
Abstract
It is conservatively estimated that 5,000 deaths per year and 20,000 injuries in the USA are due to poisonings caused by chemical exposures (e.g., carbon monoxide, cyanide, hydrogen sulfide, phosphides) that are cellular inhibitors. These chemical agents result in mitochondrial inhibition resulting in cardiac arrest and/or shock. These cellular inhibitors have multi-organ effects, but cardiovascular collapse is the primary cause of death marked by hypotension, lactic acidosis, and cardiac arrest. The mitochondria play a central role in cellular metabolism where oxygen consumption through the electron transport system is tightly coupled to ATP production and regulated by metabolic demands. There has been increasing use of human blood cells such as peripheral blood mononuclear cells and platelets, as surrogate markers of mitochondrial function in organs due to acute care illnesses. We demonstrate the clinical applicability of measuring mitochondrial bioenergetic and dynamic function in blood cells obtained from patients with acute poisoning using carbon monoxide poisoning as an illustration of our technique. Our methods have potential application to guide therapy and gauge severity of disease in poisoning related to cellular inhibitors of public health concern.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chemical threat agents are compounds that could be released by a deliberate attack, unintentional release during storage/transportation, or a natural disaster leading to mass casualties. The chemical threat is a wide spectrum that includes chemical warfare agents (Lewisite and sulfur mustard), farming agents (organophosphorus compounds), and cellular inhibitors (cyanide, hydrogen sulfide, and phosphides) that inhibit mitochondrial bioenergetic function. These mitochondrial inhibitors represent a growing threat to international security and safety through potential terrorist use. Despite these growing concerns, funding for developing and testing new antidotes and therapies for these agents are limited. The 2018 federal budget assigns only 3% of its annual budget towards chemical health security and 12% towards biologic health security [1].
Cyanide (CN) is a weak acid that blocks complex IV (CIV or cytochrome c oxidase) resulting in inhibition of mitochondrial respiration as demonstrated in our in vitro study [2]. CN leads to severe hemodynamic instability, metabolic acidosis, seizures, and cardiac arrest [3, 4]. Exposure to CN can occur through a number of ways that represents a public health concern, as only small amounts are required to cause significant toxicity. Other cellular inhibitors include phosphides (PO) and hydrogen sulfide (H2S), which also inhibits CIV respiration resulting in a decrease in ATP production [5,6,7,8]. These agents will also inhibit protein synthesis and leads to the production of reactive oxygen species (ROS), all of which lead to rapid cell death [6, 9]. Cells dependent on oxidative phosphorylation, notably cardiac and neuronal tissues, account for the profound hypotension and refractory shock seen in acute toxicity. The most common cause of death remains multi-organ failure from hypotension and cardiogenic shock. As with cyanide, both H2S and PO toxicity are still associated with significant morbidity and mortality, and further research into early diagnostic tools for cellular mechanisms is needed.
Mitochondrial research in medical science has increased substantially in the recent years as advances reveal a common underpinning with many different disease states that involve the mitochondria [10]. The mitochondria play a central role in cellular metabolism where oxygen consumption through the electron transport system (ETS) is tightly coupled to ATP production and regulated by metabolic demands [11]. The mitochondria are also involved in a variety of important cellular processes that include heat dissipation, production of ROS, and regulation of ion gradients which can be measured with the simultaneous measurement of respirometry and select fluorophores demonstrated with our prior work [12].
Although the effect of cellular inhibitors on bioenergetic function is well established, it remains unclear what effect these inhibitors have on mitochondrial movement, fusion and fission. The mitochondria are sometimes thought of as static organelles; however, they are very dynamic and can adapt to a wide range of environmental stresses with the ability to localize to areas of the cell that require more energy [13]. The mitochondrial dynamic function, in addition to movement, also includes splitting (fission) or merging (fusion) depending on the circumstances of the stress response [14]. For example, when cells undergo growth and division, the mitochondria can undergo fission to populate new cells with adequate amounts of mitochondria. Fission can also occur when there is significant mitochondrial damage that will allow the cell to segregate the damaged portion in response to cellular injury [15, 16]. Mitochondrial fission or fragmentation has been demonstrated in pathological disease and may account for cellular dysfunction and increased ROS production [17, 18]. At this time, the effect of cellular inhibitors on mitochondrial dynamics is not well explored.
