
Abstract
Non-small cell lung cancer (NSCLC) is the common type of lung cancer, which is the leading cause of cancer death throughout the world. Most patients were diagnosed too late for curative treatment. So, it is necessary to develop a minimal invasive method to identify NSCLC at an early stage. In recent years, cell-free circulating tumor DNA (ctDNA) has attracted increasing attention as a potential tumor marker for its minimal invasive, convenient, and easily accepted properties. The amount of ctDNA in plasma or serum was significantly higher in NSCLC patients than that in healthy controls or patients with benign diseases. Furthermore, many studies have proved an association among tumor stage, tumor grade, lymph node involvement, the number of metastatic sites, tumor response, survival outcome, and the ctDNA levels. Many genetic changes, such as gene mutation, loss of heterozygosity, microsatellite instability, and gene methylation were also found in ctDNA in NSCLC patients. These findings demonstrated that the ctDNA could serve as a viable tool to monitor NSCLC and prompted us to find more sensitive and specific biomarkers for clinical practice, especially monitor these cases with at least one known gene abnormality. Here, we reviewed the evidence of ctDNA in NSCLC and consider possible future applications in patient management.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lung cancer is the leading cancer killer in the World. An estimated 160,340 Americans were expected to die from lung cancer in 2012, accounting for approximately 28 % of all cancer deaths [1]. The number of deaths due to lung cancer has increased approximately 4.3 % between 1999 and 2008. Non-small cell lung cancer (NSCLC) is the most common type of lung cancer [2]. About 85 % of all lung cancers are identified as NSCLC, and approximately 75 % of these are metastatic or advanced at diagnosis [3]. Earlier tumor detection is associated with excellent survival. The overall 5-year survival rate was 60–80 % in stage I and 40–50 % in stage II NSCLC after the patients were given surgical resection [4]. However, the current screening tests employed in clinical practice are not good at detecting NSCLC at the early stage, and this is a key factor in the high mortality rate of the disease. So, it is necessary to develop new methods to facilitate the early and rapid detection of NSCLC.
In the recent years, cell-free circulating tumor DNA (ctDNA) has attracted more and more attention as a potential tumor marker for its minimal invasive, convenient, and easily accepted properties. The level of ctDNA in healthy controls is low, but it is obviously increased in the blood of NSCLC patients [5, 6]. Some studies reported that ctDNA could be used as a significant predictor of disease progression in patients undergoing chemotherapy [7, 8]. Other studies found a relationship between the ctDNA concentrations and the patients’ outcome [6, 8, 9]. Moreover, an obvious transient rise in the concentrations of ctDNA in NSCLC patients occurred immediately after chemotherapy or tumor resection, followed by a rapid decrease [10]. These observations suggested that the kinetics of tumor-specific DNA in plasma may reflect tumor burden, i.e., the rapid cell death following treatment may release tumor cell DNA into the circulation, which decreases as the tumor regresses.
Although the precise mechanism of DNA release into the blood is not clear until now, many studies indicated that lysis of tumor may be the main source of the DNA found in plasma/serum of cancer patients and cell death by apoptosis or necrosis possibly play important roles in the process (Fig. 1) [11, 12]. Cancer treatment by radiotherapy and chemotherapy can cause cell death by apoptosis. The chromosomal DNA in the apoptotic bodies is degraded, and then the DNA fragments are released into the circulation. Necrotic cells also produce a large amount of ctDNA. Furthermore, inflammation frequently occurring in cancer also involves the increase in ctDNA [13]. Some studies have proved that the ctDNA in cancer patients mimics cancer cell DNA. In other words, tumor-specific genetic alterations are also found in ctDNA in cancer patients [14]. Therefore, ctDNA might be a highly promising biomarker in the examination of tumor DNA and could be applied in diagnosis, prognosis, and follow-up cancer testing in the future.

Possible source of circulating tumor DNA. Cell-free circulating tumor DNA (ctDNA) is thought to originate from apoptotic and necrotic cells of the primary or metastatic tumor, which discharge DNA early during tumorigenesis. The physiology and rate of release is still not well understood; tumor burden and tumor cell proliferation rate may have a substantial role in these events. Many genetic changes, such as gene mutation, loss of heterozygosity, microsatellite instability, and gene methylation, which were thought to be cancer biomarkers, were found in ctDNA in NSCLC patients
In this review, we summarized the evidence in ctDNA in the blood of NSCLC patients and consider possible future applications in patient management (Fig. 2).

