
Abstract
Objectives
Negative automatic thoughts about self (NATS) are a central feature of depression, and have been linked cross-sectionally and prospectively with its symptoms. This suggests negative self-referent thoughts are both a by-product and accelerant of depression. Accordingly, reducing NATS is worthwhile given its downstream effects on depression. Very few trials have examined the efficacy of mindfulness-based interventions in remediating this important outcome. Even fewer still have examined the efficacy of low-intensity, online, and scalable interventions in reductions of NATS. We conducted a large randomized controlled trial examining the efficacy of a brief (4-week), self-guided, online mindfulness and self-compassion intervention (Mind-OP) in reducing the frequency and severity of NATS.
Methods
We recruited general population participants using a popular crowdsourcing website (CloudResearch) and randomized them to the Mind-OP intervention condition (n = 221) or the Active Control condition (n = 221), and examined pre- to post-change in their NATS on the Cognitive Triad Inventory – Self Subscale.
Results
Both intention-to-treat (ITT) and per-protocol mixed-linear model (MLM) analyses demonstrated that participants randomized to the Mind-OP condition reported significantly greater reductions in NATS, with ITT analyses demonstrating small-medium effects (Cohen’s d = 0.38) compared to those randomized to the active control condition at post-treatment.
Conclusions
Results suggest brief, self-guided mindfulness-focused interventions demonstrate promising effects in reducing NATS, which has important implications given their downstream consequences.
Preregistration
The hypotheses of the current study were not preregistered. The trial on whose data the current study builds was preregistered on AsPredicted (#18806) on 2019–01-22.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Depression is a highly prevalent condition, with approximately 3–4% of the global population meeting diagnostic criteria for the disorder (Santomauro et al., 2021; GBD 2019 Diseases and Injuries Collaborators 2020). A common feature of depression is the preponderance of negative self-referent thoughts during acute phases of the condition. Traditional forms of cognitive behavioral therapy (CBT) are efficacious in reducing negative automatic thoughts about self (NATS) and depression symptoms (Dozois et al., 2009; Stefan et al., 2019). However, much more research is needed to establish the efficacy of third-wave CBT and acceptance-based techniques in reducing NATS. Further, given the high demand for efficacious depression interventions around the world (Richards, 2011), and the dynamic relationship between NATS and depression symptoms, scalable and easy-to-use interventions designed to lessen negative self-thoughts are warranted.
Depression is a syndrome in which sad mood and/or anhedonia (i.e., loss of pleasure in usually pleasurable activities) have persisted for most days over a 2-week period or longer (American Psychiatric Association, 2013). These central features are usually accompanied by several other cognitive (e.g., poor concentration), affective (e.g., feelings of worthlessness), and somatic (e.g., disruptions in sleep and appetite) symptoms, all contributing to significant distress or impairment in daily functioning. Higher levels of NATS are a central feature of Aaron Beck’s cognitive theory of depression (Chahar Mahali et al., 2020). Beck noted that patients with depression displayed a distinct cognitive profile dominated by negative thoughts. These negative thoughts were observed to have three themes: they represented thoughts about self (e.g., “I am no good”; “I am unlovable”), the world (e.g., “the world is a harsh place”), and future (e.g., “I will never amount to anything”; “My future is bleak”; Beck, 2008). Beck described this tripartite nature of depressive thought content as the cognitive triad. Since then, negative automatic thoughts about self, world, and future, otherwise known as the negativity hypothesis, became one of the foundations for the cognitive theory and therapy for depression (Clark et al., 1999). There is a large body of research supporting the negativity hypothesis in depression. Researchers have consistently demonstrated that NATS is linearly and positively associated with depressive symptoms, so that with higher symptoms there is a higher likelihood of experiencing NATS (Blatt et al., 1982; Dobson & Shaw, 1986; Dudek et al., 2007; Lamberton & Oei, 2008; Oei et al., 2010). This close relationship of depressive symptoms and NATS seems to be near universal, with supportive evidence from several countries and continents across the globe (Beshai et al., 2012, 2016; Chahar Mahali et al., 2020).
Depression and its associated symptoms likely represent an ancient evolutionary system. This system is activated after experiencing substantial loss or failure, and is designed to preserve resources and reduce likelihood of competition with others perceived as dominant in the social hierarchy during a period of critically low or depleted personal resources (Clark et al., 1999; Gilbert, 2000). Negative automatic self-referent thoughts are likely one of the mechanisms through which depression sufferers preserve energy. NATS appear linked with increased withdrawal and avoidance (Holahan et al., 2005), and reduced competition through perceived low self-efficacy and low outcome expectancy (Saltzman & Holahan, 2002). That is, NATS are both the signatures and engines of the evolutionary depression system.
This suggests depression symptoms have a feed-forward relationship with NATS, with NATS and depression likely having a bidirectional influence over one another. While NATS is a biproduct of depression symptoms, the presence and severity of NATS go on to exacerbate depression symptoms, which then go on to fuel additional NATS in a vicious cycle. Evidence from some prospective studies support this feed-forward relationship between negative self-referent cognitions and depression (Choon et al., 2015; Flouri & Panourgia, 2014; Hjemdal et al., 2013).
CBT has been found to be efficacious in reducing NATS (Beevers & Miller, 2005). Classic forms of CBT guide patients to dismantle the unhelpful and correct the biased nature of negative self-cognitions. By contrast, mindfulness and compassion-based therapies, often called “third wave” CBT, help patients change their relationship with negative cognitions (Kang et al., 2013). Mindfulness is defined as the capacity to pay purposeful attention to present-moment experiences with acceptance, curiosity, and balance (Kabat-Zinn, 2003). Compassion is a broad construct, and is often defined as the awareness of and concern for suffering, understanding the universality of suffering, tolerance of negative emotions elicited by suffering, and motivation to alleviate such suffering (Strauss et al., 2016). Self-compassion is therefore the awareness of suffering within oneself, and the motivation to alleviate it (Neff, 2003a, 2003b). Neff’s conceptualization of self-compassion as a response to suffering comprised of three subpolarities: self-kindness (as opposed to self-criticism); common humanity (as opposed to isolation); and mindfulness of painful experiences (balance between over-indulging or avoiding suffering; Neff, 2003a). Mindfulness-based interventions (MBIs) directly cultivate the capacity for mindfulness, which instigates a cascade of other protective and pathology-reversing processes (Shapiro et al., 2006). Within mindfulness and compassion frameworks, thoughts, like other experiences, are passing events that need not implicate or be fused with self (Grabovac et al., 2011). Accordingly, patients using MBIs learn to become aware of NATS and accept them as they are, without becoming reactive or resistant to them. Evidence supports this theoretical relationship between mindfulness and NATS; dispositional forms of mindfulness are associated with reduced frequency of and ability to tolerate NATS (Frewen et al., 2008). Further, the inverse relationship between dispositional mindfulness and NATS appears to hold among patients formally meeting diagnostic criteria for depression (Ayhan & Kavak Budak, 2021). Finally, evidence suggests people attending mindfulness meditation sessions experience reductions in NATS (Mehdipour et al., 2017; Tarkhan, 2018). Accordingly, while few, results of extant studies demonstrate NATS are meaningfully associated with and may be remediable by mindfulness.
