
Abstract
Napsin A and thyroid transcription factor-1 (TTF-1) are useful biomarkers for differentiating lung adenocarcinoma from squamous cell carcinoma and also for differentiating primary lung adenocarcinoma from metastatic lung carcinoma. Pair-boxed 8 (PAX8) can help in distinguishing primary lung carcinoma from metastatic carcinomas and help to determine the primary sites of metastatic carcinomas. Immunohistochemistry for Napsin A, TTF-1, and PAX8 were performed on 193 cases of carcinoma: 50 primary lung carcinoma and 143 carcinomas from other sites. Napsin A and TTF-1 were positive in 54, 52 % of lung carcinomas cases, respectively. While in adenocarcinoma cases, their expressions were 86.7 and 83.3 %, respectively. PAX8 was negative in all lung carcinomas. TTF-1 and PAX8 were positive in 93.3 and 96.7 % of thyroid carcinoma cases and in 87.5 and 93.8 % of papillary carcinoma respectively, and both were positive in 100 % of follicular carcinoma. Napsin A was negative in all thyroid carcinomas. Napsin A and PAX8 were positive in 50 and 93.3 % of renal carcinoma cases and in 81.8 and 100 % of papillary carcinoma, 38.5 and 92.3 % of clear cell carcinoma, and 16.7 and 83.3 % of chromophobe carcinoma respectively. TTF-1 was negative in all renal carcinomas. PAX8 was positive in 80 % of ovarian carcinoma cases; 100 and 60 % of serous mucinous carcinomas, respectively. It was also positive in 100 % of endometrial carcinoma. Napsin A and TTF-1 were negative in both ovarian and endometrial carcinomas. Our data demonstrated that combined use of Napsin A, TTF-1, and PAX8 may help in differentiating between primary lung adenocarcinoma and metastatic lung carcinomas.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lung cancer is one of the common cancers and the leading cause of cancer-related death worldwide [1]. Approximately, 80 % of lung cancers are diagnosed as non-small cell lung cancer (NSCLC); a heterogeneous group comprised of adenocarcinoma (AC) and squamous cell carcinoma (SCC) [2].
Accurate classifications of different subtypes of NSCLC have risen to allow maximal therapeutic benefit [3]. Therefore, both routine histological diagnosis and immunohistochemistry (IHC) may play an important role in this process [4].
Lung carcinoma is one of the common primary carcinomas; other common types include renal, thyroid, ovarian, breast, endometrial, upper gastrointestinal tract, and colorectal carcinomas [5]. Metastatic carcinomas of an unknown primary accounts for approximately 3 to 5 % of all malignant neoplasms and, as such, is one of the ten most frequently diagnosed cancers in humans [6]. Lung is a common site for metastases from extrapulmonary carcinomas. Differential diagnoses of primary lung AC from metastatic carcinomas, especially poorly differentiated ones, are challenging [7]. Immunohistochemistry has emerged as a powerful diagnostic and confirmatory tool for the differential diagnosis of lung carcinomas, whether primary or secondary especially from common sites including colon, breast, prostate, pancreas, stomach, kidney, bladder, ovaries, and uterus.
Recently, Napsin A and thyroid transcription factor 1 (TTF-1) are considered as a promising tool to distinguish poorly differentiated lung AC from lung SCC [8–11]. Both markers are useful for primary AC of the lung [1, 11, 12]. However, they also expressed in other extrapulmonary carcinomas, so we need an additional new marker to verify the diagnosis. A transcriptional factor, Paired box gene 8 (PAX8), appears to be a marker for this purpose.
Napsin A is a functional aspartic proteinase involved in the maturation of active surfactant protein B in type II pneumocytes [13]. The expression of Napsin-A is regulated by TTF-1 [14].
TTF-1 is a 38-kDa homeodomain protein containing DNA-binding activity. TTF-1 transcriptional factor regulates gene expression in follicular cells of the thyroid, type II pneumocytes, nonciliated bronchiolar epithelial cells of the lungs, and developing brain during embryogenesis [13]. TTF-1 is used for the differentiation between primary lung AC and metastatic AC of the lung [1, 2, 11, 15–18]. In addition, TTF-1 positivity is seen in up to 100 % of primary thyroid carcinomas [1, 2, 7, 12, 15].
Pair-boxed 8 (PAX8) is a pair-boxed transcriptional factor that is expressed during organogenesis of the kidney, thyroid, and central nervous system [19]. PAX8 has been also shown to be expressed in several primary human malignancies including carcinomas arising in endometrium, endocervix, ovary, thyroid, kidney, and urothelium [20] but not in primary lung AC [21–24]. These findings suggest that PAX8 has potential value for differential diagnosis of primary lung carcinoma from that are metastatic to the lung and may be helpful in determining primary site.
The aim of this study is to test the hypothesis that PAX8 in combination with Napsin A and TTF-1 constitutes a valuable immunostaining panel for differentiating AC from SCC on the one hand and in differentiation between primary lung AC and metastatic AC to the lung on the other hand.
Materials and methods
Cases selection
One hundred ninety-three specimens of resected primary carcinomas which included 50 cases of primary lung carcinoma and 143 primary carcinomas from different organs were selected. The specimens were obtained from the archives of the Department of Pathology, Minia University Hospital, Egypt during the period from March 2008 to December 2013.