Quantitative analysis of circulating tumor DNA level and genetic changes. Besides the changes in ctDNA levels in the NSCLC patients, some tumor-specific changes of ctDNA have also been detected, including gene mutation, microsatellite alterations, and gene hypermethylation. These genetic changes provide clues to understand the initiation, progression, and metastasis of cancer. The circulating tumor DNA concentration was determined by PCR or fluorescence methods after the ctDNA was extracted from the plasma or serum of NSCLC patients. Gene mutations in ctDNA can be detected by many methods, including qPCR, ME-PCR, qPCR and direct sequencing, PCR-RFLP, PCR-SSCP, PCR-ARMS, PNA-LNA PCR clamp, DHPLC, digital PCR, and NGS. These methods each have its own advantages and disadvantages, so the primary considerations when choosing a method are sensitivity, specificity, the cost per genotype, and throughput. Microsatellite alterations can be detected by PCR technology to observe band shifts and allele losses. Gene hypermethylation can be evaluated by methylation-specific PCR
Quantitation of ctDNA in NSCLC patients
As early as 1965, Bendich et al. [15] had proven that ctDNA was an important vehicle of oncogenesis. Then, Leon et al. [16] determined the free ctDNA in the serum of cancer patients using radioimmunoassay method and proved that the ctDNA could serve as a valuable tool to monitor the efficiency of anticancer therapy. After that, hundreds of papers on ctDNA in different cancer types have been published every year, and many novel quantification methods were developed and employed to detect ctDNA precisely. In recent years, with the rapid development of polymerase chain reaction (PCR)-based techniques and their widespread application, those methods used in early studies have been replaced gradually by PCR, including radioimmunoassay, enzyme-linked immunosorbent assay (ELISA), DNA dipstick, dot-hybridization, and nick translation. Furthermore, direct fluorescent PicoGreen staining was also employed by some researchers for DNA quantification due to its advantages of being inexpensive, less time-consuming, and relatively high sensitivity [17]. For example, Ulivi et al. [5] examined the level of free ctDNA in both 100 healthy donors and 100 NSCLC patients by real-time quantitative PCR (qPCR). The results showed that free ctDNA level was significantly higher in NSCLC patients than in healthy donors. The median value of ctDNA was 47.2 ng/ml (range, 0.7–251) for patients and 9.2 ng/ml (range, 2.2–184) for healthy donors. Catarino et al. [6] determined the amounts of ctDNA in both NSCLC patients and healthy individuals by qPCR. They found increased ctDNA levels in NSCLC patients compared with control individuals. A decreased overall survival time can be observed in patients presenting high ctDNA levels when compared with lower ctDNA concentrations. Kumar et al. [17] assessed the plasma ctDNA levels in 42 NSCLC patients and 100 patients with benign diseases by a fluorescence detection method. A significantly lower plasma ctDNA level was found in patients with remission or stable disease than in those with progression. Higher levels and insufficient decrease in plasma ctDNA levels during the course of chemotherapy indicated poor outcome. Monitoring of plasma ctDNA levels during the course of chemotherapy could identify patients who are likely to exhibit an insufficient therapeutic response and disease progression at an early stage. All these results suggested that quantification of ctDNA may be a good tool for NSCLC detection with potential for clinical applicability and could lead to better management of advanced-stage lung cancer.
The results of studies reporting the levels of ctDNA in NSCLC patients are shown in Table 1. From Table 1, we can see that almost all studies employed the QIAamp DNA Mini kit or DNA Blood Mini kit to isolate DNA from plasma or serum. Apart from two studies using fluorescence detection method with PicoGreen dsDNA kit [17, 24], most of the studies determined the concentration of ctDNA by qPCR [5, 6, 8–10, 18–23]. At present, qPCR is regarded as a standard method for DNA quantification, characterized by high accuracy, reproducibility, and time effectiveness. A significant advantage of qPCR is its ability to detect and quantify DNA samples even from very small amounts of starting material. When using the same DNA extraction method, as little as 2 μl of DNA sample extracted from 8 μl of plasma is enough to quantify ctDNA concentration by qPCR [8], whereas 50 μl of DNA sample obtained from 200 μl of plasma is required by PicoGreen assay [17]. It should be noted that efficient qPCR largely depends on high-quality probe design, including probe molecule sequence, length, concentration, and G-C compositions. For example, a TaqMan probe is the most frequently used probe for qPCR technique, and its length should be 18 to 32 bases for optimal PCR efficiency. Increasing probe’s length can increase sensitivity, but will lead to decreased specificity. There is considerable variation in the reported results, with estimates of median ctDNA levels ranging from 4.3 to 270 ng/ml in the NSCLC patients and 2.0 to 122.7 ng/ml in the controls, reflecting a number of problems in interpreting these data. Although the plasma/serum ctDNA levels varied widely across studies, overall higher ctDNA concentrations were detected in both patients and their corresponding controls in the same study and vice versa. This suggested that different laboratory procedures and techniques utilized for quantification of ctDNA might be the main reasons for the differences in ctDNA levels among laboratories. Different reference genes, such as GAPDH, β-actin, or hTERT, were used to calculate the level of ctDNA in many studies, which might partly explain the inconsistent results across studies. Furthermore, many studies have proved an association among tumor stage, tumor grade, lymph node involvement, the number of metastatic sites, tumor response, survival outcome, and the ctDNA levels, indicating that individual differences cannot be ignored. Most of the studies compared the differences in levels of ctDNA between patients and control cases, including healthy controls or patients with benign diseases. Most of the researchers took into account the issue of consistency between controls and NSCLC patients, and both of them were matched in age, sex, geographic area, smoking history, and comorbidity. Furthermore, study size was usually small, so it is necessary to increase the number of patients enrolled in the study to provide convincing evidence in the future.
Genetic changes in ctDNA in NSCLC
Besides the changes in the levels of ctDNA in the blood of NSCLC patients, some tumor-specific changes of ctDNA have also been detected, including mutation in oncogenes or tumor-suppressor genes, microsatellite alterations, hypermethylation of promoter genes, and chromosomal rearrangements. These genetic changes provide clues to understand the initiation, progression, and metastasis of cancer. Therefore, the detection of multiple genetic changes in ctDNA can help in diagnosis, assessment of response to treatment, and evaluation of recurrence.
