
Abstract
Implantable chemoport is a very useful device for long-term venous access for infusion of chemotherapeutic drugs and other agents. Niederhuber et al. (Surgery 92:706–712, 1982) reported on the first use of the totally implantable central venous port system (TICVPS) in 1982. Five hundred patients undergoing surgical implantation of chemoports in Bharath Cancer Hospital, Mysore, India, between September 2020 and June 2022 were included in this prospective observational cohort study. Five hundred chemoport implantations were available for analysis. The cephalic vein cut down technique was attempted in 500 patients and successful in 410 patients (82.2%). There were no intraoperative complications. Venous access device systems are nowadays widely used in cancer patients to facilitate frequent perfusions of chemotherapy (Vescia et al. in Ann Oncol 19(1):9–15, 2008). The placement of totally implanted venous access devices started 30 years ago. Since then, different techniques were established to reduce complications and to make the implantation safe and comfortable for patients (Teichgraber et al. in Cardiovasc Intervent Radiol 32(5):975–979, 2009). The cephalic vein cutdown approach for CICVAD placement appears to be a safe and better alternative to the percutaneous subclavian vein approach in cancer patients. Cephalic vein cut down approach is LESS with More benefits.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Implantable chemoport is a very useful device for long-term venous access for infusion of chemotherapeutic drugs and other agents. Niederhuber et al. [1] reported on the first use of the totally implantable central venous port system (TICVPS) in 1982. The port system is built of a central catheter, which is inserted into a cannulated vein beneath the skin and attached to a port chamber that is placed into a subcutaneous pocket. Access of this totally implanted reservoir is possible with a special needle that allows puncture of the skin and silicone membrane of the port chamber. Chamber puncture has to take place under sterile conditions. These devices have decreased the patient anxiety associated with repeated venipunctures, and due to the totally subcutaneous position, the port devices are invisible and are cosmetically more acceptable [2]. Although several methods have been established for the implantation of these devices, the surgical team has a learning curve with respect to the choice of vein and the choice of technique. Techniques for external cannulation of the subclavian and internal jugular veins were described by Broviac and Hickman in the 1970s [3]. In 2008, Gallieni et al. have outlined the choice of the different devices suitable for different settings. The cephalic vein cut down technique was described in the 1980s initially for placement of pacemakers and later used for implantation of chemoports. This technique is attractive for the beginner as the theoretical chances of complications are lesser. But no technique is flawless and the same patient may need multiple attempts and multiple vein punctures for the successful implantation of the chemoport. Patients who have received chemotherapy earlier may have extensively thrombosed veins causing further difficulties in implantation of chemoports. Advantages include less interference with daily activities, less frequent flushing, and reduced risk of infection. Disadvantages include the need for needle insertion, increased discomfort, and risk of extravasation. These devices are expensive and are more difficult and time-consuming to insert and remove but on the long run of chemotherapy, they have proved to be cost-effective [4]. We present our experience of chemoport placement using the cephalic vein cut down technique to begin the implantation of the chemoports in our institution and assessment of various postoperative complications associated with the TICVPS at our centre.
Patients and Methods
Five hundred patients undergoing surgical implantation of chemoports in Bharath Cancer hospital, Mysore, India, between September 2020 and June 2022 were included in this prospective observational cohort study. Patients undergoing second time implantation of chemoport after failure or removal of the previously inserted port were excluded from the study. The demographic details of patients and surgical techniques were entered into a database and they were followed up at the chemotherapy units, where further follow-up details with respect to the chemoport access, usage and other outcomes were collected. Informed consent was obtained from all patients included in the study.
Chemoport Insertion Technique
The chemoports were implanted either during the time of primary cancer surgery under general anaesthesia or as a day-care procedure under local anaesthesia. Size of the chemoport was selected according to patient build and physique.
The procedure is as follows:
-
Site of Open Cut Down: The cephalic vein is accessed via an incision made in the deltopectoral groove, approximately 2–3 cm below the clavicle.
