
Abstract
Purpose
To identify differences between three-phase bone scan and SPECT/CT (TBS) and WBC SPECT/CT (WS) and compare diagnostic accuracies of each modality in patients with suspicious post-traumatic osteomyelitis (OM).
Methods
Twenty-one patients with suspicious post-traumatic OM were enrolled. All patients performed TBS and WS within 1 week. Foci of MDP and WBC accumulation were divided into three categories: bone (OM), soft tissue (soft tissue inflammation; STI), negative for inflammation (NI). Confirmative diagnosis was made upon operative pathology or long-term clinical follow-up.
Results
Of 21 patients, four OM, eight STI, nine NI were finally diagnosed. TBS diagnosis was correct in three of four positive cases and nine of 17 negative cases. Sensitivity, specificity, accuracy, positive predictive value (PPV), negative predictive value (NPV) of TBS were 75 %, 52.9 %, 57.1 %, 27.3 %, 90 %. WS diagnosis was correct in two of four positive cases and 17 of 17 negative cases. Sensitivity, specificity, accuracy, PPV, NPV were 50 %, 100 %, 81.0 %, 100 %, 89.5 %. Twelve of 21 cases showed agreement between TBS and WS. TBS misdiagnosed nine cases (six STI and two NI as eight OM; one OM as one STI), while WS misdiagnosed four cases (two OM as two STI; two STI as two NI). Combining results from TBS and WS led to better diagnostic accuracy (91.7 %) than either TBS or WS alone.
Conclusion
TBS and WS showed moderate agreement in assessment of clinically suspected post-traumatic OM. WS better evaluated inflammation than TBS. WS tended to underestimate inflammation whereas TBS tended to overestimate inflammation. Combining TBS and WS enhanced diagnostic accuracy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteomyelitis (OM) is one of the most serious complications of surgery or trauma. Despite advances in operative and antibiotic therapy, OM often fails to respond to treatment, thus leading to a chronic clinical course [1]. Post-traumatic OM is defined as the bone infection resulting from an open fracture or surgical procedure involving the bone. The incidence of bone infection after open fracture is 2 to 16 %, depending on the severity of the trauma and type of therapy [2]. Many cases of acute bone infection progress to chronic infection, and accurate diagnosis is essential to determine treatment [1, 3].
Computed tomography (CT) detects cortical bone changes in chronic OM, however this modality is not good at detecting the early stage of bone infection. Magnetic resonance imaging (MRI) shows high sensitivity (82–100 %) and specificity (75–96 %) in the early stage of OM, but its abilities can be hampered by prosthesis insertion or trauma [4–8].
Nuclear imaging using 99mTc-methylene diphosphonate (MDP) or white blood cell (WBC) has played an important role in the evaluation of bone infection since altered bone metabolism precedes anatomical changes. Three-phase bone scan and WBC scan have been performed to diagnose OM. 99mTc-MDP three-phase bone scan has high sensitivity (82 %) but quite low specificity (25 %) for detecting bone infection [9] because localized uptake on the bone scan does not indicate active infection itself but increased osteoblastic activity. WBC scan with 99mTc-hexamethylpropyleneamine oxime (HMPAO)-labeled WBC shows higher specificity (60–68 %) than three-phase bone scan [9]. The results are derived from autologous WBCs representing inflammation. However, both image modalities are limited by poor imaging resolution. Single-photon emission computed tomography/computed tomography (SPECT/CT) is a recently introduced hybrid imaging modality, which offers anatomical information to overcome the inherent scintigraphic shortcoming of poor imaging resolution. Bone SPECT/CT and WBC SPECT/CT (WS) enhance diagnostic accuracy as they combine metabolic and anatomical data.
Several studies have demonstrated the usefulness of 99mTc-MDP bone SPECT/CT or 99mTc-HMPAO-labeled WS for differential diagnosis of bone and joint infection [10–14]. Bone SPECT/CT improves diagnostic evaluation of OM by excluding false positives and equivocal findings [10]. WS improves localization of lesions in cases of suspected OM [11, 12] and prosthesis infection [13]. Some authors have emphasized that dual imaging methods using both bone SPECT/CT and WS can improve the diagnosis of diabetic foot infection [14].
