
Abstract
Inflammatory pseudotumour of the testis is a rare but important clinical entity to be recognised by the surgical trainee. We present a case of a 30-year-old gentleman who presented with a hard painless testicular mass. Ultrasound scrotum revealed a diffuse paratesticular swelling arising from the tunica vaginalis with a normal-appearing testis. Germ cell tumour markers were normal. Exploration through an inguinal approach confirmed it to be arising from the tunica vaginalis. Wide excision of the tumour along with a cuff of adherent tunica albuginea was done. Final histopathology revealed a diffuse fibrous pseudotumour of the tunica vaginalis confirming its benign nature.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Testicular swellings are one of the most commonly encountered cases in a surgical trainee’s outpatient posting. The diagnosis is most often straightforward as clinical examination is adequate to diagnose a solid or cystic swelling arising from the testis or its coverings and then investigating accordingly. The trouble arises in solid para testicular tumours that arise from the coverings of the testis. These cannot be reliably distinguished from a testicular mass and are frequently misdiagnosed as testicular tumours leading to needless orchidectomies. Further, as these arise in young men, the social and emotional cost may be significant.
Case Presentation
A 30-year-old gentleman presented to our outpatient clinic with a painless testicular mass and vague history of trauma to the same side 1 month ago. On examination of the right semi-scrotum, there were hard nodular masses palpable superior and posterior to the testis with restricted mobility with respect to the testis.
The skin over the scrotum, the cord structures and contralateral testis were normal.
There were no groin nodes or abdominal masses palpable.
Hernial orifices and bilateral supraclavicular fossae were empty.
Investigations
Germ Cell Tumour Markers
-
Beta Hcg-(0.10mIU/ml)—normal
-
AFP-(1.61 ng/ml)—normal
-
LDH- 639 U/L—normal
USG Scrotum
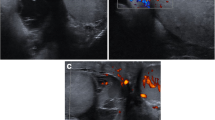
Multiple rounded/oval hypoechoic lesions (11 × 11 mm, 7 × 8 mm, 9 × 5 mm, 21 × 10 mm) were noted within the outer layer of tunica vaginalis indenting the testis with mild internal vascularity-s/o paratesticular tunica vaginalis mass lesions. The testis was normal.
Differential Diagnosis
-
1.
Diffuse variety of fibrous pseudo tumour
-
2.
Adenomatoid tumour
-
3.
Testicular tumour
Treatment
The treatment was inguinal exploration and wide excision of the tumour (Figs. 1, 2, 3, 4, 5, 6 and 7).

Tumour arising from the tunica vaginalis

Tumour adherent to the tunica

Cuff of tunica albuginea excised

Specimen

Final after closure

Microscopy—fibrosis with nodular appearance

Microscopy—paucicellular with hyalinised collagen and scattered lymphocytes
Outcome
The patient went home uneventfully after 2 days. The first follow-up after 3 months was normal, and the patient was asymptomatic.
Histopathology
Nodular fibrous periorchitis.
Macroscopy
-
1.
Para testicular tumour—single grey white 3 × 2.1 × 0.7 cm with nodular external surface (Fig. 1)
-
2.
Cuff of testicular parenchyma—single grey-brown 1.6 × 0.8 × 0.6 cm tissue
Microscopy
-
1.
Multiple nodules composed of hyalinized collagen with intervening scattered lymphocytes and plasma cells. There is no evidence of nuclear atypia, mitotic figures and necrosis (Fig. 6).
-
2.
Normal but slightly reduced spermatogenesis. No evidence of inflammation or neoplasm.
Mild thickening of basement membrane and atrophy of a few tubules were noted.
Discussion
Nodular and fibrous proliferations of the testis are rare benign conditions which mimic testicular cancer [1]. They are known by various monikers such as “inflammatory pseudotumour”, nodular periorchitis, proliferative orchitis, and fibromas of the tunica [2]. The term fibrous pseudotumour of the testis was first introduced by Mostrofi and Price [3]. Nodular and diffuse fibrous proliferations (NDFB) of the tunica vaginalis were proposed by van der Walt et al. as a better unifying term to encompass these inflammatory fibroblastic lesions [4]. Clinically, they are difficult to distinguish from solid testicular tumours, however, in the authors experience, significant nodularity and some amount of mobility with respect to the testis favour these lesions. They are commonly seen in the 3rd and 4th decade and are frequently preceded by trauma and infection reflecting their inflammatory origin. There seem to be two variants—one confined to a single part of the tunica which is easy to identify on ultrasound and another a more diffuse variant which is difficult to identify preoperatively. Irrespective of the type, any paratesticular mass on ultrasound should always alert the clinician of a possibility of a benign tumour. It is always safer to do an inguinal exploration rather than a scrotal one in the rare case of the tumour coming as malignant in the final histology report. In our patient, there was diffuse involvement of the tunica vaginalis with a focal area of adhesion to the tunica albuginea. Hence, we went ahead with a wide excision along with a cuff of tunica albuginea for the margin. The tunica was closed primarily with 3–0 polypropylene suture, and the testis was fixed in its anatomical position to prevent torsion.
Learning Point
Nodular periorchitis is a rare paratesticular tumour common in the 3rd decade of life which mimics malignancy.
The scrotal ultrasound helps to differentiate the testicular vs paratesticular origin of the tumour. Most testicular tumours are malignant whereas paratesticular masses are seldom malignant.The tumour markers in these cases will always be normal further aiding in their management.
Organ preservation is the rule and should be attempted in all cases always through an inguinal approach.
References
Morgan AD (1964) Inflammatory lesions simulating malignancy. Br J Urol 36(Suppl):95–102
Parveen T, Fleischmann J, Petrelli M (1992) Benign fibrous tumor of the tunica vaginalis testis. Arch Pathol Lab Med 116:277–280
Mostofi FK, Price EB (1673) Tumors of the male genital system. In: Mostofi FK, Price EB (eds) Atlas of Tumor Pathology, Second Series. Armed Forces Institute of Pathology, fasciclem, vol 8. Washington DC
Thompson JE, van der Walt JD (1986) Nodular fibrous proliferation (fibrous pseudotumour) of the tunica vaginalis testis. A light, electron microscopic and immunocytochemical study of a case and review of the literature. Histopathology 10:741–748
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Learning point—Paratesticular swellings mimic malignant tumours of the testis and are more likely to be benign. A high index of suspicion goes a long way in preventing unwanted orchidectomies for this benign condition.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Dasu, S., Seripalli, S. & De Padua, M. Pseudotumour of the Testis—Awareness Prevents Mismanagement. Indian J Surg Oncol 15, 405–408 (2024). https://doi.org/10.1007/s13193-024-01904-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13193-024-01904-2