-
Technique:
-
1.
Patient Preparation: The patient is positioned supine with the arm abducted to 90 degrees.
-
2.
Incision: A 3–4-cm transverse incision is made in the deltopectoral groove.
-
3.
Vein Identification: The cephalic vein is identified and mobilised.
-
4.
Venotomy: A venotomy is performed, and a guide wire is inserted into the cephalic vein.
-
5.
Port Insertion: A peel-away sheath is introduced over the guide wire, followed by the insertion of the port catheter.
-
6.
Port Pocket Creation: A subcutaneous pocket is created in the pectoral region for the port reservoir.
-
7.
Connection: The catheter is connected to the port reservoir, and the system is flushed with saline to ensure patency.
-
8.
Closure: The incision is closed in layers, and the port is secured in the pocket.
-
1.
The cephalic vein was the initial vein of choice for all patients except in patients with severe truncal obesity.
No. 8 Fr. Groshong tip BARD Catheter (MRI compatible) was used in all patients. Catheter placement was guided by fluoroscopy. The tip of the catheter was placed at the superior vena cava–right atrial junction.
In case of failure of cannulation of cephalic vein, the second vein attempted was either the subclavian or the internal jugular vein by Seldinger technique. All surgical details including vein of insertion, sequence of veins used, and reason for failure were duly recorded. Any attempts in contralateral vein were recorded. Prior chemotherapy status was noted.
A check X-ray was taken for confirmation of port position. The patient was discharged on a 3rd-generation cephalosporin and an analgesic on the same day. Stitches were removed on 14th postoperative day. After every cycle of chemotherapy, the port was flushed using 1:10 diluted heparin (5000 IU/ml) and every 3 months, when the port was not in use. Data was analysed using the Statistical Package for Social Sciences (SPSS) version 17.0 for Windows. Collected data will be analysed by frequencies, percentages, and mean. Analyses of the present study were performed by reviewing the electronic medical records of the patients. The definition of periprocedural complications was classified into immediate, early, and late complications. Immediate complications are intra-procedural. Early complications were defined as complications that arose within 24 h, which were mostly procedure associated; early complications were the ones that occurred within 30 days after the procedure. Late complications were those that were detected beyond 30 days of insertion.
Results
Five hundred chemoport implantations were available for analysis. The cephalic vein cut down technique was attempted in 500 patients and successful in 410 patients (82.2%). There were no intraoperative complications.
The first vein of insertion was successful in 392 (63%) patients. Subclavian vein was not used as first vein of attempt in any patient. Ninety required conversions to the standard percutaneous subclavian vein approach. In those 90 patients, there were three reasons for the inability to place a CICVAD via the cephalic vein cutdown approach:
-
1.
The cephalic vein was too small for the catheter (50 patients).
-
2.
There was no predominant cephalic vein, but, rather, several tiny, branching venous tributaries within the deltopectoral groove generally associated with a large, predominant artery (35patients).
-
3.
It was not possible to transverse the angle of insertion of the cephalic vein into the subclavian vein (5 patient).
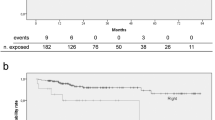
One hundred ninety CICVADs were placed via the right cephalic vein, and 220 CICVADs were placed via the left cephalic vein. Median operating time was 35 min (range, 25–64 min).
Although the right side is generally preferred due to anatomical considerations and ease of access, in our study, 220 ports were inserted on the left side compared to 190 on the right side. This variation was due to patient-specific factors, such as previous surgeries, anatomical variations, or other clinical considerations that necessitated left-sided insertion.
No immediate postoperative complications, such as pneumothorax, hemothorax, or injury to great vessels, were seen. Twenty-two patients (4.4%) developed post-operative hematoma at the port pocket. Majority of the patient were treated conservatively, and 3 patients required aspiration and compressive dressing (Table 1).