Tissue specimens of 50 primary lung carcinomas included were 30 AC, 15 SCC, and 5 large cell carcinomas.
Thirty thyroid specimens were included and subtyped as 16 papillary thyroid carcinomas and 14 follicular carcinomas.
Thirty specimens from the kidney were also included of which 13 were clear cell, 11 were papillary, and 6 were chromophobe renal cell carcinomas.
Twenty cases from ovaries, comprised of 10 serous carcinoma and 10 mucinous carcinoma, were also included.
Other carcinomas included 15 cases from the uterus, 10 cases from breast tissue, 10 cases from the colon, 10 cases from the liver, 10 cases from the prostate, 3 cases from the esophagus, and 5 cases from the stomach.
All tissues were obtained from routine formalin-fixed paraffin-embedded tissue blocks. Hematoxylin and eosin (H&E) stained sections were prepared and examined to confirm the diagnoses.
Immunohistochemistry
Streptavidin-biotin immunoperoxidase complex procedure was applied for immunostaining. In brief, 4-μm-thick sections from prediagnosed cases were transferred to adhesive slides from representative formalin-fixed, paraffin-embedded blocks. The sections were deparaffinized in xylene and dehydrated through a series of graded alcohols. Endogenous peroxidase activity was blocked by incubation with 0.3 % hydrogen peroxide in methanol for 30 min. Antigen retrieval was achieved by microwave treatment in sodium citrate buffer, pH 6, for Napsin A and in EDTA buffer, pH 9, for TTF-1 and PAX8 for 10 min.
Tissue sections were then incubated with monoclonal antibodies for Napsin A; mouse monoclonal antibody, clone (TMU-Ad 02) from Biocare Medical (Biocare Medical, Concord, CA), was used at 1:100 ilution. TTF-1, mouse monoclonal antibody 8G7G3/1 from Dako (Dako Cytomation), was used at 1:100 dilution for 30 min and PAX8, mouse monoclonal antibody, clone (BC12) from Biocare Medical (Biocare Medical, Concord, CA), was used at 1:80 dilution, followed by biotinylated secondary antibody for 30 min at room temperature. Visualization of the reaction was performed with an avidin-biotin complex immunoperoxidase system using 3,3′ diaminobenzidine (DAB) as a chromogen. Sections were then counterstained with hematoxylin, dehydrated, cleared, and mounted with distyrene, plasticizer, and xylene (DPX). Negative control sections were treated with phosphate-buffered saline (PBS) instead of primary antibody. Sections of known positive controls used were lung adenocarcinoma for Napsin A and TTF-1 and renal cell carcinomas for PAX8.
Scoring system
Cytoplasmic staining for Napsin A and nuclear staining for TTF-1 and PAX8 were considered positive. Scoring was performed according to percentage of positive immunoreactive neoplastic cells; positivity of Napsin A, TTF-1, and PAX8 were defined by staining of more than 5 % of tumor cells [7].
Statistical analysis
Using MedCalc version 12.0 software, the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of Napsin A, TTF-1, and PAX8 as regards the histopathologic findings of study group were estimated according to the following:
-
1.
Sensitivity
The test ability to identify the cases that truly have the diagnosis. High sensitivity implies few false negatives.
Sensitivity = (true positive / true positive + false negative).
-
2.
Specificity
The test ability to identify those cases that do not have the diagnosis. High specificity implies few false positive.
Specificity = (true negative / true negative + false positive).
-
3.
Positive predictive value
Probability of the case having the diagnosis when the test is positive (true positive / true positive + false positive).
-
4.
Negative predictive value
Probability of the case not having the diagnosis when the test is negative (true negative / true negative + false negative).
-
5.
Receiver operating characteristic curve
It is a graph that measures the test accuracy that combines sensitivity and specificity. The area under the curve is one of the most popular measures of the accuracy of a diagnostic test.
Results
The results of immunohistochemical expression for Napsin A, TTF-1, and PAX8 were summarized in Table 1.
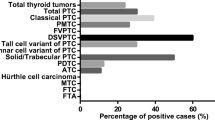
Expression pattern of Napsin A, TTF-1, and PAX8 in primary lung adenocarcinoma and carcinoma in other organs were shown in Fig. 1.


Expression pattern of Napsin A, TTF-1, and PAX8 in primary lung adenocarcinoma and carcinoma in other organs. Lung adenocarcinoma was positive for Napsin A (a) and TTF-1 (b), and negative for PAX8 (c). Thyroid carcinoma was negative for Napsin A (d) and positive for TTF-1 (e) and PAX8 (f). Renal cell carcinoma was positive for Napsin A (g), negative for TTF-1 (h), and positive for PAX8 (i). Ovarian carcinoma was negative for Napsin A (j) and TTF1 (k) and positive for PAX8 (l). Endometrial carcinoma was negative for Napsin A (m) and TTF1 (n) and positive for PAX8 (o). Sections were immunohistochemically stained, DAB chromogen; hematoxylin counterstain (original magnification ×400)
Napsin A immunoreactivity
Twenty-seven cases (54 %) of all lung carcinoma cases were positive for Napsin A immunostaining. Twenty-six cases (86.7 %) of AC cases and 1 (6.7 %) case of SCC were positive for Napsin A expression. As regarded cases of renal cell carcinoma, 15/30 (50 %) were positive for Napsin A immunostaining including 5/13 (38.5 %) clear cell, 9/11 (81.8 %) papillary, and 1/6 (16.7 %) chromophobe type. None of other primary carcinomas was positive for Napsin A immunostaining.
