
Abstract
Objective
This study was conducted to compare underweight and obese women and their weight gain during pregnancy on fetomaternal outcome.
Method
This is a prospective, non-interventional, observational study on 1000 women (BMI between 20 and 30 were excluded). Women attending ANC OPD with singleton pregnancy at or before 16 weeks were included and BMI calculated in early pregnancy. Their weight gain during pregnancy was noted. Any complications in the mother or perinate were noted.
Results
Incidence of obesity in our institute was 17 % and that of underweight was 18 %. Pre-eclampsia, gestational hypertensions, gestational DM, antepartum hemorrhage, all were more common among obese women, while anemia was more common in the underweight. Post-dated pregnancy, induction of labor, cesarean delivery, and postpartum complications were more common in obese women. Fetal complications were also higher in obese patients.
Conclusion
Lower as well as higher prepregnancy BMI is an independent risk factor that is associated with increased morbidity and mortality in both the mother and the fetus.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obesity is attaining the status of global epidemic worldwide. Overall, in 2014, about 13 % of the world’s adult populations (11 % of men and 15 % of women) were obese. In 2014, more than 1.9 billion adults, 18 years and above, were overweight. Of these, over 600 million were obese [1]. According to National Family Health Survey (NFHS) [2], the percentage of married women (15–49 years) who are overweight or obese increased from 11 % (NFHS 2) to 15 % (NFHS 3). Undernutrition is more prevalent in rural areas, whereas obesity is three times higher in urban area.
India is unique as it suffers from a dual burden of obesity and malnutrition. More than one-third (36 %) women have BMI lower than 18.5. In India, a higher number of malnourished women reside in Chhattisgarh, Bihar, and Jharkhand, whereas most of the obese women are from Punjab, Delhi, and Kerala [3].
Obesity during pregnancy carries a higher risk (1.32 times) of morbidity and mortality for both mother and the fetus. On the other hand, underweight is associated with IUGR & anemia. Weight gain during pregnancy has a recommended range throughout 40 weeks of pregnancy. If the weight gain is more or less than the proposed, it is associated with an adverse outcome for both the mother and the baby [4].
Material and Method
This was a prospective, non-interventional, observational study on 1000 pregnant underweight women with BMI less than 19.9 and obese women with BMI more than 30.
Inclusion criteria: Singleton pregnancy at/before 16 weeks of gestational age (before any significant impact of weight gain).
Exclusion criteria:
-
Women with BMI 20–29.9,
-
Multiple pregnancies,
-
Major structural anomaly and
-
Medical complications such as diabetes and hypertension.
BMI was calculated and women were categorized into 5 groups:
-
Group A, Underweight <19.9 kg/m2;
-
Group B, Normal = 20–24.9 kg/m2 (excluded);
-
Group C, Overweight = 25–29.9 kg/m2 (excluded);
-
Group D, Obese = 30–34.9 kg/m2;
-
Group E, Morbidly obese > 35 kg/m2 (no woman was in this group).
In both groups, weight gain was noted according to Institute of Medicine (IOM) [5] criteria on regular basis till delivery, along with the complications and outcome. The outcomes of labor and delivery were compared between both groups. Descriptive statistics were calculated for all study variables. Continuous variables were presented as the mean and standard deviation, while categorical data were calculated as percentage. Bivariate analysis was done to examine the association between prepregnancy BMI and fetomaternal outcomes. A value of P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS for windows version 20.
Results
A total of 2700 women were enrolled in this study from 2011 to 2014. After applying inclusion and exclusion criteria, 1000 women were included in the study sample. Among these 1000 women, 486 were obese and 514 were underweight. There was not a single woman in the morbidly obese group.
Women who were obese before pregnancy had a mean age of 27.00 as compared to lean women with mean age of 24.25. Lean women were mostly from rural area.
Significant number of the women had recommended weight gain in both groups. In the obese group, 55.9 % women had induced labor and 57.8 % delivered by cesarean section (Table 1).
Obese women suffered more complications such as gestational diabetes, gestational hypertension, pre-eclampsia, macrosomia, antepartum hemorrhage, etc. Birth weight and proportion of babies weighing over 4 kg increased in the obese group (Table 2).
An interesting observation was that a higher total weight gain in pregnancy led to more antenatal complications (Table 3).
Preterm as well as post-term delivery are more common in the obese women (Table 4).
Anemia was more prevalent in lean women, whereas postpartum complications such as PPH and infections were frequently seen in obese women.