There has been increased use of human blood cells such as peripheral blood mononuclear cells (PBMCs), which contains a mixed population of monocytes and lymphocytes, as surrogate markers of mitochondrial function [19]. The measurement of mitochondrial respiration in PBMCs obtained from subjects with acute care illnesses has been explored [2, 20,21,22,23,24,25]. We have also published a study that now combines the ability to measure mitochondrial networking in human blood cells [26]. The objective of this paper is to demonstrate the clinical applicability of measuring both mitochondrial bioenergetic and dynamic function in blood cells obtained from patients with acute poisoning using carbon monoxide exposure as an example of a cellular inhibitor.
Materials and Methods
Study Design
The University of Pennsylvania Institutional Review Board approved this study and informed consent was obtained from the patient or an appropriate surrogate. Samples were obtained from healthy controls and subjects with toxicity from confirmed carbon monoxide poisoning to illustrate the simultaneous measurement of mitochondrial bioenergetic and dynamic function in a clinically relevant time frame. Patients with significant CO poisoning with elevated levels and symptoms were eligible for enrollment upon arrival to the emergency department and within 1 h of presentation. Exclusion criteria for both groups include known malignancy, pregnancy, fire exposure, and history of smoking by chart review and/or clinical assessment.
Mitochondrial Bioenergetics and Dynamics Methods
The following methods were used to measure mitochondrial function (bioenergetics and dynamics) measured in freshly prepared blood cells defined as PBMCs consisting of a mixed population of monocytes/lymphocytes. Mitochondrial bioenergetic function is defined as mitochondrial respiration with simultaneous measurement of hydrogen peroxide (H2O2) with the use of Amplex red. Mitochondrial dynamics is defined as the number of mitochondria, mitochondrial movement, and rates of fusion/fission events. Unless otherwise specified, all reagents were obtained from Sigma-Aldrich and Invitrogen.
-
a.
Human blood cell isolation: All enrolled patients underwent phlebotomy with volumes of 15 ml drawn in K2EDTA tubes, as this has resulted in the best yield and prohibits platelet activation. Blood samples were freshly prepared and analyzed within 1 h of blood draw. We obtained a population of PBMCs from a buffy coat from the plasma using a combination of Ficoll-Paque™ PLUS (GE) and Leucosep tubes (Greiner Bio-one) with centrifugation at room temperature. A cell count and viability with trypan blue exclusion was performed with the Cell Countess II (Invitrogen). We have found that there were no differences in mitochondrial respiration between monocytes and lymphocytes supported by other studies so we used PBMCs [27]. Figure 1 illustrates the workflow once PBMCs were obtained for both microscopy and respirometry.
-
b.
Mitochondrial bioenergetics: High-resolution respirometry was measured at a constant temperature of 37 °C in a high-resolution oxygraph (OROBOROS Instruments), and all cells were suspended in a mitochondrial respiration medium (MiR05). In addition to supporting mitochondrial function, this medium allows for the simultaneous measurement of respiration and the stated fluorophore. We performed a specialized protocol to establish the respiratory capacities at various complexes providing more detailed respiratory activity at complex (C) I, II, III, IV. Our published manuscripts describe these methods in further detail in regard to injections with specific concentrations [12, 25, 28].
