
Abstract
Background
The aim of this study is to examine rates of magnesium sulfate utilization by emergency obstetric care trainees to treat preeclampsia–eclampsia in India. Secondarily, structural barriers are identified which limit the use of magnesium sulfate, highlighting limitations of emergency obstetric care training, which is a commonly implemented intervention in resource-poor settings.
Methods
Trainees’ curriculum specified magnesium sulfate treatment for eclampsia and severe preeclampsia. Case records were analyzed for preeclampsia–eclampsia diagnosis, magnesium sulfate utilization, delivery route, and maternal and neonatal outcomes from 13,238 reported deliveries between 2006 and 2012 across 75 district hospitals in 12 Indian states.
Results
Of 1320 cases of preeclampsia–eclampsia, 322 (24.4%) had eclampsia. Magnesium sulfate was given to 12.9% of preeclamptic and 54.3% of eclamptic women, with lower usage rates in rural communities. Among the 1308 women with preeclampsia–eclampsia, only 24 deaths occurred (1.8%). In contrast, among the 17,179 women without preeclampsia–eclampsia, there were 95 reported deaths (0.6%). Both maternal mortality ratios were found to be much higher than the Millennium Development Goal target of 0.15%. Magnesium sulfate administration was associated with a higher death rate in preeclamptic but not eclamptic women, representing possible confounding by severity.
Conclusion
To optimize resources spent on emergency obstetric care training, the consistent availability of magnesium sulfate should be improved in India. Increasing drug availability, implementing clinical guidelines around its administration, and training health-care providers on the identification and treatment of preeclampsia–eclampsia could lead to notable improvements in maternal and infant mortality.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
India is home to almost one-fifth of the world’s population [1], but suffers from a health-care provider shortage which directly affects health-care access and utilization, impacting the well-being of vulnerable populations such as pregnant women and those residing in rural communities [2, 3]. Specifically, 69% of Indians live in rural areas, and 49% of community health centers (CHCs) which are located in rural areas did not have an obstetrician/gynecologist on staff [4]. These shortages have a direct effect on maternal health-care utilization and subsequently maternal mortality in India. The current Indian maternal mortality ratio (MMR) is about 167 per 100,000 live births, which is higher than the United Nations Millennium Development Goal 5, which aimed to reduce MMR to 150 by 2015 [5, 6]. Hypertensive disorders complicate 5% of Indian pregnancies [7] and are responsible for 5% of their maternal mortality [7, 8]. Thus, treating preeclampsia and eclampsia PE–E (hypertensive disorders) with magnesium sulfate (magnesium) could positively impact India’s MMR. Unfortunately, magnesium utilization is less than optimal and this lower-than-necessary utilization is due to supply shortages, lack of institutional clinical guidelines, and lack of knowledge about its usage by health-care workers [9]. In addition to challenges with the administration of magnesium to treat PE–E, lack of emergency obstetric and neonatal care contributes critically to persistently high rates of maternal and neonatal morbidity and mortality [7, 11]. Interventions promoting institutional delivery have been able to reduce India’s MMR, but other gaps in care, such as suboptimum quality of services during institutional deliveries and lack of knowledge around the treatment of PE–E, persist [12–15].
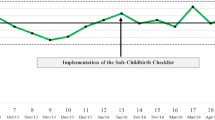
To address this deficit, a competency-based certificate program to train Indian non-specialist public sector physicians in emergency obstetric care (EmOC) was developed through a partnership between the Ministry of Health and Family Welfare, Government of India (GOI), the Federation of Obstetric and Gynaecological Societies of India (FOGSI), and its academic wing, the Indian College of Obstetricians and Gynaecologists (ICOG) (Fig. 1). Non-specialist public sector physicians were those who minimally held an Medicinae Baccalaureus, Baccalaureus Chirurgiae (MBBS) and were posted in public health facilities run by the Indian government. This EmOC training program was managed and implemented by Avni Health Foundation (AVNI), conducted in medical colleges and district hospitals, and intended to increase the provision of comprehensive EmOC in underserved areas. Details of this program have been documented elsewhere [14]. The aim of this study is to examine rates of magnesium utilization by EmOC trainees to treat PE–E in India. We examine rates of maternal and neonatal mortality among pregnant women who receive care from an EmOC-trained non-specialist physician and explore associations between mortality, magnesium administration, and cesarean delivery. We hypothesize that magnesium administration varies and is associated with PE–E severity.

