
Abstract
Previous studies describe the use of a large area parallel-plate chamber, the PTW Bragg Peak chamber, for measuring dose-area product (DAP) and output factors in small megavoltage photon fields. However, in radiotherapy departments without protons, this detector would have to be purchased separately for this purpose. This work investigated the feasibility of alternatively using a large transmission ionisation chamber, the IBA round Stealth chamber (SC), for output factor measurements of stereotactic fields. This type of detector is more commonly found in radiotherapy departments as a reference chamber for water tank scanning of small fields, and hence DAP could be performed without an additional purchase. The SC’s large sensitive area (diameter of 94 mm) measures the integral dose, also known as DAP, over the whole two-dimensional (2D) dose distribution of the small field. The measurements were performed using a 6 MV beam from an Elekta Infinity linear accelerator. Conversion of DAP to central axis point dose was performed using 2D dose maps from Gafchromic EBT3 films. The field sizes measured ranged from side length of 5 mm to 50 mm (all square). The resultant output factors were compared against measurements with a stereotactic diode. The small field output factors measured using SC + film were in good agreement with the stereotactic diode (within 2% for field sizes as small as 6 mm; 3% difference at 5 mm). The new proposed method showed that a transmission chamber like SC is a good alternative large-area parallel plate chamber to measure DAP and derive small field OFs. Furthermore, the feasibility of using 2D reconstructed dose maps from water tank profiles and hence filmless approach was investigated. Results showed that filmless conversion of DAP to central axis point dose is feasible using profiles. However, a large number of profiles are required (i.e. 15° increments (star pattern) are required for accurate 2D dose reconstruction), and hence the water tank scanning for this approach may be prohibitively time-consuming.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Special procedures such as stereotactic radiotherapy (SRT), stereotactic radiosurgery (SRS), intensity modulated radiotherapy (IMRT), and volumetric modulated arc radiotherapy (VMAT), differ from conventional conformal radiotherapy such that small radiation fields (narrow or sub-centimeter) are used for treatment delivery. Hence, accuracy in small field dosimetry is important in order to achieve the clinical goal of radiotherapy, i.e. to deliver precise dose to the target volume and better sparing of normal tissue. This increases the demand for more precise and accurate small field measurements [1, 2].
A small photon field is generally defined as the one having dimensions smaller than the lateral range of the charged particles that contribute to the dose deposited at a point along the central axis of the beam [2, 3]. According to these criteria, field sizes of less than approximately 30 × 30 mm2 are considered to be small for 6 MV photon beam [4]. The IPEM Report 103 classified field sizes less than 40 mm under the category of small photon fields [3]. Charles et al. proposed using the practical definition of very small field sizes to distinguish them from conventional small photon field to further improve the accuracy in measurements of dosimetric parameters (e.g. output factors). This study defined very small field to be ≤ 15 mm (for 6 MV photon beams) based on the impact of a 1 mm error in field size or detector position on OFs at a 1% output factor uncertainty level [4].
Small field dosimetric measurement is challenging to characterise experimentally using commercial detectors due to lack of electronic equilibrium, volume averaging effects, and source occlusion. These difficulties associated with the use of small fields has been recognised and discussed in several publications (see for example references 1, 2, 5 and 6 for a general overview). An output factor (OF) is a key parameter that can characterise small fields. An OF accounts for the dose difference between the conventional reference field (typically 10 × 10 cm2) and the field of interest. OFs are traditionally taken as the ratio of the point dose at the centre of a given field to that measured at the centre of a reference field. However, for small photon fields, the traditional output factor measurement has some issues due to detector resolution, volume effects, non-water equivalence of the detector, and the positioning accuracy on the narrow-beam axis [1, 2, 5,6,7]. Often, the sensitivity of the detector is different in a small field than it is in the reference field and therefore a field size specific correction factor is required (see TRS 483 for extensive details [6]). The detector selection is an important consideration and accurate detector positioning is significant. However, accurate measurements can be performed with appropriate methodology [5]. Oliver et al. have recently published an interesting comparison of small field output factors performed by clinical departments using uninhibited methodology [8]. These results showed that close agreement between centres could be found if they followed a similar, reproducible methodology. Many of the centres used diodes. Due to the high spatial resolution and high sensitivity of diodes, these detectors are widely used for small field output factor measurements [5, 7]. However, due to the diode’s overresponse at small field sizes, a field size specific correction factor needs to be applied which can be based on accurate Monte Carlo models [6, 9, 10].