-
Routine: Cellular energy turnover at routine activity
-
LEAK: Dissipative component of respiration which is not available for performing biochemical work
-
OXPHOS: The respiratory capacity of mitochondria in the ADP-activated state of oxidative phosphorylation with saturating concentrations of ADP
-
Maximal (Max) respiration: The maximal capacity of cellular respiration with the use of an uncoupler
-
CI, II, III, IV (uncoupled state): CI-linked or NADH-linked respiration or CII-linked of succinate-linked respiration. CIII-linked and CIV respiration are measured with artificial substrates
-
Gp: The mitochondrial glycerophosphate dehydrogenase complex oxidizes glycerophosphate to dihydroxyacetone phosphate and feeds electrons directly to ubiquinone
-
Residual oxygen consumption (ROX): Represents non-mitochondrial oxygen consumption
-
-
c.
Mitochondrial dynamics: We measured mitochondrial dynamics, including mitochondrial number, movement, and rates of fusion/fission events. We have previously described the method to track whole cell mitochondrial motility with PBMCs [26, 29, 30]. Briefly, we measured mitochondrial dynamics in conjunction with respiration using isolating PBMCs plated on a 24-well glass bottom plate (10 k/well) with the use of Cell-Tak (Corning) and centrifugation. Cells will then be stained with MitoTracker Green (ThermoFisher) at a concentration of 100 nM and placed in recording HBSS for imaging. Cells will be imaged using a QImaging QIClick camera attached to Olympus IX70 microscope (Olympus) with an Olympus 100× oil immersion objective lens (Olympus) and Photofluor light source (89 North). ImageJ and MATLAB were used for post-imaging processing to obtain parameters of dynamics as seen in Figs. 2 and 3.

Workflow to perform microscopy and respiration. Flowchart of peripheral blood mononuclear cell (PBMC) isolation for simultaneous data acquisition to obtain mitochondrial dynamics and respiration which can be obtained in 2–3 h which includes PBMC isolation and preparation

Image processing (ImageJ) of a sample image with a PBMC obtained from a patient with CO poisoning showing the PBMC in different stages of processing with the mitochondria fluoresced with MitoTracker Green FM (Thermo Fisher Scientific). a Original image. b Post-convolution and FFT. c Final image after thresholding

Color coded motility of individual mitochondria within PBMCs obtained from a subject with CO-poisoning (a) and a healthy control subject (b) after ImageJ processing as seen in Fig. 2. An increase in the number (blue to red color coding) indicates a greater degree of net movement for each mitochondrion.
Statistical Analysis
Statistics for mitochondrial bioenergetics were calculated by using Graph Pad Prism v.7 (GraphPad Software Inc.). Data were tested for normal distribution with the D’Agostino and Pearson omnibus normality test. Data are presented as mean ± SD if not indicated otherwise. Differences between control and CO groups were assessed using ANOVA in repeated measures. Post hoc pairwise comparisons using Tukey Kramer t tests to adjust for multiple comparisons were used to assess differences between groups and respiratory states. A P value of < 0.05 was considered statistically significant. For data related to mitochondrial dynamics computing the coefficient of determination (R2) of the probability plots, a probability plot was first made by applying the MatLab normplot function to the log values of the net distances traveled by mitochondria in a given cell or cells. X and y values were extracted from the plot, with each data point represented as (xi,yi). The MatLab function normfit gave the mean and standard deviation of the normal distribution best fitting the distribution of logs of net distances. P values comparing log distributions were computed using two-sample Kolmogorov-Smirnov tests (K-S test; kstest2 function in MatLab). This statistical method tests the null hypothesis that two sets of data are taken from the same continuous distribution. We also used unpaired t tests to compare differences in net distance and fusion/fission events (GraphPad Prism 7) [30].