Similarly, researchers have demonstrated a consistent relationship between self-compassion and negative thoughts. For example, researchers found indirect relationships between self-compassion—as mediator or moderator—in the relationship between NATS and depression symptoms (Mantzios & Wilson, 2014; Pedro et al., 2019). Self-compassion has also been demonstrated to moderate the effects of negative automatic thoughts on depression symptoms among participants with a history of childhood maltreatment (Hou et al., 2021). To the authors’ knowledge, only one study examined the effects of a self-compassion intervention on NATS, and found promising effects among a group of Japanese participants (Arimitsu, 2016).
Given the ubiquity of depression, combined with the fact that NATS are a by-product and accelerant of symptoms, making readily available scalable interventions that are effective in reducing such deleterious outcomes on a population level is a priority (Holmes et al., 2018). Unfortunately, and despite the effectiveness of psychological interventions in reducing distress, there are major barriers that prevent people from accessing them. Logistical (e.g., excessive wait times; geographical challenges; time constraints) and financial (i.e., cost of treatment) factors are chief among the barriers preventing access to effective mental health care (Moroz et al., 2020). Brief, self-guided, low-cost, online interventions are proliferating, and are able to address the identified barriers to access, and accordingly are a promising approach to addressing the ballooning mental health crisis (Barak et al., 2008; Schueller & Parks, 2014).
These scalable interventions are especially attractive in light of the high rates of subthreshold depression among members of the general population (Zhang et al., 2023), which is also associated with elevated NATS (Beshai et al., 2012). Indeed NATS appears to be a transdiagnostic factor implicated in depression, and anxiety, and perceived stress (Beshai et al., 2017; Yapan et al., 2022). Given such high rates and increased risk, easily accessible, low-intensity treatment options for depression and NATS are worthwhile for ethical and practical reasons (Bennett-Levy et al., 2010). Thankfully, self-guided and internet-based mindfulness and self-compassion interventions are proliferating. These self-guided interventions are particularly promising, as they have demonstrated effectiveness in reducing mild to moderate symptoms of depression and other forms of distress (Beshai et al., 2016; Taylor et al., 2021). Unfortunately, several trials examining the effectiveness of self-guided treatments have employed small samples and/or an inadequate control condition. Further, many self-guided mindfulness and compassion interventions do not take advantage of the synergistic effects of these concepts and their applications when they are explicitly combined in the same intervention (Beshai et al., 2020). For these and other reasons, researchers developed Mind-OP, a brief, online self-guided mindfulness and self-compassion intervention for milder distress (Beshai et al., 2020). Mind-OP demonstrated effectiveness in reducing distress (e.g., anxiety, stress), and in improving mindfulness and self-compassion skills over a 6-week period among a large general adult sample. Mind-OP was developed to meet the ever growing need to improve access to evidence-based treatments for the management of symptoms of mild psychological distress (Holmes et al., 2018). Further, the intervention was explicitly developed to be very brief (approximately 2 hr, not including practice), scalable, flexible, and most importantly low-cost, which addresses a number of accessibility barriers (Patel et al., 2011). Finally, the treatment was also developed in line with the stepped-care approach, which suggests providing brief, less intensive interventions for patients reporting milder forms of distress (Bower & Gilbody, 2005).
To the authors’ knowledge, there are currently no published trials examining a mindfulness and self-compassion-based self-guided intervention specifically in reducing negative thoughts. In the present trial, we analyzed previously unpublished data from Beshai et al. (2020) to determine the efficacy of Mind-OP in specifically reducing NATS. To this goal, we randomized 442 community participants recruited from a popular online crowdsourcing website to receive Mind-OP or an active control condition (watching relaxing nature videos and completing assessments). We hypothesized that participants randomized to receive the self-guided mindfulness and self-compassion intervention, Mind-OP, would report significantly greater reductions in NATS at the end of the trial compared to those randomized to receive relaxing nature videos in the control condition.
Method
Participants
Data for the present trial represent a subset of unpublished data from a larger, now published trial examining the effectiveness of Mind-OP in reducing mild distress (Beshai et al., 2020). The original trial hypotheses were pre-registered (AsPredicted #18806) prior to carrying out any research activities; however, we did not pre-register current study goals or hypotheses.
A total of 606 participants were recruited from CloudResearch (Litman et al., 2017), an Amazon Mechanical Turk extension. CloudResearch gives researchers access to recruiting thousands of unique participants and has been used extensively in several behavioral and clinical studies (e.g., Beshai et al., 2017; Chandler & Shapiro, 2016). Data collection for the trial was completed between April and September of 2019. Participants were compensated for their participation in each of the weekly trial tasks. The highest compensation amount was presented in the final week of assessment (Week 6 or post-intervention). Initially, participants were compensated with $1.50/week (total of US$9); however, and given the initially high attrition rates, we increased payment to $2.50/week (total of US$15.00). This rate is commensurate with compensation schedules in most crowdsourcing studies (Chandler & Shapiro, 2016).
Consistent with previous self-guided mindfulness or self-compassion intervention trials, we expected small-medium effects (Spijkerman et al., 2016). Given the active control element, sample size estimates were based on a small effect between groups and across time (f = 0.10). G*Power (Faul et al., 2009) suggested a total sample size of 164 participants to detect a small effect with power of 0.80. We anticipated 50% eligibility and 50% attrition based on patterns observed in similar studies (Beshai et al., 2020; Cuijpers et al., 2011; Karyotaki et al., 2015). Accordingly, we planned to recruit 700 participants (for an anticipated 175 protocol-adherent participants). We stopped recruitment after 606 participants given budgetary constraints.