TTF-1 immunoreactivity
Twenty-six (52 %) of primary lung carcinomas showed positive TTF-1 immunostaining including 25/30 (83.3 %) AC, 1/15 (1.7 %) SCC, and 0/5 large cell carcinoma. Thyroid carcinoma showed TTF-1-positive immunostaining in 28/30 (93.3 %). Papillary thyroid carcinoma was positive for TTF-1 in 14/16 (87.5 %). All cases of follicular carcinoma were positive for TTF-1 immunostaining (100 %). Among TTF-1-positive expression in other carcinomas were 1/20 (6.7 %) in ovarian and 2/15 (13.3 %) in endometrium carcinomas.
PAX8 immunoreactivity
All 50 cases of primary lung carcinoma either AC, SCC, or large-cell carcinoma were completely negative for PAX8. Among 143 cases of other carcinomas, positive immunostaining was observed in carcinomas from thyroid (29/30; 96.7 %). We noted that 28 (93.3 %) of 30 renal clear cell carcinomas were positive for PAX8. In ovarian carcinoma, PAX8 expression was positive in 16/20 (80 %), and all cases of serous carcinoma were positive (100 %) and 6/10 (60 %) of mucinous carcinoma. Other PAX8 positive carcinomas included those originated from endometrium (15/15; 100 %); all other cases of adenocarcinoma were negative for PAX8 immunostaining.
Sensitivity, specificity, positive predictive value, and negative predictive value of Napsin A and TTF-1 in lung carcinoma
Positive immunoreactivity (sensitivity, 54 % and specificity, 90 %) was seen in 27 of 50 primary lung carcinoma and for Napsin A, compared with 26 of 50 (sensitivity, 52 % and specificity, 78 %) for TTF-1. Napsin A showed 64 % positive predictive value (PPV) and 85 % negative predictive value (NPV) while TTF-1 showed 46 % PPV and 82 % NPV. As regarded AC, the sensitivity (87 %), specificity (95 %), PPV (96 %), and NPV (83 %) of Napsin A. TTF-1 sensitivity and specificity were 83 and 96 % respectively and PPV and NPV were 96 and 79 % respectively as shown in Table 2. In Fig. 2a, for AC from other lung carcinomas, the mean of area under receiver operating characteristic (ROC) curve for Napsin A was 0.93 with confidence interval (0.83–0.98) and for TTF-1 was 0.92 with confidence interval (0.80–0.98) and p value = 0.31.

a Receiver operating characteristic (ROC) plots curve of Napsin A and TTF-1 in the diagnosis of lung adenocarcinoma from other lung carcinomas. b ROC plots curve of Napsin A and TTF-1 in diagnosis of lung carcinoma from other examined carcinomas. c ROC plots curve of TTF-1 and PAX 8 in diagnosis of thyroid Carcinoma from other examined carcinomas. d ROC plots curve of Napsin A and PAX 8 in diagnosis of renal carcinoma from other examined carcinomas
Sensitivity, specificity, PPV, and NPV of TTF-1 and PAX8 in thyroid carcinoma
As shown in Table 3, TTF-1-positive immunoreactivity was seen in 28/30 of thyroid carcinoma with sensitivity of 93 %, specificity of 82 %, and PPV and NPV were 49 and 99 % respectively, while the sensitivity and specificity of PAX8 were 97 and 64 % respectively, PPV (33 %) and NPV (99 %). TTF-1 was more specific but less sensitive than PAX8 in all examined cases of thyroid carcinoma and papillary thyroid carcinoma.
TTF-1 sensitivity, specificity, PPV, and NPV were 88, 76, 25, and 99 % respectively in papillary carcinoma while PAX8 sensitivity, specificity, PPV, and NPV were 94, 59, 17, and 99 % respectively. In follicular thyroid carcinoma, the specificity was 76 % for TTF-1 and 59 % for PAX8, so TTF-1 was more specific than PAX8 and the sensitivity was equal 100 % for both markers.
Sensitivity, specificity, PPV, and NPV of Napsin A and PAX8 in renal carcinoma
In renal cell carcinoma, the total sensitivity, specificity, PPV, and NPV of Napsin A were 50, 83, 36, and 90 % respectively while PAX8 were 93, 64, 32, and 98 % respectively. As regarding clear cell type, we found sensitivity (38 %), specificity (79 %), PPV (12 %), and NPV (95 %) for Napsin A, and the sensitivity (92 %), specificity (58 %), PPV (14 %), and NPV (99 %) for PAX8. In papillary type, Napsin A sensitivity, specificity, PPV, and NPV were 82, 82, 21, and 99 % respectively, while in PAX8 were 100, 57, 13, and 100 % respectively. In chromophobe type, sensitivity, specificity, PPV, and NPV were 17, 78, 2, and 97 % respectively for Napsin A and 83, 56, 6, and 99 % respectively for PAX8. Specificity of Napsin A in renal cell carcinoma as a total and for the entire examined variant was more than PAX8 but the sensitivity of PAX8 was more than Napsin A; this indicated that PAX8 was more sensitive and less specific than Napsin A in renal cell carcinoma as shown in Table 4.