To our knowledge, no study has directly compared the results of three-phase bone scan and SPECT/CT (TBS) and WS. In this study, we figured out how different they are from each other and compared diagnostic accuracies of each imaging modality for patients with clinically suspicious post-traumatic OM.
Materials and Methods
Patients
Subjects were retrospectively enrolled in this study among those who underwent both 99mTc-MDP TBS and 99mTc-HMPAO-labeled WS between February 2014 and October 2015. Data were collected from symptomatic patients with a history of trauma who were clinically suspicious of OM and for whom the time interval between TBS and WS was 1 week or less. Twenty-one patients were included in this study. All had clinical symptoms of OM (mostly pain, swelling and redness with or without fever), and their abnormal laboratory data (elevated WBC count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP)) was reviewed.
Imaging Protocol
Bone SPECT/CT was performed after 99mTc-MDP three-phase bone scan. At first, blood flow, blood pool, and delayed bone images were obtained. After administration of 99mTc-MDP, ranging from 1110 MBq to 1295 MBq, a blood flow image was sequentially obtained for 60 s, immediately followed by a blood pool image. Blood pool image acquisition was completed within 10 min of tracer injection. The delayed image was acquired 3 to 4 h after injection. Continuous whole body bone scanning was performed with a dual-head gamma camera (ECAM, Siemens) and a low-energy high-resolution collimator in a 256 × 1024 matrix. Bone SPECT/CT was performed on the suspicious area. SPECT images were taken with dual-head gamma cameras (Symbia T16, Siemens) equipped with a low-energy high-resolution collimator in continuous step-and-shoot mode (64 steps over 180°, 15 s/step). The CT component used a vendor-provided CARE dose with a tube current of 20–345 mA; tube voltage of 80, 110, and 130 kV; and 5-mm thickness. The SPECT images were reconstructed by 3D-OSEM iterative image reconstruction into a 256 × 256 matrix.
Thirty-five mL of venous blood was drawn into a 50-mL plastic syringe for WBC scan. WBCs were isolated and labeled with 99mTc-HMPAO at an average labeling yield of 80 %. The radiolabeled WBCs were reinjected into the patient. The injected dose of 99mTc-HMPAO-labeled WBC ranged from 1295 to 1480 MBq. The whole body planar image was obtained 4 h after intravenous administration with a dual-head gamma camera (ECAM, Siemens) and a low-energy high-resolution collimator in a 256 × 1024 matrix. WS was performed on the suspicious area immediately after planar imaging was done. The SPECT and CT components and image reconstruction of the WS were conducted in the same way as the bone SPECT/CT, with the exception of the SPECT scan speed. Due to the relatively low radioactivity count, a WBC SPECT scan speed of 25 s/step was used instead.
Final Diagnosis
Final diagnosis was made upon either pathology from surgery or clinical follow-up by an experienced orthopedic surgeon over at least 5 months. In specimens, OM was confirmed when inflammatory cells were found in bone tissue. If inflammation was absent in bone tissue but present in surrounding soft tissue, then soft tissue inflammation (STI) was diagnosed. Final diagnosis criteria by clinical follow-up is as follow: OM, if clinical symptoms did not subside or inflammatory markers including WBC, ESR, CRP remained elevated after antibiotic administration for 4 weeks; and STI, if clinical symptoms subsided or inflammatory markers decreased after antibiotic administration for less than 4 weeks; and negative for inflammation (NI), if clinical symptoms improved without any medical or surgical intervention during the follow-up period.
Image Analysis
Two nuclear medicine physicians reviewed both TBS and WS images independently. When the two physicians did not give concordant ratings, they reached consensus by discussion. The TBS was considered to indicate OM if focal increased perfusion, blood pool, and corresponding bone uptake was present; and STI if increased perfusion and blood pool was present without increased bone uptake; and NI if increased perfusion, blood pool, and bone uptake was absent. Focal accumulation on the WBC scan was considered to indicate OM if accumulation was present in the bone of suspicion; and STI if WBC accumulation was confined to soft tissue; and NI if no WBC accumulation was detected. The hybrid SPECT/CT images were then assessed to correctly localize both the bone and WBC uptake. When combining the results from TBS and WS, only matched results from two imaging modalities were included in the analysis. Those concordant results were compared with final diagnosis.
