
Abstract
The microRNAs (miRNAs), miR-194 and miR-29b, have been shown to downregulate in colorectal cancer (CRC) and may identify and classify CRC patients as compared with those in control subjects. In the current study, we aimed to explore whether the serum levels of the miRNAs could be potential biomarkers for diagnosis and prognosis of CRC. A quantitative reverse-transcription polymerase chain reaction (qRT-PCR) assay was utilized to determine and compare serum levels of miR-194 and miR-29b in 55 patients with CRC and 55 control subjects. The correlations between levels of the miRNAs and clinicopathological stages of cancer were analyzed in patients. Receiver operating characteristic (ROC) curve and survival analyses were carried out, respectively, to determine diagnostic and prognostic values of the miRNAs. Serum levels of miR-194 and miR-29b were found to be significantly lower in CRC patients than those in control subjects (P < 0.0001). Moreover, serum levels of the miRNAs in patients were inversely correlated with the advanced TNM stages (P = 0.01). ROC curve and survival analyses revealed that reduced levels of the miRNAs could serve as diagnostic and prognostic biomarkers for patients with CRC (P = 0.0001). Serum levels of miR-194 and miR-29b may serve as potential biomarkers for diagnosis and prognosis of CRC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) has been reported as the fourth most common cause of cancer mortality around the world with considerable health burden [1]. Early stage diagnosis of the disease by noninvasive approaches could lead to effective treatment and better consequences [2]. In this regard, microRNAs (miRNAs) in a few biological samples may deserve as early detection biomarkers for CRC [2, 3]. miRNAs are endogenous small, nonprotein-coding RNAs that posttranscriptionally regulate expression of a broad range of biologically important genes, functioning as either oncogenes or tumor-suppressor genes depending on their physiopathological contribution and the tumor microenvironment [4, 3]. Given the contribution of miRNAs in the pathogenesis of tumor cells, dysregulation of some miRNAs in tumor tissue would be conceivable. In fact, altered expression of a variety of miRNAs has been corroborated in CRC tissues [3].
Alteration in the expression of miRNAs in cancerous tissue could also be reflected in circulation [5]. Therefore, altered levels of some miRNAs in plasma/serum or other body fluids of CRC patients have been extensively explored in an effort to find suitable diagnostic and prognostic biomarkers [6]. In this regard, the miRNAs, miR-194 and miR-29b, may act as circulating invaluable and surrogate biomarkers for CRC. While miR-194 has been shown to be upregulated in esophageal squamous cell carcinoma and prostate cancer [7], its downregulation has been recently reported in endometrial cancer [8], primary renal cell carcinoma [9], and CRC tissues [10, 11]. Notably, the low expression level of miR-194 in CRC tissues was shown to be correlated with increased tumor size [10, 11]. Furthermore, the decreased level of miR-194 in stool samples was indicated to differentiate CRC patients from normal subjects [11]. On the other hand, miR-29b suppresses proliferation of epithelial cells in the intestinal mucosa [12], inhibits migration of colon cancer cells [13], and is significantly downregulated in osteosarcoma tissues [14]. Given the involvement of miR-194 and miR-29b in some cancers, including CRC and that there were no studies regarding their circulating levels in CRC, we determined the serum levels of miR-194 and miR-29b in a fairly large number of CRC patients, relative to control subjects, by real-time PCR assay to explore their diagnostic and prognostic values.
Materials and methods
Participants of the study consisted of individuals who consecutively referred to the Cancer Institute of Tehran in Iran for suspected colorectal diseases since April 2011 to May 2012. During the time period, serum samples were obtained from 55 patients with CRC and 55 control subjects. The obtained serum samples were further centrifuged in Eppendorf tubes for 10 min at 20,000g and 4 °C in a fixed-angle rotor centrifuge to remove residual cell debris, and the new supernatants were immediately preserved at −80 °C until further analyses. Diagnosis of patients and control subjects were based on colonoscopy and histopathological findings. Control subjects had no evidence of previous or current (based on colonoscopy) malignancy. The time relapsed between sampling and diagnosis was less than 2 weeks. None of the subjects under study had undergone any medical intervention such as radiotherapy, chemotherapy, and surgery before sampling. All CRC patients underwent curative surgical or endoscopic tumor resection, and their pathological stages were determined according to the tumor-node-metastasis (TNM) staging system [15]. After that, the overall stage groups (0–IV) of the patients were assigned by histopathologists of the Cancer Institute. The tumor type of patients consisted of 41 adenocarcinomas, 9 squamous cell carcinomas, and 5 adenosquamous cell carcinomas. Exclusion criteria included inflammatory conditions, familial adenomatous polyposis, colorectal adenomas, any precancerous polyp or lesion, hereditary nonpolyposis CRC, and other malignancies except CRC. Information regarding the traditional clinical features of the participant was provided from their history and clinical findings.
