN, 2008.
Sung LC, et al. Methylation markers for diagnosis of cervical cancer, Patent application publication, 2013.
Steenbergen R, Snijders P, Heideman D, et al. Clinical implications of (epi) genetic changes in HPV-induced cervical precancerous lesions. Nat Rev Cancer. 2014;14:395–405.
Arbyn M, Roelens J, Cuschieri K, et al. The APTIMA HPV assay versus the Hybrid Caoture II test in triage of women with ASC-US or LSIL cervical cytology: a meta-analysis of the diagnostic accuracy. Int J Cancer. 2013;132(1):101–8.
Janusicova V, Mendelova A, Zubor P, et al. mRNA Expression in cervical specimens for determination of severe dysplasia or worse in HPV-16/18-positive squamous lesions. J Low Genit Tract Dis. 2014;18(3):273–80.
Fiolka R, Zubor P, Holubekova V, et al. Promoter hypermethylation of the tumor-suppresor genes RASSF1A, GSTP1 and CDH1 in endometrial cancer. Oncol Rep. 2013;30(6):2878–86.
Visnovsky J, Fiolka R, Kudela E, et al. Hypermethylation of selected genes in endometrial carcinogenesis. Neuro Endocrinol Lett. 2013;34(7):675–80.
Culbova M, Lasabova Z, Stanclova A, et al. Metylácia vybraných tumor-supresorových génov v benígnych a malígnych ovariálnych nádoroch. Article in Czech. Česká gynekologie. 2011;76(4):274–9.
Zubor P, Kajo K, Stanclova A, et al. Human epithelial growth factor receptor 2 polymorphism and risk of fibroadenoma. Eur J Cancer Prev. 2008;17(1):33–8.
Thomas LK, Bermejo JL, Vinokurova S, et al. Chromosomal gains and losses in human papillomavirus-associated neoplasia of the lower genital tract—a systematic review and meta-analysis. Eur J Cancer. 2014;50(1):85–98.
Bierkens M, Krijqsman O, Wilting S, et al. Focal aberrations indicate EYA2 and hsa-miR-375 as oncogene and tumor suppressor in cervical carcinogenesis. Genes Chromosom Cancer. 2013;52(1):56–68.
Kudela E, Farkasova A, Visnovsky J, et al. Amplification of 3q26 and 5p15 regions in cervical intraepithelial neoplasia. Acta Obstet Gynecol Scand. 2014;93(10):997–1002.
Visnovsky J, Kudela E, Farkasova A, et al. Amplification of TERT and TERC genes in cervical intraepithelial neoplasia and cervical cancer. Neuro Endocrinol Lett. 2014;35(6):518–22.
Wajed SA, Laird PW, DeMeester TR, et al. DNA methylation: an alternative pathway to cancer. Ann Surg. 2001;234(1):10–20.
Merlo A, Herman JG, Mao L, et al. 5’CpG Island methylation is associated with transcirptional silencing of the tumor suppressor gene p16/CDKN2/MTS1 in human cancers. Nat Med. 1995;1(7):686–92.
Mayrand MH, Duarte-Franco E, Rodrigues I, et al. Human papillomavirus DNA versus Papanicolaou screening tests for cervical cancer. N Engl J Med. 2007;357:1579–88.
Szalmas A, Konya J. Epigenetic alterations in cervical carcinogenesis. Semin Cancer Biol. 2009;19(3):144–52.
Herfs M, Yamamoto Y, Laury A, et al. A discrete population of squamocolumnar junction cells implicated in the pathogenesis of cervical cancer. Proc Natl Acad Sci. 2012;109:10516–21.
Wentzensen N, Sherman ME, Schiffman M, et al. Utility of methylation markers in cervical cancer early detection: appraisal of the state-of-the science. Gynecol Oncol. 2009;112(2):293–9.