Accurate detector positioning can be achieved by measuring cross-axis (perpendicular to beam direction) radiation profiles at the same time as output factors for each field size setting [4, 11], but this can be time consuming. The very small field classification (field size ≤ 15 mm for 6 MV photon beam) can be set as a threshold at which this careful experimental methodology should be required to achieve better dosimetric accuracy [4]. Nonetheless, even with careful detector set-up, a 1 mm error in detector position was still found to lead to > 1% error in measured OF for field sizes < 10 mm while a 1 mm error in field size can lead to > 1% error in measured OF for field sizes < 15 mm [4].
To address the difficulty of choosing the suitable detector for small field dosimetry, an alternative to central axis point dose is to measure integral dose or Dose-Area Product (DAP) using an ionisation chamber with area larger than the field under consideration. It has been suggested in previous works that DAP, which is the integral dose in a plane perpendicular to the beam direction, can be a useful dose metric for small fields [12, 13]. Using a detector with large sensitive volume compared to the field size has the advantage of being insensitive to its lateral alignment in the beam central axis.
Several publications describe the use of a large area parallel-plate chamber (LAC), the PTW Bragg Peak chamber type 34070-2.5 (PTW Freiburg, Germany), for measuring DAP in small megavoltage photon fields [12,13,14]. Djouguela et al. first proposed using LAC and showed that the central axis point dose can be replaced by “dose-area product” or DAP [12]. They also replaced the usual “output factor” (for point doses) by the “modified output factor” MOF (for DAP). A similar study was performed by Sanchez-Doblado et al. where they used the combination of large area ionisation chamber (LAC) and relative film dosimetry for measurement of output factors [13]. Due to the large sensitive area of the LAC, it integrates the dose over the whole 2D dose distribution of the small field, including scatter and transmission dose. Using film dosimetry, the integrated dose measured by LAC per unit area was converted to its corresponding absolute dose value delivered to a very small region. The results were compared to output factors measured using other detectors and Monte Carlo simulation. An excellent agreement was found between LAC + 3 films, diamond detector, diode and Monte Carlo. Dufreneix et al. have extended the concept further, showing that it is possible to use DAP for absolute dosimetry [15]. The same authors also expand on this work, investigating the possibility of using profiles scanned with a 1D detector to convert DAP to point dose [16]. However, a single profile can only be used in a circular field, with assumed radial symmetry.
Whilst the above studies have shown it is feasible measuring small field output factors with a Bragg Peak chamber, its use may be limited. This is because the Bragg Peak chamber, designed for proton dosimetry, is not widely used and not readily available in all radiotherapy departments (as most do not have proton therapy). Purchasing a Bragg peak chamber for the sole purpose of small field dosimetry also may not be an attractive option from a financial point of view. An alternative LAC that may be more prevalent in standard radiotherapy departments is a large transmission reference chamber. The IBA Round Stealth chamber (IBA Dosimetry GmbH, Schwarzenbruck, Germany) is an example of a large transmission ionisation chamber, designed as a reference chamber with minimal beam perturbation. Similar to the Bragg Peak chamber, the round Stealth chamber (SC) measures integral dose or DAP over its large active area (diameter of 94 mm as shown in Fig. 1). This study will explore the idea that an existing transmission chamber (that may have already been purchased as a reference chamber) can be used as an integral dosimeter, negating the need to purchase a specific, separate chamber for this purpose. The SC measurement of output factors should be insensitive to positioning errors. It also does not require perturbation correction factors as it is assumed that the beam perturbation is field size independent due to each field being smaller than the detector.

