
Abstract
PIK3CA pathway is one of the important signaling pathways in cells, which is involved in cell proliferation, cell survival, motility, and growth. Mutation in PIK3CA gene negatively effects to anti-HER2 therapy in breast cancer patients. PIK3CA gene of HER2-positive breast cancers associated with reduced sensitivity to neoadjuvant therapy. In this study, we assessed the frequency of PIK3CA mutations and influence of PIK3CA mutations on patient survival in a series of HER2-positive breast cancer patients. PIK3CA mutations were assessed by pyrosequencing and next generation sequencing in 107 HER2-positive breast cancer patients of a tertiary Cancer Centre of India from Jan 2012 to Jun 2013 with minimum follow-up of 3 years. We found PIK3CA mutations in 26 tumors (24.2%) of which 5 were in exon 9, 20 were in exon 20, and 1 was in both exon 9 and 20. In exon 9, the mutation c.1634A>G was found in 4 cases and mutation c.1636C>A was found in 2 cases. In exon 20, the mutation c.3140A>G was found in 15 cases and c.3140A>T was found in 6 cases. The outcome between PIK3CA mutated versus PIK3CA wild type was significant showing p value 0.014. Overall survival of mutation and treatment with herceptin, mutation with other chemotherapy treatment in both early breast cancer (EBC), and locally advanced breast cancer (LABC) showed significant p value 0.037 and 0.044 respectively. In conclusion, we identified 24.2% somatic mutation of PIK3CA in HER2-positive breast cancer patients. PIK3CA mutation is significantly associated with ER-positive tumors. The frequency and distribution pattern reported in this study is similar to the global report. Overall survival of PIK3CA mutation is slightly lower but in patients who received herceptin with PIK3CA mutation showed better clinical outcome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the second most common cancer for women in the India. Researches have shown that about 20–30% of the breast cancer patients have HER2 amplification or overexpression that is associated with a more aggressive phenotype and decreased survival [1]. Phosphatidylinositol-4, 5-biphosphate 3-kinase catalytic subunit α (PIK3CA) is the gene located at chromosome 13 which encodes p110α. The gene consists of 20 exons that code for a total of 1068 amino acids. The PIK3CA gene is mutated frequently in common cancers, including carcinoma of breast, prostate, colon and endometrium [2]. Dysregulation of tyrosine kinase receptor (TKR)-phosphatidylinositol 3-kinase (PI3K) signaling pathways is frequent in human cancers. Among the most important molecular events downstream of TKR activation is PI3K activation, which catalyzes the phosphorylation of inositol lipids to phosphatidylinositol-3,4,5-triphosphate which in turn activates the serine/threonine kinase AKT and this regulates several signaling pathways controlling cell survival, apoptosis, proliferation, motility and adhesion [3]. The frequency of PIK3CA mutations in breast cancer cases ranges from 16.4 to 45% [4]. There are 3 mutation “hotspots” in the PIK3CA gene: E542K, E545K at exon 9 (helix domain), and H1047R at exon 20 (kinase domain). The 3 hotspots represent almost 80% of PIK3CA mutation and lead to constitutive PI3K activity by different mechanisms [5]. PIK3CA pathway plays an important role in cancer development and progression. Recent report suggests that PIK3CA pathway activation negatively affect the response to trastuzumab therapy. This observation was described on both retrospective and prospective patient series [6,7,8]. In this study, we assessed the frequency of PIK3CA mutations and influence of PIK3CA mutations on patient survival in a series of HER2-positive breast cancer patients.
Materials and Methods
One hundred seven consecutive cases of HER-2overexpressing/amplified breast cancer cases were studied in tertiary Cancer Centre from Jan 2012 to Jun 2013 with minimum follow-up of 3 years. All patients who came to our institution were informed that their tumor samples might be used for scientific purposes and had the opportunity to decline. This study was approved by the institutional ethics committee (Institutional Review Board, Rajiv Gandhi Cancer Institute).
Genomic DNA was extracted from formalin-fixed paraffin embedded (FFPE) tissue chosen after examination of “H & E”-stained section for maximum viable tumor without pigment, necrosis or other fixation artifact.
Genomic DNA was extracted using QIAamp Mini Kit (Qiagen) according to the manufacturer’s instructions. The extracted DNA was stocked at − 20 °C for future analysis.