Statistical Analysis
Agreement between the TBS and WS diagnoses was evaluated with the kappa value. Agreement between each imaging modality and the final diagnosis was also evaluated. Diagnostic accuracies for OM of TBS, WS, and combining both imaging modalities were calculated and compared. The associations between the imaging findings and abnormal laboratory data (increased WBC count, ESR, and CRP) were also assessed by Kruskal-Wallis test. Analyses were conducted with SPSS software version 21.0. A P value < 0.05 was considered statistically significant.
Results
Patient’s Characteristics
Twenty-one patients (14 males and seven females; 51.9 ± 18.1 years) with suspicious post-traumatic OM were enrolled. Clinical features, final diagnoses, findings from the TBS and WS, and concordance between two imagings are summarized in Table 1. Mean symptom duration of patients was 4.9 ± 3.9 months, ranging from 0.5 to 13 months. Most patients presented a chronic clinical course. Fourteen patients had symptom duration for more than 3 months, whereas only three patients had symptom duration for less than a month. Of the 21 patients, 17 had a traumatic fracture history and ten had a metallic prosthesis implanted. The most common site was tibia (n = 11), followed by ankle (n = 4), femur (n = 3), pelvis (n = 2), and foot (n = 1).
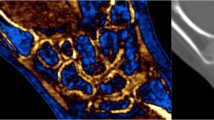
Final diagnosis was four patients with OM, eight patients with STI, and nine patients who were NI by surgery (nine cases) or clinical follow-up (12 cases). The time interval between TBS study day and surgical intervention was 17.7 ± 16.6 days (range, 3 to 57 days). All four OM cases were confirmed by surgery. Representative histopathologic images of OM and STI are presented in Fig. 1. Negative results included postoperative change, healing fracture, nonunion, and hematoma.

Representative surgical histopathologic images (Hematoxylin and eosin stain, 1 : 200) of OM (a, case No. 4 in Table 1) and STI (b, case No. 11 in Table 1). Plasma cell infiltrations and fibrosis are seen in foot bone marrow, indicative of chronic OM (a). Abundant lymphoid and plasma cell infiltrations are seen in soft tissue of calf, indicative of chronic STI (b)
Comparison of TBS and WS
A comparison of the results from the TBS and WS is presented in Table 2. The time interval between TBS and WS was 3.3 ± 1.3 days (range, 2 to 7 days). The two imaging modalities showed agreement in 12 of 21 cases (kappa value of 0.406). In 12 concordant cases, correct diagnoses were made in 11 cases, thus yielding high diagnostic accuracy (91.7 %, 11/12) of combining TBS and WS.
There were nine discordant cases. In five of the nine cases, the TBS diagnosis was OM and the WS diagnosis was STI, while the final diagnoses were four cases of STI and one case of OM. Figure 2 illustrates a case for which the final diagnosis was STI. In this case, increased bone uptake was detected in the TBS but no WBC uptake was seen in the corresponding bone portion. WBC accumulation is limited to adjacent soft tissue in WS. Figure 3 illustrates a case for which the final diagnosis was OM. Hyperperfusion, increased blood pool, and increased bone uptake at the site of the fracture was noted in the TBS, but subtle WBC accumulation was seen only in the surrounding soft tissue in WS. In this case, there was no definite WBC uptake involving the bone, even though bone infection was confirmed by surgical pathology.

A 70-year-old male (case No. 8 in Table 1) who had a fracture in his right tibia midshaft underwent bone graft surgery, TBS (a–d) and WS (e and f). Hyperperfusion (arrow) and increased blood pool activity (arrow) was noted on perfusion (a) and blood pool (b) images. On the bone SPECT/CT images, increased uptake (arrows) was noted in the grafted bone (c, sagittal image; d, coronal image). On the WS images, WBC uptake (arrow) was confined to the adjacent soft tissue (e, sagittal image), and no WBC uptake (arrow) was seen in the corresponding grafted bone (f, coronal image). STI was confirmed by clinical follow-up

A 33-year-old male (case No. 3 in Table 1) who had a fracture in the right tibia midshaft underwent TBS and WS. Increased blood flow (arrow) and blood pool activity (arrow) was detected on the perfusion (a) and blood pool (b) phase of the 3-phase bone scan and matched increased bone uptake (arrow) was seen at the fracture site on the bone SPECT/CT image (c, coronal view). On the WS image, only subtle WBC uptake (arrows) was seen in the surrounding soft tissue (d, WBC scan image; e, coronal WS image). OM was confirmed by surgery
For the remaining four discordant cases, the TBS diagnosis was OM and the WS diagnosis was negative, while the final diagnosis was two cases of STI and two negative results. Figure 4 illustrates a case with a final diagnosis of STI. In this case, the TBS resulted in a false positive, which focal increased bone uptake confined to the lateral malleolar cortex was seemingly nonspecific.