Long-term complications included shoulder pain which was the most frequent subjective complaint of the patients (46%). None of the patients required any intervention for pain. Catheter-related bacteraemia occurred in 22 patients of which 10 patients managed conservatively and 12 patients required port removal. The catheter-related bacteremia rate was 0.07 episodes per 1000 catheter-days. Median time to catheter-related bacteremia was 76 days (range, 36–164 days).
Deep venous thrombosis occurred in 18 of 410 patients (4.3%). All patients developing a deep venous thrombosis were determined to be hypercoagulable secondary to their primary malignancy. Median time to deep venous thrombosis was 83 days (range, 14–284 days). A superior vena cava stricture occurred in one patient. This was diagnosed 498 days after port placement. The port was removed at the time of balloon venoplasty of the superior vena cava.
Of the 90 CICVADs placed via the percutaneous subclavian vein approach, Median operating time was 60 min (range, 36–149 min). Catheter-related bacteremia occurred in 10 of 90 patients (11%).
Catheter pinch syndrome/kinking was noted in 8 patients, which was re-inserted in all cases.
Catheter tip malposition noted in 38 patients, of which 12 required reposition again and 26 patients no further management required as there was free flow and blood aspiration noted.
Chemoport cannulation-related complication included no blood aspiration was noted 28 patients (no patients required of any intervention as free flow and radiologically conformed the position) and difficult port palpation in 6 patients (required re-exploration in 4 patients and 2 accessed under ultrasound guidance).
Catheter migration is noted in 4 patients, and all of them required percutaneous angioplasty via CTVS team of doctors.
Discussion
Venous access device systems are nowadays widely used in cancer patients to facilitate frequent perfusions of chemotherapy [5]. The placement of totally implanted venous access devices started 30 years ago. Since then, different techniques were established to reduce complications and to make the implantation safe and comfortable for patients [6]. Biffi and colleagues were to show the equivalence of the three mostly used implantation techniques, i.e. percutaneous puncture of the internal jugular vein (‘blind’ via anatomical landmarks), ultrasound-guided access to the subclavian vein, and surgical cut-down access to the cephalic vein [7]. In the present study, the cephalic vein cutdown approach for CICVAD placement was successful in 82% and unsuccessful in 18% of the patients. Previous authors have reported a wide range of failure rates for the cephalic vein cutdown approach. Perry et al. [8] reported that the cephalic vein route was not technically possible in only 8% of cases. Au [9] reported that the cephalic vein was too small for admission of a catheter in 17% of cases. Davis et al. [10] and Gallichio et al. [11] reported that the cephalic vein cutdown approach was unsuccessful 25% of the time. Finally, Wade et al. [12] reported that the cephalic vein route was not successful in 62% of cases (Table 2).
No method has been shown to be superior to another [7, 12]. A Cochrane review of the methods used to insert the catheter such as Seldinger technique for the subclavian vein compared to the venous cut down technique had a higher implantation rate with the Seldinger technique [13].
The finding of the present study of an 18% failure rate for the cephalic vein cutdown approach is relatively consistent with two earlier cadaver-based studies [14]. Koketsu et al. attributed failure to small lumen (< 3 mm), absent cephalic vein and inability to traverse the cephalic vein into the subclavian vein [15]. In our study, we report similar difficulties with obliterated vein, absent vein, and < 3-mm lumen.
In most institutions, the chemoport is implanted at the beginning of the chemotherapy treatment. This theoretically leads to higher success rates and with the first vein of attempt itself. In lower resource populations, chemoports are implanted only in the setting of recurrence or palliation when all the peripheral venous access options are emptied. Chemotherapy causes thrombosis/obliteration of the vein lumen along the entire length of the vein. Our cohort had 53% patients previously treated with chemotherapy, and this probably is the cause for the lower cephalic vein success rate. A thorough literature search did not reveal any study correlating the success rate of cephalic vein cut down with prior chemotherapy status.