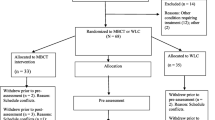
Inclusionary criteria included (a) residing in an English-speaking country (i.e., Canada, USA, UK, New Zealand, and Australia), (b) being 18 years of age or older, and (c) reporting at least mild distress defined as a score of eight or higher on depression (PHQ-9; Kroenke et al., 2001) or anxiety (GAD-7; Spitzer et al., 2006) scales, and/or 14 or higher on the perceived stress scale (PSS; Cohen et al., 1983). A total of 606 participants were initially recruited. Of these, 442 participants (female n = 200; 43.9%) were eligible and provided consent to be part of the trial, passed baseline attention checks, and were randomized into the Mind-OP intervention condition (n = 221; Mage = 36.26; 46.3% female) or active control condition (n = 221; Mage = 34.16; 41.5% female). The CONSORT participant flow diagram is presented in Fig. 1. As can be observed, n = 159 (approximately 36% of the total randomized) participants completed the program/control condition tasks, were attentive, and engaged (defined as passing the included knowledge questions, described below) with study tasks and measures. This subset of participants was included in the per-protocol MLM. We summarized pertinent demographic information of randomized participants included in the final analyses in Table 1.

CONSORT participant flow diagram
Procedures
The present trial used a randomized, active controlled, parallel group, repeated measures design over a 6-week study period. All study tasks were hosted on Qualtrics, and distributed to potential participants through CloudResearch (Litman et al., 2017). CloudResearch workers interested in participating in the trial were guided to click a Qualtrics survey link upon which the informed consent process and the full battery of trial pre-intervention measures, including the Cognitive Triad Inventory – Self subscale (CTI-S), were hosted (see Beshai et al., 2020, for a full list of measures). Eligibility was determined by a trained, unblinded research assistant for each participant providing consent. Those consenting, and meeting eligibility requirements and passing initial attention checks were provided with trial materials for Week 1 within a maximum of 7 days of receiving their pre-intervention responses. In this trial, we used a 1:1 randomization sequence using random case selection using SPSS. Materials (e.g., modules for Mind-OP participants; nature videos for active control participants) for each week of the 6-week trial period were sent to participants via email on Fridays, with one email reminder sent each Wednesday. Participants completing all modules or active control tasks received the online post-intervention questionnaire package, including the CTS-S, on Week 6 of the trial. Only participants completing intervention modules and/or active control tasks assigned in previous trial weeks were provided with subsequent modules/tasks. Those not engaging with all weekly tasks were considered to exhibit low protocol adherence.
Mind-OP Intervention Condition
Mind-OP is a brief, online program designed to cultivate mindfulness and self-compassion. Mind-OP is a completely self-guided, 4-week program consisting of four modules administered at a pace of one module per week. The modules consist of psychoeducational videos, guided audio meditations, as well as several goal-setting and motivational interviewing inspired exercises. The modules contain videos that focus on several aspects of mindfulness and self-compassion, in addition to providing opportunities for participants to engage with meditations and other exercises embedded within each module. All videos in the modules are superimposed with calming music and are narrated by the first author. At the end of each module, participants were directed to do brief reflection exercises wherein they were directed to (a) schedule a date and time to practice meditation between modules, (b) rate how confident they are that they will practice on a scale of 1 to 10, and (c) answer open-ended questions to describe any factors that may help or hinder their practice. These activities are based on motivational interviewing exercises (Friederichs et al., 2015; Webber et al., 2008) and are intended to enhance decisional control and encourage consistent meditation practice. Mind-OP module content and session breakdown is presented in Table 2.
Active Control Condition
Participants randomized to the active control condition were guided to watch one video per week, for the 4-week duration paralleling the intervention. Each video featured 40 high-quality, peaceful stock nature images that were presented in a slideshow, and each image appeared on screen for 6 s. Accordingly, the videos were 4 min long and were superimposed onto the music soundtrack featured in the guided meditations of the Mind-OP condition. Watching high-quality nature videos, in which participants’ engagement was monitored and recorded, was deemed a robust active control condition. This is because evidence suggests that being in nature, or even watching videos wherein nature is featured, appears to have anxiolytic properties (Mayer et al., 2009). To ensure participants were engaged in their weekly tasks, control participants were shown two words during each of the four 4-min nature videos. These words (e.g., “Psychology” or “Attention”) were in small, white font, and appeared in the corners of the screen for only a few seconds at random intervals throughout each video.
Measures
Cognitive Triad Inventory – Self Subscale — The Cognitive Triad Inventory (CTI; Beckham et al., 1986) is a 36-item, three-subscale self-report measure designed to assess frequency and intensity of negative automatic thoughts related to self, world, and future. Six items of the 36-item CTI are non-scored, filler items. Accordingly, each of the three subscales assess negative cognitions using 10 items. The 10-item CTI Self Subscale (CTI-S) measures frequency and intensity of negative automatic thoughts related to self (e.g., “I am a failure”; “I am guilty of a great many things”) using a 7-point Likert scale (from 1 or totally disagree, to 7 or totally agree). Scores on the CTI-S can range from 10 to 70. After reversing positively valanced items (e.g., “I can do a lot of things well.”), higher scores on the CTI-S are indicative of greater presence of negative automatic thoughts related to self. Beckham et al. (1986) found CTI subscales have high internal consistencies (ranging from 0.81 for other subscale to 0.93 for world subscale), and that scores were strongly correlated with scores on the Beck Depression Inventory (Beck et al., 1996). Beshai et al. (2012) found CTI-S possessed high internal reliability (α = 0.81), and was strongly correlated with scores on the Centre for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977; r = 0.67) and the Automatic Thoughts Questionnaire (ATQ; Hollon & Kendall, 1980; r = 0.79). In the current sample, pre-intervention Cronbach’s alpha and McDonald’s omega coefficients for the CTI-S were α = 0.92 and ω = 0.93, respectively.
We also administered several other questionnaires, including Patient Health Questionnaire – 9 (PHQ-9; Kroenke et al., 2001); Generalized Anxiety Disorder Scale – 7 (GAD-7; Spitzer et al., 2006); The Perceived Stress Scale (PSS; Cohen et al., 1983); Five Facet Mindfulness Questionnaire – 15 (FFMQ-15; Gu et al., 2016); and the Self-Compassion Scale – Short Form (SCS-SF; Raes et al., 2011). For a full list of measures and their description, please see Beshai et al. (2020).
Knowledge Questions, Attentiveness, and Fidelity Checks
To ensure participants were engaging with and paying attention to weekly tasks, they were asked to respond to two multiple choice or True/False knowledge questions related to the content of the intervention (Mind-OP condition) or nature videos (active control condition) at the end of each week (Moncher & Prinz, 1991). For example, after Module 1, participants in the Mind-OP intervention condition were asked “Which of the following is NOT a quality of mindful attention?” and provided with four answer choices to which there is one correct response. Participants in the control condition were asked questions related to the words that were embedded in each of the nature videos (see description of the active control condition). For example, participants who completed the first week of the active control condition were asked “Which of the following words was shown on the side of the screen during the video?” and provided with four answer choices to which there was one correct response. In total, participants in either condition were asked eight knowledge questions throughout the duration of the study.