Results
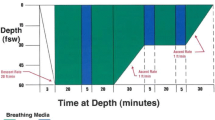
We enrolled a total of eight subjects, including four subjects with confirmed CO poisoning (CO group) and four healthy subjects (control group). The patient characteristics are presented in Table 1. The subjects in the control group were healthy volunteers enrolled as a convenience sample to serve as a comparison group for the measurement of mitochondrial respiration and dynamics. The subjects in the control group were 50% male with a median age of 40 years (interquartile range or IQR, 36 to 51 years). The subjects in the CO group included three men (75%) and one women (25%). The median age of CO subjects enrolled was 54 (IQR, 42 to 61 years). The mean COHb was 29% with a range of 21–35%, and the mean lactate was 3.4 mmol/L with a range of 1.8–4.1 mmol/L in the CO group. Patient clinical characteristics included the following: two (50%) had no medical problems, two had hypertension with one of the two having diabetes. Regarding the source of CO exposure, all four were related to a faulty heat generator. In the CO group, on arrival at the ED, two (50%) experienced syncope, one (25%) had a seizure, two (50%) presented with chest pain/EKG changes, and two (50%) presented with nausea and vomiting. As an outcome index, all four were discharged from the observation unit after undergoing three hyperbaric oxygen dives. All four CO subjects survived hospitalization to discharge.
We compared mitochondrial function in PBMCs obtained from subjects in the CO group and the control group. We compared both respiration and hydrogen peroxide per results in the CO group to the control group. All the units of respiration were measured in pmol O2·s−1·10−6 cells. Table 2 contains both mitochondrial respiration and H2O2 production rates at all the key respiratory states. The following key parameters of respiration were significantly lower in the CO group when compared to the control group, respectively: maximal or Max respiration, uncoupled CI respiration, uncoupled CI + II respiration, and CIV respiration as seen in Fig. 4. We also determined the rate of H2O2 production (as well as superoxide converted to H2O2 with the administration of superoxide dismutase) measured in pmol H2O2·s−1·10−6 cells simultaneously with the measurement of respiration in Fig. 5. The final H2O2 production values were obtained after correction for both background fluorescence and changes in sensitivity over time. There were no differences in H2O2 production in the CO group when compared to the control group (P > 0.9).

Mitochondrial respiration in PBMCs. Cellular mitochondrial respiration obtained in permeabilized PBMCs for the control group and the CO group. This is a typical respiration tracing as it appears during an experiment. Values presented as mean ± SD. *The CO group significantly different at the following respiratory states from the control group (P < 0.001)

ROS production in PBMCs. Measurement of ROS production using the Amplex Red assay. H2O2 levels are measured in the presence of superoxide dismutase to ensure that all superoxide is converted into H2O2. Values presented as mean ± SD. The CO group did not significantly differ from the control group at any of the respiratory states (P > 0.9 for all comparisons)
We also measured mitochondrial dynamics in PMBCs obtained from both the control and CO group to obtain the following parameters: net movement and rates of fusion and fission events. This was performed in a sample of 4–6 PBMCs per subject. The geometric mean of the mitochondrial net distances traveled in PBMCs obtained from the control group was 184.2 ± 23.9 nm, and the CO group was 242 ± 29.5 nm (P < 0.0001). Figure 6 compares the logs of the net distances of the mitochondria within PMBCs between the control and CO groups. The mitochondria in PBMCs obtained from the CO group exhibited greater net movement when compared to the control group.

Mitochondria within PBMCs obtained from CO group exhibit greater net distances traveled when compared to control group. Grouped histograms of net distances traveled by mitochondria in the control group compared to the CO group. Mitochondria are pooled together from 10 to 12 cells from four subjects per group. Histograms are normalized to reflect percentages of objects rather than absolute numbers. There is an overall increase in net movement in the CO group. The net distance traveled in the control group was 184.2 ± 23.9 nm when compared to 242 ± 29.5 nm in the CO group (P < 0.0001). Values presented as mean ± SD
We also measured rates of fusion and fission events in addition to net movement. The percentages of mitochondria that undergo fission and fusion for the control and CO groups are displayed in Fig. 7. Mitochondrial fission and fusion rates of PBMCs obtained from the control group and the CO group. The control group fusion rates (27.2 ± 9.1%) and fission rates (28.4 ± 9.3%) were statistically similar. The CO group fusion rates (35 ± 4.1) and fission rates (36.7 ± 4.2%) were also statistically similar. While the rates for both events were lower in the control group, it was not statistically significant when compared to the CO group (P = 0.1).