Sensitivity, specificity, PPV, and NPV of immunohistochemical positive expression of Napsin A, TTF-1, and PAX8 in diagnosis of primary carcinoma from other examined carcinomas
Sensitivity, specificity, PPV, and NPV of Napsin A, TTF-1, and PAX8 in diagnosis of primary carcinomas from other carcinomas were shown in Table 5.
When examining lung cancer from other carcinomas, we found that the sensitivity of Napsin A and TTF-1 were 54 and 52 % respectively, as regarding the specificity Napsin A was more specific than TTF-1 (80, 68 % respectively). In Fig. 2b, the mean of area under ROC curve for Napsin A was 0.76 with confidence interval (0.69–0.81) and for TTF-1 was 0.75 with confidence interval (0.68–0.80) and p value = 0.31.
Regarding thyroid carcinomas from other carcinomas, we found that TTF-1 was less sensitive (93 %) but more specific (93 %) than PAX8 which was sensitive in 97 % and specific in 81 %. The mean area under ROC curve for TTF-1 was 0.96 with confidence interval (0.93–0.98) and for PAX8 was 98 with confidence interval (0.95–0.99) and p value = 0.31 as shown in Chart Fig. 2c.
As regarding renal cell carcinoma from other examined carcinomas, we found that Napsin A was more specific (93 %) than TTF-1 (50 %) but it was more specific (88 %) than Napsin A (83 %). The mean of area under ROC curve for Napsin A was 0.75 with confidence interval (0.68–0.80) and for PAX 8 was 0.96 with confidence interval (0.93–0.98) and p value <0.001 shown in Fig. 2d.
In ovarian and endometrial carcinoma, PAX8 specificity was 80 and 100 % respectively, more than TTF-1 which was 5 and 13 % respectively, also the sensitivity of PAX8 (75 % for both carcinomas) was more than TTF-1 (59, 61 %) respectively; this indicated that PAX8 was more sensitive and more specific than TTF-1 in ovarian and endometrial carcinoma.
Sensitivity, specificity, PPV, and NPV of immunohistochemical positive expression of Napsin A, TTF-1, and PAX8 in diagnosis of primary carcinoma
Sensitivity, specificity, PPV, and NPV of immunohistochemical positive expression of Napsin A, TTF-1, and PAX8 in diagnosis of primary carcinoma as shown in Table 6.
As regarding Napsin A which was expressed in lung and renal carcinoma when compared to other carcinomas, we found Napsin A sensitivity (54 %) and specificity (100 %) for lung carcinoma from other carcinomas except renal carcinomas. Napsin A sensitivity and specificity were 93, 100 % respectively for renal carcinoma from other carcinomas except lung carcinoma.
For TTF-1, when examining lung carcinoma compared to other carcinomas except thyroid, we found that TTF-1 was less sensitive (52 %) but more specific (96 %) for diagnosis of lung carcinoma. TTF-1 sensitivity and specificity were 93 and 96 % respectively for thyroid carcinomas from other carcinomas except lung carcinoma.
PAX8 sensitivity and specificity were 98 and 100 % respectively for thyroid carcinoma compared to other carcinomas except renal, ovarian, and endometrial carcinomas. Renal cell carcinoma sensitivity was 93 % and specificity was 100 % compared to other examined carcinomas except thyroid, ovarian, and endometrial carcinomas. PAX8 sensitivity (80 %) and specificity (100 %) were for ovarian carcinoma compared to other carcinomas except thyroid, renal, and endometrial carcinomas. Endometrial cancer sensitivity and specificity were 100 % for both from other examined carcinomas except thyroid, renal and ovarian carcinomas.
Discussion
With recent advances in targeted therapies, histologic typing of NSCLC has become important [1]; however, the diagnostic accuracy has not always been satisfactory [8]. Both primary lung AC and metastatic carcinomas from other organs are common in the peripheral lung field, and their differential diagnoses are sometimes difficult. Therefore, specific markers for primary lung AC are needed to distinguish between both lesions [11].
To the best of our knowledge, this study is the second research in differentiating primary lung AC from other AC using Napsin A, TTF-1, and PAX8 following the first one by [7]. The formal study used a restricted number of cases and compared the expression of study markers in metastasize AC and primary AC of the lung. The current study used larger number of cases and compared primary AC from different site with that of lung, making our results more reliable.
In this study, we found that Napsin A expression rate in lung carcinoma was 54 % which was in concordance with previous studies reported that Napsin A expression ranged from 48.5 to 87.1 % [2, 15, 16, 18, 22]. Napsin A expression was positive in 50 % of renal cell carcinoma, which was slightly lower than 57 % reported by [15]. On studying extrapulmonary carcinomas, we found no Napsin A expression in thyroid, breast, ovary, endometrium, and colon carcinomas. These results are largely in accordance with previous results [1, 2, 11, 15].