Gene mutation
Many methods can be used to detect gene mutations in ctDNA in NSCLC, including qPCR [25, 26], mutant-enriched PCR (ME-PCR) [27–29], qPCR and direct sequencing [30], PCR-restriction fragment length polymorphism (RFLP) [31], PCR-single-strand conformational polymorphism (SSCP), PCR-amplification refractory mutation system (ARMS) [32], peptide nucleic acid-locked nucleic acid PCR clamp (PNA-LNA PCR clamp) [33], denaturing high-performance liquid chromatography (DHPLC) [34], digital PCR [35], and next-generation sequencing (NGS) [36]. Some of them can be used to identify known mutations (i.e., most PCR-based techniques), and others can be employed to screen unknown mutations (i.e., next-generation sequencing).
Most methods of mutation detection depend on PCR technique. In these methods, conventional or modified PCR techniques are employed to selectively amplify specific target DNA sequence, and then the amplified products are analyzed by electrophoresis or some other methods to find possible mutations within the sequences. At present, direct sequencing of PCR products is still considered the gold standard for gene mutation analysis and can be used to detect novel mutations, but its sensitivity is relatively low (about 20 %) [37]. To improve the selectivity of PCR-based technologies for enhancing the detection of minority (mutant) alleles in clinical samples, some methods with high sensitivity were developed over the past two decades. For example, qPCR shows increased sensitivity (about 5 %), decreased experimental time, and higher throughput when compared with conventional PCR, but it can only identify known mutations [25]. PCR-SSCP is a reproducible, rapid, and simple method for both known and unknown gene mutations; however, its sensitivity varied dramatically with fragment size; the optimum size was about 150 bp [38]. Both PCR-RFLP and PCR-ARMS are simple and rapid methods with relatively high sensitivity for detection of known mutations, but their final results need to be verified by DNA sequencing [31, 32]. DHPLC detect mutations according to differential retention time of homo- and heteroduplex DNA under conditions of partial thermal denaturation. The main advantages of DHPLC are its high sensitivity and high throughput, coupled with minimal post-PCR manipulation and no requirement for sample labeling, although precise temperature needs to be predicted for analysis of each DNA fragment [39].
In recent years, digital PCR and NGS have been applied more and more in mutation detection in ctDNA. In digital PCR, each sample is diluted and separated into many individual reaction chambers so that each contains one or no copies of the sequence of interest. Then, real-time PCR reaction is carried out in all the chambers, and results are analyzed to get absolute number of PCR target templates present in the original sample. This separation allows a more reliable collection and sensitive measurement of nucleic acid amounts. Compared with qPCR, digital PCR is capable of higher sensitivity and precision and can offer direct quantification without requiring a calibration curve. The method has been demonstrated as useful for studying variations in gene sequences, including copy number variants and point mutations. Yung et al. employed digital PCR to identify epidermal growth factor receptor (EGFR) mutation in ctDNA from the plasma of NSCLC patients [35]. They found that exon 19 deletion and L858R mutation were detectable in 17 and 26 % pretreatment plasma samples, respectively. When compared with the sequencing results of the tumor samples, the sensitivity and specificity of plasma EGFR mutation analysis were 92 and 100 %, respectively. The plasma concentration of the mutant sequences was highly correlated with the clinical response.
Next-generation sequencing (NGS) provides high multiplexing possibilities together with high sensitivity and broad spectrum of detected mutations. NGS can accurately identify low-level mutations down to a level of 2.3 %, with an average coverage of 500×, and with a false discovery rate of less than 1 % [40]. Narayan et al. distinguish circulating Kirsten rat sarcoma 2 viral oncogene homolog (KRAS), BRAF, and EGFR mutations in NSCLC patients by NGS technique [36]. They proved that the method was sensitive and could detect approximately 1 variant in 5000 molecules. Furthermore, the presence or absence of KRAS mutations in all tested tumor tissues was concordant with the findings in plasma.
These methods described above each have their own advantages and disadvantages. Some are not sensitive enough and yield ambiguous results, while others are sensitive but give nonspecific false positives. Also, some of these methods are labor-intensive and time-consuming, and they may require specialized or costly equipment and reagents. Because ctDNA represents only a small fraction of the total circulating DNA, and in many cases, the quantity of wild-type DNA often exceeds the mutant DNA, making it difficult to detect and identify minority alleles present at extremely low concentrations. So, no matter which method is chosen, the primary considerations are sensitivity and specificity, and furthermore, the cost per genotype and throughput should also be taken into account.
In recent years, the key molecular mechanisms underlying tumor initiation, maintenance and progression in NSCLC have been clarified one by one. These findings have led to the development of small molecules that target genetic mutations known to play critical roles in NSCLC.
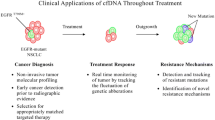
About 10 % of NSCLC patients in the USA and 35 % in East Asia have tumor-associated EGFR mutations [41, 42]. The identification of EGFR mutations not only has offered a screening biomarker to select EGFR mutation-positive patients but also has led to the development of genotype-based targeted therapies directed against EGFR, including gefitinib and erlotinib. Especially erlotinib, which was only approved by the FDA for the second-line treatment of NSCLC in 2004; while in 2013, it was further approved by the FDA for the first-line treatment of metastatic NSCLC with EGFR exon 19 deletions or exon 21 (L858R) mutations. At the same time, the corresponding EGFR mutation test kit (cobas®) was also approved by the FDA [43]. This is the first FDA-approved companion diagnostic that detects EGFR gene mutations, which will lead hopefully to a more personalized and effective treatment of NSCLC (Table 2).