Pyrosequencing assay was developed to detect PIK3CA mutations, because pyrosequencing has been shown to be applicable to FFPE and more sensitive than Sanger dideoxy sequencing. The exon 9 PCR primers were: PIK3CA 9-F: 5′-biotin-AACAGCTCAAAGCAATTTCTACACG-3′ and PIK3CA 9-R: 5’-ACCTGTGACTCCATAGAAAATCTTT-3′. The exon 20 PCR primers were: PIK3CA 20-F: 5′-biotin-CAAGAGGCTTTGGAGTATTTCA-3′ and PIK3CA 20-R: 5’-CAATCCATTTTTGTTGTCCA-3′. [9]
PCR was carried out using Pyromark mastermix. PCR conditions were as follows: 95 °C for 15 min; 42 cycles of 95 °C for 20 s, 53 °C for 30 s, and 72 °C for 20 s; and final extension at 72 °C for 5 min. The PCR products were electrophoresed in an agarose gel to confirm successful amplification of the 81-bp (exon 9) and 74 bp (exon 20) products. The PCR products were then prepared with the Vaccum Prep workstation (Pyromark Q24 work station, Qiagen, German) according to following protocol: 10 μl of the amplicon, 1 μl streptavidin sepharose HP beads (GE Healthcare), 40 μl binding buffer, and 29 μl Nuclease free water were mixed for 15 min. The biotinylated amplicons were immobilized onto streptavidin Sepharose beads, washed by 70% ethanol, denatured by 0.2 mol NaOH, and washed by 10 M Tris Acetate using the Vaccum Prep workstation. The amplicons were transferred to a plate containing corresponding sequencing primer in 24.2 μl annealing buffer. For exon 9, the sequencing primer is PIK3CA 9-RS: 5’-CCATAGAAAATCTTTCTCCT-3′; for exon 20, the sequencing primer is PIK3CA 20-RS: 5’-GTTGTCCAGCCACCA-3′ [6]. The plate was heated with samples at 80 °C for 2 min. Pyrosequencing was performed using Pyromark Q24 (Qiagen, German).
Next-generation sequencing (NGS) was done using Ion Ampliseq Cancer Hot Spot Panel V2 (4475346) which targets the 50 oncogenes of tumor suppressor genes. This panel includes 207 pairs of primers in a single tube. For library preparation, we used 10 ng of DNA and Ion Ampliseq Library Kit 2.0 (4480441). Ion Hi-Q One Touch2 (OT2) 200 template kits were used for emulsion PCR and Ion One Touch ES instrument was used for enrichment.
For sequencing, we used Ion PGM Hi-Q Sequencing kit using 316 chip and Ion torrent PGM Machine (Life Technologies). Ion express barcodes and Adapters from Life Technologies were used for sample barcoding during Library Preparation. All protocols were followed as recommended by the manufacturers without modification.
Sequencing data were analyzed with Torrent Suite 5.0.2 (Life Technologies). Analysis for 50 oncogenes and tumor suppressor genes in Torrent Variant Caller by using specific BED files and in Ion Reporter using filters. IGV (Integrative Genomic Viewer) version 2.3 was used to verify the variants called and to identify short reads with potential mispriming events.
Statistical analyses were performed using the statistical packages SPSS (version 23.0 for Windows, IBM SPSS statistics). Relationships between PIK3CA mutation status and clinical, histological, and biological parameters were estimated with the chi-squared test. Survival distributions were estimated with the Kaplan-Meier method.
Result
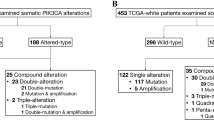
We examined PIK3CA mutation by pyrosequencing (Figs. 1 and 2) and next generation sequencing (Figs. 3 and 4) and mutations were found in 26 tumors (24.2%) of which 5 were in exon 9, 20 were in exon 20 and 1 was in both exon 9 and 20. In exon 9, the mutation c.1634A>G was found in 4 cases and mutation c.1636C>A was found in 2 cases. In exon 20, the mutation c.3140A>G was found in 15 cases and c.3140A>T was found in 6 cases. Out of 107 cases, 65 cases were early breast cancer (EBC) and 42 cases were locally advanced breast cancer (LABC). In cases of EBC, we found 14 (33.3%) cases were PIK3CA mutated and in LABC 12 (18.4%) were PIK3CA mutated Table 1.

PIK3CA exon 9 Pyrograms (antisense strand). a Wild-type exon 9 by the 9-RS1 primer. b The c.1634A>G mutation (arrow) causes a shift in reading frame and results in a new peak at a (arrowhead). c The c.1636C>A mutation (arrow) causes a shift in reading frame and results in a new peak at C (arrowhead)

On analysis by Ion reporter software shows PIK3CA Exon 9 mutation (c.1634A>G) 37.77%

PIK3CA exon 20 pyrograms (antisense strand). (A) Wild-type exon 20. (D) The c.3140A > T mutation (arrow) causes a shift in reading frame and results in a new peak at G (arrowhead). (E) The c.3140A > G mutation (arrow) causes a shift in reading frame and results in a new peak at G (arrowhead)
No significant association between PIK3CA mutations and clinicopathological characteristics was found except ER status. Survival analysis found significantly lower overall survival (p = 0.014; Fig. 5a) in PIK3CA-mutated cases, whereas PIK3CA-mutated cases who received Herceptin chemotherapy showed improved overall survival (p = 0.002; Fig. 5b) than PIK3CA wild type who received herceptin.