Mitochondrial fusion and fission rates for the control group and the CO group. Overall, fusion and fission rates were the same within the control group and within the CO group. While the rates for each of these events appears to be trending higher for the CO group when compared to controls, differences did not achieve statistical significance
Discussion
We utilize acute carbon monoxide poisoning as an example to demonstrate our technique to obtain mitochondrial function in a clinically relevant time frame. Human blood cells have been increasingly used to monitor potential mitochondrial dysfunction that may occur in a variety of acute care illnesses such as poisoning and sepsis [20,21,22,23]. The use of circulating human blood cells such as platelets and PBMCs used for this study offer numerous advantages such as being obtained non-invasively and offers an opportunity for serial measurements [31,32,33].
In this study, we were able to simultaneously obtain both mitochondrial bioenergetic and dynamic function using PBMCs obtained from subjects with confirmed CO poisoning compared to healthy subjects as a comparison group. In the CO group, mitochondrial respiration was significantly lower at key respiratory states that includes complex IV or cytochrome c oxidase respiration with a resultant decrease in other key respiratory states such as Max respiration and uncoupled CI respiration. The finding that CO results in a decrease in CIV respiration with a decrease in other complex activity is a consistent finding in our previous work as well as others [12, 25, 34, 35]. There were no differences in other respiratory states such as uncoupled CII which is most likely related to our sample size where a larger sample size may detect a significant difference [12, 25, 34, 35]. In this study, we also obtained rates of H2O2 production at key respiratory states described for respiration. Similar to our previous study, we found that there was no significant difference in H2O2 production in the CO group when compared to the control group. This is consistent with the fact that CI and CIII are considered the primary sites of ROS production as opposed to CIV [12].
One of the unique aspects of this study is the measurement of mitochondrial dynamics in tandem with bioenergetic function. We advance our prior work where we performed whole cell mitochondrial tracking in adherent cells using fluorescence live imaging [30]. We have leveraged our experience in this area to perform whole cell mitochondrial tracking using PBMCs obtained in both groups. As demonstrated in our previous work, whole cell mitochondrial movement follows a lognormal distribution [26]. As illustrated with our data in this study, it provides a wealth of data on mitochondrial networking in conjunction with the obtained bioenergetic data. One of the findings in this study is a significant increase in net movement in PBMCs obtained from the CO group. This may be related to increased activity of the immune cells related to CO poisoning from increased energetic demand and metabolic activity. Our previous work has demonstrated that PBMCs obtained from patients with septic shock exhibit higher mitochondrial net movement [26]. As we have enrolled subjects in the CO group early in their disease course, this finding may differ in late CO poisoning as is the case in sepsis where immune cells often exhibit anergy [36].
In addition to tracking mitochondrial movement, we can also track rates of mitochondrial fusion and fission events. Mitochondria are dynamic organelles that split and merge in the setting of stress. Mitochondrial fusion allows the mitochondria to combine to cross complete each other when there is mitochondrial injury to preserve oxidative function [13]. Mitochondrial fission occurs when cells divide to populate new cells with an adequate amount of mitochondria. Mitochondrial fission can also occur in cellular injury in order to segregate damaged mitochondria [37]. An interesting finding in our study is an increase in both rates of mitochondrial fusions and fission events compared to the control group, and while not significant, a larger sample size may reveal a significant difference.
The human blood cells serve as a proxy of organ mitochondrial function in other areas of acute care illnesses such as sepsis with little work done in the area of acute poisoning. The use of human blood cells has been described as a “canary in the coal mine” by acting as a predictive biomarker in biological stresses such as sepsis or poisoning [31, 38]. The mitochondria are sensitive to environmental stresses as illustrated in this study, responding with changes in both a functional and structural manner. An attractive feature of directly measuring mitochondrial function is to detect early changes in cellular function before systemic dysfunction occurs leading to multi-organ involvement. We have found in our previous study that the measurement of mitochondrial function may serve as a better reflection of disease severity [25]. Investigators can obtain mitochondrial function in a span of 2–3 h with the potential to influence clinical care. In the case of mitochondrial inhibitors such as CN, H2S, and PO, concentrations are often not available in a meaningful timeframe often taking days for results. While severe cases of poisoning from cellular inhibitors such as cyanide often require immediate action in this first hour of care, our technique could be used as potential gauge of disease severity as well as a model to explore mitochondrial-directed treatment.