Our data demonstrated high frequency of Napsin A staining in primary lung AC, compared with other carcinomas. This result was consistent with previous studies [11, 23]. This study supports the efficacy of Napsin A as a marker for lung AC, distinguishing primary lung AC from other carcinomas which metastasize to the lung except for renal cell carcinoma cases.
In the current study, TTF-1 expression was found in 52 % of primary lung carcinoma. TTF-1 positive expression rates ranged from 39 to 85 % for lung AC as reported by previous studies [2, 16–18]. In thyroid carcinoma, the present study showed TTF-1 positive immunostaining in 93.3 % of cases. A similar result was reported [1, 2, 7, 12, 15]. TTF-1 is rarely expressed in tumors of extrapulmonary origin [2, 25, 26].
In this study, TTF-1 was positive in small number of carcinoma from endometrium and ovary, and similar results were reported in previous studies by [1, 7, 12, 26]. Although the reported frequency of positivity of TTF-1 is low in this carcinoma, this can lead to an incorrect diagnosis. Thus, TTF-1 is a potentially useful marker in differentiating metastatic pulmonary from extrapulmonary adenocarcinoma, provided that the possibility of thyroid origin has been excluded.
Previous studies have shown that PAX 8 was noticed in thyroid (89–91 %) [22, 23], most renal cell (90 %) [17, 22, 23], ovarian (64–100 %) [20, 22, 27–29], and endometrial (93–98 %) [22, 23] carcinomas. Consistent with these reports, we found that carcinomas from these organs were positive for PAX8 immunostaining. As expected, PAX8 was completely negative in primary lung AC, which was consistent with previous reports [21–24].
These findings indicate that PAX8 is a valuable diagnostic biomarker for differentiating primary lung AC from carcinomas of these organs. Consistent with previous reports of [21, 28, 30], our results showed that PAX8 was negative in all of non-Mullerian carcinomas (except for thyroid and renal carcinomas), which indicated its higher specificity.
Our study and previous studies suggested that PAX8 expression was an extremely valuable tool in clinical application; however, as with any immunohistochemical stain, the results should not be evaluated in segregation or without the clinical situation for each case, and H&E morphology must always be considered.
In the present study, comparing markers expression in AC and SCC cases, we found that 54 % of all lung carcinoma were positive for Napsin A immunostaining. Eighty-six percent of AC cases and 6.7 % cases of SCC were positive for Napsin A expression. In addition, 52 % of primary lung carcinomas showed positive TTF-1 immunostaining including 83.3 % AC and 1.7 % SCC. We found that the overall sensitivity and specificity were greater for Napsin A than for TTF-1, and for AC the sensitivity and specificity of Napsin A were slightly greater than TTF-1.
These results were consistent with previous studies of Napsin A which found that the sensitivity and specificity were similar or higher than that of TTF-1 in the identification of lung AC. The sensitivity and specificity of Napsin A were 79–84 and 94–100 %, respectively and those of TTF-1 were 84 and 76–97 % respectively in the diagnosis of lung AC [1, 2, 11, 15–18]. On the contrary, previous studies demonstrated lower sensitivity of Napsin A 33–60 % than TTF-1 54–90 % [24, 31]. We have shown that a combined Napsin A (+)/TTF-1 (+) and PAX8 (−) immunoprofile patterns were highly sensitive and specific for primary lung AC. Similar finding was reported by [7, 12].
Currently, TTF-1 is a commonly used marker for confirming the diagnosis of pulmonary AC. The high sensitivity and specificity of TTF-1 for lung AC has been reported by previous studies [24, 31]. In the current study, TTF-1 staining was positive in the great majority of lung AC specimens (83.3 %). On the other hand, TTF-1 was detected in 6.7 % of SCC cases. Although TTF-1 is usually not detected in SCC [2, 24, 32], previously published data demonstrated that 3–21 % of SCC were TTF-1 positive [32, 33] as well as our study.
Regarding thyroid carcinoma, we showed TTF-1 positive immunostaining in 93.3 % of cases. Among cases, 87.5 and 100 % of papillary and follicular thyroid carcinomas were positive for TTF-1 respectively. A similar result was reported by [1, 2, 7, 12, 15]. Therefore, it is sometimes difficult to distinguish primary lung AC from metastatic AC of thyroid origin using TTF-1 IHC [11]. On the contrary, all examined thyroid carcinoma cases were negative for Napsin A, suggesting Napsin A is a valuable marker in differentiating primary lung carcinoma from thyroid carcinoma.
Our study showed PAX8 immunostaining in 96.7 % of thyroid carcinoma, which was positive in 93.8 % of papillary and in all cases of follicular carcinomas. Similar finding was reported by previous studies [12, 19, 20, 28, 30]. The use of PAX8 IHC may be a suitable marker.
The present study showed that the sensitivity of TTF-1 and PAX8 were approximately equal in thyroid carcinoma while TTF-1 was more specific than PAX8. TTF-1 was more specific but less sensitive than PAX8 in all examined cases of thyroid carcinoma and papillary thyroid carcinoma. In follicular thyroid carcinoma, TTF-1 was more specific than PAX8 while the sensitivity was equal reaching 100 % for both markers.