The Dimensions of the round Stealth chamber (Reproduced from [20] with permission)
Diode orthogonal profiles, which are normally measured to verify accurate detector positioning relative to radiation isocenter and report dosimetric field size, can be potentially used for the reconstruction of the 2D dose distribution. The accuracy of 2D-dose plane reconstruction (and therefore the “DAP to CAX dose” curve determined) from profiles was investigated using film, to possibly eliminate the need for the additional film measurement in the future. This can avoid some disadvantages associated with using film such as cost, need for dosimetry system for calibration, lateral artefact for scanning films, and other handling issues.
The primary aim of this work was to investigate the feasibility of using a transmission chamber for a second purpose: measuring DAP and deriving small field OFs. The second aim of this work was to test the feasibility of film-less DAP to point dose conversion. Both these aims combine to test the general idea that this work can be performed using existing equipment within a department without the additional costs of a Bragg-Peak chamber or film.
Materials and methods
Stealth chamber
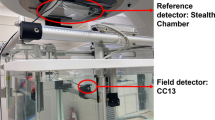
The IBA Round Stealth chamber (IBA Dosimetry GmbH, Schwarzenbruck, Germany) is a large transmission ionisation chamber used as a reference chamber for water phantom scanning systems, for energy the range of Co-60 to 21 MV/MeV [17,18,19,20]. The Stealth chamber (SC) was designed with small fields in mind, since the presence of the chamber provides minimal beam perturbation [17, 18], and can be mounted directly to the linac head so that it can be used as a reference detector for water tank scans (see Fig. 2). Other important design advantages of the SC include its transparent nature (so the one can view the light field) and its robust construction. The round SC has a circular active area with a diameter of 94 mm as shown in Fig. 1. It has a total attenuation equivalent of less than 0.5 mm Aluminium [20].

The round Stealth chamber mounted on Elekta treatment head as a reference chamber
Since the SC was intended to be used as a reference chamber for water tank scanning and as a field chamber for measuring small field output factor, the chamber was commissioned based on the recommended commissioning tests from AAPM TG142 [21], ACPSEM Position Paper [22], and IPEM 81 [23]. The commissioning tests included pre- and post-irradiation leakage, short-term reproducibility, dose linearity, dose rate linearity, and transmission measurements. Note that the polarity effect was not considered as this detector is only used for relative measurements both in its standard use as a reference chamber and in its novel use in this study.
Small field measurements using DAP with the stealth chamber
The chamber was irradiated with a 6 MV photon beam (TPR20,10 = 0.678) using an Elekta Infinity linear accelerator (Elekta, Stockholm, Sweden). This linear accelerator uses an Agility beam collimation system consisting of 160 MLC leaves, each with a width of 5 mm (at the isocentre) as the upper collimator. The lower collimator, in the direction perpendicular to the MLC, is a traditional large jaw pair. This enabled square fields of any size to be created. The field sizes used were all square with side lengths of 5, 6, 8, 10, 20 and 50 mm. The PTW Unidos Webline electrometer (PTW, Freiburg, Germany) was used to provide the polarizing voltage and collect the charge produced in the SC. An operating voltage of + 300 V was applied, which is within the recommended voltage by the manufacturer. The SC was positioned at a depth of 5 cm of Plastic Water (CIRS, Norfolk, USA) with a SSD of 95 cm as shown in Fig. 4 (Set-up 1). A custom jelly bolus (Jel Products Australia, NSW, Australia) was used around the SC so that it could be placed in the stack of Plastic Water, and 10 cm of Plastic Water was used as backscatter.
The Stealth DAP ratio (DAP OFSC (fs)), i.e. the integral dose values for the field size of interest normalised to the field size of 50 × 50 mm2, was calculated using Eq. (1). 50 mm was chosen as it is often used as an intermediate field size when ‘daisy-chaining’ small field output factors with normal size field output factors.
where DAP OFSC (fs) = Dose area product measured by Stealth chamber for the field size of interest (DAPfs) normalised to the field size of 50 × 50 mm2, (DAP50 mm fs).