An important implication of the described methodology is the impact it may have on poisoning as a whole. While the obvious use for measuring mitochondrial function relates to cellular inhibitors, these methods could apply to other poisonings such as cardioactive medications that cause hypotension or neurotoxin exposure in which mitochondrial dysfunction may occur. While we demonstrated changes in mitochondrial dynamics, it is not clear what effect treatment may have on dynamic function and whether or not measurement of mitochondrial dynamics could be clinically useful in gauging response to treatment or providing predictive value regarding outcome in poisoning.
There are some limitations to consider in this study. One of the limitations is the time the blood cells may be stored to perform these experiments. While our technique can be performed in a timely fashion, fresh blood cells obtained must be used within 4–6 h that makes long-term storage of PBMCs for later analysis problematic. A second limitation of our study is the use of PBMCs as a cell population. PBMCs are composed of monocytes and lymphocytes, and there may be subtle differences in mitochondrial function in response to poisoning. There is at least one study that explores the bioenergetics profile of human blood cells in which there were no bioenergetic differences between monocytes and lymphocytes although there was significantly less CIV subunit I in lymphocytes when compared to monocytes [27]. Future studies may explore differences between the different PBMC types, but in our own experience, we have found that there is additional cost and time required for additional isolation of PBMCs to monocytes and lymphocytes with no demonstrable benefit reported.
Conclusion
This preliminary study is one of the first to investigate the use of human blood cells obtained from subjects to measure both mitochondrial bioenergetic and dynamic function in the area of acute poisoning. We demonstrate that in PBMCs obtained in subjects with acute CO poisoning, there is a decrease in key respiratory states but no significant difference in H2O2 production when compared to controls. We also demonstrate a change in mitochondrial net movement and rates of fission/fusion events between the CO and control group. Our method demonstrates the feasibility of using human blood cells to measure both mitochondrial bioenergetic and dynamic function to better elucidate the relationship between functional and structural aspects of the mitochondria. This has significant application in other areas of poisoning such as agents of bioterrorism where levels are not readily available.
References
Watson C, Watson M, Kirk ST. Federal Funding for health security in FY2018. Health Secur. 2017;4:351–72.
Jang DH, Shofer FS, Weiss SL, Becker LB. Impairment of mitochondrial respiration following ex vivo cyanide exposure in peripheral blood mononuclear cells. Clin Toxicol (Philadelphia, Pa). 2016;54:303–7.
Lee SK, Rhee JS, Yum HS. Cyanide poisoning deaths detected at the national forensic service headquarters in seoul of Korea: a six year survey (2005~2010). Toxicol Res. 2012;28:195–9.
Anseeuw K, Delvau N, Burillo-Putze G, de Iaco F, Geldner G, Holmström P, et al. Cyanide poisoning by fire smoke inhalation: a European expert consensus. Eur J Emerg Med. 2013;20:2–9.
Beauchamp RO Jr, Bus JS, Popp JA, Boreiko CJ, Andjelkovich DA. A critical review of the literature on hydrogen sulfide toxicity. Crit Rev Toxicol. 1984;13:25–97.
Truong DH, Eghbal MA, Hindmarsh W, Roth SH, O'Brien PJ. Molecular mechanisms of hydrogen sulfide toxicity. Drug Metab Rev. 2006;38:733–44.
Dadpour B, Mokhtarpour M, Abdollahi M, Afshari R. An outbreak of aluminium phosphide poisoning in Mashhad, Iran. Arhiv za higijenu rada i toksikologiju. 2016;67:65–6.