Hesselink AT, Heideman DA, Steenbergen RD, et al. Combined promoter methylation analysis of CADM1 and MAL: an objective triage tool for high-risk human papillomavirus DNA-positive women. Clin Cancer Res. 2011;17:2459–65.
Eijsink JJ, Lendvai Á, Deregowski V, et al. A four-gene methylation marker panel as triage test in hig-hrisk human papillomavirus positive patients. Int J Cancer. 2012;130(8):1861–9.
Bierkens M, Hesselink AT, Meijer CJ, et al. CADM1 and MAL promoter methylation levels in hrHPV-positive cervical scrapes increase proportional to degree and duration of underlying cervical disease. Int J Cancer. 2013;133:1293–9.
Fraga MF, Esteller M. DNA methylation: a profile of methods and applications. Biotechniques. 2002;33(4):6–49.
Swift- Scanlan T, Blackford A, Argani P, et al. Two-color quantitative multiplex methylation-specific PCR. Biotechniques. 2006;40(2):210–9.
Jiménez I, Cardeñosa EE, Suela SP, et al. Advantages of the high resolution melting in the detection of BRCA1 or BRCA2 mutation carriers. Clin Biochem. 2009;42:1572–6.
Snellenberg S, De Strooper LM, Hesselink AT, et al. Development of a multiplex methylation-specific PCR as candidate triage test for women with an HPV-positive cervical scrape. BMC Cancer. 2012;12:551.
Bian YS, Yan P, Osterheld MC, et al. Promoter methylation analysis on microdissected paraffin-embedded tissues using bisulfi te treatment and PCR- SSCP. Biotechniques. 2001;30(1):66–72.
Steenbergen RD, Kramer D, Braahuis BJ, et al. TSLC1 gene silencing in cervical cancer cell lines and cervical neoplasia. J Natl Cancer Inst. 2004;96(4):294–305.
Xiong Z, Laird PW. COBRA: a sensitive and quantitative DNA methylation assay. Nucleic Acids Res. 1997;25(12):2532–4.
Rauch TA, Pfeifer GP. The MIRA method for DNA methylation analysis. Methods Mol Biol. 2009;507:65–75.
Hyman ED. A new method of sequencing DNA. Anal Biochem. 1988;174:423–36.
Mikeska T, Felsberg J, Hewitt CA, et al. Analysing DNA methylation using bisulphite pyrosequencing. Methods Mol Biol. 2011;791:33–53.
Kyrgiou M, Koliopoulos G, Martin-Hirsch P, et al. Obstetric outcomes after conservative treatment for intraepithelial or early invasive cervical lesions: systematic review and meta-analysis. Lancet. 2006;367(9509):489–98.
Wright AA, Howitt BB, Myers AP, et al. Oncogenic mutations in cervical cancer: genomic differences between adenocarcinomas and squamous cell carcinomas of the cervix. Cancer. 2013;119:3776–83.
Kocken J, Helmerhorst TJ, Bekhof J, et al. Risk of recurrent high-grade cervical intraepithelial neoplasia after successful treatment: a long-term multi-cohort study. Lancet Oncol. 2011;12(5):441–50.
Arbyn M, Kyrgiou M, Simoens C, et al. Perinatal mortality and other severe adverse pregnancy outcomes associated with treatment of cervical intraepithelial neoplasia: meta-analysis. BMJ. 2008;337:284.
Acknowledgments
This work was supported by the project “Molecular diagnostics of cervical cancer” (ITMS:26220220113), Comenius University Grants 303/2011, 242/2012, 287/2015, 121/2015, and the VEGA Grant 1/0271/12 as well as the APVV-0224-12 grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Rights and permissions
About this article

Cite this article
Mersakova, S., Nachajova, M., Szepe, P. et al. DNA methylation and detection of cervical cancer and precancerous lesions using molecular methods. Tumor Biol. 37, 23–27 (2016). https://doi.org/10.1007/s13277-015-4197-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-015-4197-1