The co-expression of TTF-1 (+)/PAX8 (+) and Napsin A (−) immunoprofiles, especially in a metastatic site, is diagnostic of a primary thyroid carcinoma and excludes a TTF-1 expressing lung AC. These observations clearly indicate PAX8 as a sensitive and specific marker for thyroid differentiation.
In renal cell carcinoma, Napsin A expression, we found that 38.5 % of clear cell, 72.9 % of papillary, and 16.7 % chromophobe renal cell carcinomas were positive for Napsin A, and all the cases were negative for TTF-1. Earlier studies have shown that 33 % of clear cell, 80 % of papillary, and 3 % of chromophobe renal cell carcinomas were positive for Napsin A and negative for TTF-1 [1, 2, 12, 25].
In the current study, we found that 96.7 % of renal cell carcinoma including 92.2 % of clear cell RCC, 100 % of papillary RCC, and 83.3 % chromophobe renal cell carcinomas were positive for PAX8 immunostaining. Previous studies were reported that PAX8 was positive in approximately all cases of renal cell carcinoma [1, 20, 22, 23, 34]. It was positive in 93–7 % of clear cell RCC, 76–100 % of papillary RCC, and 80–88 % chromophobe renal cell carcinomas [22, 23, 35].
In renal cell carcinoma cases, specificity of Napsin A expression showed less sensitivity and higher specificity than PAX8. Considering renal cell carcinoma subtypes, we found 38 % sensitivity and 79 % specificity for Napsin A and 92 % sensitivity and 58 % specificity for PAX8 in clear cell type. In papillary type, Napsin A sensitivity and specificity were 82 and 82 % respectively, while PAX8 were 100, 57, 13, and 100 % respectively. Specificity of Napsin A in renal cell carcinoma as a total and for the entire examined variant was more than PAX8, but the sensitivity of PAX8 was more than Napsin A, indicating that PAX8 was more sensitive and less specific than Napsin A in renal cell carcinoma. Previous study reported that PAX8 sensitivity was 92 % [36]. Therefore, our results together with previous studies suggested that PAX8 was a useful adjunct for confirmation of RCC diagnoses. We have shown that PAX8 (+), Napsin A (+), and TTF-1 (−) immunoprofiles were useful for differentiating primary lung AC from renal cell carcinoma.
In the current study, positive PAX8 expression was detected in 80 % of ovarian carcinoma. All cases of serous carcinoma and 60 % of mucinous carcinoma were PAX8 positive. Several studies have shown that a great proportion of ovarian carcinomas were immunoreactive for PAX8 [19, 21, 23, 27–29, 37–39].
PAX8 expression was detected in 79–100 % of ovarian serous carcinoma [27, 37, 38] and ranged from 0 to 50 % in mucinous carcinoma [24, 34]. In this study, we showed that detection of PAX8 in ovarian mucinous carcinoma confirmed the diagnosis of a primary ovarian carcinoma over a metastasis from the gastrointestinal tract, as none of carcinoma of colon, stomach, and esophagus was positive for PAX8 expression. Similar results were reported by [24, 34].
Ovarian and breast cancers encompass various histopathological variants, clinical behaviors, and prognosis. Both are commonly metastasizing carcinomas, and their metastases are histological similar, resulting in difficulty in distinguishing between them [40]. In this study, no Napsin A or TTF-1 expression was found in our specimens of AC of breast or ovarian origin. Moreover, PAX8 staining was absent in all breast carcinoma. These findings were consistent with previous studies [7, 9, 19, 20, 24, 28, 29]. This finding indicated that PAX8 was a more superior marker for the differential diagnosis of ovarian and breast cancer in metastatic sites.
In endometrial carcinoma, we found that PAX8 was positive on all examined cases. The results of this study were similar to that of [24, 27, 34, 39]. Overall, these findings confirmed the suggestions of previous studies regarding the sensitivity of this marker.
The sensitivity and specificity of PAX8 by IHC for differentiation of Mullerian from non-Mullerian carcinomas were 78.4 and 97.3 %, respectively [24].
Hepatocellular carcinoma may show morphologic overlap with RCC. Consistent with previous studies [7, 22, 34], hepatocellular carcinoma was negative for PAX8 expression, making it a useful marker to distinguish among carcinomas of unknown primary site.
In conclusion, the combination of Napsin A, TTF-1, and PAX8 is suggested as the best panel of IHC markers in distinguishing between primary lung AC and metastatic carcinoma to the lung. Napsin A appears to be a useful marker when used in conjunction with TTF-1 because it provides high sensitivity and specificity for both sorting primary lung carcinoma as AC and for identifying lung origin in the setting of a metastatic AC. This is particularly important in view of recent advances in the treatment of non-small cell carcinomas and in particular, of AC of the lung. PAX 8 is a highly sensitive and specific marker for carcinomas of renal, thyroid, and Müllerian origins and is suggested as beneficial marker to distinguish between primary lung AC and metastatic AC from thyroid, renal, and Müllerian carcinomas.
References
Bishop JA, Sharma R, Illei PB. Napsin A and thyroid transcription factor-1 expression in carcinomas of the lung, breast, pancreas, colon, kidney, thyroid, and malignant mesothelioma. Hum Pathol. 2010;41(1):20–5.