The side of insertion was chosen on the right side for the majority. Left side was used only in patients who had breast cancer on the right side and in one patient who specifically wanted it on the non-dominant side. Right side catheter implantation is preferred as it decreases length of implanted catheter and the angulation between the catheter axis and the axis of the superior vena cava is lesser [13]. In this study, the side planned was successful in majority of patients, and there were very few contralateral attempts. In a randomised study done on the preference of the side of implantation of a chemoport, there was no significant difference in the implantation rate or complications [13].
In a study by Wei et al., an established algorithm helps to choose the best entry vessel for the catheter insertion [13]. We have tried a similar approach in this study attempting the cephalic vein first, but the internal jugular vein and subclavian vein have been equally preferred for the subsequent percutaneous approach following failure of the cephalic vein attempt. While some authors completely avoid the subclavian vein, Harish et al. describe some additional manoeuvres such as bending the sheath for the natural curvature of the vein [16]. In this study, the subclavian approach was equally successful as the internal jugular vein and no additional complications were noted. We suggest that the subclavian vein may be equally placed in the algorithm.
In theory, the major advantage of the cephalic vein cutdown approach compared to the percutaneous subclavian vein approach is the elimination of the risks of developing immediate complications such as pneumothorax, haemothorax, and injury to the great vessels at the time of catheter insertion. In the present study, there were no cases of pneumothorax, haemothorax, or injury to the great vessels associated with the cephalic vein cutdown approach, thus, supporting this theory. Pre-existing medical conditions that could predispose an individual to the development of a haemothorax or injury to the great vessel would include thrombocytopenia, coagulopathy, hypovolaemia, and inability to tolerate the Trendelenburg position secondary to pre-existing cardiopulmonary diseases and abnormal body habitus (such as kyphosis, cachexia, or morbid obesity). Therefore, any patient with above pre-existing medical condition would benefit from use of the cephalic vein cutdown approach.
The 4.4% patients had fluid collection around the port in the immediate post-operative period managed conservatively and resolved with extended antibiotic therapy. Kinking of the catheter (catheter pinch-off), displacement, breakage, catheter migration are known delayed complications of chemoport placement. However, these complications are decreasing with better port design and better insertion techniques. Catheter-related blood stream infection is a lesser but significant complication in patients with indwelling chemoports. This necessitates surgical removal of the implanted device. Differential time to positivity is considered the best method to diagnose catheter related bacteraemia. In this study, 12 patients needed surgical removal of the chemoport for catheter-related bacteraemia.
The guidelines for indwelling catheters mandate that blood return on aspiration when cannulating the chemoport is necessary for administration of the drugs or heparin flushes. Absence of blood return (partial occlusion) was the cause for concern in 18% of the cannulations in this study. This was seen in patients who had completed chemotherapy and were undergoing flushing of the port to maintain patency. A standard chest x-ray can detect catheter dislocation or migration. However, the gold standard for diagnosis is radiographic visualisation with contrast injection via the chemoport. This is not a routine procedure before each cycle of chemotherapy as it is associated with the risk of contrast–medium-related complications, need for radiological facilities, and higher costs. Chest x-ray was adequate to confirm port position in majority of the patients in this study. These patients continued to have heparin saline flushing of the chemoport 3 monthly until the ports were removed. None of these patients had any untoward effect. The patients who had no blood return detected during the course of the chemotherapy schedule underwent radiological imaging including CT scans to ensure port position and had the rest of the chemotherapy without any complications using the chemoport, although blood could not be aspirated at any subsequent port cannulation. Fibrin sheath formation is said to be the commonest cause of this problem acting as a one-way valve preventing aspiration of blood while allowing infusion of fluids. The Groshong tip catheter used in all patients in this study is designed to decrease the risk of thrombus formation; however, fibrin film formation in the tips of the catheters can still occur.
Conclusion
The cephalic vein cutdown approach for CICVAD placement was successful in 82% of cancer patients. No immediate postoperative complications, such as pneumothorax, hemothorax, or injury to great vessels, were seen. Long-term complications of the cephalic vein cutdown approach for CICVAD placement, such as catheter-related bacteremia, site infections, and deep venous thrombosis, were relatively low and were comparable to those seen with the percutaneous subclavian vein approach in previous reports. An algorithm for the preference of veins to be used depending on prior chemotherapy status and preoperative vascular sonography can increase the success rate of insertion.