EmOC training program setup
Materials and Methods
EmOC trainees maintained logbooks of clinical encounters, including primary and secondary diagnoses, procedures performed, treatments administered, and maternal and neonatal outcomes. These deidentified case records were entered in a centralized repository; 18,528 patient entries (13,238 deliveries) from 75 district hospitals in 12 states between 2006 and 2012 were included. Women with a pregnancy-related hypertensive disorder were identified as those with the diagnosis of pregnancy-induced hypertension (PIH), preeclampsia, or eclampsia. Those with PIH or preeclampsia were subsumed as “preeclampsia,” in view of their common pathophysiology and risk of eclampsia. Records containing a PE–E diagnosis and a diagnosis or procedure unique to the first half of pregnancy (N = 13) were excluded. Additional variables included in this analysis were: route of delivery, receipt of magnesium, maternal mortality, and neonatal mortality. Univariate and multivariate analyses were conducted. Logistic regressions were performed with SAS JMP Pro 10.0 software. A P value less than 0.05 was taken as statistically significant. Ethical approval for secondary analysis of these data was obtained by the University of Alabama at Birmingham (UAB) Institutional Review Board.
Results
There were 1320 identified cases of PE–E (7.1% of records, 10.0% of deliveries), of which 322 (24.4%) reported having eclampsia. Comparatively, national estimates show the rate of PE–E is about 8.0% in India [7, 15]. The proportion of cases with PE–E and eclampsia differed by state (Table 1); PE–E ranged from 1 to 14%, and eclampsia ranged from less than 1–83%. To examine the direct management of PE–E by trainees, health records were aggregated for the seven states reporting thirty or more cases of PE–E (Supplementary Table 1). Trainees directly managed 48% of all reported PE–E cases.
Use of Magnesium Sulfate
The EmOC training manual that was used advises treatment with magnesium in eclampsia and severe preeclampsia, employing a loading dose of 4 gm intravenously (IV) and 10 gm intramuscularly (IM) in 2 divided doses, followed by maintenance treatment with 5 g IM every 4 h. Trainees received extensive education on the management of PE–E and administration of magnesium which included but was not limited to side effects of magnesium on mother and fetus (e.g., maternal nausea, low calcium levels in fetus) and guidelines for proper use (e.g., loading dose, maintenance dose, and toxicity). Trainees were also informed that, depending on the severity of the PE–E, magnesium alone may not be a sufficient treatment. Of the 58 training centers with at least one reported PE–E case, 33 (57%) reported at least one use of magnesium in PE–E. “Other anticonvulsants” were reported in only eight cases overall, five of whom had stated PE–E and four of whom received magnesium.
With a view to identifying regional and hospital-wise differences in the availability and utilization of magnesium, the number of PE–E cases who received magnesium was examined both by state and by the presence or absence of eclampsia. As shown in Table 2, across the seven largest volume states magnesium was given to a mean of 12.9% of preeclamptic and 54.3% of eclamptic women (P < 0.001 for difference). The proportion with eclampsia that received magnesium in each state varied from 12 to 76%, with lower rates found in rural communities.
Route of Delivery and Association with Use of Magnesium
Of the 1268 women with PE–E treated in the seven largest volume states, route of delivery was noted for 741 (58.4%). Among these, the overall cesarean delivery rate was 59.0% and the instrumental vaginal delivery rate for non-breech presentations, including forceps and vacuum, was 2.2%. The cesarean rate according to the diagnosis of eclampsia and the use of magnesium is shown in Table 3. The cesarean rate was greater in cases where magnesium was not given (P < 0.001); after stratification by eclampsia status, this difference was significant only in the preeclampsia subgroup. The cesarean rate was higher in preeclamptic (63.5%) than in eclamptic women (38.9%; P < 0.001).
Maternal and Neonatal Morbidity
PE–E was associated with an excess risk of maternal hemorrhage due to disseminated intravascular coagulopathy (DIC) [9.0% vs. 0.6% without PE–E (P < 0.001); RR 15.7 (95% confidence interval {CI} 12.1–20.3)]. Women with PE–E were also more likely to undergo induction of labor [1.8 vs. 1.1% (P = 0.02); RR 1.7 (CI 1.1–2.6)] and to receive an antihypertensive medication [8.0 vs. 0.1% (P < 0.001); RR 81 (CI 49–135)]. PE–E was not associated with an excess risk of maternal sepsis, hemorrhage from causes other than DIC, requirement for resuscitation, or with an excess risk of neonatal resuscitation.