Discussion
Pregnancy is a valuable event in the life of a woman. During pregnancy, a woman often visits the antenatal clinics. Small and simple parameter like weight gain over the past visit is often ignored by the busy obstetricians. Ideal weight gain is an important factor for a good fetomaternal outcome. Obesity is emerging as an epidemic worldwide. We were surprised to see the incidence of obesity in the antenatal woman as 17 %, not too far behind from that of the U.S, where it is 20 % in some antenatal clinics [6]. Incidence of underweight was 18 %, almost similar to that of obesity.
Although pregnancy complications in obese women are well documented, the evidence in relation to problems of underweight is less clear [7]. In this study, we have compared both the extremes of BMI with fetomaternal outcome.
In 2009, IOM put forth new guidelines regarding the gestational weight gain in relation to BMI [5]. The pregnancy and gestational weight gain, whether excessive or inadequate, are associated with a poor fetomaternal outcome.
The women in our study were mostly 25 years old in the underweight group and 27 years old in the obese group. They usually had unplanned pregnancy and low awareness about nutrition and its impact on pregnancy.
Evidence across different obstetric populations is consistent that increased prepregnancy BMI associates with increased obstetric interventions such as labor induction and surgical interventions [8, 9]. In support of these reports, Table 1 results showed that intranatal problems such as induction and cesarean section were more likely in the obese group. Increase in the risk of cesarean section rate after induction was independent of obstetric complications and confounding factors. One hypothesis for increased risk of cesarean section after induction includes altered uterine contractility combined with dysfunctional labor. Furthermore, priming the myometrium for transitioning from quiescence to contractility may be altered with increased BMI and adipose tissue mass [10].
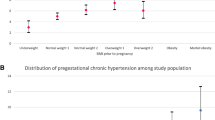
After adjusting for all confounding factors, we found positive association of BMI with GDM, pre-eclampsia, GHTN, and APH (Table 2). Nan Li et al. [11] and other previous studies concluded that obesity is associated with adverse pregnancy outcomes such as GDM and pregnancy-induced hypertension.
Consistent with the previous results, we found significantly high incidence of still birth with high BMI. Single most common modifiable factor for still birth in developed world is maternal obesity [12]. According to Auckland prospective stillbirth study [13], obesity is an independent risk factor.
We found a significant correlation of obese women with fetal weight. The same has been shown in other study. Maternal obesity is a strong predictor of fetal birth weight or large for gestational age [14–17]. Recently, Modi et al. [18] have shown that increasing maternal BMI is associated with the increasing abdominal and intrahepatocellular lipid content in neonatal offspring. It was observed that with the increase in abdominal circumference, neonatal morbidity increased.
We found positive association between gestational weight gain and GDM, Macrosomia, GHTN, and Pre-eclampsia (Table 3). This association was consistent with the previous results [11].
Table 4 showed that incidences of preterm and post-term delivery both are high in the obese group. However, data supporting the preterm delivery in obesity are less conclusive [19–21]. A recent meta-analysis provided evidence that the association between preterm birth and obesity may vary depending upon the subtype of preterm births [22]. Obesity and excess weight gain are associated with preterm birth, macrosomia, and stillbirth, while underweight BMI and low weight gain have been associated with small for gestation or IUGR and preterm births.
Among studies related to risk factors for PPH, BMI is rarely considered as a risk factor for PPH. In these studies, results are inconsistent with the one showing no association of BMI with PPH [23], but others showing positive association [24].
There is a direct impact of high or low BMI on hospital admission and short-term costs to the health services.
Conclusion
In our study, we observed that both groups correlated well with various adverse fetomaternal outcomes. Apart from deleterious impact on pregnancy, obesity may also affect clinical decision for the management of labor and delivery, which ultimately may have repercussion on health care cost and maternity services. Thus, not only the antenatal period, but the intranatal as well as the postnatal period may be adversely affected in relation to BMI.
There is a lack of studies on underweight pregnant women. Our study shows its association with anemia only. Given a choice, obesity is more commonly associated with worse fetomaternal outcome. Weight is a very simple parameter which can be easily measured. So weight gain during pregnancy is an important clinical parameter to be followed. Identifying an obese or an underweight pregnant woman allows a proper planning throughout the antenatal period for any risk management. So referral to a dietician for dietary assessment and counseling should be considered for both lean and obese women.
References
WHO Global InfoBase- data and analysis of overweight and obesity, Fact sheet N0, 311, updated on January 2015.
Mohan Reddy N, Kalyana Kumar CH, Jamil K. New world syndrome (obesity) in South India. 2012;1:567 .doi:10.4172/scientificreport.567.
National Family Health Survey on Adult Nutrition. 2005–2006 .
Ahmed SR, Ellah MA, Mohamed OA, et al. Prepregnancy obesity and pregnancy outcome. Int J Health Sci, Qassim. 2009;3(2):203–8.