On analysis by Ion reporter software shows PIK3CA Exon 20 mutation (c.3140A>G) 35%

Overall survival of PIK3CA mutation
Discussion
PIK3CA is most frequently mutated oncogene in breast cancer. PIK3CA mutations were identified in 26 (24.2%) of 107 HER2-positive breast tumors, in keeping with results of the previous study, showing mutation rate 21.3% [10]. Exons 9 and 20 encode the helical and kinase domains of PIK3CA, respectively. We found a higher frequency of mutation in exon 20 (19.6%) compared to exon 9 (5.6%) similar to the study which shows predominance of exon 20 mutations in breast cancer has been reported [8]. We found one double mutation in exon 9 and exon 20. Double mutations in PIK3CA have been reported previously in gastric and breast cancers [11, 12] and it has been suggested these could indicate multiclonal tumors or a second hit in the alternate allele. In the present study, PIK3CA-mutated tumors showed poorer outcome than PIK3CA wild-type cases (Figure 3) similar to the study of M Cizkova et al. [10]. We found no significant association between PIK3CA mutations and important clinical or pathological features as in several studies [13]. As far as the prognostic significance of PIK3CA mutation is concerned, it is still debatable whether the presence of PIK3CA mutation is associated with good or poor clinical outcome. Some studies reported significantly longer metastasis-free survival and better clinical outcomes in patients with PIK3CA mutations [14, 15], while another series of studies reported lower survival and poor clinical outcomes [16, 17]. Our results state that PIK3CA-mutated cases who received herceptin shows improved clinical outcome in HER2-positive breast cancers than PIK3CA wild-type HER2-positive breast cancer.
Conclusion
In conclusion, we identified 24.2% somatic mutation of PIK3CA in HER2-positive breast cancer patients. PIK3CA mutation is significantly associated with ER-positive tumors. The frequency and distribution pattern reported in this study is similar to the global report. Overall survival of PIK3CA mutation is slightly lower but in patients who received Herceptin with PIK3CA mutation showed better clinical outcome. PIK3CA mutation seems to be potential to be used as an indicator of favorable prognosis with Herceptin. Our preliminary result needs to be confirmed by further study in larger series of patients with longer follow up period.
References
Panigrahi MK, Kumar D, Mehta A, Saikia KK (2017) Outcome of HER2 testing by FISH applying ASCO/CAP 2007 and 2013 guideline in IHC equivocal group of breast cancer: experience at tertiary cancer care centre. South Asian J Cancer 6:45–46. https://doi.org/10.4103/2278-330X.208841
Vanhaesebroeck B, Welham MJ, Kotani K, Stein R, Warne PH, Zvelebil MJ, Higashi K, Volinia S, Downward J, Waterfield MD (1997) P110delta, a novel phosphoinositide 3-kinase in leukocytes. Proc Natl Acad Sci U S A 94:4330–4335
Zhao L, Vogt PK (2008) Class I PI3K in concogenic cellular transformation. Oncogene 27:5486–5496. https://doi.org/10.1038/onc.2008.244.
Mangone FR, Bobrovnitchaia IG, Salaorni S, Manuli E, Nagai MA (2012) PIK3CA exon 20 mutations are associated with poor prognosis in breast cancer patients. Clinics (Sao Paulo) 67:1285–1290. https://doi.org/10.6061/clinics/2012(11)11
Drury SC, Detre S, Leary A, Salter J, Reis-Filho J, Barbashina V, Marchio C, Lopez-Knowles E, Ghazoui Z, Habben K, Arbogast S, Johnston S, Dowsett M (2011) Changes in breast cancer biomarkers in the IGF1R/PI3K pathway in recurrent breast cancer after tamoxifen treatment. Endocr Relat Cancer 18:565–577. https://doi.org/10.1530/ERC-10-0046
Dave B, Migliaccio I, Gutierrez MC, Wu MF, Chamness GC, Wong H, Narasanna A, Chakrabarty A, Hilsenbeck SG, Huang J, Rimawi M, Schiff R, Arteaga C, Osborne CK, Chang JC (2011) Loss of phosphatase and tensin homolog or phosphoinositol-3 kinase activation and response to trastuzumab or lapatinib in human epidermal growth factor receptor 2-overexpressing locally advanced breast cancers. J Clin Oncol 29:166–173. https://doi.org/10.1200/JCO.2009.27.7814