Maternal Mortality
Among the 1308 women with PE–E for whom maternal vital status was included in the database, there were 24 deaths (1.8%). By contrast, among the 17,179 women without reported PE–E, there were 95 reported deaths (0.6%). Both MMRs, for those with and without PE–E, are much higher than the Millennium Development Goal target of 0.15%. The relative risk of death in women with PE–E was 3.3 (CI 2.1–5.2). The death rate in eclamptic women (5.1%; 16 deaths) was significantly greater than that in preeclamptic women (0.8%; eight deaths; P < 0.001).
Use of magnesium was associated with a higher death rate in preeclamptic (RR for death with magnesium use 6.5, CI 1.6–25.5, P = 0.01) but not eclamptic women (RR 1.1, CI 0.4–2.9). This finding is consistent with the trainees’ curriculum, which specified magnesium treatment for eclampsia and severe but not mild preeclampsia, and which, if followed, would be expected to produce confounding by severity. Thus, those with severe preeclampsia and eclampsia are at greater risk of death, as well as treatment with magnesium; provision of magnesium may not stop all maternal deaths, and its effectiveness is dependent on dosage and time of administration. Indeed, logistic regression of maternal mortality on magnesium use and eclampsia status revealed a significant (P < 0.05) positive interaction between these two variables. Controlling for the interaction in the regression, the presence of eclampsia and the use of magnesium were associated with odds ratios (OR) of 3.9 (CI 1.9–7.8) and 2.7 (CI 1.3–5.2) for maternal death, respectively. Performance of cesarean delivery did not alter the maternal mortality rate, before or after adjustment for eclampsia and magnesium use.
Neonatal Mortality
Overall, 16 of 797 neonates (2.0%) born to mothers with PE–E died, compared with 148 of 13,049 neonates (1.1%) born to mothers without PE–E (P = 0.03); the RR of neonatal death with PE–E was 1.8 (CI 1.1–2.9). The Indian infant mortality rate is 39 per 1000 live births, or 0.39%; comparatively, outcomes from this dataset reflect that pregnant women with PE–E show a higher rate of infant deaths as compared to pregnant women without PE–E.
Thirteen of these 16 deaths occurred in Jharkhand. As expected, neonatal mortality was greater in offspring of eclamptic than of preeclamptic mothers (9.0 vs. 0.46%; P < 0.001). This difference was not found, however, in the subgroup that received magnesium (N = 105; P = 0.3). When the combined effects on neonatal mortality of magnesium use and eclampsia status are analyzed by logistic regression including an interaction term, eclampsia (OR = 9.2 [CI 2.8–48.4]), but not magnesium use, significantly altered mortality. A modest improvement in neonatal mortality was noted with cesarean section among mothers with PE–E (1.1 vs. 3.5% mortality, P = 0.023), but this effect was not seen after adjustment for eclampsia status.
Discussion
Consistent with the 8% prevalence of PE–E reported nationwide [7, 15], women in this sample with PE–E represented 7% of the cases logged by the trainees. Eclampsia was reported in 24% of those cases, and these women were more likely to receive magnesium (54 vs. 13% in preeclampsia). In preeclamptic but not eclamptic women, magnesium treatment was negatively associated with cesarean delivery and positively associated with mortality, pointing to the use of magnesium in more severe cases of preeclampsia. Non-use of magnesium in eclamptic women was associated with greater neonatal mortality. Great variability in magnesium use by state and by facility was observed, pointing to differences in either magnesium availability or in the onsite availability of personnel trained in its use.
Considering the well-documented success of EmOC training programs [16, 17], these less-than-optimal statistics point to structural barriers that persist across India. Being such a populous country, with high levels of poverty, adequate health care for its citizens is lacking [9]. This includes the accessibility of magnesium sulfate [10]. Magnesium provision and appropriate health care were further hindered by limited drug availability, especially at tertiary care health facilities [10]. These shortages may be due to magnesium being unavailable from pharmaceutical providers [18], gaps in medication management, or because of issues in transporting the drug from urban hubs to more remote communities.
Limitations
Not included in the dataset was information on patient age, timing of a first eclamptic seizure, dosage of magnesium, magnesium initiation relative to delivery, and magnesium-related measures at complementary primary and secondary centers. Parity was not consistently noted. These are significant limitations of our dataset that preclude a better understanding of regional patterns of magnesium utilization and the clinical context of its use. An additional limitation of our findings is that because care and training took place in district hospitals, the patient population in the dataset is not representative of obstetric patients in the states or even districts as a whole, and likely displays a greater level of acuity and severity. Trainee records from some regions were likely incompletely entered into the database. Despite these limitations, our dataset does allow for examination of the utilization of magnesium for PE–E within the context of the experience of EmOC trainees in tertiary hospitals in disparate regions of India, as well as examination of the maternal and neonatal mortality rates in the seven states for which sufficient case volume is available.