An 80-year-old male (case No. 12 in Table 1) who had trauma on his right ankle 3 months previously underwent TBS and WS. Increased blood flow (arrow) and blood pool activity (arrow) was noted on the perfusion (a) and blood pool phase (b) of the 3-phase bone scan and matched increased bone uptake (arrow) was seen on the right lateral malleolus on the bone SPECT/CT image (c, coronal view). On the WS image, no WBC uptake was noted in the corresponding right lateral malleolus (d, WBC scan image; e, coronal WS image). STI was confirmed by surgery
Table 3 compares the predictive diagnosis by TBS and WS with the final diagnosis. Of the 21 cases, the TBS showed agreement with the final diagnosis in 12 cases (kappa value of 0.390). For the nine discordant cases, TBS overestimated inflammation in eight cases and underestimated inflammation in one case. With regards to OM, the TBS diagnosis was correct in three of four positive cases and nine of 17 negative cases. Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) for OM were 75 % (3/4), 52.9 % (9/17), 57.1 % (12/21), 27.3 % (3/11), and 90 % (9/10), respectively. The predictive diagnosis by WS was in concordance with the final diagnosis in 17 of 21 cases (kappa value of 0.689). The WS underestimated inflammation in the four discordant cases. With regards to OM, the WS diagnosis was correct in two of four positive cases and 17 of 17 negative cases. Sensitivity, specificity, accuracy, PPV, and NPV were 50 % (2/4), 100 % (17/17), 81.0 % (17/21), 100 % (2/2), and 89.5 % (17/19), respectively.
We also assessed the association between the diagnosis predicted by the TBS or WS and clinical laboratory data, including WBC count, CRP, and ESR by Kruskal-Wallis test. Groups (OM, STI, and NI) divided by either TBS (P value of WBC, CRP, ESR: 0.355, 0.840, 0.834, respectively) or WS (P value of WBC, CRP, ESR: 0.199, 0.138, 0.258, respectively) did not show any significant differences in terms of inflammatory marker values.
Discussion
99mTc-MDP three-phase bone scan and 99mTc-HMPAO-labeled WBC scan are known to be helpful in the diagnosis of OM. In general, 99mTc-MDP three-phase bone scan is very sensitive at detecting bone infection; however, its specificity depends on the circumstances. The specificity of 99mTc-MDP three-phase bone scan is high (>90 %) in normal bone but much lower (35 %) when the bony structures are complicated by trauma or surgery [15]. The 99mTc-HMPAO-labeled WBC scan has similar sensitivity to 99mTc-MDP three-phase bone scan for bone infection but greater specificity (up to 90 %) even in post-traumatic and postoperative cases, especially in the peripheral skeleton [15]. However, specificity is poor in the central skeleton due to physiologic bone marrow uptake; it is also poor in leukopenic patients. Previous studies reported that combining the 99mTc-MDP three-phase bone scan with 99mTc-HMPAO-labeled WBC scan improved diagnostic accuracy [16, 17]. In the present study, combining TBS and WS (91.7 %, 11/12) led to better diagnostic accuracy in 12 cases of concordant findings than either TBS (57.1 %) or WS (81.0 %) alone. This is probably due to different mechanisms for the MDP uptake and WBC accumulation so that the two imaging modalities are complementary to each other. That may contributed to diagnostic accuracy enhancement.
Adding SPECT/CT modality to planar scan enhanced diagnostic performance by providing exact lesion location. Likewise, TBS and WS showed better diagnostic accuracies over planar bone and WBC scan [13, 14]. Both TBS and WS are powerful imaging modalities to assess bone infection but they are different in that they use different tracers. MDP uptake reflects the status of perfusion and osteoblastic activity, while WBC accumulation reflects leukocytes activity itself. However, studies trying to figure out how different those two hybrid imaging results are from each other is scarce to date. In this study, we tried to find out differences between them. TBS and WS showed moderate concordance rate with a kappa value of 0.406 in evaluation of clinically suspected post-traumatic OM.
