
Abstract
Ossifying fibroma is a benign osteogenic mesenchymal tumor that is classified in the fibro-osseous lesions. Fibro-osseous lesions contain minerals, blood vessels, and giant cells that have the same radiographic and pathologic features but have different clinical behaviors, and were replaced with the normal bone. These lesions include fibrous dysplasia, cemento-osseous dysplasia, and ossifying fibroma. Juvenile ossifying fibroma is a type of uncommon and has invasive behavior, high incidence and occurs in young men, especially in maxilla, and is different from the type of adult in age, location, and clinical behavior and microscopic view. Pathologically, ossifying fibroma is divided into two types of trabecular and psammomatoid. The trabecular type is characterized by the presence of the osteoid trabeculae and the woven bone, and the type of psammomatoid by the presence of round, integrated, and small ossicles that are similar to the components of the psammoma. The purpose of this report is the clinical examination, radiography, pathology, and the treatment of a rare case of ossifying fibroma (trabecular) in mandible in a 7-year-old boy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fibro-osseous lesions of the jaws are referred to as bone lesions which the normal bone is replaced by fibrous connective tissue, including osteoid, mature and immature bone, and have slow growth [1, 2]. The origin of the lesion is from the periodontal ligament [3]. This group of lesions includes fibrous dysplasia, cystic fibrosis, and osteoporosis. Ossifying fibroma is a benign fibro-osseous lesions of the jaws, first described in 1927 by Montgomery [1]. Ossifying fibroma is more limited than fibrous dysplasia and is usually surrounded by a capsule fibrosis [4]. The ossifying fibroma is clinically and pathologically divided into two types of juvenile and conventional [5]. The juvenile type was first used by Johnson in 1952 to describe an invasive type of ossifying fibroma that occurred in craniofacial bone of children [1]. In most cases, the juvenile type involves paranasal sinuses, ethmoid, eyes, and the upper jaw [6] and seldom in the long bones of the body [3] and in the mandible [7] with equal proportions in men and women. This type is more aggressive and higher recurrence [2] and pathologically characterized by cellular fibrous stroma, bone ropes similar to garland, and cementation particles [8], pathologically divided into trabecular and psammomatoid.
The trabecular type is characterized by the presence of the osteoid trabeculae and the woven bone, and the type of psammomat [9].
Its trabecular type occurs in the jaws and its invasion and recurrence is less. In the diagnosis of ossifying fibroma (juvenile type), pathology, MRI, CT SCAN, and clinical findings are helpful [10]. Its treatment is due to excision surgery, and the cause of recurrence is incomplete withdrawal of the lesion, especially in the maxillary regions, and eye [11]. The purpose of the case report is clinical examination, radiography, pathology, and treatment of trabecular ossifying fibroma in the mandible of the 7-year-old boy.
Case Report
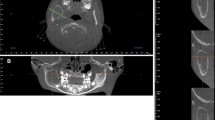
A 7-year-old boy refers to a general physician with complaints of pain in the neck and throat, and has been prescribed with antibiotics for 1 week, but he has not recovered, then he has been referred to the dentist due to oral swelling. The dentist referred him to the department of oral surgery in Babol University of Medical Sciences. In his clinical examination, he had an inflammation in the right side of the mandible that existed from 1 year ago and was gradually enlarged (Fig. 1). In the intraoral examination, the buccal and lingual swellings were noticeable, with an uncertain range of approximately 3 × 4 cm, and are located adjacent to the deciduous teeth and prevent the growth of the tooth germ 4 (Fig. 2). The lesion was not painful at the touch and it has normal mucous. In the panoramic and periapical radiography, lesions with mixed radiolucent and radiopaque views with unlimited border along with displacement of dental buds were observed that prevent the growth of the teeth 4 (Fig. 3a). In CT scan, bone marrow swelling was reported (Fig. 4). Differential diagnosis of of central giant cell granuloma and odontogenic tumors was discussed. The incisional biopsy was performed under anesthesia for the patient. Macroscopically, a few brown tissues in the size of 1.1 × 0.8 × 0/4 were observed. In the microscopic view, bone-shaped neoform tissue containing bone trabeculae with different sizes, peripheral osteoids and osteoblastic rim were evident in a context of connective tissue containing spindly mesenchymal cells. In areas of multi-nucleus giant cells (Fig. 5), the patient was followed up for 4 months by the size of the lesion and the patient complained of pain and the final treatment was done. After transferring the patient to the hospital, 20% lidocaine was injected with epinephrine 80,000/1 in the area, and sulcular incision and releasing in the anterior and posterior lesion were performed and access to the lesion area was achieved. Lower teeth 6 along with the buds of the permanent teeth of 4 and 5 were removed. After the ostectomy, access to the lesion was possible and enucleation and curettage were performed (Figs. 6 and 7a) and the lesion was sent to the pathology. Then, the defect was regenerated with 10-cm3 large orthopedic bone powder and two 2 × 3 and 2 × 2 membranes; the area was sutured with 3 to 3 vikryl. The patient was transferred to a recovery mode with a vigorous state. Radiographic images of the patient were attached after the operation (Figs. 8 and 9). The patient was followed up in 6 months. We did not see recurrence.