Conversion of dose-area-product to point dose
A similar approach to Sanchez-Doblado et al. [13] was adopted to obtain the “DAP to central axis point dose (CAX)” conversion from the combination of a large area ionisation chamber (SC) and relative film dosimetry. This method required obtaining both the central axis dose (dose to a very small region of interest (ROI)) and the integral dose (over the SC area) from a known 2D distribution (e.g. film) to get the “DAP to CAX” conversion.
A calibrated batch of Gafchromic EBT3 film (EBT3, Ashland Inc., Covington, Kentucky, USA) was used with the measurement set-up shown in Fig. 4. Two (5 and 50 mm) to three (6, 8, 10, and 20 mm) large films with the size of the film equivalent to the SC diameter were stacked and irradiated for each field size. The three different films were required in order to minimise film noise by delivering a large dose to each region of the dose profile (inside the field, in the penumbra, and outside the field). Firstly, the stack of three films was irradiated with the number of monitor units (MUs) required to deliver approximately 3 Gy to the centre of the field. The top piece of film was removed, and approximately four times as many additional MUs were delivered again so that the 20% of penumbra received approximately 3 Gy in total. The second film was then removed and an additional 10,000 MU was delivered to the remaining piece of film, in order to get a large dose to region of the profile that is outside the main field, but inside the region equivalent to the size of the SC. This method was required, because it was not possible to measure the centre of the field after 10,000 MU of irradiation due to film saturation. After irradiation, the films were processed using EPSON Expression 10000 XL flatbed scanner with 148 dpi resolution. Optical density of the red channel was calibrated to the dose, using the known dose delivered (0–3.5 Gy) to 16 small squares of film. Note that an unirradiated film was scanned to represent 0 Gy. The processing of the digitized film to dosemaps was performed using an in-house Matlab software.
The resulting EBT3 measured dosemaps were used to measure both central axis dose and dose area product, to obtain a “DAP to CAX” output factor conversion curve. Central axis output factors were extracted from the film dose maps using a 2D linear interpolation, where the field centre was determined as the average centre of isodose contours. This was performed by extracting isodose contours at 1 cGy increments, calculating the centre of each contour, and averaging these centres (See Fig. 3). The central axis dose was measured as the mean dose to the central 1 mm square (\({D}_{point,fs}).\) The dose area product was the mean of the central 94 mm diameter circle, which corresponds to the Stealth chamber area \({(D}_{SC\,area,fs}).\)

Field centre estimation using isodose contours for 5 × 5 mm2
The output factor from the SC measurements (DAP OFSC (fs)) was obtained normalising the SC result from the field size in question, to the SC result from the 50 mm field size. The DAP OFSC (fs) was then converted to its corresponding central axis OF (OFSC (fs)) using “DAP to CAX” correction factor, F, as shown in Eq. (2).
The “DAP to CAX” correction factor, F, for each field size was taken as the ratio of output factors obtained for a very small region of interest (\({OF}_{point}\)) to that corresponding to the Stealth sensitive area \({(OF}_{SC\,area})\) (see Eq. 3). The radius of integration was kept constant.
where
Dpoint, fs = Central axis dose for the field size of interest measured as the mean dose to the central 1 mm square. Dpoint, 50mm fs = Central axis dose for the reference field size (50 × 50 mm2 fs) measured as the mean dose to the central 1 mm square. DSC area, fs = Dose area product for the field size of interest measured as the mean of the central 94 mm diameter circle, corresponding to the Stealth chamber area. DSC area, 50mm fs = Dose area product for the reference field size (50 × 50 mm2 fs) measured as the mean of the central 94 mm diameter circle, corresponding to the Stealth chamber area.
Verification of point dose measurements with diode detector
The PTW 60018 SRS diode (PTW, Freiburg, Germany) was set-up in a water tank at a depth of 5 cm and SSD of 95 cm, with the long axis of the detector parallel to the beam axis (Fig. 4 Set-up 3). The SRS diode is an unshielded diode with an active volume of 0.3 mm3. Orthogonal profiles were collected to check the diode central axis (CAX) centering and radiation field size for each field size setting, and the measured radiation field size was also recorded [4, 11]. Two profile scans along each axis were collected to make sure that the detector positional uncertainty was only due to the water tank system accuracy (± 0.1 mm) [11]. For each field size, the average field width was obtained and the effective field size (FSeff) was calculated using Eq. (6) as recommended by Cranmer-Sarsigon et al. [11]. Once the set-up was confirmed, OFs were acquired for 5, 6, 8, 10, 20 and 50 mm nominal field sizes. Field size specific correction factors were applied to the diode OFs to correct for diode over-response [24]. The corrected diode OFs were compared with the SC OF.