Brown AF, Sirohi D, Fukuoka J, Cagle PT, Policarpio-Nicolas M, Tacha D, et al. Tissue-preserving antibody cocktails to differentiate primary squamous cell carcinoma, adenocarcinoma, and small cell carcinoma of lung. Arch Pathol Lab Med. 2013;137(9):1274–81.
Mukhopadhyay S, Katzenstein AL. Subclassification of non-small cell lung carcinomas lacking morphologic differentiation on biopsy specimens: utility of an immunohistochemical panel containing TTF-1, napsin A, p63, and CK5/6. Am J Surg Pathol. 2011;35(1):15–25.
Stang A, Pohlabeln H, Muller KM, Jahn I, Giersiepen K, Jockel KH. Diagnostic agreement in the histopathological evaluation of lung cancer tissue in a population-based case–control study. Lung Cancer. 2006;52(1):29–36.
Antic T, Gong Y, Sneige N. Tumor type and single cell/mesothelial-like cell pattern of breast carcinoma metastases in pleural and peritoneal effusions. Diagn Cytopathol. 2012;40(4):311–5.
Varadhachary GR, Abbruzzese JL, Lenzi R. Diagnostic strategies for unknown primary cancer. Cancer. 2004;100(9):1776–85.
Ye J, Hameed O, Findeis-Hosey JJ, Fan L, Li F, McMahon LA, et al. Diagnostic utility of PAX8, TTF-1 and Napsin A for discriminating metastatic carcinoma from primary adenocarcinoma of the lung. Biotech Histochem. 2012;87(1):30–4.
Loo PS, Thomas SC, Nicolson MC, Fyfe MN, Kerr KM. Subtyping of undifferentiated non-small cell carcinomas in bronchial biopsy specimens. J Thorac Oncol. 2010;5(4):442–7.
Stoll LM, Johnson MW, Gabrielson E, Askin F, Clark DP, Li QK. The utility of Napsin-A in the identification of primary and metastaticlung adenocarcinoma among cytologically poorly differentiated carcinomas. Cancer Cytopathol. 2010;118(6):441–9.
Bishop JA, Benjamin H, Cholakh H, Chajut A, Clark DP, Westra WH. Accurate classification of non-small cell lung carcinoma using a novel microRNA-based approach. Clin Cancer Res. 2013;16(2):610–9.
Hirano T, Gong Y, Yoshida K, Kato Y, Yashima K, Maeda M, et al. Usefulness of TAO2 (napsin A) to distinguish primary lung adenocarcinoma from metastatic lung adenocarcinoma. Lung Cancer. 2003;41(2):155–62.
Ye J, Findeis-Hosey JJ, Yang Q, McMahon LA, Yao JL, Li F, et al. Combination of napsin A and TTF-1immunohistochemistry helps in differentiating primary lung adenocarcinoma from metastatic carcinoma in the lung. Appl Immunohistochem Mol Morphol. 2011;19(4):313–7.
Gu K, Shah V, Ma C, Zhang L, Yang M. Cytoplasmic immunoreactivity of thyroid transcription factor-1 (clone 8G7G3/1) in hepatocytes true positivity or cross-reaction? Am J Clin Pathol. 2007;128(3):382–8.
DeFelice M, Silberschmidt D, DiLauro R, Xu Y, Wert SE, Weaver TE, et al. TTF-1 phosphorylation is required for peripheral lung morphogenesis, perinatal survival, and tissue-specific gene expression. J Biol Chem. 2003;278(37):35574–83.
Turner BM, Cagle PT, Sainz IM, Fukuoka J, Shen SS, Jagirdar J. Napsin A, a new marker for lung adenocarcinoma, is complementary and more sensitive and specific than thyroid transcription factor 1 in the differential diagnosis of primary pulmonary carcinoma: evaluation of 1674 cases by tissue microarray. Arch Pathol Lab Med. 2012;136(2):163–71.
Kim MJ, Shin HC, Shin KC, Ro JY. Best immunohistochemical panel in distinguishing adenocarcinoma from squamous cell carcinoma of lung: tissue microarray assay in resected lung cancer specimens. Ann Diagn Pathol. 2013;17(1):85–90.
Ao MH, Zhang H, Sakowski L, Sharma R, Illei PB, Gabrielson E, et al. The utility of a novel triple marker (combination of TTF1, napsin A, and p40) in the subclassification of non-small cell lung cancer. Hum Pathol. 2014;45(5):926–34.
Sun T, Xie H, Kong L. Role of p40 (ΔNP63), p63, thyroid transcritpion factor-1 and Napsin A in differential diagnosis between lung squamous cell carcinoma and lung adenocarcinoma. Acta Med Mediterr. 2014;30:923–7.
Nitsch R, Di Dato V, di Gennaro A, de Cristofaro T, Abbondante S, De Felice M, et al. Comparative genomics reveals a functional thyroidspecific element in the far upstream region of the PAX8 gene. BMC Genomics. 2010;11:306.
Albadine R, Schultz L, Illei P, Ertoy D, Hicks J, Sharma R, et al. PAX8 (+)/p63 (−) immunostaining pattern in renal collecting duct carcinoma (CDC): a useful immunoprofile in the differential diagnosis of CDC versus urothelial carcinoma of upper urinary tract. Am J Surg Pathol. 2010;34(7):965–9.