Approval for the study was given by the ethics committee of the institute, and all patients and control subjects provided written informed consents before enrollment in the study.
Serum RNA extraction
For RNA isolation, the frozen serum samples were thawed thoroughly on ice. Total RNA was isolated from 200 μl of serum using the miRNeasy Serum/Plasma Kit (Qiagen, CA, USA) following the manufacturer’s instructions, with minor modifications. At first, 1.7 μl glycogen (10 mg/ml), as a co-precipitant, was added to 1000 μl Qiazol solution (denaturant reagent of the kit) and the new mixture was used as denaturant reagent of the serum. For the aqueous and organic phase separation step, 200 μl of molecular grade chloroform was added to the denatured serum and vortexed vigorously for 30 s, followed by incubation at room temperature for 5 min. After denaturation by the denaturant reagent, the serum samples were evenly spiked with 5 μl of 25 fmol synthetic cel-miR-39 (Qiagen) as an internal control. Cel-miR-39 has been used as a reliable normalizer for accurate measurement of circulating miRNAs in patients with colorectal neoplasia [16]. At final, total RNA was eluted from the spin column membrane (provided in the kit) in 30 μl RNase-free water (pre-warmed to 55 °C) and about 28 μl of the total RNA solution was obtained. The optical density of the extracted total RNA samples was assessed at the wavelengths 260 and 280 nm on a NanoDrop spectrophotometer (NanoDrop, Wilmington, DE, USA) to determine their concentrations and purities. The isolated total RNA samples were aliquotted and preserved at −80 °C until subsequent analysis.
Quantitative real-time PCR
Reverse transcriptase (RT) reaction for complementary DNA (cDNA) synthesis from mature miRNAs was carried out using a miScript II Reverse Transcription Kit (Qiagen, CA, USA) according to the manufacturer’s instructions. Each RT reaction (as duplicate) included 5 μl of the isolated total RNA, 2 μl miScript Reverse Transcriptase Mix, 4 μl RT buffer (5×), 2 μl miScript Nucleics Mix (10×), and 7 μl RNase-free water to a total volume of 20 μl. To synthesize the cDNAs, the RT reaction mixtures were incubated at 37 °C for 60 min, 95 °C for 5 min, and then placed on ice. The component of each RT reaction (cDNAs) was diluted with 200 μl RNase-free water. The tubes containing diluted cDNAs were briefly centrifuged and immediately placed on ice to proceed with quantitative real-time PCR.
To amplify the resulted cDNAs, a real-time SYBR green PCR platform containing miScript SYBR Green PCR Kit (Qiagen) and miScript Primer Assay (Qiagen) was used. The real-time PCR mixture for each miRNA under study comprised of 2 μl cDNA, 12.5 μl of 2× QuantiTect SYBR Green PCR Master Mix, 2.5 μl of 10× miScript Universal Primer, 2.5 μl of 10× miRNA-specific forward primer (miScript Primer Assay, Qiagen), and 5.5 μl of water (nuclease free) in a final volume of 20 μl. All reaction mixtures prepared in 96-well optical plates were run on a CFX96™ real-time PCR apparatus (Bio-Rad, Hercules, CA, USA). A negative template (without cDNA) control was also simultaneously run on the same plate to ensure target-specific amplification. The real-time PCR cycling conditions included a preliminary activation step at 95 °C for 15 min followed by 40 amplification cycles, each set as denaturation at 94 °C for 15 s, annealing at 55 °C for 30 s, and elongation at 70 °C for 30 s. All real-time PCR measurements were done in duplicate. After the completion of real-time PCR reaction, a melting curve analysis was accomplished to ensure specific amplification of the target miRNA. Threshold cycles (Ct) for target miRNAs and the spiked-in control were determined in each sample.