Measurement set-up used for output factor determination
where A and B correspond to the inline and crossline measured full-width-half-maximum.
Filmless conversion of DAP to point dose
DAP to CAX conversion using multiple 1D profiles
The proposed method for filmless conversion of “DAP to CAX” includes measuring multiple 1D profiles and reconstructing 2D dose maps from the 1D profiles. The CAX dose and DAP are calculated from these generated 2D dose maps, generating the “DAP to CAX” conversion curve. The validity of this “DAP to CAX” conversion curve could be quantified by comparing with the output factor ratios measured using the two detectors (i.e. SC and diode). To test the feasibility of computing integral dose from multiple 1D profiles, the 2D dosemaps acquired previously with film were used as a gold standard. In order to isolate this theoretical concept from measurement uncertainty, 1D profiles were extracted from the same 2D film dose map. 1D profiles were extracted at 90°, 45°, 15°, 5°, and 1° increments (using Matlab) (See Fig. 5). A 2D dose map was then reconstructed 5 times using the following number of profiles: 2 (90° apart), 4 (45° apart), 12 (15° apart), 36 (5° apart) and 180 (1° apart). The resulting DAP corresponding to the Stealth sensitive area measured from the reconstructed 2D dosemaps was then compared to the raw 2D film dose map. The mean DAP error was calculated as the average DAP difference of the reconstructed and the original 2D dosemaps for all field sizes.

Extracting profiles from the film 2D dosemaps using in-house Matlab program. This example shows 45° increments
Estimation of scanning time required for water tank profiles
The time required to acquire water tank profiles at 45°, 15°, 5°, and 1° increments was estimated from the actual scanning time of 15° and 45° “star” patterns in the water phantom. This was the basis in evaluating the efficiency of using water tank profiles to derive the “DAP to CAX” conversion curve as a filmless approach.
Comparison of “DAP to CAX” conversion curve obtained from film and detectors
To check the validity of the “DAP to CAX” conversion curve, the film output factor ratios obtained from film raw 2D dose maps were compared to the device measured output factor ratios. The device measured output factor ratio was taken simply as the ratio of output factors of SRS diode and Stealth chamber.
Results
Field size evaluation using diode profiles
The field widths measured using the SRS diode profiles are summarised in Table 2. From these average values, the maximum difference from the nominal values is 1.85 mm in the crossline direction for 5 × 5 mm2 field size. Table 1 shows that the measured values of effective field size (FSeff) are noticeably different from their nominal values with a maximum difference of 0.94 mm for 5 × 5 mm2 field size. Note that asymmetric nature of the effective field size is due to source occlusion and the asymmetric Elekta focal spot [24].
Stealth chamber output factor
The commissioning tests confirmed the suitability of SC for clinical use. The DAP measured by SC was converted to its corresponding absolute dose value at the CAX using the “DAP to CAX” conversion curve derived from film as shown in Fig. 8. The plot of output factors for SC + film is shown in Fig. 7 in comparison with OF measured using SRS diode.
There was a good agreement between central axis output factors measured using the diode and SC + film as shown in Fig. 6 and Table 2. The largest discrepancy between SRS diode and SC + film was 3% for 5 × 5mm2 field size.

Comparison of output factor measured using SRS diode (red squares) and Stealth chamber + film (blue circles)
Uncertainty estimation
Table 3 summarises the sources of uncertainty associated with diode OF measurement and SC + film procedure. The diode positioning error was found to be within 0.1 mm between repeated scans of each field. The estimated uncertainty was 0.7% based on 0.1 mm centering error in a 5 × 5 mm2 field size [4]. The diode readout reproducibility, which was 0.3%, was based on the calculated standard deviation of the diode measurements for each field size and taken as the maximum value. The uncertainty in diode over-response correction factor was estimated as 0.5%, which is the statistical uncertainty in the Monte Carlo calculated factor from Charles et al. [24].