Figure 2 explains how WS more accurately assessed the extent of inflammation than did TBS, a result consistent with previous studies [12, 14]. Differentiating STI from OM is very important because the treatment strategy varies according to the extent of infection [18]. Antibiotic therapy alone can be adequate for management of STI, whereas surgical intervention, such as prosthesis removal, is required for bone involvement [19–21]. Figure 3 demonstrates how chronic low grade inflammation can be better evaluated by TBS than WS. Because only one case out of 21 is the case such as Fig. 3, it is hard to generalize that point. However, this case explains TBS can better assess OM than WS in certain clinical settings. In this case, the infected bone was proceeding through the chronic clinical course and therefore had low grade inflammation. In chronic OM, inflammation is usually low-grade, with insufficient 99mTc-granulocyte count to be visualized on WBC scintigraphy [22]. Bone infection can also be disguised by the protective membrane formation of bacteria [23] and by administration of antibiotics [24].
Figure 4 presents a false positive of TBS and a false negative of WS. Increased radiotracer accumulation on bone scintigraphy reflects increased rate of bone turnover, which is also a finding of many different conditions other than OM [25]. The false positive bone uptake may be the result of reactive osteitis due to immediate STI. However, the WS yielded a false negative result in this patient. Increased WBC accumulation was not observed, even when actual inflammation was present in the soft tissue. This patient showed a chronic clinical course, which may explain the false negative. Chronic inflammation is different from acute inflammation with respect to the types and proportion of leukocytes involved, chemotactic factors, vascularity, and permeability. In the chronic phase of inflammation, leukocytic infiltration becomes mononuclear, thus diminishing the role of neutrophils [26]. In this situation, the WBC count at the site of inflammation is much lower than in cases of acute inflammation. Vascularity and permeability of the affected vessels is much decreased as well. Altogether, these conditions increase the risk that chronic inflammation will go unnoticed on WBC scintigraphy.
In the two discordant cases that were negative at the final diagnosis, the WS diagnosis was correct, showing no WBC accumulation, while the TBS misleadingly showed an increased blood pool and matched increased bone uptake. Like the case of Fig. 4, the increased bone uptake was nonspecific. Likewise, hyperemia and abnormal blood pool can also occur in noninfected conditions [27]. In these two cases, persistent bone remodeling by prosthesis insertion at the fracture site was mimicking bone infection on the TBS. In this study, TBS resulted in all eight false positives. Possible causes of false positive TBS result include post-traumatic, postsurgical changes, hypertrophic non-union, and reactive osteitis. The fact that MDP uptake on TBS is not an indicator of infection but a secondary change to infection contributed to the false positives. In half of those eight false positive cases, WS correctly diagnosed STI. Among the other half, WS correctly diagnosed NI in two cases whereas WS resulted in two false negatives when final diagnosis was STI.
In the current study, WS was superior to TBS for the assessment of suspected bone infection. Most incorrect predictions by TBS were overestimation of inflammation, which appears to be caused by nonspecific findings due to post-traumatic, postsurgical, and reactive changes. This nonspecific uptake contributed to low specificity, accuracy, and PPV for OM. In contrast, all erroneous diagnoses by WS were underestimation of inflammation, probably owing to chronic inflammatory conditions, which lowered the specificity for OM. Overall, undergoing both TBS and WS is suggested to more accurately diagnose the post-traumatic OM. If the two imaging results are concordant, then the imaging diagnosis is very likely to be correct. Otherwise, overestimation of TBS and underestimation of WS can be helpful to reach correct diagnosis.