Lotan TL, Ye H, Melamed J, Wu XR, Shih Ie M, Epstein JI. Immunohistochemical panel to identify the primary site of invasive micropapillary carcinoma. Am J Surg Pathol. 2009;33(7):1037–41.
Ozcan A, Shen SS, Hamilton C, Anjana K, Coffey D, Krishnan B, et al. PAX 8 expression in non-neoplastic tissues, primary tumors, and metastatic tumors: a comprehensive immunohistochemical study. Mod Pathol. 2011;24(6):751–64.
Laury AR, Perets R, Piao H, Krane JF, Barletta JA, French C, et al. A comprehensive analysis of PAX8 expression in human epithelial tumors. Am J Surg Pathol. 2011;35(6):816–26.
Heidarpour M, Tavanafar Z. Diagnostic utility of PAX8 in differentiation of mullerian from non-mullerian tumors. Adv Biomed Res. 2014;3:96.
Zhang P, Han YP, Huang L, Li Q, Ma DL. Value of Napsin A and thyroid transcription factor-1 in the identification of primary lung adenocarcinoma. Oncol Lett. 2010;1(5):899–903.
Siami K, McCluggage WG, Ordonez NG, Euscher ED, Malpica A, Sneige N, et al. Thyroid transcription factor-1 expression in endometrial and endocervical adenocarcinomas. Am J Surg Pathol. 2007;31(11):1759–63.
Bowen NJ, Logani S, Dickerson EB, Kapa LB, Akhtar M, Benigno BB, et al. Emerging roles for PAX8 in ovarian cancer and endosalpingeal development. Gynecol Oncol. 2007;104(2):331–7.
Nonaka D, Tang Y, Chiriboga L, Rivera M, Ghossein R. Diagnostic utility of thyroid transcription factors Pax8 and TTF-2 (FoxE1) in thyroid epithelial neoplasms. Mod Pathol. 2008;21(2):192–200.
Laury AR, Hornick JL, Perets R, Krane JF, Corson J, Drapkin R, et al. PAX 8 reliably distinguishes ovarian serous tumors from malignant mesothelioma. Am J Surg Pathol. 2010;34(5):627–35.
Wiseman W, Michael CW, Roh MH. Diagnostic utility of PAX8 and PAX2 immunohistochemistry in the identification of metastatic Müllerian carcinoma in effusions. Diagn Cytopathol. 2011;39(9):651–6.
Terry J, Leung S, Laskin J, Leslie KO, Gown AM, Ionescu DN. Optimal immunohistochemical markers for distinguishing lung adenocarcinomas from squamous cell carcinomas in small tumor samples. Am J Surg Pathol. 2010;34(12):1805–11.
Kim GY, Lim SJ, Kim WS, Lee GK. A minimal immunohistochemical panel for subtyping poorly differentiated non-small cell lung carcinoma: a tissue microarray study simulating small biopsy conditions. J Lung Cancer. 2012;11(1):21–32.
Downey P, Cummins R, Moran M, Gulmann C. If it’s not CK5/6 positive, TTF-1 negative it’s not a squamous cell carcinoma of lung. APMIS. 2008;116(6):526–9.
Tacha D, Zhou D, Cheng L. Expression of PAX8 in normal and neoplastic tissues: a comprehensive immunohistochemical study. Appl Immunohistochem Mol Morphol. 2011;19(4):293–9.
Ozcan A, de la Roza G, Ro JY, Shen SS, Truong LD. PAX2 and PAX8 expression in primary and metastatic renal tumors: a comprehensive comparison. Arch Pathol Lab Med. 2012;136(12):1541–51.
Knoepp SM, Kunju LP, Roh MH. Utility of PAX8 and PAX2 immunohistochemistry in the identification of renal cell carcinoma in diagnostic cytology. Diagn Cytopathol. 2012;40(8):667–72.
Liliac L, Carcangiu ML, Canevari S, Căruntu ID, Ciobanu Apostol DG, Danciu M, et al. The value of PAX8 and WT1 molecules in ovarian cancer diagnosis. Rom J Morphol Embryol. 2013;54(1):17–27.
Wang M, Ma H, Pan Y, Xiao W, Li J, Yu J, et al. PAX2 and PAX8 reliably distinguishes ovarian serous tumors from mucinous tumors. Appl Immunohistochem Mol Morphol. 2015;23(4):280–7.
Tong GX, Devaraj K, Hamele-Bena D, Yu WM, Turk A, Chen X, et al. Pax8: a marker for carcinoma of Müllerian origin in serous effusions. Diagn Cytopathol. 2011;39(8):567–74.
Xiang L, Kong B. PAX8 is a novel marker for differentiating between various types of tumor, particularly ovarian epithelial carcinomas. Oncol Lett. 2013;5(3):735–8.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
El-Maqsoud, N.M.R.A., Tawfiek, E.R., Abdelmeged, A. et al. The diagnostic utility of the triple markers Napsin A, TTF-1, and PAX8 in differentiating between primary and metastatic lung carcinomas. Tumor Biol. 37, 3123–3134 (2016). https://doi.org/10.1007/s13277-015-3964-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-015-3964-3