The SC readout reproducibility was based on the maximum standard deviation of the SC DAP measurements. The total uncertainty for the film “DAP to CAX” conversion was calculated using a similar method to Sanchez-Doblado et al. [13]. Briefly, the reproducibility of the film results (point dose and integral dose), as well as uncertainty in the film calibration curve are calculated for each field size, and then averaged across all field sizes. This uncertainty is dominated by statistical noise in the outside of field region in the integral dose calculations. Note that a uniformity correction factor was not considered for either measurement as the fields are uniform across the central 1 mm.
Filmless conversion of DAP to point dose
“DAP to CAX” conversion using multiple 1D profiles
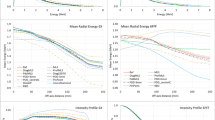
It was found that the “DAP to CAX” calibration curve estimation was poor for the 2D dose reconstruction from the inline and crossline profiles alone. The errors were up to 15% for the 5 × 5 mm2 field size. The reconstructed 2D maps from film profiles at 45°, 15°, 5°, and 1° increments confirmed that the 2D dose reconstruction was more effective with increasing number of profiles (see Table 4). The reconstruction errors for the 15° and 45° star patterns were within 1% and 2%, respectively which would take 12.5 and 4 min to acquire in a water phantom for each field size setting (See Table 4; Fig. 7).

DAP error results of the 2D dose map reconstruction from profiles. Shown are profile increments of 1° (blue circles), 5° (red squares), 15° (green triangles) and 45° (crosses)
Comparison of “DAP to CAX” conversion curve obtained from film and detectors
The comparison of the output factor ratio (“DAP to CAX OF” conversion curve) obtained from film (raw 2D dosemaps) vs. detectors (i.e. SC and diode) is shown in Fig. 8 and Table 5. The “DAP to CAX OF” conversion calibration can be obtained from film with an accuracy of 2%.

Comparison of DAP-to-CAX OF Conversion Curve derived from film (raw 2D dosemaps) (blue circles) and detectors (SRS diode and SC) (red squares)
Discussion
The results showed that a transmission chamber like SC is a good alternative to large-area parallel plate chamber (e.g the Bragg Peak chamber) to measure DAP and derive small field OFs. By comparison to Monte Carlo simulations, Sanchez-Doblado et al. have shown that the PTW T34070 Bragg-Peak chamber can be used (with film) to accurately calculate small field output factors [13]. In this study we have shown (comparing to diode measured output factors) that the Stealth Chamber is similarly effective at calculating small field output factors. However, the disadvantage of this SC + film method is that it requires Gafchromic EBT3 films and very high linac workload. Furthermore, the data also revealed that filmless conversion of DAP to CAX dose is feasible using profiles, but reconstruction will be more effective the larger the number of profiles that are acquired (e.g. 15° increments (star pattern) are required for 2D dose reconstruction with an error of < 1%). Table 4 shows that the reconstruction error is almost zero when many profiles are extracted and reconstructed. However, this may be a disadvantage when it comes to acquiring the water phantom profiles, as the data acquisition may be excessively long. The validity of the “DAP to CAX” OF conversion calibration derived from film was confirmed to be within an accuracy of 2%. The “DAP to CAX” OF conversion curve can then be derived from merely the ratio of diode OF and Stealth DAP ratio supporting the potential of filmless conversion of DAP to CAX dose. The acceptability of this uncertainty will depend on the intended use.