The Ct values of miR-194 and miR-29b in patients and control subjects were normalized relative to the Ct value of cel-miR-39 (the spiked-in control) and their relative levels were calculated using the 2−ΔΔCt method [17].
Statistical analysis
All statistical analyses were accomplished with SPSS 16.0 software (SPSS Inc., Chicago, IL, USA) and values were displayed as mean ± SD, median [interquartile range (IQR)], number, and percentage. Based on a pilot study (containing 10 patients and 10 control subjects) for the serum levels of miR-194 and miR-29b, we found that with considering 80 % power and 2-sided α = 0.05, a sample size of 55 (for each group) would be sufficient to detect a potential difference between CRC patients and control subjects. Two tailed Mann-Whitney U test was used to assign the differences of miR-194 and miR-29b levels between patients and control subjects. To compare the differences of the miRNAs between patient’s subgroups, Kruskal-Wallis test was employed. Chi-squared test was also used to compare dichotomous variables between patients and control groups. The Kendall’s tau correlation coefficient (τ) was used to examine the association between serum miR-194 and miR-29b levels and cancer TNM staging. After converting to logarithmic scale for values with skewed distribution, multiple logistic regression analyses were performed to find whether the serum levels of miR-194 and miR-29b could predict the presence of CRC. Receiver operating characteristics (ROC) curve analysis was used to define useful diagnostic cutoff values for the miRNAs under study. To understand whether the serum levels of miR-194 and miR-29b were associated with overall survival of the patients, Kaplan-Meier and stepwise Cox proportional hazard regression analyses were carried out from the day of sampling until the death or censor date (follow-up period, 40 months). A P value <0.05 was interpreted as statistically significant.
Results
Clinical and pathological features of patients and control subjects are displayed in Table 1. As seen, the distribution of age, gender, and smoking are comparable in the patients and control subjects.
We compared the relative amounts of miR-194 and miR-29b in the serum of patients and control subjects. As shown in Fig. 1, in patients as a whole, the serum median levels of miR-194 and miR-29b [0.88 (0.68–1.02) and 0.54 (0.45–0.64)] were revealed to be significantly lower than those in control subjects [1.34 (1.03–1.74) and 0.79 (0.67–0.94) (Mann-Whitney U test, P < 0.0001), respectively.

Serum levels of miR-194 and miR-29b in control subjects and colorectal cancer patients. Serum levels of miR-194 and miR-29b were significantly decreased in patients compared to those in control subjects (P < 0.0001). Lines within boxes represent median values; edges of the boxes demonstrate interquartile ranges
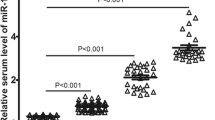
Additionally, serum levels of miR-194 and miR-29b showed a significant decreasing trend with the advancement of cancer TNM stages (Kruskal-Wallis test, P < 0.001) (Fig. 2). The medians (IQR) values of serum miR-194 and miR-29b levels according to patient’s TNM stage subgroups were, respectively, as follows: 0.99 (0.91–1.16), 0.83 (0.70–0.89) in stage 0, 1.02 (0.76–1.61), 0.64 (0.58–0.69) in stage I, 1.02 (0.84–1.26), 0.61 (0.49–0.68) in stage II, 0.79 (0.66–0.97), 0.52 (0.42–0.60) in stage III, 0.68 (0.55–0.91), and 0.44 (0.37–0.52) in stage IV. Furthermore, serum levels of miR-194 and miR-29b in the patients demonstrated negative associations with TNM stage progression (τ = −0.55, P = 0.01 for miR-194 and τ = −0.61, P = 0.01 for miR-29b, respectively). Surprisingly, neither miR-194 nor miR-29b serum levels did show notable correlations with other clinicopathological features of patients such as age, gender, smoking, tumor size, tumor differentiation, lymphatic invasion, tumor depth invasion, and histological grade.