Clinical view: swelling is visible in the right region of the mandible

Intra-oral examination of the buccal and lingual enlargement is noteworthy, with an uncertain range of approximately 3 × 4 cm dimensions from the deciduous teeth to the first molar

Periapical and panoramic veiw

In the CT scan, the buccal swelling of mandible is evident

Hematoxylin-eosin staining (× 10) bone-shaped neoform tissue containing different trabecular bone in the context of the connective tissue of the spindly mesenchymal cells

Hematoxylin-eosin staining (× 40): bone-shaped neoform tissue containing different trabecular bone in the context of the connective tissue of the spindly mesenchymal cells

Lesion surgery

Panoramic radiography after surgery

Clinical view after surgery
Discussion
Most benign fibro-osseous lesions of the jaws are asymptomatic and grow slowly. In some cases, an unusual clinical symptom may develop in the lesions and may occur in younger people, especially under 25 years of age [10, 12]. Juvenile ossifying fibroma is a fibro-osseous lesions that occur in the bones of the face [13], as opposed to other lesions, is called invasive fibro-osseous, due to aggressive behavior and a tendency to recurrence [14]. Juvenile ossifying fibroma is a relatively rare fibro-osseous lesions of jaws that occur at age below 15 years. Keles et al. [15], Khan et al.[16], and Anisha [1] reported the lesion occur at the age of 8, 9, and 17 years. In the recent case report, the age of patient was 7 years old.
Juvenile ossifying fibroma occurs in both sexes in equal proportions and has no specific sexual desire. Although some studies have shown that it occurs more often in men [17]. In contrast, Johnson and Change et al. reported that mandibular tumors were more prevalent in girls aged 5–11 or during the second to fourth decades [11, 17]. In the case report, lumbar spasm occurred in the mandible, which prevented the growing of the teeth 4. Although the prevalence of juvenile ossifying fibroma in the upper jaw has been more reported [9]. In the case report of Aboujaoude and Aoun [18] and Kubbi et al. [19], the site of the lesion was in the maxilla, and Khan et al. [16] and Keles et al. [15] reported that in mandible.
The etiology of ossifying fibroma is uncertain, but for which the origin of odontogenic, evolutionary, and in the small number of cases, trauma has been introduced as an etiologic factor [20]. No history of trauma or developmental defect has been reported in the patient in the present case report.
The origin of fibro-osseous lesions is assumed to be due to the ability to produce cement and osteoid, periodontal ligaments [16], so it is expected to occur in the teeth areas [3], which in our case also in the area of the deciduous teeth to the first permanent molar. According to other studies, the skin or mucosa of the lesion is relatively intact [3], which was also the case in the recent report.
In reviewing articles about ossifying fibroma, the main cause of patients’ complaints is often the painless swelling and sometimes the displacement of the involved teeth that our case report is in agreement with the above.
In the radiographic view of various papers, radiolucency with a certain range, and some other mixed radiolucent and radiopaque lesions and some others, radiopaque with a certain range were observed [15]. In the recent case report, a mixed radiolucent-radiopaque lesion with a specific area and location of the teeth was observed. The duration of the lesion was reported from 3 months to 4 years, but it was reported 1 year in recent report. Overall, the radiographic profile of the lesion is related to its evolutionary stage.
There is no specific agreement on the treatment of juvenile ossifying fibroma, and so radical resection, localized conservative excision, or enucleation with curettage is a selective treatment. Slootweg and Muller [20] argue that there is no difference in outcome between cases with limited surgical treatment and those with extensive surgery, and therefore conservative surgery is suggested. On the other hand, Waldron et al. [10] suggested that localized and curettage is the preferred method for preventing recurrence. After a conservative treatment, recurrence has been reported to be between 30 and 58% [21].