The diode is widely used for small field OF because of its high resolution and high sensitivity, and its high availability in clinical departments. However, a correction factor has to be applied to account for perturbation effects, non-water equivalence of detector, and diode’s overresponse at small field sizes [5,6,7]. Moreover, the impact of diode positioning accuracy is more significant than the Stealth chamber, especially for very small field sizes. Charles et al. [4] reported that a 1 mm error in detector position can lead to a 6.8% error in the measured field output factor, in a field 5 mm across. The diode centering was verified prior to OF measurement to be within 0.1 mm which is equivalent to a 0.7% error. This could explain some of the discrepancy found between diode and the SC especially for very small field sizes. Use of radiochromic film is attractive due to its high spatial resolution, water-equivalence, and insensitivity to positioning uncertainties [25]. Furthermore, 2D dose distributions can be easily obtained from film. On the other hand, there are some issues associated with using film such as cost, need for dosimetry system for calibration, lateral artefact for scanning films, and other handling issues [26]. Due to the complexity and the higher probability of introducing error in the whole calibration, measurement and analysis process can make film an unattractive option. Using a large-area chamber, like Stealth chamber, to measure DAP and derive small field OF is a promising approach as long as “DAP to CAX” conversion factor has been obtained from known 2D dose distribution. The Stealth chamber is easy to set-up since it is insensitive to positioning uncertainties and provides minimal beam perturbation. Lastly, the “DAP to CAX” conversion factor can be derived from diode star scans instead of using film. However, the user should also consider the additional scanning time required to collect these profiles. Further work can investigate reducing the time required for the diode scans, for example by using the concept of radially symmetric scans if appropriate.
Conclusion
The proposed new technique of measuring small field output factor based on the concept of “dose-area product” (DAP) aims to eliminate positioning uncertainties and issues on selecting an appropriate small field detector. It has been shown that the Stealth chamber is a good alternative for measuring DAP to LAC, like Bragg Peak chamber, which is not widely used in all radiotherapy departments. Moreover, the SC is suitable for measuring small field output factors for field sizes < 50 × 50 mm2 as long as “DAP to CAX” conversion factor is available from known 2D dose distribution (i.e. from film or diode profiles).
The feasibility of using 2D reconstructed dose maps from profiles and hence filmless conversion of “DAP to CAX dose” was investigated. The optimal number of profiles needed to achieve a better 2D reconstruction was found to be 15° increments (star pattern) but the water tank scanning might be time-consuming. It then depends on the user preference with some cost and efficiency considerations whether it is better to set-up the water tank to collect star pattern profiles or use film to get the “DAP to CAX” conversion factors. It was also found that the “DAP to CAX OF” conversion curve can be potentially derived from the ratio of diode OF and Stealth DAP ratio as a filmless approach.
The central axis output factors measured using SRS diode and SC + film were found to have an excellent agreement with the maximum discrepancy for the 5 × 5 mm2 field size.
References
Taylor ML, Kron T, Franich RD (2011) A contemporary review of stereotactic radiotherapy: inherent dosimetric complexities and the potential for detriment. Acta Oncol (Madr) 50:483–508
Das IJ, Ding GX, Ahnesjo A (2008) Small fields: nonequilibrium radiation dosimetry. Med Phys 35:206–215
Aspradakis M, Byrne J, Palmans H, Conway J, Rosser K, Warrington J et al (2010) Small field MV photon dosimetry. IPEM Report No. 103. Institute of Physics and Engineering in Medicine, York
Charles PH, Cranmer-Sargison G, Thwaites DI, Crowe SB, Kairn T, Knight RT, Kenny J, Langton CM, Trapp JV (2014) A practical definition of very small field size for radiotherapy output factor measurements. Med Phys https://doi.org/10.1118/1.4868461