Box plots depicting serum miR-194 (a) and miR-29b (b) levels in control subjects, as well as in colorectal cancer patients according to their cancer TNM staging (0–IV). As seen, the miRNAs values have a tendency to be decreased in proportion to the progression of TNM stags. Lines within boxes represent median values; edges of the boxes demonstrate interquartile ranges
Given the presence of significant differences in miR-194 and miR-29b levels between patients and control subjects, a multiple logistic regression analysis, controlling for the effects of other covariates, was performed. As shown in Table 2, serum levels of the miRNAs appeared as independent biomarkers, negatively associated with the presence of CRC.
To define the best cutoff values of serum miR-194 and miR-29b levels with the capability to discriminate patients from control subjects, ROC curve analyses were performed. It was found that serum miR-194 at cutoff value of 1.08 provides 72 % sensitivity and 80 % specificity with an area under curve (AUC) of 0.85 [95 % confidence interval (CI) = 0.79 to 0.93, P = 0.0001] to discriminate patients from control subjects. Likewise, serum miR-29b at cutoff value 0.66 provided 77 % sensitivity and 75 % specificity with an AUC of 0.87 (95 % CI = 0.80 to 0.96, P = 0.0001) (Fig. 3).

Receiver operating characteristic (ROC) curve analyses of miR-194 and miR-29b to find the best cutoff values for discriminating colorectal cancer patients from control subjects
The relationships of serum miR-194 and miR-29b with prognosis status in CRC patients were further examined by Kaplan-Meier curve analysis and log-rank test. Furthermore, prognostic values of the miRNAs was compared with carcinoembryonic antigen (CEA, a currently used routine tumor biomarker of CRC; data was only available for patients). The median values of the biomarkers (after log transformation) were used as cutoffs to segregate the patients with low levels from those who had the high levels. The analysis revealed that patients with miR-194 levels ≤0.88 fold change, miR-29b ≤0.54 fold change, and CEA >3.61 ng/ml had a significantly lower overall survival rate than those patients with miR-194 levels >0.88 fold change (log-rank = 13.393, P = 0.0001), miR-29b >0.54 fold change (log-rank = 29.820, P = 0.0001), and CEA ≤3.61 ng/ml (log-rank = 4.008, P = 0.045), respectively (Fig. 4).

Kaplan-Meier overall survival curves for serum (a) miR-194, (b) miR-29b, and (c) carcinoembryonic antigen (CEA) levels in patients with colorectal cancer. Median levels of the biomarkers (after log transformation) were considered as cut off values to subgroup patients into those with low and high levels of the biomarkers. Overall survival rates between the two subgroups were compared by log-rank test and significant differences were recognized
In order to identify the factors with potential impact on survival rate, univariate and multivariate Cox proportional hazard regression analyses were carried out. As expected, decreased serum miR-194 and miR-29b levels were remained as independent indicators of poor prognosis in CRC patients (Table 3).
Discussion
The results of this systematically designed study delineated that the serum levels of miR-194 and miR-29b were significantly reduced in patients with CRC and these decrements were in proportionate to the advancing tumor TNM stage. Most importantly, serum levels of the miRNAs were found to discriminate CRC patients from control subjects and it was also evidenced that these miRNAs could serve as robust prognostic biomarkers of CRC.
