
Abstract
Fibromatosis covers a broad spectrum of benign fibrous tissue proliferation and is characterized by slow growing, locally infiltrative growth pattern with a high propensity for local recurrence. We report on a case of multicentric fibromatosis originating from the retroperitoneal space and submandibular triangle, in an 18-year-old lady. Computed tomography revealed a retroperitoneal abdominopelvic tumor extending from the left sub-diaphragmatic space to the pelvic inlet which had enveloped the solid viscera in the left upper quadrant with a displaced celiac axis. She also had a recurrent resectable fibromatosis in left submandibular gland. Histopathological evaluation revealed fibromatosis. Preoperatively, Vinblastin-, Methotrexate-, Tamoxifen-based systemic chemotherapy was offered for 12 weeks in an attempt to downsize the mass. An en bloc complete resection of tumor with multi-visceral resection was performed to achieve negative margins and since then, the patient has remained asymptomatic without any signs of tumor recurrence during the 12th month follow-up visit. Complete resection with negative margins is the treatment of choice and majority of the lesions are amenable for surgical resections. Adjuvant therapy using non-steroidal anti-inflammatory agents, tamoxifen, interferon, anti-neoplastic agents, and radiotherapy, either alone or in combination finds application for un-resectable or recurrent cases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fibromatosis has been a disease of curiosity from time immemorial. The term fibromatosis covers a broad spectrum of benign fibrous tissue proliferation, characterized by infiltrative growth pattern and a potential tendency towards local recurrence, but an inability to metastasize [1]. Annual incidence is 2–4 cases per million in the USA [2]. Intra-abdominal fibromatoses are rare but those arising from the retroperitoneum are even rarer [1, 3]. Extraabdominal fibromatosis principally originates from the connective tissue of muscles and the overlying fascia or aponeurosis [4]. These locally infiltrative tumors have a high propensity for adjacent organ involvement and its clinical presentation usually is determined by the organs it invades. The present report outlines a case of symptomatic giant retroperitoneal fibrosis in a young female patient.
Case Report
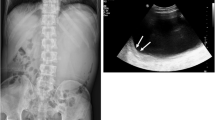
An 18-year-old lady with a past history of surgical excision of left submandibular swelling 4 months prior presented with recurrent swelling in the left submandibular region and progressively worsening of vague abdominal pain and a left sided palpable abdominal mass since 4 months. General physical examination showed 6 × 4 cm firm swelling in the left submandibular region with restricted mobility. Abdominal examination revealed a 20 × 15-cm, non-tender, firm, irregular mass with restricted mobility encompassing the entire abdomen. The upper border of the mass was not clearly defined on palpation. A contrast-enhanced computed tomography (CECT) scan showed a 22 × 33-cm heterogeneously enhancing solid cystic mass occupying the left side of the abdomen with an anterior displacement of the spleen, proximal body of the pancreas with a partial encasement of distal body and tail pancreas, left kidney, and circumferential encasement of splenic artery with celiac axis deviation to the right (Fig. 1). CECT neck showed 6.8 × 6.6-cm mass abutting the hyoid, left body angle of the mandible. A Trucut biopsy of both the mass showed spindle cells, consistent with fibromatosis. In view of large size of the tumor and vascular involvement, she was treated with Vinblastin-, Methotrexate-, Tamoxifen-based chemotherapy for 12 weeks; however, the systemic therapy did not reward the desired downstaging.

CT image showing solid cystic mass extending from the left sub-diaphragmatic region to the superior surface of the urinary bladder with an anterior displacement of the spleen, proximal body of pancreas with a partial encasement of distal body and tail pancreas, left kidney and circumferential encasement of splenic artery with celiac axis deviation to right
Laparotomy revealed a giant abdominopelvic retroperitoneal tumor extending from the left sub-diaphragmatic space to the pelvic inlet with an encasement of the stomach distal pancreas, spleen, and caudally displaced left kidney. An en block excision of tumor along with the adherent greater curvature of the stomach, distal pancreas, spleen, left kidney, and segment of transverse colon was successfully performed (Fig. 2) along with excision of neck lesion. The patient tolerated the procedure well and was discharged subsequently with no significant morbidity. The specimen weighed 4 kg.