We administered one attentiveness check item and one data retention item at the end of the pre-intervention and post-intervention assessment timepoints. The questions prompted participants to indicate on a 7-point Likert scale (1 = Not at all attentive; 7 = Very attentive) how much attention and care they devoted in completing the measures. The second question used a yes/no format asking participants whether their data should be retained. Attentiveness was defined as a score of 4 or higher on the first question and a “Yes” response on the second. Protocol adherence was achieved when participants scored at least 5/8 or higher on such knowledge questions, combined with an attentive profile (as defined above).
Data Analyses
Data were first checked for completeness, accuracy, and skewness. Scale items were then reversed where necessary, and total scores on study measures calculated. We also calculated knowledge and attentiveness scores, and only retained in the final analyses those passing our a priori criteria on the included attentiveness and knowledge questions. We computed internal reliabilities for the CTI-S at the pre-intervention timepoint using Cronbach’s (1951) alpha (α) and McDonald’s (1999) omega (ω). To address the main study hypothesis, we conducted two analyses.
First, we conducted an intention-to-treat (ITT) mixed-linear model (MLM) analysis of all participants randomized and passing initial attention checks. MLM analyses are a type of multilevel models designed to accommodate both fixed and random effects, and their interactions (Kahn, 2011; Peugh, 2010). Fixed effects are population parameters assumed to be the same each time data are collected (e.g., interventions), while random effects are sample parameters that vary each time (e.g., intraindividual factors). MLM is particularly advantageous in longitudinal studies where attrition and data loss are significant, as it can handle unbalanced data. In our MLM, we included fixed effects (Randomized Condition: Mind-OP vs. Active Control; Assessment Time: Pre-Intervention vs. Post-Intervention) and random intercept models to account for individual differences over time to examine changes in scores on the CTI-S (outcome). We used unstructured covariance matrix for the random effects, which provides flexibility and is commonly used in MLM analyses for randomized controlled trials (Haverkamp & Beauducel, 2017). We also included the intercept (within-person variation across time) in the random effects model. The results include main effects of group randomization and time, as well as interaction effects. The interaction effect, which investigates changes between conditions over time, was of primary importance in addressing the trial hypothesis (Carvajal et al., 2001). MLM outputs include F statistics (type III tests of fixed effects), which function as an omnibus test of effects, as well as more specified beta estimates of specific comparisons within the model.
Second, we conducted an MLM analysis using data from protocol-adherent participants (completing all modules, passing all attention check and knowledge questions). Descriptive statistics of protocol-adherent participants, stratified by condition, are summarized in Table 3. These analyses examined differences on NATS (CTI-S) across condition and time. A significant interaction effect between group membership and time was of most interest to our hypothesis. Similar to the above described MLM, we used unstructured covariance matrix, and included the intercept in the random effects model.
We conducted two additional MLM analyses to examine group differences at each pre- and post-intervention timepoints. We calculated Cohen’s d estimates of group differences at each time point using the formula using estimated group means at each timepoints, d = (x̄1 − x̄2) / SDpooled for between-subjects effects (e.g., condition). For within-subjects effects (e.g., time), we used d = (x̄1 − x̄2) / sqrt((SD12 + SD22 − 2rSD1*SD2) where r is the correlation between pre- and post-intervention CTI-S scores (Tabachnick & Fidell, 2007).
Results
As planned, we conducted a mixed-linear model (MLM) analysis with 442 participants who met inclusionary criteria and passed attention checks during the baseline assessment. The analyses revealed a significant interaction effect between Randomized Condition and Time, F(1, 212.85) = 10.64, p = 0.001. Beta estimates (provided in Table 4) suggested participants randomized to the Mind-OP condition reported significantly greater decreases in scores on the CTI-S from pre- to post-intervention. There was no significant main effect of Randomization Condition, F(1, 508.61) = 1.993, p = 0.16. Finally, there was a significant main effect of Time, F(1, 212.85) = 71.99, p < 0.001, wherein participants in both conditions reported decreased scores on the CTI-S at the post-intervention assessment.
As planned, we conducted an additional MLM analysis with protocol-adherent participants (n = 159) to examine change in CTI-S scores across conditions and over the 6-week trial period. The analyses (summarized in Table 4) revealed a significant interaction effect of Randomization Condition and Time, F(1, 159) = 9.82, p < 0.002, wherein participants in the Mind-OP intervention condition experienced greater reductions in CTI-S scores over the trial period compared to those in the active control condition.
There was a significant main effect of Time on CTI-S scores, F(1, 159) = 64.74, p < 0.001, wherein participants across conditions were reporting lower CTI-S scores at the end of the trial compared to pre-intervention. Finally, there was no significant main effect of Randomization Condition collapsed across Time, F(1, 159) = 2.04, p = 0.16.
We conducted two additional MLM analyses to compare differences between Mind-OP and active control participants pre- and post-intervention. These analyses are summarized in Table 5. There was no significant difference between conditions on CTI-S scores at Pre-Intervention, F(1, 157) = 0.09, p = 0.76, d = 0.05 (95% CI: − 0.22 to 0.32); however, there was a significant difference between conditions on CTI-S at Post-Intervention, F(1, 157) = 5.51, p = 0.02, d = 0.38 (95% CI: − 0.06 to 0.70).
Discussion
Depression is a prevalent and debilitating mental health condition. Negative thoughts about self are a central feature of depression. These negative self-referent thoughts appear to be both a by-product and an accelerant of depression. Accordingly, disrupting the predominance of NATS is a worthwhile intermediary goal of psychological interventions, since disrupting such thoughts can dampen depression symptoms over time, and in turn their pernicious effects. While there are many treatments that appear efficacious in reducing NATS, these treatments are usually intensive, requiring substantial therapist support and other resource investments. In the present trial, participants randomized to a brief self-guided internet intervention reported significantly less NATS post-intervention compared to those randomized to an active control condition. Although there are a few published trials demonstrating the efficacy of self-guided interventions in reducing NATS about self, the tested interventions almost always utilize classic cognitive behavioural principles. To the authors’ knowledge, this is the first randomized trial of a self-guided intervention demonstrating mindfulness and self-compassion techniques in reducing NATS.