Etemadi-Aleagha A, Akhgari M, Iravani FS. Aluminum phosphide poisoning-related deaths in Tehran, Iran, 2006 to 2013. Medicine. 2015;94:e1637.
Sciuto AM, Wong BJ, Martens ME, Hoard-Fruchey H, Perkins MW. Phosphine toxicity: a story of disrupted mitochondrial metabolism. Ann N Y Acad Sci. 2016;1374:41–51.
Picard M, Wallace DC, Burelle Y. The rise of mitochondria in medicine. Mitochondrion. 2016;30:105–16.
Brown GC. Control of respiration and ATP synthesis in mammalian mitochondria and cells. Biochem J. 1992;284(Pt 1):1–13.
Jang DH, Khatri UG, Shortal BP, et al. Alterations in mitochondrial respiration and reactive oxygen species in patients poisoned with carbon monoxide treated with hyperbaric oxygen. Intensive Care Med Exp. 2018;6:4. https://doi.org/10.1186/s40635-018-0169-2.
Benard G, Bellance N, James D, Parrone P, Fernandez H, Letellier T, et al. Mitochondrial bioenergetics and structural network organization. J Cell Sci. 2007;120:838–48.
Frederick RL, Shaw JM. Moving mitochondria: establishing distribution of an essential organelle. Traffic. 2007;8:1668–75.
Giedt RJ, Pfeiffer DR, Matzavinos A, Kao CY, Alevriadou BR. Mitochondrial dynamics and motility inside living vascular endothelial cells: role of bioenergetics. Ann Biomed Eng. 2012;40:1903–16.
Giedt RJ, Yang C, Zweier JL, Matzavinos A, Alevriadou BR. Mitochondrial fission in endothelial cells after simulated ischemia/reperfusion: role of nitric oxide and reactive oxygen species. Free Radic Biol Med. 2012;52:348–56.
Balog J, Mehta SL, Vemuganti R. Mitochondrial fission and fusion in secondary brain damage after CNS insults. J Cereb Blood Flow Metab. 2016;36:2022–33.
Rosdah AA, Holien JK, Delbridge LM, Dusting GJ, Lim SY. Mitochondrial fission - a drug target for cytoprotection or cytodestruction? Pharmacol Res Perspect. 2016;4:e00235.
Jang DH, Greenwood JC, Spyres MB, Eckmann DM. Measurement of mitochondrial respiration and motility in acute care: sepsis, trauma, and poisoning. J Intensive Care Med. 2017;32:86–94.
Callahan LA, Supinski GS. Sepsis induces diaphragm electron transport chain dysfunction and protein depletion. Am J Respir Crit Care Med. 2005;172:861–8.
d'Avila JC, Santiago AP, Amancio RT, Galina A, Oliveira MF, Bozza FA. Sepsis induces brain mitochondrial dysfunction. Crit Care Med. 2008;36:1925–32.
Japiassu AM, Santiago AP, d'Avila JC, et al. Bioenergetic failure of human peripheral blood monocytes in patients with septic shock is mediated by reduced F1Fo adenosine-5′-triphosphate synthase activity. Crit Care Med. 2011;39:1056–63.
Karamercan MA, Weiss SL, Villarroel JP, et al. Can peripheral blood mononuclear cells be used as a proxy for mitochondrial dysfunction in vital organs during hemorrhagic shock and resuscitation? Shock (Augusta, Ga). 2013;40:476–84.
Villarroel JP, Guan Y, Werlin E, Selak MA, Becker LB, Sims CA. Hemorrhagic shock and resuscitation are associated with peripheral blood mononuclear cell mitochondrial dysfunction and immunosuppression. J Trauma Acute Care Surg. 2013;75:24–31.
Jang DH, Kelly M, Hardy K, Lambert DS, Shofer FS, Eckmann DM. A preliminary study in the alterations of mitochondrial respiration in patients with carbon monoxide poisoning measured in blood cells. Clin Toxicol (Philadelphia, Pa). 2017;55:579–84.