Conclusion
Magnesium sulfate is on the World Health Organization’s Model List of Essential Medicines [19] and has been included in India’s registry of essential medicines since 2003. The Indian Ministry of Health and Family Welfare, as well as curriculum guidelines for our EmOC trainees, states that “MgSO4 is the drug of choice to control convulsions in eclampsia” and that in women laboring with severe (but not mild) preeclampsia, “MgSO4 should be given to prevent eclampsia” [20]. Despite these guidelines, magnesium was received by only 54% of eclamptic women, and magnesium was administered at the district hospital level in only 13% of preeclamptic women. Possible reasons for this considerable shortfall include a lack of drug availability, a lack of facility support such as staff training for its use, or a lack of physician education on its indications [18]. Although our dataset cannot inform or distinguish between the first two considerations, it is valuable to juxtapose the well-documented success of EmOC training programs in lowering the MMR and IMR [16, 17] against the also-noted shortage of magnesium sulfate in India, with its availability reported in only 39 and 48% of “higher public facilities” [9, 21].
Therefore, to optimize monies spent on provider training, specifically EmOC training, the consistent availability of magnesium sulfate to treat PE–E in India should be improved. Increasing drug availability, implementing clinical guidelines around its administration, and training health-care providers on the identification and treatment of PE–E could lead to notable improvements in maternal and infant mortality. This anticipated reduction in preventable deaths has significant implications for community health and would likely elevate the health standing of India as compared to other low- and middle-income nations.
References
CensusInfo India Dashboard 2011 [cited 2014 November 26]. http://www.censusindia.gov.in/2011-common/census_info_2011.html.
Sanneving L, Trygg N, Saxena D, et al. Inequity in India: the case of maternal and reproductive health. Glob Health Action. 2013;6:19145.
World Health Organization. Global health observatory country views: India. Statistics summary 200–2015. Geneva: World Health Organization; 2015. http://apps.who.int/gho/data/node.country.country-IND?lang=en.
India in Figures 2015, Ministry of Statistics and Programme Implementation Central Statistics Office, Research & Publication Unit, Government of India, New Delhi. http://mospi.nic.in/mospi_new/upload/India_in_figures-2015.pdf.
Press Information Bureau Government of India, Ministry of Health and Family Welfare. Millennium Development Goals May 2013 [cited 2015 5 February]. http://pib.nic.in/newsite/PrintRelease.aspx?relid=95498.
Planning Commission Government of India. Brief on the functions of Health, and Family Welfare Division, Twelfth Five Year Plan (2012–2017) [cited 2015 23 March]. http://planningcommission.gov.in/sectors/index.php?sectors=hea.
Gupta SK, Pal DK, Tiwari R, et al. Impact of Janani Suraksha Yojana on institutional delivery rate and maternal morbidity and mortality: an observational study in India. J Health Popul Nutr. 2012;30:464–71.
Salvador-Moysén J, Martínez-López Y, Ramírez-Aranda J, et al. The social conditions in the genesis of preeclampsia. Open J Epidemiol. 2014;4:115–21. doi:10.4236/ojepi.2014.43016.
Jayanna K, Mony P, Ramesh B, et al. Assessment of facility readiness and provider preparedness for dealing with postpartum haemorrhage and pre-eclampsia/eclampsia in public and private health facilities of northern Karnataka, India: a cross-sectional study. BMC Pregnancy Childbirth. 2014;14(1):304.
Health Management Information System. Health and Family Welfare Statistics in India 2013 Ministry of Health & Family Welfare2013 [cited 2014 November 26]. https://nrhm-mis.nic.in/SitePages/Pub-FW-Statistics2013.aspx.
Moran NF, Naidoo M, Moodley J. Reducing maternal mortality on a countrywide scale: the role of emergency obstetric training. Best Pract Res Clin Obstet Gynaecol. 2015;29:1102–18.
Ng M, Misra A, Diwan V, et al. An assessment of the impact of the JSY cash transfer program on maternal mortality reduction in Madhya Pradesh, India. Glob Health Action. 2014;7. http://www.globalhealthaction.net/index.php/gha/article/view/24939/0. Accessed 23 Jan 2017.