In the current randomized trial and as predicted, we found participants randomized to the Mind-OP condition reported significantly less intense negative self-referent thoughts at the post-intervention assessment compared to active control condition participants. The significant reductions in NATS are noteworthy; the original trial results indicated no significant difference between participants across conditions and time in depression symptoms (Beshai et al., 2020). Accordingly, it appears the intervention was operating on NATS independently from its operation on depression symptoms, despite the close relationship between these constructs. The reported reductions in NATS by Mind-OP participants over the trial period were of small-medium effect size compared to the same change reported among active control participants. As reviewed, few trials exist demonstrating self-guided interventions using classic cognitive techniques are efficacious in reducing negative automatic thoughts (Everitt et al., 2021; Martinengo et al., 2021). Consistent with the cognitive model, these classic CBT-based self-guided interventions focus on identifying and dismantling negative automatic thoughts. On the other hand, mindfulness and other acceptance-based techniques do not emphasize the direct identification and challenging of unhelpful cognitions. Instead, through the cultivation of mindfulness skills of equanimity and decentring, participants begin to view cognitions as fleeting experiential events (Shapiro et al., 2006). Consistent with this hypothesis, researchers found participants completing a high-intensity mindfulness-based intervention reported significant reductions in negative self-referent thoughts at the end of the trial (Frewen et al., 2008). Accordingly, emphasizing acceptance, compassion, and decentring (or distancing) in one’s approach to dealing with NATS appears no less efficacious than emphasis of classic CBT techniques.
Interestingly, we found that participants randomized to the active control condition also reported significant reductions in NATS from pre- to post-intervention. Although the videos used in the active control condition were short, the presentation of relaxing nature photos and music simultaneously was enough to instigate some changes in negative thoughts and accompanying symptoms (Beshai et al., 2020; Mayer et al., 2009). Indeed, this pattern underscores that trial design, and in particular choice to use a non-active waitlist control, can often result in inflated efficacy for MBIs (Goldberg et al., 2018).
Mind-OP and similar scalable interventions are revolutionary since they can meet the high demand for good mental health services, while addressing several barriers to access that plague uptake (Cavanagh et al., 2014). Such interventions are a natural fit within the stepped care model of mental health (Bower & Gilbody, 2005). This partially addresses the service gap by reserving more resource-heavy interventions for those with more severe symptoms, appropriately leaving self-guided, online interventions as an option for patients with milder distress.
The current trial has several strengths that contribute to this growing literature. For example, this trial employed a relatively large and representative sample. Many self-guided trials generally, and in the field of mindfulness specifically have used small sample sizes composed of student or other unrepresentative samples (Taylor et al., 2021). Further, the efficacy of Mind-OP intervention in reducing NAT was compared against a strong active control condition.
To conclude, there is currently very high unmet need for quality mental health care (Walker et al., 2015). Low-intensity and highly scalable interventions such as Mind-OP offer hope to many. Subthreshold depression, or presence of significant symptoms that are not meeting clinical criteria, is highly prevalent in the general population and is a risk factor for major depression and other psychiatric disorders (Lewinsohn et al., 2000). Evidence suggests NATS have a positive feedback loop with depression, wherein they are predominant during acute phases of the disorder but go on to intensify the symptoms and increase vulnerability to future episodes (Hjemdal et al., 2013). Accordingly, interventions that efficaciously target negative thoughts about self among people with even subthreshold depression help in slowing the momentum of depression. Efficacious self-guided interventions can be deployed immediately, widely, and at low costs to many who need them.
Limitations and Future Research
The trial suffered from several limitations that contextualize the findings and pave the way for future research. First, we did not preregister the current study goals and hypotheses. Second, while samples recruited from crowdsourcing websites are more representative of the general population than student samples, they show disparities with general population samples in several domains. For example, participants recruited from crowdsourcing websites tend to be younger, more educated, more internet and computer savvy, and experiencing more symptoms of psychopathology than general population samples (Walters et al., 2018); however, results from clinical studies completed with crowdsourced samples appear largely reliable and generalizable to general population participants (Daly & Nataraajan, 2015). Third, the primary outcome of the current trial was assessed with one subscale of negative self-referent thoughts. However, it is important to note that scores on the CTI-S subscale, which was used in the current trial, were found to be strongly correlated (r = 0.75) with the most validated and commonly used measure of negative automatic thoughts, the Automatic Thoughts Questionnaire (Beshai et al., 2012; Hollon & Kendall, 1980). Fourth, the current trial did not assess the efficacy of Mind-OP in sustaining reductions in NATS in the long-term and well beyond the post-intervention period. Fifth, we only assessed NATS at the pre- and post-intervention timepoints, and accordingly, could not observe the week-to-week declines in NATS as participants progressed through the intervention.
Future trials should employ more sophisticated methodologies to examine NATS using several measures, over several assessment timepoints and longer follow-up. Further, future trials can assess whether NATS mediate the effects of Mind-OP and similar interventions in reducing symptoms over time.
Data Availability