Jensen JD, Knoop A, Laenkholm AV, Grauslund M, Jensen MB, Santoni- Rugiu E, Andersson M, Ewertz M (2012) PIK3CA mutations, PTEN, and pHER2 expression and impact on outcome in HER2-positive early-stage breast cancer patients treated with adjuvant chemotherapy and trastuzumab. Ann Oncol 23:2034–2042. https://doi.org/10.1093/annonc/mdr546
Wang L, Zhang Q, Zhang J, Sun S, Guo H, Jia Z, Wang B, Shao Z, Wang Z, Hu X (2011) PI3K pathway activation results in low efficacy of both trastuzumab and lapatinib. BMC Cancer 11:248. https://doi.org/10.1186/1471-2407-11-248
Nosho K, Kawasaki T, Ohnishi M, Suemoto Y, Kirkner GJ, Zepf D et al (2008) PIK3CA mutation in colorectal Cancer: relationship with genetic and epigenetic alterations. Neoplasia 10(6):534–541
Cizkova M, Dujaric ME, Lehmann-Che J, Scott V, Tembo O, Asselain B, Pierga JY, Marty M, de Cremoux P, Spyratos F, Bieche I (2013) Outcome impact of PIK3CA mutations in HER2-positive breast cancer patients treated with trastuzumab. Br J Cancer 108(9):1807–1809. https://doi.org/10.1038/bjc.2013.164
Saal LH, Holm K, Maurer M, Memeo L, Su T, Wang X, Yu JS, Malmström PO, Mansukhani M, Enoksson J, Hibshoosh H, Borg Å, Parsons R (2005) PIK3CA mutations correlate with hormone receptors, node metastasis, and ERBB2, and are mutually exclusive with PTEN loss in human breast carcinoma. Cancer Res 65:2554–2559. https://doi.org/10.1158/0008-5472-CAN-04-3913
Lee JW, Soung YH, Kim SY, Lee HW, Park WS, Nam SW, Kim SH, Lee JY, Yoo NJ, Lee SH (2005) PIK3CA gene is frequently mutated in breast carcinomas and hepatocellular carcinomas. Oncogene 24:1477–1480. https://doi.org/10.1038/sj.onc.1208304
Michelucci A, Di Cristofano C, Lami A, Collecchi P, Caligo A, Decarli N et al (2009) PIK3CA in breast carcinoma: a mutational analysis of sporadic and hereditary cases. Diagn Mol Pathol 18:200–205. https://doi.org/10.1097/PDM.0b013e31818e5fa4
Loi S, Haibe-Kains B, Majjaj S, Lallemand F, Durbecq V, Larsimont D, Gonzalez-Angulo AM, Pusztai L, Symmans WF, Bardelli A, Ellis P, Tutt ANJ, Gillett CE, Hennessy BT, Mills GB, Phillips WA, Piccart MJ, Speed TP, McArthur GA, Sotiriou C (2010) PIK3CA mutations associated with gene signature of low mTORC1 signaling and better outcomes in estrogen receptor-positive breast cancer. Proc Natl Acad Sci 107:10208–10213
Cizkova M, Susini A, Vacher S, Cizeron-Clairac G, Andrieu C, Driouch K, Fourme E, Lidereau R, Bièche I (2012) PIK3CA mutation impact on survival in breast cancer patients and in ER alpha, PR and ERBB2-based subgroups. Breast Cancer Res 14:R28. https://doi.org/10.1186/bcr3113
Jensen JD, Knoop A, Laenkholm AV, Grauslund M, Jensen MB, Santoni-Rugiu E, Andersson M, Ewertz M (2012) PIK3CA mutations, PTEN, and pHER2 expression and impact on outcome in HER2- positive early-stage breast cancer patients treated with adjuvant chemotherapy and trastuzumab. Ann Oncol 23:2034–2042. https://doi.org/10.1093/annonc/mdr546
Baselga J, Corte’s J, Im SA, Clark E, Ross G, Kiermaier A, Cortés J, Im SA, Clark E, Ross G, Kiermaier A, Swain SM (2014) Biomarker analyses in CLEOPATRA: a phase III, placebo-controlled study of pertuzumab in human epidermal growth factor receptor 2-positive, first-line metastatic breast cancer. J Clin Oncol 32:3753–3761. https://doi.org/10.1200/JCO.2013.54.5384
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed Consent
Informed consent was obtained from the patient.
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
This study approved by the institutional ethics committee (Institutional Review Board, Rajiv Gandhi Cancer Institute). (RGCI ID-406/PA/AMH-09).
Rights and permissions
About this article

Cite this article
Saikia, K.K., Panigrahi, M.K., Mehta, A. et al. Clinico-pathological Features of PIK3CA Mutation in HER2-Positive Breast Cancer of Indian Population. Indian J Surg Oncol 9, 381–386 (2018). https://doi.org/10.1007/s13193-018-0749-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13193-018-0749-3