Patients with EGFR gene mutations would eventually develop resistance to these EGFR tyrosine kinase inhibitors (TKIs) [57]. The main resistance mechanisms involved might be a secondary mutation in the EGFR gene (T790M mutation) and amplification of the mesenchymal-epithelial transition (MET) proto-oncogene [58]. T790M could cause steric hindrance and impair the binding of gefitinib/erlotinib and accounts for about half of the acquired-resistant cases [59]. MET amplification accounts for about 20 % of TKI acquired-resistant patients by a different molecular pathway from T790M; some of these patients will also concurrently have T790M mutation [60]. It has recently been reported that T790M mutations present in small fractions of tumor cells before therapy are crucial in response to treatment [61]. Indeed, neoplastic cells carrying this mutation are drug-selected until the tumor becomes widely resistant. Therefore, use of extremely sensitive analytic methods to monitor resistant-inducing mutations in minor clones has been suggested. Fortunately, cobas® EGFR mutation test already includes T790M.
About 4 % of NSCLC patients have a chromosomal rearrangement which generates a fusion gene between anaplastic lymphoma kinase (ALK) and echinoderm microtubule-associated protein-like 4 (EML4), which results in constitutive kinase activity that contributes to carcinogenesis and drives the malignant phenotype [62]. Along with the identification of ALK-activating point mutations, aberrant-activated ALK became a major therapeutic target and a good biomarker to predict tumor response. In addition, crizotinib was the first approved ALK inhibitor by the FDA for the treatment of certain late-stage NSCLC patients carrying abnormal ALK gene [63]. The KRAS gene is mutated in about 25 % of NSCLC patients. Although KRAS mutations have been identified in NSCLC patients for many years, it still cannot become an effective, cost-efficient cancer screening strategies until now [64]. Some studies suggested a potential negative prognostic effect, but other studies did not confirm any negative impact on survival for individuals harboring KRAS mutation. Furthermore, EGFR, KRAS, and ALK are mostly exclusive in patients with NSCLC, and the presence of one mutation in lieu of another can influence response to targeted therapy. Therefore, testing for these mutations and tailoring therapy accordingly is widely accepted as standard practice [65, 66].
Many studies have detected that there were higher frequency of EGFR and KRAS mutations and ALK gene arrangements in the circulation of NSCLC patients than the normal controls and/or patients with benign diseases (Table 2). The significantly improved median progression free survival (PFS) and median overall survival (OS) were found in patients with gene mutations after they were given the targeted treatment. For example, He et al. [27] found that the EGFR mutation rate was 49.3 % by the blood-based, mutant-enriched PCR technology. In the patients treated with gefitinib as a second-line therapy, those with plasma EGFR mutation have a prolonged median PFS compared with those with EGFR wild type (7.6 vs. 2.9 months). On comparing the efficacy of gefitinib with that of docetaxel, it was found that the median PFS was significantly longer for patients treated with gefitinib than those with docetaxel in those harboring plasma EGFR mutation (7.6 vs. 3.2 months). These results suggested that the blood-based EGFR mutations test had the ability to provide a reliable guidance for clinical decision making for the treatment of the advanced NSCLC patients. The results of a study enrolled 246 NCSLC patients showed that 17.5 % of patients presented with KRAS mutation. Patients with a detectable plasma KRAS mutation had a significantly shorter OS and PFS compared with the wild-type patients (median OS 4.8 vs. 9.5 months and median PFS 3.0 vs. 5.6 months). The response rate to chemotherapy was significantly lower in the group of patients with a mutation compared with wild type. The results indicated that the presence of KRAS mutations in plasma may be a marker of poor prognosis and may also hold predictive value [32]. The similar results were also gotten by Wang et al. [31] in their study, KRAS mutation was detected in 12.8 % of NSCLC patients. Among 120 patients who received EGFR-TKI treatment, the response rate was only 5.3 % for patients with plasma KRAS mutation compared with 29.7 % for patients with no KRAS mutation in plasma ctDNA. The median PFS of patients with plasma KRAS mutation was 2.5 months compared with 8.8 months for patients with wild-type KRAS.
When ctDNA was used to take a snapshot of the DNA mutations in NSCLC patients, one key concern was whether or not the genetic variation within blood was consistent with tumor tissue. Indeed, many studies have demonstrated that blood samples could be used to monitor genetic changes in tumor of NSCLC patients over time. Kimura et al. [50] found that in pairs of tumor and serum samples obtained from 11 patients, the EGFR mutation status in the tumors was consistent with those in the serum of 8 of 11 (72.7 %) of the paired samples. Punnoose et al. [45] observed that EGFR mutation status in ctDNA were strongly concordant with the matched tumor tissues, which suggested a potential role for using ctDNA for real-time assessment of mutation status. Wang et al. [31] found that KRAS mutation in plasma ctDNA correlates with the mutation status in the matched tumor tissues of patients with NSCLC. The consistency of KRAS mutations between plasma and tumors is 76.7 %.
Microsatellite instability
Microsatellites are repeated sequences of DNA, which are composed of repeating units of 1–6 bp in length. Microsatellites can be found anywhere in the genome, both in protein-coding and noncoding regions [69]. Due to their high rate of polymorphism, microsatellites are thought as useful genetic markers and play a significant role in many human diseases.
Microsatellite instability (MSI) and loss of heterozygosity (LOH) are the main alterations in microsatellite gene sequence. MSI means somatic alterations in microsatellite sequences due to a deletion or an insertion of one or more repeat units. LOH is the condition that tumor-suppressor genes are generally inactivated by an intragenic mutation within one allele and the subsequent loss of the corresponding allele.