Jang DH, Greenwood JC, Owiredu S, Ranganathan A, Eckmann DM. Mitochondrial networking in human blood cells with application in acute care illnesses. Mitochondrion. 2017. https://doi.org/10.1016/j.mito.2017.12.009.
Chacko BK, Kramer PA, Ravi S, Johnson MS, Hardy RW, Ballinger SW, et al. Methods for defining distinct bioenergetic profiles in platelets, lymphocytes, monocytes, and neutrophils, and the oxidative burst from human blood. Lab Investig. 2013;93:690–700.
Jang DH, Seeger SC, Grady ME, Shofer FS, Eckmann DM. Mitochondrial dynamics and respiration within cells with increased open pore cytoskeletal meshes. Biol Open. 2017;6:1831–9.
Barel O, Christine VMM, Ben-Zeev B, et al. Deleterious variants in TRAK1 disrupt mitochondrial movement and cause fatal encephalopathy. Brain. 2017;140:568–81.
Kandel J, Chou P, Eckmann DM. Automated detection of whole-cell mitochondrial motility and its dependence on cytoarchitectural integrity. Biotechnol Bioeng. 2015;112:1395–405.
Chacko BK, Kramer PA, Ravi S, Benavides GA, Mitchell T, Dranka BP, et al. The bioenergetic health index: a new concept in mitochondrial translational research. Clin Sci (London, England: 1979). 2014;127:367–73.
Kramer PA, Chacko BK, Ravi S, Johnson MS, Mitchell T, Darley-Usmar VM. Bioenergetics and the oxidative burst: protocols for the isolation and evaluation of human leukocytes and platelets. J Vis Exp. 2014;85:e51301. https://doi.org/10.3791/51301.
Ravi S, Mitchell T, Kramer P, Chacko B, Darley-Usmar VM. Mitochondria in monocytes and macrophages-implications for translational and basic research. Int J Biochem Cell Biol. 2014;53:202–7.
Garrabou G, Inoriza JM, Moren C, et al. Mitochondrial injury in human acute carbon monoxide poisoning: the effect of oxygen treatment. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2011;29:32–51.
Miro O, Alonso JR, Lopez S, Beato A, Casademont J, Cardellach F. Ex vivo analysis of mitochondrial function in patients attended in an emergency department due to carbon monoxide poisoning. Med Clin (Barc). 2004;122:401–6.
Piel S, Ehinger JK, Elmer E, Hansson MJ. Metformin induces lactate production in peripheral blood mononuclear cells and platelets through specific mitochondrial complex I inhibition. Acta Physiol (Oxford, England). 2015;213:171–80.
Reddy PH, Reddy TP, Manczak M, Calkins MJ, Shirendeb U, Mao P. Dynamin-related protein 1 and mitochondrial fragmentation in neurodegenerative diseases. Brain Res Rev. 2011;67:103–18.
Kramer PA, Chacko BK, George DJ, Zhi D, Wei CC, Dell’Italia LJ, et al. Decreased bioenergetic health index in monocytes isolated from the pericardial fluid and blood of post-operative cardiac surgery patients. Biosci Rep. 2015;35(4):e00237. https://doi.org/10.1042/BSR20150161.
Funding
This work was funded by NIH grant K08HL136858 and the American College of Medical Toxicology (ACMT)-Medical Toxicology Foundation Research and Teaching Award (DJ) and Office of Naval Research grants N000141612100 and N000141712643 (DME).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The University of Pennsylvania Institutional Review Board approved this study and informed consent was obtained from the patient or an appropriate surrogate.
Conflicts of Interest
None.
Rights and permissions
About this article

Cite this article
Jang, D.H., Khatri, U.G., Mudan, A. et al. Translational Application of Measuring Mitochondrial Functions in Blood Cells Obtained from Patients with Acute Poisoning. J. Med. Toxicol. 14, 144–151 (2018). https://doi.org/10.1007/s13181-018-0656-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13181-018-0656-6