There is some controversy regarding the exact role of miR-194 in various cancers. Although few studies have indicated that miR-194 is significantly upregulated in some cancers [7, 8], many others report contradictory results, especially in CRC, highlighting its contribution as a tumor-suppressor factor [10, 8, 11]. Consistent with the latter studies, our findings exhibited a lower level of miR-194 in the serum of patients with CRC compared to control subjects. Also, the declined serum miR-194 level in a mutual relation to the progression of tumor stage in the patients under study gives further evidence that miR-194 may probably behave as a tumor-suppressor factor. Some mechanistic links of miR-194 as a tumor-suppressor have been come from various in vitro studies. In one study, it has been reported that miR-194 inhibits CRC cell viability and invasion through targeting the PDK1/AKT2/XIAP pathway [11]. In endometrial cancer, miR-194 inhibits tumor invasion process by suppressing the expression of BMI-1, an important oncogene involved in the transition of epithelial to mesenchymal cells [18]. Furthermore, miR-194 has shown to suppress murine double minute 2 (MDM2), thymidylate synthase (TYMS), and Smad-interacting protein 1/zinc finger E-box binding homeobox 2 (SIP1/ZEB2) in renal cell carcinoma cell line [19]. It should be noted that the three latter targets of miR-194 have a detrimental role in tumor progression [20–22]; therefore, the miR-194 effects also reflect its tumor-suppressing activity. The responsible factors for the increased level of miR-194 in normal cells have not been clearly identified. Hepatic nuclear factor 1α (HNF1α) has shown to upregulate miR-194 expression in the gastrointestinal tract [23]. On the other hand, activation of the tumor-suppressor gene p53 in tumor cell lines has led to the increased expression of miR-194 [24]. Taken together, this line of evidence as well as those we discovered in the present study, potentiate the notion that miR-194 may act as a tumor-suppressor factor; therefore, our finding of the deregulated (decreased) level of the miRNA in the serum of patients with CRC would be conceivable.
With regard to miR-29b, the situation is also conflicting to some extent. Overexpression of miR-29b in B-cell chronic lymphocytic leukemia (CLL) [25] and pancreatic cancer tissue specimens [26] has been reported. On the contrary, the contribution of miR-29b as a tumor-suppressor factor has been corroborated in several cancers including prostate [27], cholangiocarcinoma [28], AML [29], colon cancer [13], osteosarcoma [14], and primary hepatic carcinoma [30]. In this regard, as for miR-194, we found a lower level of miR-29b in the serum of patients with CRC, being also decreased with the advancement of clinical stages of tumors. Several possible mechanisms have been proposed for the anti-cancer property of miR-29b. In colon cancer, miR-29b suppresses the malignant cells via the repression of matrix metalloproteinase-2, a key enzyme degrading extracellular matrix and consequently involved in tumor invasion and metastasis [13]. It has been shown that miR-29b directly modulates the molecular chaperone VEGF in the osteosarcoma cell line MG63, leading to the inhibition of cell proliferation, migration, and invasion [14]. Also, miR-29b represses the expression of cyclin-dependent kinase 2; thereby, inhibiting the growth of epithelial cells of the small intestine [12] and restraining metastatic capacity of prostate cancer via modulating the expression of epithelial-mesenchymal transition signaling cascade [27]. Anyway, here again, our finding is in accordance with the mentioned studies, confirming a tumor-suppressor role for miR-29b.
Of importance, we found, for the first time, that serum levels of miR-194 and miR-29b can be used as potential noninvasive diagnostic and prognostic predictors of CRC. Consistent with our finding were two recent studies in which the diagnostic and/or prognostic implications of miR-194 [11] and miR-29b [30] for CRC were elucidated in other human samples such as the tissue and stool. Similarly, serum miR-29b was shown to be a diagnostic and prognostic biomarker in patients with primary hepatic carcinoma [31], suggesting its potential clinical importance for diagnostic and prognostic purposes.
It is noteworthy to point out that the decreased circulating levels of some other miRNAs, such as miR-601, miR-760 [32], miR-31, miR-92a, miR-181b, and miR-203 [33] have been also reported to serve as diagnostic biomarkers in CRC patients with discriminating powers (sensitivity and specificity ranging approximately from 70 to 90 %) comparable with those values we gained in the current study. Considering that there were no further studies investigating the utility of serum miR-194 and miR-29b levels as indicators of CRC, results of the present study may provide a reliable evidence of the circulating miRNAs for further researches and also clinical use.
There were some limitations in the present study that should not be ignored. The control subjects selected from persons who underwent colonoscopy examination for colorectal illness and likely were not a typical sample of a comprehensively healthy population. However, we excluded all subjects with underlying known diseases that could interfere with the miRNAs under study. Additionally, although the sample size of the study was seemingly adequate, including larger sample number may improve our results. Investigating miR-194 and miR-29b expressions in CRC tissues could provide a stronger evidence of the origin of the biomarkers in the serum. However, the expression pattern of the biomarkers has been studied recently in CRC tissues [10, 11, 30] and may be of fewer interest compared to the serum samples. Whatever the source of the miRNAs might be, their circulating levels are further requirements for diagnosis and prognosis.