Both MSI and LOH can be detected by PCR technology to observe band shifts and allele losses. Several studies have proven that the occurrence of allele shift and LOH in plasma ctDNA was a frequent and relatively early event in NSCLC. Carpagnano et al. [67] found that microsatellite alterations in ctDNA from whole blood and matched tumor tissues of NSCLC patients presented overlapping profiles of loss of heterozygosity and microsatellite instability, and microsatellite alterations in blood ctDNA from NSCLC patients were significantly more frequent than that in the control subjects. In another study, altogether four markers (D3S1300, D3S1289, D3S1266, and D3S2338) located on chromosome 3p were detected by radiolabeled PCR, and the results showed that microsatellite alterations in at least one locus was found in 39.5 % of NSCLC tumors [20].
Both of the studies used four to five markers, and four of the five markers employed in the two studies were the same (Table 3). The better sensitivity (94 %) for detecting microsatellite alterations in ctDNA was reported by Carpagnano et al. [67] who used five markers. Choice of microsatellite alterations could influence the results. Microsatellite alterations in NSCLC are restricted to single loci [70]. Hence, to detect microsatellite alterations, one must select markers which display a high polymorphism rate and are changed in most, if not all, of the tumor cells. A lower plasma frequency of allelic imbalance may be observed for larger-sized gene products because plasma ctDNA is highly fragmented and alterations may therefore be detected more easily if the sequence to be amplified is smaller than 200 bp [71]. To compare the results obtained in different laboratories, it is necessary to standardize the methods used and to select an optimized panel of genetic markers.
Gene hypermethylation
Hypermethylation of CpG islands in the promoter regions of genes is a common phenomenon in NSCLC. Hypermethylation represses transcription of the promoter regions of genes, leading to gene silencing, and is particularly important in inactivating tumor-suppressor genes in cancer [72]. Determination of the methylation patterns of multiple genes to obtain complex ctDNA methylation signatures can contribute importantly to cancer development and/or progression.
In recent years, some techniques (such as methylation-specific PCR) have been successfully applied in the area of evaluating gene hypermethylation in the ctDNA, leading to a highly sensitive and specific method for NSCLC diagnosis. Zhang et al. [73] determined the methylation status of 20 tumor-suppressor genes in plasma of 110 NSCLC patients using methylation-specific PCR. They found that nine genes (APC, CDH13, KLK10, DLEC1, RASSF1A, EFEMP1, SFRP1, RARbeta, and p16 (INK4A)) demonstrated significantly higher frequencies of methylation in NSCLC patients. The methylation frequencies in the plasma were consistent with those in the paired tumor tissues. The results indicated that methylated alteration of multiple genes played important roles in NSCLC pathogenesis and the methylated genes in ctDNA might be potential candidate epigenetic biomarkers for NSCLC detection. Fischer et al. [74] examined hypermethylation status of seven genes (APC1A, DAPK, FHIT, p14 (ARF), p16 (INK4a), RARbeta, and RASSF1A) in serum ctDNA of 92 NSCLC patients by a nested methylation-specific PCR. They found that 87 patients showed at least one epigenetic alteration and the methylation frequencies of individual genes varied between 25.9 and 47.3 %. The hypermethylation of RASSF1A or p14 (ARF) may be useful prognostic markers in NSCLC patients.
The results of studies of methylated gene alterations in ctDNA of NSCLC patients were shown in Table 4. Three studies reported methylation of p16 and RARbata; two studies showed methylation of APC, RASSF1A, DAPK, SHP1P2, DLEC1, KLK10, and SFRP1. The other genes were reported to be methylated only once. The genes found to be hypermethylated in over 30 % of NSCLC (based on at least two independent studies) were APC and RASSF1A. The methylation frequency of DAPK between different studies varied from 26.1 to 68.4 %. Except for DAPK, the methylation frequencies of other genes had little differences across studies (Table 4).
Most of the studies involved controls; therefore, comparison of the data across cases and controls was possible. Methylation-specific PCR techniques have been employed by most of the studies to quantify the methylation statues of genes (Table 4). The genomic DNA was treated with bisulphite (a critical step in methylation analysis) in all studies in order to convert unmethylated cytosines of CpG dinucleotides into uracil or UpG [47, 75, 82]. In the past, researchers had to collect relatively large amounts of clinical samples to avoid DNA degradation during bisulfite treatment, but now, some commercial kits have been developed successfully which enable highly efficient bisulfite conversion, even the amount of starting material is limited.
Summary and perspectives
The finding that tumors are capable of shedding DNA into the blood stream, which can be detected from both serum and plasma and used as surrogate source of tumor DNA, has opened new areas in diagnosis and prognosis. The development of sensitive and accurate diagnostic methods and explore specific biomarker in ctDNA are becoming an area of study with growing interest, mainly because of the simplicity of sampling and the potential value of the methods in clinical use.
Many studies have proven that the levels of ctDNA in plasma or serum increased in NSCLC patients and correlated with tumor stage, survival, and early response to therapy, and the genetic and epigenetic changes in ctDNA might be related to NSCLC carcinogenesis, but some problems still should be settled. As discussed earlier, the levels of ctDNA in plasma or serum were significantly higher in NSCLC patients than in healthy controls or patients with benign diseases. However, the concentrations of ctDNA reported in both NSCLC patients and controls by different studies were highly variable, and the distributions show considerable overlap, making it is difficult to draw firm conclusions based on these studies. The results of genetic and epigenetic changes in ctDNA varied greatly among different published studies. For example, KRAS mutation occurred in NSCLC patients from 4.1 to 23.1 % and EGFR mutation occurred from 16.0 to 61.3 %, leading to difficulties in the interpretation of results. Furthermore, the sensitivity and specificity of assay methods were not mentioned clearly by some studies.