All data will be made available at the Open Science Framework https://doi.org/10.17605/OSF.IO/58D6K.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Arimitsu, K. (2016). The effects of a program to enhance self-compassion in Japanese individuals: A randomized controlled pilot study. The Journal of Positive Psychology, 11(6), 559–571. https://doi.org/10.1080/17439760.2016.1152593
Ayhan, M. O., & Kavak Budak, F. (2021). The correlation between mindfulness and negative automatic thoughts in depression patients. Perspectives in Psychiatric Care, 57(4), 1944–1949. https://doi.org/10.1111/ppc.12770
Beck, A. T., Steer, R. A., & Brown, G. (1996). Beck Depression Inventory–II (BDI-II) [Database record]. APA PsycTests. https://doi.org/10.1037/t00742-000
Barak, A., Hen, L., Boniel-Nissim, M., & Shapira, N. (2008). A comprehensive review and a meta-analysis of the effectiveness of internet-based psychotherapeutic interventions. Journal of Technology in Human Services, 26(2–4), 109–160. https://doi.org/10.1080/15228830802094429
Beck, A. T. (2008). The evolution of the cognitive model of depression and its neurobiological correlates. American Journal of Psychiatry, 165(8), 969–977. https://doi.org/10.1176/appi.ajp.2008.08050721
Beckham, E. E., Leber, W. R., Watkins, J. T., Boyer, J. L., & Cook, J. B. (1986). Development of an instrument to measure Beck’s cognitive triad: The Cognitive Triad Inventory. Journal of Consulting and Clinical Psychology, 54(4), 566–567. https://doi.org/10.1037/0022-006X.54.4.566
Beevers, C. G., & Miller, I. W. (2005). Unlinking negative cognition and symptoms of depression: Evidence of a specific treatment effect for cognitive therapy. Journal of Consulting and Clinical Psychology, 73(1), 68–77. https://doi.org/10.1037/0022-006X.73.1.68
Bennett-Levy, J., Richards, D. A., & Farrand, P. (2010). Low intensity CBT interventions: A revolution in mental health care. In J. Bennett-Levy, D. A. Richards, P. Farrand, H. Christensen, K. M. Griffiths, D. J. Kavanaugh, B. Klein, M. A. Lau, J. Proudfoot, L. Ritterband, J. White, & C. Williams (Eds.), Oxford guide to low intensity CBT interventions (pp. 3–18). Oxford University Press. https://doi.org/10.1093/med:psych/9780199590117.003.0001
Beshai, S., Dobson, K. S., & Adel, A. (2012). Cognition and dysphoria in Egypt and Canada: An examination of the cognitive triad. Canadian Journal of Behavioural Science/revue Canadienne Des Sciences Du Comportement, 44(1), 29–39. https://doi.org/10.1037/a0025744
Beshai, S., Dobson, K. S., Adel, A., & Hanna, N. (2016). A cross-cultural study of the cognitive model of depression: Cognitive experiences converge between Egypt and Canada. PLoS ONE, 11(3), e0150699. https://doi.org/10.1371/journal.pone.0150699
Beshai, S., Mishra, S., Meadows, T. J. S., Parmar, P., & Huang, V. (2017). Minding the gap: Subjective relative deprivation and depressive symptoms. Social Science & Medicine, 173, 18–25. https://doi.org/10.1016/j.socscimed.2016.11.021
Beshai, S., Bueno, C., Yu, M., Feeney, J. R., & Pitariu, A. (2020). Examining the effectiveness of an online program to cultivate mindfulness and self-compassion skills (Mind-OP): Randomized controlled trial on Amazon’s Mechanical Turk. Behaviour Research and Therapy, 134, 103724. https://doi.org/10.1016/j.brat.2020.103724
Blatt, S. J., Quinlan, D. M., Chevron, E. S., McDonald, C., & Zuroff, D. (1982). Dependency and self-criticism: Psychological dimensions of depression. Journal of Consulting and Clinical Psychology, 50(1), 113–124. https://doi.org/10.1037/0022-006X.50.1.113
Bower, P., & Gilbody, S. (2005). Stepped care in psychological therapies: Access, effectiveness and efficiency: Narrative literature review. The British Journal of Psychiatry, 186(1), 11–17. https://doi.org/10.1192/bjp.186.1.11
Carvajal, S. C., Baumler, E., Harrist, R. B., & Parcel, G. S. (2001). Multilevel models and unbiased tests for group based interventions: Examples from the Safer Choices Study. Multivariate Behavioral Research, 36(2), 185–205. https://doi.org/10.1207/S15327906MBR3602_03
Cavanagh, K., Strauss, C., Forder, L., & Jones, F. (2014). Can mindfulness and acceptance be learnt by self-help?: A systematic review and meta-analysis of mindfulness and acceptance-based self-help interventions. Clinical Psychology Review, 34(2), 118–129. https://doi.org/10.1016/j.cpr.2014.01.001
Chahar Mahali, S., Beshai, S., Feeney, J. R., & Mishra, S. (2020). Associations of negative cognitions, emotional regulation, and depression symptoms across four continents: International support for the cognitive model of depression. BMC Psychiatry, 20(1), 18. https://doi.org/10.1186/s12888-019-2423-x
Chandler, J., & Shapiro, D. (2016). Conducting clinical research using crowdsourced convenience samples. Annual Review of Clinical Psychology, 12(1), 53–81. https://doi.org/10.1146/annurev-clinpsy-021815-093623
Choon, M. W., Abu Talib, M., Yaacob, S. N., Awang, H., Tan, J. P., Hassan, S., & Ismail, Z. (2015). Negative automatic thoughts as a mediator of the relationship between depression and suicidal behaviour in an at-risk sample of Malaysian adolescents. Child and Adolescent Mental Health, 20(2), 89–93. https://doi.org/10.1111/camh.12075
Clark, D. A., Beck, A. T., & Alford, B. A. (1999). Scientific foundations of cognitive theory and therapy of depression. John Wiley.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. https://doi.org/10.2307/2136404
Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika, 16(3), 297–334. https://doi.org/10.1007/BF02310555
Cuijpers, P., Donker, T., Johansson, R., Mohr, D. C., van Straten, A., & Andersson, G. (2011). Self-guided psychological treatment for depressive symptoms: A meta-analysis. PLoS ONE, 6(6), e21274. https://doi.org/10.1371/journal.pone.0021274
Daly, T. M., & Nataraajan, R. (2015). Swapping bricks for clicks: Crowdsourcing longitudinal data on Amazon Turk. Journal of Business Research, 68(12), 2603–2609. https://doi.org/10.1016/j.jbusres.2015.05.001
Dobson, K. S., & Shaw, B. F. (1986). Cognitive assessment with major depressive disorders. Cognitive Therapy and Research, 10(1), 13–29. https://doi.org/10.1007/BF01173379
Dozois, D. J. A., Bieling, P. J., Patelis-Siotis, I., Hoar, L., Chudzik, S., McCabe, K., & Westra, H. A. (2009). Changes in self-schema structure in cognitive therapy for major depressive disorder: A randomized clinical trial. Journal of Consulting and Clinical Psychology, 77(6), 1078–1088. https://doi.org/10.1037/a0016886
Dudek, D., Dudek, D., Siwek, M., Datka, W., Rzeszutko, Ł, Silczuk, A., & Zięba, A. (2007). Depressive symptoms in patients with coronary artery disease after percutaneous coronary interventions (PCIs). Archives of Psychiatry and Psychotherapy, 3, 63–70.