In conclusion, the current study disclosed that miR-194 and miR-29b levels are significantly decreased in sera from patients with CRC in comparison with those in control subjects. Given that the decreased serum levels of the miRNAs discriminated CRC patients from control subjects and was correlated with tumor TNM stages progression as well as poor survival in the patients, measuring their levels in the serum may be utilized as a noninvasive diagnostic and prognostic tool for CRC. The results may be extended into clinical setting provided that further validation studies are to be performed.
References
Max Parkin D, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74.
Narayanan V, Peppelenbosch MP, Konstantinov SR. Human fecal microbiome-based biomarkers for colorectal cancer. Cancer Prev Res. 2014;7(11):1108–11.
Schetter AJ, Okayama H, Harris CC. The role of microRNAs in colorectal cancer. Cancer J Sudbury Mass. 2012;18(3):244.
Bartel DP. MicroRNAs: target recognition and regulatory functions. Cell. 2009;136(2):215–33.
Mitchell PS, Parkin RK, Kroh EM, Fritz BR, Wyman SK, Pogosova-Agadjanyan EL, et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc Natl Acad Sci. 2008;105(30):10513–8.
Blanco-Calvo M, Calvo L, Figueroa A, Haz-Conde M, Antón-Aparicio L, Valladares-Ayerbes M. Circulating microRNAs: molecular microsensors in gastrointestinal cancer. Sensors. 2012;12(7):9349–62.
Selth L, Townley S, Bert A, Stricker P, Sutherland P, Horvath L, et al. Circulating microRNAs predict biochemical recurrence in prostate cancer patients. Br J Cancer. 2013;109(3):641–50.
Zhai H, Karaayvaz M, Dong P, Sakuragi N, Ju J. Prognostic significance of miR-194 in endometrial cancer. Biomark Res. 2013;1(12):10.1186.
White NM, Bao TT, Grigull J, Youssef YM, Girgis A, Diamandis M, et al. miRNA profiling for clear cell renal cell carcinoma: biomarker discovery and identification of potential controls and consequences of miRNA dysregulation. J Urol. 2011;186(3):1077–83.
Chiang Y, Song Y, Wang Z, Liu Z, Gao P, Liang J, et al. microRNA-192, -194 and -215 are frequently downregulated in colorectal cancer. Exp Ther Med. 2012;3(3):560–6.
Zhao H-J, Ren L-L, Wang Z-H, Sun T-T, Yu Y-N, Wang Y-C, et al. MiR-194 deregulation contributes to colorectal carcinogenesis via targeting AKT2 pathway. Theranostics. 2014;4(12):1193.
Xiao L, Rao JN, Zou T, Liu L, Cao S, Martindale JL, et al. miR-29b represses intestinal mucosal growth by inhibiting translation of cyclin-dependent kinase 2. Mol Biol Cell. 2013;24(19):3038–46.
Poudyal D, Cui X, Le PM, Hofseth AB, Windust A, Nagarkatti M, et al. A key role of microRNA-29b for the suppression of colon cancer cell migration by American ginseng. PLoS One. 2013;8(10):e75034.
Zhang K, Zhang C, Liu L, Zhou J. A key role of microRNA-29b in suppression of osteosarcoma cell proliferation and migration via modulation of VEGF. Int J Clinical Exp Pathol. 2014;7(9):5701.
Fleming I, Cooper J, Henson D, Hutter R, Kennedy B, Murphy G et al. American Joint Committee on Cancer. AJCC cancer staging manual. 5. Lippincott-Raven, Philadelphia; 1997.
Yamada A, Cox MA, Gaffney KA, Moreland A, Boland CR, Goel A. Technical factors involved in the measurement of circulating microRNA biomarkers for the detection of colorectal neoplasia. PLoS One. 2014;9(11):e112481.
Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2− ΔΔCT method. methods. 2001;25(4):402-8.
Dong P, Kaneuchi M, Watari H, Hamada J, Sudo S, Ju J, et al. MicroRNA-194 inhibits epithelial to mesenchymal transition of endometrial cancer cells by targeting oncogene BMI-1. Mol Cancer. 2011;10:99.