The present analysis methods are not perfect, but the approval of the cobas EGFR mutation test still gives us hope. It is a milestone which highlights the importance of sensitive, accurate tests that can be conducted in time to inform crucial treatment decisions. Another drug in this class of EGFR TKIs, afatinib (Boehringer Ingelheim), has been approved by FDA in July 2013. Afatinib also have its own companion diagnostic test (Therascreen EGFR PCR Kit, from Qiagen). We believe that more and more targeting agents and companion diagnostics that are more tailored to an individual’s genetic profile or a disease’s profile will be developed and approved in the future.
In other to expend and strengthen the utility of ctDNA in the screening and management of NSCLC, standardized methodologies and quality control standard methods should be imported into the research in the future to reduce sources of variation. Moreover, large-scale prospective studies are necessary for population-based studies and molecular epidemiologic studies, in order to implement a clinical application in NSCLC detection, diagnosis, prognosis, and prediction of treatment response.
References
Society AC. Cancer facts and figures. 2012.
Jemal A et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59(4):225–49.
Reade CA, Ganti AK. EGFR targeted therapy in non-small cell lung cancer: potential role of cetuximab. Biogeosciences. 2009;3:215–24.
Agarwal M et al. Age, tumor size, type of surgery, and gender predict survival in early stage (stage I and II) non-small cell lung cancer after surgical resection. Lung Cancer. 2010;68(3):398–402.
Ulivi P et al. Multiple marker detection in peripheral blood for NSCLC diagnosis. PLoS One. 2013;8(2):e57401.
Catarino R et al. Circulating DNA: diagnostic tool and predictive marker for overall survival of NSCLC patients. PLoS One. 2012;7(6):e38559.
Diaz Jr LA et al. The molecular evolution of acquired resistance to targeted EGFR blockade in colorectal cancers. Nature. 2012;486(7404):537–40.
Lee YJ et al. Circulating cell-free DNA in plasma of never smokers with advanced lung adenocarcinoma receiving gefitinib or standard chemotherapy as first-line therapy. Clin Cancer Res. 2011;17(15):5179–87.
Pan S et al. Can plasma DNA monitoring be employed in personalized chemotherapy for patients with advanced lung cancer? Biomed Pharmacother. 2012;66(2):131–7.
Szpechcinski A et al. Quantitative analysis of free-circulating DNA in plasma of patients with resectable NSCLC. Expert Opin Biol Ther. 2012;12 Suppl 1:S3–9.
van der Vaart M, Pretorius PJ. The origin of circulating free DNA. Clin Chem. 2007;53(12):2215.
Schwarzenbach H, Hoon DS, Pantel K. Cell-free nucleic acids as biomarkers in cancer patients. Nat Rev Cancer. 2011;11(6):426–37.
Viorritto IC, Nikolov NP, Siegel RM. Autoimmunity versus tolerance: can dying cells tip the balance? Clin Immunol. 2007;122(2):125–34.
Fleischhacker M, Schmidt B. Cell-free DNA resuscitated for tumor testing. Nat Med. 2008;14(9):914–5.
Bendich A, Wilczok T, Borenfreund E. Circulating DNA as a possible factor in oncogenesis. Science. 1965;148(3668):374–6.
Leon SA et al. Free DNA in the serum of cancer patients and the effect of therapy. Cancer Res. 1977;37(3):646–50.
Kumar S et al. Plasma DNA level in predicting therapeutic efficacy in advanced nonsmall cell lung cancer. Eur Respir J. 2010;36(4):885–92.
Sirera R et al. Can serum be used for analyzing the EGFR mutation status in patients with advanced non-small cell lung cancer. J Thorac Oncol. 2011;6(2):286–90.
Vinayanuwattikun C et al. The impact of non-tumor-derived circulating nucleic acids implicates the prognosis of non-small cell lung cancer. J Cancer Res Clin Oncol. 2013;139(1):67–76.
Ludovini V et al. Plasma DNA, microsatellite alterations, and p53 tumor mutations are associated with disease-free survival in radically resected non-small cell lung cancer patients: a study of the perugia multidisciplinary team for thoracic oncology. J Thorac Oncol. 2008;3(4):365–73.
Yoon KA et al. Comparison of circulating plasma DNA levels between lung cancer patients and healthy controls. J Mol Diagn. 2009;11(3):182–5.
Szpechcinski A et al. Real-time PCR quantification of plasma DNA in non-small cell lung cancer patients and healthy controls. Eur J Med Res. 2009;14 Suppl 4:237–40.
Paci M et al. Circulating plasma DNA as diagnostic biomarker in non-small cell lung cancer. Lung Cancer. 2009;64(1):92–7.
Roth C et al. Screening for circulating nucleic acids and caspase activity in the peripheral blood as potential diagnostic tools in lung cancer. Mol Oncol. 2011;5(3):281–91.
Camps C et al. The identification of KRAS mutations at codon 12 in plasma DNA is not a prognostic factor in advanced non-small cell lung cancer patients. Lung Cancer. 2011;72(3):365–9.