Guin G, Sahu B, Khare S, et al. Trends in maternal mortality and impact of Janani Suraksha Yojana (JSY) on maternal mortality ratio in a tertiary referral hospital. J Obstet Gynecol India. 2012;62(3):307–11.
Bhushan H, Bhardwaj A. Task shifting: a key strategy in the multipronged approach to reduce maternal mortality in India. Int J Gynecol Obstet. 2015;131:S67–S70.15.
Sajith M, Nimbargi V, Modi A, et al. Incidence of pregnancy induced hypertension and prescription pattern of antihypertensive drugs in pregnancy. Int J Pharma Sci Res. 2014;23:4.
Otolorin E, Gomez P, Currie S, et al. Essential basic and emergency obstetric and newborn care: from education and training to service delivery and quality of care. Int J Gynecol Obstet. 2015;130(Supplement 2):S46–53.
Ahmed U, Farid S, Luqman M, et al. An evaluative study of emergency obstetric care services in Southern Punjab. Int J Innov Appl Stud. 2015;10(4):1233.
American Society of Health-System Pharmacists. Current Shortages Magnesium Sulfate Injection 2015. http://www.ashp.org/menu/DrugShortages/CurrentShortages/Bulletin.aspx?id=757.
World Health Organization. WHO model list of essential medicines, 19th list. World Health Organization; 2015. http://www.who.int/medicines/publications/essentialmedicines/en/. Accessed 23 Jan 2017.
Ministry of Health and Family Welfare Government of India. National Health Mission Guidelines: Protocol posters from FRU to MC [cited 2015 5 February]. http://www.who.int/medicines/services/expertcommittees/essentialmedicines/TRS933SelectionUseEM.pdf.
Chaturvedi S, Randive B, Mistry N. Availability of treatment for eclampsia in public health institutions in Maharashtra, India. J Health Popul Nutr. 2013;31(1):86.
Acknowledgements
We would like to thank the maternal health division team at GOI (Dr. H Bhushan and Dr. Rajeev Agarwal), FOGSI, ICOG, chief coordinators, technical coordinators, master trainers, district trainers, nodal officers, state government officials, non-specialist physician trainees, and Avni Health Foundation team members, who have all contributed to successful program implementation. Additionally, the team thanks the UAB Sparkman Center for Global Health for their ongoing partnership.
Author Contributions
NAC was responsible for hypothesis formulation, data analysis, and initially drafting the manuscript. AB contributed to the development, implementation and management of the training program described, and revised the manuscript critically. CNP contributed to the development, administrative support for program implementation, and reviewing the manuscript. SD and PB conceptualized the EmOC program and developed partnerships with the Government and other agencies for the national scale up of the program and reviewed the manuscript. DB provided GOI led program support and reviewed the manuscript. HBu provided the public health perspective, coordinated communication between UAB and AVNI, and revised the manuscript critically. PS was one of the key program implementers and revised the manuscript critically.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethical Approval
Ethical approval was provided by the University of Alabama at Birmingham’s Institutional Review Board (#N150209004).
Additional information
Dr. Henna Budhwani is an Assistant Professor and Deputy Director at School of Public Health, University of Alabama at Birmingham, Birmingham, USA; Dr. Poonam Shivkumar is a HOD at Mahatma Gandhi Institute of Medical Sciences, Wardha, India; Dr. Chittaranjan Narhari Purandare is a President at International Federation of Gynecology and Obstetrics, FIGO House, London, UK; Dr. Nicholas A. Cataldo is a Gynecologist and Obstetrician at School of Public Health, University of Alabama at Birmingham, Birmingham, USA; Dr. Sadhana Desai is a Gynecologist and Obstetrician at Federation of Obstetric and Gynaecological Societies of India, Mumbai, India; Dr. Prakash Bhatt is a Gynecologist and Obstetrician at Federation of Obstetric and Gynaecological Societies of India, Mumbai, India; Dr. Dinesh Baswal is a Deputy Commissioner—Maternal Health at Ministry of Health and Family Welfare, Government of India, New Delhi, India; Dr. Ajey Bhardwaj is a Founder Director at Avni Health Foundation, Mumbai, India.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Budhwani, H., Shivkumar, P., Purandare, C.N. et al. Examining the Use of Magnesium Sulfate to Treat Pregnant Women with Preeclampsia and Eclampsia: Results of a Program Assessment of Emergency Obstetric Care (EmOC) Training in India. J Obstet Gynecol India 67, 330–336 (2017). https://doi.org/10.1007/s13224-017-0964-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-017-0964-9