Khella HW, Bakhet M, Allo G, Jewett MA, Girgis AH, Latif A, et al. miR-192, miR-194 and miR-215: a convergent microRNA network suppressing tumor progression in renal cell carcinoma. Carcinogenesis. 2013;34(10):2231–9.
Kahlert C, Lahes S, Radhakrishnan P, Dutta S, Mogler C, Herpel E, et al. Overexpression of ZEB2 at the invasion front of colorectal cancer is an independent prognostic marker and regulates tumor invasion in vitro. Clin Cancer Res. 2011;17(24):7654–63.
Polański R, Warburton HE, Ray-Sinha A, Devling T, Pakula H, Rubbi CP, et al. MDM2 promotes cell motility and invasiveness through a RING-finger independent mechanism. FEBS Lett. 2010;584(22):4695–702.
Rose MG, Farrell MP, Schmitz JC. Thymidylate synthase: a critical target for cancer chemotherapy. Clin Colorectal Cancer. 2002;1(4):220–9.
Hino K, Tsuchiya K, Fukao T, Kiga K, Okamoto R, Kanai T, et al. Inducible expression of microRNA-194 is regulated by HNF-1α during intestinal epithelial cell differentiation. RNA. 2008;14(7):1433–42.
Braun CJ, Zhang X, Savelyeva I, Wolff S, Moll UM, Schepeler T, et al. p53-responsive microRNAs 192 and 215 are capable of inducing cell cycle arrest. Cancer Res. 2008;68(24):10094–104.
Santanam U, Zanesi N, Efanov A, Costinean S, Palamarchuk A, Hagan JP, et al. Chronic lymphocytic leukemia modeled in mouse by targeted miR-29 expression. Proc Natl Acad Sci. 2010;107(27):12210–5.
Zhang Y, Li M, Wang H, Fisher WE, Lin PH, Yao Q, et al. Profiling of 95 microRNAs in pancreatic cancer cell lines and surgical specimens by real-time PCR analysis. World J Surg. 2009;33(4):698–709.
Ru P, Steele R, Newhall P, Phillips NJ, Toth K, Ray RB. miRNA-29b suppresses prostate cancer metastasis by regulating epithelial–mesenchymal transition signaling. Mol Cancer Ther. 2012;11(5):1166–73.
Mott JL, Kobayashi S, Bronk SF, Gores GJ. mir-29 regulates Mcl-1 protein expression and apoptosis. Oncogene. 2007;26(42):6133–40.
Garzon R, Volinia S, Liu C-G, Fernandez-Cymering C, Palumbo T, Pichiorri F, et al. MicroRNA signatures associated with cytogenetics and prognosis in acute myeloid leukemia. Blood. 2008;111(6):3183–9.
Akira Inoue, Hirofumi Yamamoto, Mamoru Uemura, Junichi Nishimura,Taishi Hata, Ichiro Takemasa, et al. MicroRNA-29b is a novel prognostic marker in colorectal cancer. Ann Surg Oncol. DOI 10.1245/s10434-014-4255-8
Zheng J, Yu F, Dong P, Bai Y, Chen B. Expression of miRNA-29b and its clinical significances in primary hepatic carcinoma. Zhonghua yi xue za zhi. 2013;93(12):888–91.
Wang Q, Huang Z, Ni S, et al. Plasma miR-601 and miR-760 are novel biomarkers for the early detection of colorectal cancer. PLoS One. 2012;7:e44398.
Wang J, S-k H, Zhao M, Yang M, J-l Z, et al. Identification of a circulating microRNA signature for colorectal cancer detection. PLoS One. 2014;9(4):e87451. doi:10.1371/journal.pone.0087451.
Acknowledgments
This study was funded by the Ilam University of Medical Sciences (grant number EC/92/H/136).
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Basati, G., Razavi, A.E., Pakzad, I. et al. Circulating levels of the miRNAs, miR-194, and miR-29b, as clinically useful biomarkers for colorectal cancer. Tumor Biol. 37, 1781–1788 (2016). https://doi.org/10.1007/s13277-015-3967-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-015-3967-0