Jian G et al. Prediction of epidermal growth factor receptor mutations in the plasma/pleural effusion to efficacy of gefitinib treatment in advanced non-small cell lung cancer. J Cancer Res Clin Oncol. 2010;136(9):1341–7.
He C et al. Detection of epidermal growth factor receptor mutations in plasma by mutant-enriched PCR assay for prediction of the response to gefitinib in patients with non-small-cell lung cancer. Int J Cancer. 2009;125(10):2393–9.
Zhang L et al. Detection of EGFR somatic mutations in non-small cell lung cancer (NSCLC) using a novel mutant-enriched liquidchip (MEL) technology. Curr Drug Metab. 2012;13(7):1007–11.
Zhao X et al. Comparison of epidermal growth factor receptor mutation statuses in tissue and plasma in stage I–IV non-small cell lung cancer patients. Respiration. 2013;85(2):119–25.
Kimura H et al. EGFR mutation of tumor and serum in gefitinib-treated patients with chemotherapy-naive non-small cell lung cancer. J Thorac Oncol. 2006;1(3):260–7.
Wang S et al. Potential clinical significance of a plasma-based KRAS mutation analysis in patients with advanced non-small cell lung cancer. Clin Cancer Res. 2010;16(4):1324–30.
Nygaard AD et al. The prognostic value of KRAS mutated plasma DNA in advanced non-small cell lung cancer. Lung Cancer. 2013;79(3):312–7.
Kim ST et al. Can serum be used for analyzing the EGFR mutation status in patients with advanced non-small cell lung cancer? Am J Clin Oncol. 2013;36(1):57–63.
Bai H et al. Epidermal growth factor receptor mutations in plasma DNA samples predict tumor response in Chinese patients with stages IIIB to IV non-small-cell lung cancer. J Clin Oncol. 2009;27(16):2653–9.
Yung TK et al. Single-molecule detection of epidermal growth factor receptor mutations in plasma by microfluidics digital PCR in non-small cell lung cancer patients. Clin Cancer Res. 2009;15(6):2076–84.
Narayan A et al. Ultrasensitive measurement of hotspot mutations in tumor DNA in blood using error-suppressed multiplexed deep sequencing. Cancer Res. 2012;72(14):3492–8.
Angulo B et al. A comparison of EGFR mutation testing methods in lung carcinoma: direct sequencing, real-time PCR and immunohistochemistry. PLoS One. 2012;7(8):e43842.
Sheffield VC et al. The sensitivity of single-strand conformation polymorphism analysis for the detection of single base substitutions. Genomics. 1993;16(2):325–32.
Cohen V et al. Evaluation of denaturing high-performance liquid chromatography as a rapid detection method for identification of epidermal growth factor receptor mutations in nonsmall-cell lung cancer. Cancer. 2006;107(12):2858–65.
Li M, Stoneking M. A new approach for detecting low-level mutations in next-generation sequence data. Genome Biol. 2012;13(5):R34.
Lynch TJ et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350(21):2129–39.
Paez JG et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304(5676):1497–500.
http://www.cancer.gov/cancertopics/druginfo/fda-erlotinib-hydrochloride.
Mack PC et al. EGFR mutations detected in plasma are associated with patient outcomes in erlotinib plus docetaxel-treated non-small cell lung cancer. J Thorac Oncol. 2009;4(12):1466–72.
Punnoose EA et al. Evaluation of circulating tumor cells and circulating tumor DNA in non-small cell lung cancer: association with clinical endpoints in a phase II clinical trial of pertuzumab and erlotinib. Clin Cancer Res. 2012;18(8):2391–401.
Tsao DA et al. A fast and convenient new technique to detect the therapeutic target, K-ras mutant, from peripheral blood in non-small cell lung cancer patients. Lung Cancer. 2010;68(1):51–7.
Salazar F et al. First-line therapy and methylation status of CHFR in serum influence outcome to chemotherapy versus EGFR tyrosine kinase inhibitors as second-line therapy in stage IV non-small-cell lung cancer patients. Lung Cancer. 2011;72(1):84–91.
Kuang Y et al. Noninvasive detection of EGFR T790M in gefitinib or erlotinib resistant non-small cell lung cancer. Clin Cancer Res. 2009;15(8):2630–6.
Kimura H et al. Evaluation of epidermal growth factor receptor mutation status in serum DNA as a predictor of response to gefitinib (IRESSA). Br J Cancer. 2007;97(6):778–84.
Kimura H et al. Detection of epidermal growth factor receptor mutations in serum as a predictor of the response to gefitinib in patients with non-small-cell lung cancer. Clin Cancer Res. 2006;12(13):3915–21.
Goto K et al. Epidermal growth factor receptor mutation status in circulating free DNA in serum: from IPASS, a phase III study of gefitinib or carboplatin/paclitaxel in non-small cell lung cancer. J Thorac Oncol. 2012;7(1):115–21.
Isobe K et al. Clinical significance of circulating tumor cells and free DNA in non-small cell lung cancer. Anticancer Res. 2012;32(8):3339–44.
Nakamura T et al. Application of a highly sensitive detection system for epidermal growth factor receptor mutations in plasma DNA. J Thorac Oncol. 2012;7(9):1369–81.
Brevet M et al. Detection of EGFR mutations in plasma DNA from lung cancer patients by mass spectrometry genotyping is predictive of tumor EGFR status and response to EGFR inhibitors. Lung Cancer. 2011;73(1):96–102.