Everitt, N., Broadbent, J., Richardson, B., Smyth, J. M., Heron, K., Teague, S., & Fuller-Tyszkiewicz, M. (2021). Exploring the features of an app-based just-in-time intervention for depression. Journal of Affective Disorders, 291, 279–287. https://doi.org/10.1016/j.jad.2021.05.021
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. https://doi.org/10.3758/BRM.41.4.1149
Flouri, E., & Panourgia, C. (2014). Negative automatic thoughts and emotional and behavioural problems in adolescence. Child and Adolescent Mental Health, 19(1), 46–51. https://doi.org/10.1111/camh.12004
Frewen, P. A., Evans, E. M., Maraj, N., Dozois, D. J. A., & Partridge, K. (2008). Letting go: Mindfulness and negative automatic thinking. Cognitive Therapy and Research, 32(6), 758–774. https://doi.org/10.1007/s10608-007-9142-1
Friederichs, S. A., Oenema, A., Bolman, C., & Lechner, L. (2015). Long term effects of self-determination theory and motivational interviewing in a web-based physical activity intervention: Randomized controlled trial. International Journal of Behavioral Nutrition and Physical Activity, 12(1), 101. https://doi.org/10.1186/s12966-015-0262-9
Gilbert, P. (2000). The relationship of shame, social anxiety and depression: The role of the evaluation of social rank. Clinical Psychology & Psychotherapy, 7(3), 174–189. https://doi.org/10.1002/1099-0879(200007)7:3%3c174::AID-CPP236%3e3.0.CO;2-U
Grabovac, A. D., Lau, M. A., & Willett, B. R. (2011). Mechanisms of mindfulness: A Buddhist psychological model. Mindfulness, 2(3), 154–166. https://doi.org/10.1007/s12671-011-0054-5
Goldberg, S. B., Tucker, R. P., Greene, P. A., Davidson, R. J., Wampold, B. E., Kearney, D. J., & Simpson, T. L. (2018). Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clinical Psychology Review, 59, 52–60. https://doi.org/10.1016/j.cpr.2017.10.011
Gu, J., Strauss, C., Crane, C., Barnhofer, T., Karl, A., Cavanagh, K., & Kuyken, W. (2016). Examining the factor structure of the 39-item and 15-item versions of the Five Facet Mindfulness Questionnaire before and after mindfulness-based cognitive therapy for people with recurrent depression. Psychological Assessment, 28(7), 791–802. https://doi.org/10.1037/pas0000263
Haverkamp, N., & Beauducel, A. (2017). Violation of the sphericity assumption and its effect on type-i error rates in repeated measures ANOVA and multi-level linear models (MLM). Frontiers in Psychology, 8, 1841. https://www.frontiersin.org/articles/10.3389/fpsyg.2017.01841
Hjemdal, O., Stiles, T., & Wells, A. (2013). Automatic thoughts and meta-cognition as predictors of depressive or anxious symptoms: A prospective study of two trajectories. Scandinavian Journal of Psychology, 54(2), 59–65. https://doi.org/10.1111/sjop.12010
Holahan, C. J., Moos, R. H., Holahan, C. K., Brennan, P. L., & Schutte, K. K. (2005). Stress generation, avoidance coping, and depressive Symptoms: A 10-year model. Journal of Consulting and Clinical Psychology, 73, 658–666. https://doi.org/10.1037/0022-006X.73.4.658
Hollon, S. D., & Kendall, P. C. (1980). Cognitive self-statements in depression: Development of an automatic thoughts questionnaire. Cognitive Therapy and Research, 4(4), 383–395. https://doi.org/10.1007/BF01178214
Holmes, E. A., Ghaderi, A., Harmer, C. J., Ramchandani, P. G., Cuijpers, P., Morrison, A. P., Roiser, J. P., Bockting, C. L. H., O’Connor, R. C., Shafran, R., Moulds, M. L., & Craske, M. G. (2018). The Lancet Psychiatry Commission on psychological treatments research in tomorrow’s science. The Lancet Psychiatry, 5(3), 237–286. https://doi.org/10.1016/S2215-0366(17)30513-8
Hou, X.-L., Bian, X.-H., Zuo, Z.-H., Xi, J.-Z., Ma, W.-J., & Owens, L. D. (2021). Childhood maltreatment on young adult depression: A moderated mediation model of negative automatic thoughts and self-compassion. Journal of Health Psychology, 26(13), 2552–2562. https://doi.org/10.1177/1359105320918351
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10(2), 144–156. https://doi.org/10.1093/clipsy.bpg016
Kahn, J. H. (2011). Multilevel modeling: Overview and applications to research in counseling psychology. Journal of Counseling Psychology, 58, 257–271. https://doi.org/10.1037/a0022680
Kang, Y., Gruber, J., & Gray, J. R. (2013). Mindfulness and de-automatization. Emotion Review, 5(2), 192–201. https://doi.org/10.1177/1754073912451629
Karyotaki, E., Kleiboer, A., Smit, F., Turner, D. T., Pastor, A. M., Andersson, G., Berger, T., Botella, C., Breton, J. M., Carlbring, P., Christensen, H., de Graaf, E., Griffiths, K., Donker, T., Farrer, L., Huibers, M. J. H., Lenndin, J., Mackinnon, A., Meyer, B., ... Cuijpers, P. (2015). Predictors of treatment dropout in self-guided web-based interventions for depression: An ‘individual patient data’ meta-analysis. Psychological Medicine, 45(13), 2717–2726. https://doi.org/10.1017/S0033291715000665
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Lamberton, A., & Oei, T. P. S. (2008). A test of the cognitive content specificity hypothesis in depression and anxiety. Journal of Behavior Therapy and Experimental Psychiatry, 39(1), 23–31. https://doi.org/10.1016/j.jbtep.2006.11.001
Lewinsohn, P. M., Solomon, A., Seeley, J. R., & Zeiss, A. (2000). Clinical implications of “subthreshold” depressive symptoms. Journal of Abnormal Psychology, 109(2), 345–351. https://doi.org/10.1037/0021-843X.109.2.345
Litman, L., Robinson, J., & Abberbock, T. (2017). TurkPrime.com: A versatile crowdsourcing data acquisition platform for the behavioral sciences. Behavior Research Methods, 49(2), 433–442. https://doi.org/10.3758/s13428-016-0727-z
Mantzios, M., & Wilson, J. C. (2014). Making concrete construals mindful: A novel approach for developing mindfulness and self-compassion to assist weight loss. Psychology & Health, 29(4), 422–441. https://doi.org/10.1080/08870446.2013.863883
Martinengo, L., Stona, A.-C., Griva, K., Dazzan, P., Pariante, C. M., von Wangenheim, F., & Car, J. (2021). Self-guided cognitive behavioral therapy apps for depression: Systematic assessment of features, functionality, and congruence with evidence. Journal of Medical Internet Research, 23(7), e27619. https://doi.org/10.2196/27619
Mayer, F. S., Frantz, C. M., Bruehlman-Senecal, E., & Dolliver, K. (2009). Why is nature beneficial?: The role of connectedness to nature. Environment and Behavior, 41(5), 607–643. https://doi.org/10.1177/0013916508319745
McDonald, R. P. (1999). Test theory: A unified treatment. Lawrence Erlbaum. https://doi.org/10.4324/9781410601087
Mehdipour, F., Rafiepoor, A., & Haji Alizadeh, K. (2017). The effectiveness of mindfulness-based cognitive group therapy in reducing negative automatic thoughts and dysfunctional attitudes in cancer patients. Zahedan Journal of Research in Medical Sciences, 19(6). https://doi.org/10.5812/zjrms.10609
Moncher, F. J., & Prinz, R. J. (1991). Treatment fidelity in outcome studies. Clinical Psychology Review, 11(3), 247–266. https://doi.org/10.1016/0272-7358(91)90103-2