In the case of the patient, the recent case of treatment with enucleation and curettage with environmental ostectomy and exiting of the involved teeth was not observed in the follow-up 6 months after the surgery.
Conclusion
Juvenile ossifying fibroma is a benign osteogenic neoplasm that rarely occurs in the mandible and has a high growth potential, degeneration of bone and high recurrence. The rate of rapid growth of the lesion is alarming and clinically malignancy. Therefore, with early diagnosis of lesion, deformity, and inability of children can be prevented and due to the high incidence, long-term follow-up is suggested.
References
Anisha M, Yogesh SH, Murtuza M (2013) Juvenile ossifying fibroma of mandible :a case report. J Maxillofac Oral Surg 12:447–450
Rai SH, Kaur M, Goel S, Prabhat M (2012) Trabecular type of juvenile aggressive ossifying fibroma of the maxilla: report of two cases. Contemp Clin Dent 3:46–50
Sreenivasan BS, Joseph E, Sunil S (2010) Central ossifying fibroma of mandible. Oral Maxillofac Pathol 1:110–114
Commins DJ, Tolley NS, Milford CA (1998) Fibrous dysplasia and ossifying fibroma of the paranasal sinuses. J Laryngol Otol 112:964–968
Mehta D, Clifton N, McClelland L (2006) Paediatric fibro-osseous lesions of the nose and paranasal sinuses. Int J Pediatr Otorhinoaryngol 70:193–199
Dias DK, Kulathilaka D, Kottahachchi M (2008) Juvenile aggressive ossifying fibroma in the jaw bones: 2 case reports. J Maxillofac Oral Surg 7(4):475–480
Bertrand B, Eloy P, Cornelis JP, Gosseye S, Clotuche J, Gilliard C (1993) Juvenile aggressive cemento-ossifying fibroma :a case report and review of the literature. Laryngoscope 103:1385–1390
Dominguete PR, Meyer TN, Alves FA, Bittencourt WS (2008) Juvenile ossifying fibroma of the jaw. Br J Oral Maxillofac Surg 46:480–481
El-Mofly S (2002) Psammomatoid and trabecular juvenile ossifying fibroma of the craniofacial skeleton: two distinct clinicopathologic entities. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 93:296–304
Waldron CA (1997) Fibro osseous lesions of the jaws. J Oral Maxillofac Surg 9:551–562
Johnson LC, Yousefi M, Vinh TN et al (1991) Juvenile active ossifying fibroma: its nature dynamics and origin. Acta Otolaryngol 488:1–40
Williams HK, Mangham C, Speight PM (2000) Juvenile ossifying fibroma. An analysis of eight cases and a comparison with other fibro-osseous lesions. J Oral Pathol Med 29:13–18
MacDonald-Jankowski DS (2004) Fibro osseous lesions of the face and jaws. Clin Radiol 59:11–25
Brannon RB, Flower CB (2001) Benign fibro-osseous lesions: a review of current concepts. Adv Anat Pathol 8:126–143
Keles B, Duran M, Uyar Y et al (2010) Juvenile ossifying fibroma of the mandible: a case report. J Oral Maxillofac Res 1(2):5
Khan M, Kondajji V, Rajguru PA (2017) Case report on juvenile ossifying fibroma of the mandible (2017). J Indian Acad Oral Med Radiol 26(2):213–217
Chang CC, Hung HY, Chang JY et al (2008) Central ossifying fibroma: a clinicopathologic study of 28 cases. J Formos Med Assoc 107:288–294
Aboujaoude S, Aoun G (2016) Juvenile trabecular ossifying fibroma of the maxilla: a case report. Med ARCH 70:470–472
Kubbi R, Kumar N, Reddy V et al (2011) Juvenile ossifying fibroma. J Dent Sci Res 2(2):1–5
Slootweg PJ, Muller H (1990) Juvenile ossifying fibroma: report of four cases. J Craniomaxillofac Surg 18:125–129
Sun G, Chen X, Tang E, Li Z, Li J (2007) Juvenile ossifying fibroma of the maxilla. Int J Oral Maxillofac Surg 36:82–85
Acknowledgements
The author thanks Mr. Mohammadi for the coloring of microscopic slides.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Seifi, S., Foroghi, R., Rayyani, A. et al. Juvenile Trabecular Ossifying Fibroma—a Case Report. Indian J Surg Oncol 9, 260–264 (2018). https://doi.org/10.1007/s13193-018-0759-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13193-018-0759-1