Jiang B et al. Serum detection of epidermal growth factor receptor gene mutations using mutant-enriched sequencing in Chinese patients with advanced non-small cell lung cancer. J Int Med Res. 2011;39(4):1392–401.
Bai H et al. Influence of chemotherapy on EGFR mutation status among patients with non-small-cell lung cancer. J Clin Oncol. 2012;30(25):3077–83.
Janne PA. Challenges of detecting EGFR T790M in gefitinib/erlotinib-resistant tumours. Lung Cancer. 2008;60 Suppl 2:S3–9.
Pao W et al. Acquired resistance of lung adenocarcinomas to gefitinib or erlotinib is associated with a second mutation in the EGFR kinase domain. PLoS Med. 2005;2(3):e73.
Suda K et al. EGFR T790M mutation: a double role in lung cancer cell survival? J Thorac Oncol. 2009;4(1):1–4.
Ma C, Wei S, Song Y. T790M and acquired resistance of EGFR TKI: a literature review of clinical reports. J Thorac Dis. 2011;3(1):10–8.
Inukai M et al. Presence of epidermal growth factor receptor gene T790M mutation as a minor clone in non-small cell lung cancer. Cancer Res. 2006;66(16):7854–8.
Kris MG, Simon GR. Maintenance therapy for non-small cell lung cancer. The NCCN 15th Annual Conference: Clinical Practice Guidelines & Quality Cancer Care. 2010.
FDA approves Xalkori with companion diagnostic for a type of late-stage lung cancer. U.S. Food and Drug Administration.http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm269856.htm.
Califano R, Landi L, Cappuzzo F. Prognostic and predictive value of K-RAS mutations in non-small cell lung cancer. Drugs. 2012;72 Suppl 1:28–36.
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology. Non-Small Cell Lung Cancer V2. 2012.
Keedy VL et al. American Society of Clinical Oncology provisional clinical opinion: epidermal growth factor receptor (EGFR) Mutation testing for patients with advanced non-small-cell lung cancer considering first-line EGFR tyrosine kinase inhibitor therapy. J Clin Oncol. 2011;29(15):2121–7.
Carpagnano GE et al. 3p microsatellite signature in exhaled breath condensate and tumor tissue of patients with lung cancer. Am J Respir Crit Care Med. 2008;177(3):337–41.
Sirera R et al. Retrospective analysis of the prognostic role of p16 protein inactivation in plasma in patients with locally advanced non-small cell lung cancer. Lung Cancer. 2008;61(1):104–8.
Toth G, Gaspari Z, Jurka J. Microsatellites in different eukaryotic genomes: survey and analysis. Genome Res. 2000;10(7):967–81.
Speicher MR. Microsatellite instability in human cancer. Oncol Res. 1995;7(6):267–75.
Silva JM, Bonilla F, Correspondence re: Coulet F et al. Detection of plasma tumor DNA in head and neck squamous cell carcinoma by microsatellite typing and p53 mutation analysis. Cancer Res. 2000;60:707–9. Cancer Res. 2001;61(23):8595–6.
Esteller M. CpG island hypermethylation and tumor suppressor genes: a booming present, a brighter future. Oncogene. 2002;21(35):5427–40.
Zhang Y et al. Methylation of multiple genes as a candidate biomarker in non-small cell lung cancer. Cancer Lett. 2011;303(1):21–8.
Fischer JR et al. Prognostic significance of RASSF1A promoter methylation on survival of non-small cell lung cancer patients treated with gemcitabine. Lung Cancer. 2007;56(1):115–23.
Lee SM, Park JY, Kim DS. Methylation of TMEFF2 gene in tissue and serum DNA from patients with non-small cell lung cancer. Mol Cells. 2012;34(2):171–6.
Ponomaryova AA et al. RARbeta2 gene methylation level in the circulating DNA from blood of patients with lung cancer. Eur J Cancer Prev. 2011;20(6):453–5.
Vinayanuwattikun C et al. Epithelial-specific methylation marker: a potential plasma biomarker in advanced non-small cell lung cancer. J Thorac Oncol. 2011;6(11):1818–25.
Zhang Y et al. Frequent epigenetic inactivation of deleted in lung and esophageal cancer 1 gene by promoter methylation in non-small-cell lung cancer. Clin Lung Cancer. 2010;11(4):264–70.
Zhang YW et al. Transcriptional inactivation of secreted frizzled-related protein 1 by promoter hypermethylation as a potential biomarker for non-small cell lung cancer. Neoplasma. 2010;57(3):228–33.
Hoffmann AC et al. Lack of prognostic significance of serum DNA methylation of DAPK, MGMT, and GSTPI in patients with non-small cell lung cancer. J Surg Oncol. 2009;100(5):414–7.
Zhang Y et al. Frequent transcriptional inactivation of Kallikrein 10 gene by CpG island hypermethylation in non-small cell lung cancer. Cancer Sci. 2010;101(4):934–40.
Hoffmann AC et al. Methylated DAPK and APC promoter DNA detection in peripheral blood is significantly associated with apparent residual tumor and outcome. J Cancer Res Clin Oncol. 2009;135(9):1231–7.
Acknowledgment
This work was supported by the National Natural Science Foundation of China (no. 81202739).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nie, K., Jia, Y. & Zhang, X. Cell-free circulating tumor DNA in plasma/serum of non-small cell lung cancer. Tumor Biol. 36, 7–19 (2015). https://doi.org/10.1007/s13277-014-2758-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13277-014-2758-3