Kairn T, Charles PH, Cranmer-Sargison G, Crowe SB, Langton CM, Thwaites DI, Trapp JV (2015) Clinical use of diodes and micro-chambers to obtain accurate small field output factor measurements. Australas Phys Eng Sci Med 8:357–367
Palmans H, Andreo P, Huq MS, Seuntjens J, Christaki K (2017) Dosimetry of small static fields used in external beam radiotherapy: an IAEA-AAPM international code of practice for reference and relative dose determination. Technical Report Series No. 483. International Atomic Energy Agency, Vienna
Cranmer-Sargison G, Weston S, Sidhu NP, Thwaites DI (2011) Experimental small field 6MV output ratio analysis for various diode detector and accelerator combinations. Radiother Oncol 100(3):429–435
Oliver CP, Butler DJ, Takau V, Williams I (2018) Survey of 5 mm small-field output factor measurements in Australia. J Appl Clin Med Phys 2018 19(2):329–337
Cranmer-Sargison G, Weston S, Evans JA, Sidhu NP, Thwaites DI (2011) Implementing a newly proposed Monte Carlo based small field dosimetry formalism for a comprehensive set of diode detectors. Med Phys 38(12):6592–6602
Liu PZ, Suchowerska N, McKenzie DR (2014) Can small field diode correction factors be applied universally? Radiother Oncol 112(3):442–446
Cranmer-Sargison G, Charles PH, Trapp JV, Thwaites DI (2013) A methodological approach to reporting corrected small field relative outputs. Radiother Oncol 109:350–355
Djouguela A, Harder D, Kollhoff R, Rühmann A, Willborn KC, Poppe B (2006) The dose-area product, a new parameter for the dosimetry of narrow photon beams. Med Phys 16:217–227
Sanchez-Doblado F, Hartmann GH, Pena J, Rosello JV, Russiello G, Gonzalez-Castaño DM (2017) A new method for output factor determination in MLC shaped narrow beams. Phys Med 23:58–66
Kupfer T, Lehmann J, Butler DJ, Ganesan R, Bailey TE, Franich RD (2017) Commissioning of a PTW 34070 large-area plane-parallel ionization chamber for small field megavoltage photon dosimetry. J Appl Clin Med Phys 18:206–217
Dufreneix S, Ostrowsky A, Le Roy M, Sommier L, Gouriou J, Delaunay F, Rapp B, Daures J, Bordy JM (2016) Using a dose-area product for absolute measurements in small fields: a feasibility study. Phys Med Biol 61:650–662
Dufreneix S, Ostrowsky A, Rapp B, Daures J, Bordy JM (2016) Accuracy of a dose-area product compared to an absorbed dose to water at a point in a 2 cm dimater field. Med Phys 43:4085–4092
Vasquez Quino LA, Huerta Hernandez CI, Calvo O, Rangaraj D (2016) Clinical experience with a novel reference chamber “stealth chamber” by IBA. American Institute of Physics, AIP Conference Proccedings 1747, 040006
Gersh JA (2014) Stereotactic beam characterisation using the IBA stealth reference detector, IBA Dosimetry Whitepaper
Diego Azcona J, Barbes B (2016) Small field dosimetry in radiosurgery collimators with a Stealth chamber. American Association of Physicists in Medicine, Virginia
P-Stealth Chamber-510-001 01 User’s Guide (2014) IBA Stealth chamber user guide, IBA Dosimetry GmbH, Schwarzenbruck
AAPM Task Group 142 (2009) Comprehensive QA for radiation oncology
ACPSEM Position Paper (1996) Recommendations for the safe use of external beams and sealed brachytherapy sources in radiation oncology
IPEM 81 (1999) Physics Aspects of Quality Control in Radiotherapy
Charles PH, Ibrahim S, Paynter D, Thwaites DI, Monte Carlo simulation of \(K_{{Qclin,Qmsr}}^{{fclin,fmsr}}\) for small field detectors and the Elekta Agility collimation system
Massillon -JLG, Cueva-Procel D, Diaz-Aguirre P, Rodrıguez-Ponce M, Herrera-Martinez F (2013) Dosimetry for small fields in stereotactic radiosurgery using Gafchromic MD-V2-55 Film, TLD-100 and alanine dosimeters, PLOS ONE 8(5):e63418
Lewis D, Micke A, Yu X, Chan MF (2012) An efficient protocol for radiochromic film dosimetry combining calibration and measurement in a single scan. Med Phys 39(10):6339–6350
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
de Chavez, R., Jones, C.E. & Charles, P.H. Integral small field output factor measurements using a transmission ionisation chamber. Australas Phys Eng Sci Med 42, 235–244 (2019). https://doi.org/10.1007/s13246-018-0716-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13246-018-0716-x