MRI is a widely used modality to assess bone infection and can be useful at detecting OM because it can distinguish inflammatory changes of the bone marrow and adjacent soft tissue [4]. However, representing MRI features of bone infection, such as bone marrow edema on T2-weighted images and gadolinium contrast enhancement indicating hyperemia, are sometimes nonspecific and can lower diagnostic accuracy with false positive results, especially in post-traumatic [5] and postoperative settings [6]. Fibrovascular scar tissue of the bone marrow and soft tissue in the reparative phase can also resemble the signal changes and contrast enhancement of inflammation [7]. For patients with prosthetic devices implanted, metal artifact can be a hindrance to MRI evaluation because metallic implants distort the signal [8]. Because of these restrictions, MRI is limited in its ability to evaluate post-traumatic OM. Specificity and sensitivity of MRI to diagnose chronic post-traumatic OM were reported to be 63 % and 100 %, respectively [6]. In contrast, specificity and sensitivity were 50–70 % and 80–90 %, respectively, for TBS; and 80–100 % and 80–100 %, respectively, for WS in the evaluation of post-traumatic OM [28]. Although TBS is not better than MRI in the post-traumatic OM assessment, there are some advantages of TBS over MRI. MRI is a regional imaging study scanning only one part of the body but TBS scans the whole body so that it can detect other fever foci or other fracture sites than the suspected area. More importantly, MRI is limited by the artifact signal produced by the metal implant [1, 8]. In contrast, TBS is hardly affected by the metal implant.
This study had several limitations. First, the study was retrospective, so the timing of imaging might not have been optimal in some cases. Most patients showed a chronic clinical course, and a few had antibiotic treatment before imaging, which could have complicated the imaging findings. Second, post-traumatic condition can be a source of potential bias that TBS inherently exhibits the increased uptake in traumatic site. Third, the number of enrolled cases was relatively small, so subdividing patients by imaging diagnosis produced samples sizes that were too small to show statistical significance. This may limit the clinical usefulness of our study. Further prospective studies with a larger cohort are needed to confirm our analysis.
Conclusions
TBS and WS showed moderate agreement in the assessment of clinically suspected post-traumatic OM. WS was better able to evaluate lesions than TBS. WS was also more accurate when evaluating the extent of inflammation, as it was better at distinguishing OM from STI. Overall, TBS tended to overestimate inflammation while WS tended to underestimate inflammation. These results suggest that performing both TBS and WS can lead to better diagnosis of bone infection.
References
Kaim AH, Gross T, von Schulthess GK. Imaging of chronic posttraumatic osteomyelitis. Eur Radiol. 2002;12:1193–202.
Roesgen M, Hierholzer G, Hax PM. Post-traumatic osteomyelitis. Pathophysiology and management. Arch Orthop Trauma Surg. 1989;108:1–9.
Buhne KH, Bohndorf K. Imaging of posttraumatic osteomyelitis. Semin Musculoskelet Radiol. 2004;8:199–204.
Pineda C, Espinosa R, Pena A. Radiographic imaging in osteomyelitis: the role of plain radiography, computed tomography, ultrasonography, magnetic resonance imaging, and scintigraphy. Semin Plast Surg. 2009;23:80–9.
Sanders TG, Medynski MA, Feller JF, Lawhorn KW. Bone contusion patterns of the knee at MR imaging: footprint of the mechanism of injury. Radiographics. 2000;20:135–51.
Ledermann HP, Kaim A, Bongartz G, Steinbrich W. Pitfalls and limitations of magnetic resonance imaging in chronic posttraumatic osteomyelitis. Eur Radiol. 2000;10:1815–23.
Deely DM, Schweitzer ME. MR imaging of bone marrow disorders. Radiol Clin North Am. 1997;35:193–212.
Kaim A, Ledermann HP, Bongartz G, Messmer P, Muller-Brand J, Steinbrich W. Chronic post-traumatic osteomyelitis of the lower extremity: comparison of magnetic resonance imaging and combined bone scintigraphy/immunoscintigraphy with radiolabelled monoclonal antigranulocyte antibodies. Skeletal Radiol. 2000;29:378–86.
Hatzenbuehler J, Pulling TJ. Diagnosis and management of osteomyelitis. Am Fam Physician. 2011;84:1027–33.
Horger M, Eschmann SM, Pfannenberg C, Storek D, Vonthein R, Claussen CD, et al. Added value of SPECT/CT in patients suspected of having bone infection: preliminary results. Arch Orthop Trauma Surg. 2007;127:211–21.
Filippi L, Schillaci O. Usefulness of hybrid SPECT/CT in 99mTc-HMPAO-labeled leukocyte scintigraphy for bone and joint infections. J Nucl Med. 2006;47:1908–13.
Filippi L, Uccioli L, Giurato L, Schillaci O. Diabetic foot infection: usefulness of SPECT/CT for 99mTc-HMPAO-labeled leukocyte imaging. J Nucl Med. 2009;50:1042–6.