a Abdominopelvic retroperitoneal mass involving greater curvature of the stomach, distal body–tail of pancreas, spleen, transverse colon, and left kidney. b En bloc excision of the mass. c Grossing of specimen for histological examination
The histopathology of the specimen demonstrated fibroblastic/myofibroblastic proliferation consistent with fibromatosis. The patient is free of recurrence during the 12th month follow-up period.
Discussion
The term “desmoid” is of Greek origin and means “band-like.” The concept of fibromatosis as a group of similar lesions was first coined by Stout in 1961 [5]. Fibromatosis accounts for 0.03% of all tumors [6]. The fibromatosis can affect both superficial and deep parts of the body. The deep variant involves the abdominal wall, mesentery, retroperitoneum, and mediastinum. In a large study of 189 cases of fibromatosis, only eight (4%) were located in either the retroperitoneum or the mesentery [7]. In another study of 166 desmoid tumors complicating FAP, 83 tumors (50%) were intra-abdominal but only one (0.6%) arose from the retroperitoneum [8]. The pathogenesis of fibromatosis is most likely multifactorial. Generally, these tumors occur more frequently in women, particularly in women of childbearing age. The majority of patients with fibromatosis remain clinically asymptomatic, with little or no focal symptoms until complications due to pressure or invasion occur. These tumors tend to invade or surround muscles, tendons, nerves, vessels, the ureter, and bowel as a result of their infiltrating nature.
Complete surgical resection with negative margins is the treatment of choice, except cases when radical surgery would be mutilating or associated with considerable function loss. Adjuvant therapy using non-steroidal anti-inflammatory drugs, tamoxifen, interferon, anti-neoplastic agents, radiation, and a combination of these, have been reported for cases that are difficult to resect; the exact benefit offered by them is not known due to sparse literature. Radiation therapy is accepted as an effective treatment after incomplete resection. To the best of our knowledge, the tumor described here is the first ever case of retroperitoneal fibromatosis that attained this enormous size.
Conclusion
Fibromatosis is a rare, slow growing, locally aggressive tumor with frequent local recurrences. It invades adjacent organs and anatomic structures causing bizarre symptoms. Complete surgical resection of the tumor with negative margin is the treatment of choice and offers the best prognosis without any adjuvant therapy. Large proportion of these fibromatosis is amenable for complete surgical resection. Unresectable or partially resectable tumors and recurrent tumors have been treated with local radiation and/or adjuvant chemotherapy with variable successes.
References
Weiss SW, Goldblum JR (2001) Fibromatosis. In: Weiss SW, Goldblum JR (eds) Soft tissue tumors. Mosby, St. Louis, pp 309–346
Reitamo JJ, Scheinin TM, Häyry P (1986) The desmoid syndrome. New aspects in the cause, pathogenesis and treatment of the desmoid tumor. Am J Surg 151:230–237
Campanacci M, Enneking WF (1999) Aggressive fibromatosis. In: Campanacci M, Enneking WF (eds) Bone and soft tissue tumors. Springer Verlag, Padova, pp 925–936
Enzinger FM, Weiss SW (2001) Soft tissue tumors, 4th edn. CV Mosby, St. Louis, pp 1472–1475
Stout AP (1961) The fibromatosis. Clin Orthop 19:11–18
Guglielmi G, Cifaratti A, Scalzo G, Magarelli N (2009) Imaging of superficial and deep fibromatosis. Radiol Med 114:1292–1307
Lath C, Khanna PC, Gadewar SB, Agrawal D (2006) Inoperable aggressive mesenteric fibromatosis with ureteric fistula. Case report and literature review. Eur J Radiol 59:117–112
Kabra V, Chaturvedi P, Pathak KA, deSouza LJ (2001) Mesenteric fibromatosis: a report of three cases and literature review. Indian J Cancer 38:133–136
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicting Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Sugoor, P., Gupta, A., Patkar, S. et al. Sporadic Retroperitoneal Fibrosis: a Gentle Giant. Indian J Surg Oncol 9, 71–73 (2018). https://doi.org/10.1007/s13193-017-0710-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13193-017-0710-x