Institute of medicine. weight gain during pregnancy: reexamining the guidelines. Washington, DC: National Academic Press; 2009.
Elly Tsoi, Humera Shaikh, Stephen Robinson, et al. obesity in pregnancy; a major health care issue. Postgrad Med J. 2010;86(1020):617–23.
Sue Brydon et al. Guideline for low body mass index (BMI) in antenatal women, Nottingham University Hospitals (NHS Trust). July 2015.
Arrowsmith S, Wray S, Quenby S. Maternal obesity and labour complication following induction of labour in prolonged pregnancy. BJO. 2011;118(5):578–588.
Briese V, Voigt M, Wisser J, et al. Risk of pregnancy and birth in obese primiparous women: an analysis of German perinatal statistics. Arch Gynecol Obstet. 2011;283(2):249–53.
Lowe NK, Corwin EJ. Proposed biological linkage between obesity, stress, and inefficient uterine contraction during labour, in human. Med Hypothesis. 2011;76(5):755–60.
Li N, Liu E, Guo J, et al. Maternal prepregnancy body mass index and gestational weight gain on pregnancy outcome. PLoS One. 2013;8(12): e82310. doi:10.1371/journal.pone.0082310.
Flenady V, Middleton P, Smith GC, et al. Stillbirth: the way forward in high income countries. Lancet. 2011;377:1703–17.
Stacey T, Thompson JM, Mitchell EL et al. The auckland still birth study, a case control study exploring modifiable risk factors for third trimester still birth: method of rationale. Aust N Z J Obstet Gynecol, Article first published online 6 Dec 2010.
Makgoba M, Sawidou M, Steer P. The effect of maternal characteristics and gestational diabetes on birthweight. BJOG. 2012;119:1091–7.
Voigt M, Zels K, Guthmann F, et al. Somatic classification of neonates based on birth weight, length and head circumference: quantification of the effect of maternal BMI and smoking. J Perinat Med. 2011;39:291–7.
Ovesen P, Rasmussen S, Kesmodel U. Effect of prepregnancy maternal overweight and obesity on pregnancy outcome. Obstet Gynecol. 2011;118:305–12.
Owens LA, O’Sullivan EP, Kirwan B, et al. ATLANTIC DIP: the impact of obesity on pregnancy outcome in glucose tolerant women. Diabetes Care. 2010;33:577–9.
Modi N, Murgasova D, Ruager-Martin R, et al. The influence of maternal body mass index on infant adiposity and hepatic lipid content. Paediatr Res. 2011;70:287–91.
McDonald SD, Han Z, Mulla S, et al. Obesity and overweight in mothers and risk of preterm birth and low birth weight in infants: systematic review and meta-analysis. BMJ. 2010;341:c3428.
Savitz DA, Stein CR, Siega-Riz AM, et al. Gestational weight gain and birth outcome in relation to prepregnancy body mass index and ethinicity. Ann Epidemiol. 2011;21:78–85.
Aly H, Hammad T, Nada A, et al. Maternal obesity, associated complications and risk of prematurity. J Perinatol. 2010;30:447–51.
Torloni MR, Betran AP, Daher S, et al. Maternal BMI and preterm birth: a systematic review of literature with meta analysis. J Matern Fetal Neonatal Med. 2009;22:957–70.
Driessen M, Bouvier-Colle M-H, Dupont C, et al. Postpartum hemorrhage resulting from uterine atony after vaginal delivery: factor associated with severity. Obstet Gynecol. 2011;117(1):21–31.
Fyfe EM, Thompson JM, Anderson NH, et al. Maternal obesity and postpartum hemorrhage after vaginal and cesarean delivery among nulliparus women at term: a retrospective cohort study. BMC Pregnancy Childbirth. 2012;12:112.
Compliance with Ethical Requirements and Conflict of Interests
Abha Singh and Sumi Agrawal declares that they have no conflict of interest. As this was prospective observational study, not an interventional or case control study, informed conset with human subjects for being included in the study was not necessary, however all procedures followed were in accordance with ethical standard of the responsible committee on human experiments (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008(5).
Author information
Authors and Affiliations
Corresponding author
Additional information
Sumi Agrawal is Assistant Professor at Pt. JNM Medical College Raipur, Chhattisgarh, India; Abha Singh is Director, Professor & HOD at Pt. JNM Medical College Raipur, Chhattisgarh, India.
Rights and permissions
About this article

Cite this article
Agrawal, S., Singh, A. Obesity or Underweight—What is Worse in Pregnancy?. J Obstet Gynecol India 66, 448–452 (2016). https://doi.org/10.1007/s13224-015-0735-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-015-0735-4