Kim HO, Na SJ, Oh SJ, Jung BS, Lee SH, Chang JS, et al. Usefulness of adding SPECT/CT to 99mTc-hexamethylpropylene amine oxime (HMPAO)-labeled leukocyte imaging for diagnosing prosthetic joint infections. J Comput Assist Tomogr. 2014;38:313–9.
Heiba SI, Kolker D, Mocherla B, Kapoor K, Jiang M, Son H, et al. The optimized evaluation of diabetic foot infection by dual isotope SPECT/CT imaging protocol. J Foot Ankle Surg. 2010;49:529–36.
Gross T, Kaim AH, Regazzoni P, Widmer AF. Current concepts in posttraumatic osteomyelitis: a diagnostic challenge with new imaging options. J Trauma. 2002;52:1210–9.
Palestro CJ, Kipper SL, Weiland FL, Love C, Tomas MB. Osteomyelitis: diagnosis with (99m)Tc-labeled antigranulocyte antibodies compared with diagnosis with (111)In-labeled leukocytes--initial experience. Radiology. 2002;223:758–64.
Poirier JY, Garin E, Derrien C, Devillers A, Moisan A, Bourguet P, et al. Diagnosis of osteomyelitis in the diabetic foot with a 99mTc-HMPAO leucocyte scintigraphy combined with a 99mTc-MDP bone scintigraphy. Diabetes Metab. 2002;28:485–90.
Hernigou P, Flouzat-Lachianette CH, Jalil R, Uirassu Batista S, Guissou I, Poignard A. Treatment of infected hip arthroplasty. Open Orthop J. 2010;4:126–31.
Moyad TF, Thornhill T, Estok D. Evaluation and management of the infected total hip and knee. Orthopedics. 2008;31:581–8.
Toms AD, Mandalia V, Haigh R, Hopwood B. The management of patients with painful total knee replacement. J Bone Joint Surg (Br). 2009;91:143–50.
Leone JM, Hanssen AD. Management of infection at the site of a total knee arthroplasty. Instr Course Lect. 2006;55:449–61.
Peters AM. The utility of [99mTc]HMPAO-leukocytes for imaging infection. Semin Nucl Med. 1994;24:110–27.
Evans RP, Nelson CL, Bowen WR, Kleve MG, Hickmon SG. Visualization of bacterial glycocalyx with a scanning electron microscope. Clin Orthop Relat Res. 1998;347:243–9.
Datz FL, Thorne DA. Effect of antibiotic therapy on the sensitivity of indium-111-labeled leukocyte scans. J Nucl Med. 1986;27:1849–53.
Love C, Din AS, Tomas MB, Kalapparambath TP, Palestro CJ. Radionuclide bone imaging: an illustrative review. Radiographics. 2003;23:341–58.
Feghali CA, Wright TM. Cytokines in acute and chronic inflammation. Front Biosci. 1997;2:12–26.
Larikka MJ, Ahonen AK, Junila JA, Niemela O, Hamalainen MM, Syrjala HP. Extended combined 99mTc-white blood cell and bone imaging improves the diagnostic accuracy in the detection of hip replacement infections. Eur J Nucl Med. 2001;28:288–93.
Govaert GA, Glaudemans AW. Nuclear medicine imaging of posttraumatic osteomyelitis. Eur J Trauma Emerg Surg. 2016. doi:10.1007/s00068-016-0647-8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Chanwoo Kim, Soo Jin Lee, Ji Young Kim, Kyu Tae Hwang, and Yun Young Choi declare that they have no conflict of interest.
Ethical Statement
The study was approved by an institutional review board or equivalent and has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All subjects in the study gave written informed consent or the institutional review board waived the need to obtain informed consent.
Rights and permissions
About this article

Cite this article
Kim, C., Lee, S.J., Kim, J.Y. et al. Comparative Analysis of 99mTc-MDP Three-Phase Bone Scan with SPECT/CT and 99mTc-HMPAO-Labeled WBC SPECT/CT in the Differential Diagnosis of Clinically Suspicious Post-traumatic Osteomyelitis. Nucl Med Mol Imaging 51, 40–48 (2017). https://doi.org/10.1007/s13139-016-0441-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13139-016-0441-x