Moroz, N., Moroz, I., & D’Angelo, M. S. (2020). Mental health services in Canada: Barriers and cost-effective solutions to increase access. Healthcare Management Forum, 33(6), 282–287. https://doi.org/10.1177/0840470420933911
Neff, K. (2003a). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85–101. https://doi.org/10.1080/15298860309032
Neff, K. D. (2003b). The development and validation of a scale to measure self-compassion. Self and Identity, 2(3), 223–250. https://doi.org/10.1080/15298860309027
Oei, T. P. S., Dingle, G. A., & McCarthy, M. (2010). Urinary catecholamine levels and response to group cognitive behaviour therapy in depression. Behavioural and Cognitive Psychotherapy, 38(4), 479–483. https://doi.org/10.1017/S1352465810000093
Patel, V., Chowdhary, N., Rahman, A., & Verdeli, H. (2011). Improving access to psychological treatments: Lessons from developing countries. Behaviour Research and Therapy, 49(9), 523–528. https://doi.org/10.1016/j.brat.2011.06.012
Pedro, L., Branquinho, M., Canavarro, M. C., & Fonseca, A. (2019). Self-criticism, negative automatic thoughts and postpartum depressive symptoms: The buffering effect of self-compassion. Journal of Reproductive and Infant Psychology, 37(5), 539–553. https://doi.org/10.1080/02646838.2019.1597969
Peugh, J. L. (2010). A practical guide to multilevel modeling. Journal of School Psychology, 48(1), 85–112. https://doi.org/10.1016/j.jsp.2009.09.002
Radloff, L. S. (1977). The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. https://doi.org/10.1177/014662167700100306
Raes, F., Pommier, E., Neff, K. D., & Van Gucht, D. (2011). Construction and factorial validation of a short form of the Self-Compassion Scale. Clinical Psychology & Psychotherapy, 18(3), 250–255. https://doi.org/10.1002/cpp.702
Richards, D. (2011). Prevalence and clinical course of depression: A review. Clinical Psychology Review, 31(7), 1117–1125. https://doi.org/10.1016/j.cpr.2011.07.004
Saltzman, K. M., & Holahan, C. J. (2002). Social support, self-efficacy, and depressive symptoms: An integrative model. Journal of Social and Clinical Psychology, 21(3), 309–322. https://doi.org/10.1521/jscp.21.3.309.22531
Santomauro, D. F., Herrera, A. M. M., Shadid, J., Zheng, P., Ashbaugh, C., Pigott, D. M., ..., & Ferrari, A. J. (2021). Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. The Lancet, 398(10312), 1700–1712. https://doi.org/10.1016/S0140-6736(21)02143-7
Schueller, S. M., & Parks, A. C. (2014). The science of self-help: Translating positive psychology research into increased individual happiness. European Psychologist, 19(2), 145–155. https://doi.org/10.1027/1016-9040/a000181
Shapiro, S. L., Carlson, L. E., Astin, J. A., & Freedman, B. (2006). Mechanisms of mindfulness. Journal of Clinical Psychology, 62(3), 373–386. https://doi.org/10.1002/jclp.20237
Spijkerman, M. P. J., Pots, W. T. M., & Bohlmeijer, E. T. (2016). Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clinical Psychology Review, 45, 102–114. https://doi.org/10.1016/j.cpr.2016.03.009
Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Stefan, S., Cristea, I. A., Szentagotai Tatar, A., & David, D. (2019). Cognitive-behavioral therapy (CBT) for generalized anxiety disorder: Contrasting various CBT approaches in a randomized clinical trial. Journal of Clinical Psychology, 75(7), 1188–1202. https://doi.org/10.1002/jclp.22779
Strauss, C., Lever Taylor, B., Gu, J., Kuyken, W., Baer, R., Jones, F., & Cavanagh, K. (2016). What is compassion and how can we measure it? A review of definitions and measures. Clinical Psychology Review, 47, 15–27. https://doi.org/10.1016/j.cpr.2016.05.004
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.). Allyn & Bacon/Pearson Education. https://doi.org/10.4236/ojm.2013.33016
Tarkhan, M. (2018). The effectiveness of group mindfulness-based cognitive therapy on negative automatic thoughts, aggression and dysfunctional attitudes of aggressive students. Journal of Psychological Studies, 14(2), 161–176.
Taylor, H., Strauss, C., & Cavanagh, K. (2021). Can a little bit of mindfulness do you good? A systematic review and meta-analyses of unguided mindfulness-based self-help interventions. Clinical Psychology Review, 89, 102078. https://doi.org/10.1016/j.cpr.2021.102078
GBD 2019 Diseases and Injuries Collaborators (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. The Lancet, 396(10258), 1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
Walker, E. R., Cummings, J. R., Hockenberry, J. M., & Druss, B. G. (2015). Insurance status, use of mental health services, and unmet need for mental health care in the United States. Psychiatric Services, 66(6), 578–584. https://doi.org/10.1176/appi.ps.201400248
Walters, K., Christakis, D. A., & Wright, D. R. (2018). Are Mechanical Turk worker samples representative of health status and health behaviors in the U.S.? PLoS ONE, 13(6), e0198835. https://doi.org/10.1371/journal.pone.0198835
Webber, K. H., Tate, D. F., & Michael Bowling, J. (2008). A randomized comparison of two motivationally enhanced internet behavioral weight loss programs. Behaviour Research and Therapy, 46(9), 1090–1095. https://doi.org/10.1016/j.brat.2008.06.008
Yapan, S., Türkçapar, M. H., & Boysan, M. (2022). Rumination, automatic thoughts, dysfunctional attitudes, and thought suppression as transdiagnostic factors in depression and anxiety. Current Psychology, 41(9), 5896–5912. https://doi.org/10.1007/s12144-020-01086-4
Zhang, R., Peng, X., Song, X., Long, J., Wang, C., Zhang, C., Huang, R., & Lee, T. M. C. (2023). The prevalence and risk of developing major depression among individuals with subthreshold depression in the general population. Psychological Medicine, 53(8), 3611–3620. https://doi.org/10.1017/S0033291722000241
Funding
This investigation was supported by an internal grant by the University of Regina.
Author information
Authors and Affiliations
Contributions
Shadi Beshai contributed to writing manuscript draft, data analyses, and table creation. Christine Bueno contributed to survey development, data collection, data analyses, and table creation. Saba Salimuddin contributed to manuscript editing and table creation.
Corresponding author
Ethics declarations
Ethical Approval
The authors declare that all processes associated with this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975 and its later amendments. The University of Regina’s Research Ethics Board approved the study described in this investigation (#2018–158).
Informed Consent
Informed consent was obtained from all participants included in this investigation.
Conflict of Interest
The authors declare no competing interests.
Use of Artificial Intelligence
No artificial intelligence was utilized in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Beshai, S., Bueno, C. & Salimuddin, S. Effects of a Self-Guided Online Mindfulness and Self-Compassion Program (Mind-OP) in Reducing Negative Automatic Thoughts About Self: Randomized Active Controlled Trial. Mindfulness 15, 259–271 (2024). https://doi.org/10.1007/s12671-023-02261-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-023-02261-x