Our study demonstrates that the cephalic vein cut down technique is a safe and effective method for chemo port placement, with favourable outcomes. However, comparative studies are warranted to establish its benefits over the subclavian approach conclusively.
References
Niederhuber JE, Ensminger W, Gyves JW, Liepman M, Doan K, Cozzi E (1982) Totally implanted venous and arterial access system to replace external catheters in cancer treatment. Surgery 92(706):712
Tabatabaie O, Kasumova GG, Eskander MF, Critchlow JF, Tawa NE, Tseng JF (2017) Totally implantable venous access devices: a review of complications and management strategies. Am J Clin Oncol 40(1):94–105
Gallieni M, Pittiruti M, Biffi R (2008) Vascular access in oncology patients. CA Cancer J Clin 58:323–346
Burney IA, Khurshaidi N, Akbar MT, Bhatti FN, Siddiqui T, Sophie Z (2001) Complications of indwelling venous access devices: a single institution experience. J Pak Med Assoc 51(12):434
Vescia S, Baumgartner AK, Jacobs VR, Kiechle-Bahat M, Rody A, Loibl S, Harbeck N (2008) Management of venous port systems in oncology: a review of current evidence. Ann Oncol 19(1):9–15
Teichgraber UK, Streitparth F, Cho CH, Benter T, Gebauer B (2009) A comparison of clinical outcomes with regular- and low profile totally implanted central venous port systems. Cardiovasc Intervent Radiol 32(5):975–979
Biffi R, Orsi F, Pozzi S, Pace U, Bonomo G, Monfardini L, Della Vigna P, Rotmensz N, Radice D, Zampino MG, Fazio N, de Braud F, Andreoni B, Goldhirsch A (2009) Best choice of central venous insertion site for the prevention of catheter related complications in adult patients who need cancer therapy: a randomized trial. Ann Oncol 20(5):935–940
Perry EP, Nash JR, Klidjian AM (1990) Direct cephalic vein cannulation for safe subclavian access. J R Coll Surg Edinb 35:218–220
Au FC (1989) The anatomy of the cephalic vein. Am Surg 55:638–639
Davis SJ, Thompson JS, Edney JA (1984) Insertion of Hickman catheters. A comparison of cutdown and percutaneous techniques. Am Surg 50:673–6
Gallichio MH, Kahn D, Lempert N, Conti DJ (1994) Placement of a double lumen silastic catheter for hemodialysis access through the cephalic vein. J Am Coll Surg 178:171–172
Wade JC, Newman KA, Schimpff SC, VanEcho DA, Gelber RA, Reed WP, Wiernik PH (1981) Two methods for improved venous access in acute leukemia patients. JAMA 246:140–144
Hsu CC, Kwan GN, Evans-Barns H, Rophael JA, van Driel ML (2016) Venous cutdown versus the Seldinger technique for placement of totally implantable venous access ports. Cochrane Database Syst Rev CD008942
Chuter T, Starker PM (1988) Placement of Hickman-Broviac catheters in the cephalic vein. Surg Gynecol Obstet 166:163–164
Koketsu S, Samesima S, Yoneyama S, Okada T, Tomozawa S, Horikoshi H et al (2010) Outcome of cephalic vein cut-down approach: a safe and feasible approach for totally implantable venous access device placement. Oncol Lett 1:1029–1031
Harish K. Statperson Publications, MedPulse – International Medical Journal, ISSN: 2348–2516, EISSN: 2348–1897, 2015; 2: 34–9
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kumar, V., Sringeri, R. Our Experience of 500 Chemo Port Placements with Cephalic Vein Cut Down Technique—A Saviour for Cancer Treatment. Indian J Surg Oncol (2024). https://doi.org/10.1007/s13193-024-02000-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s13193-024-02000-1