
Abstract
Objectives
Mounting research has supported the beneficial effects of compassion-based interventions for improving psychosocial and physiological well-being and mental health. Teachers present a high risk of professional stress, which negatively impacts their mental health and professional performance. It is crucial to make compassion cultivation a focus in educational settings, supporting teachers in coping with the school context’s challenges, and promoting their mental well-being. This study aims to test the feasibility of the Compassionate Mind Training programme for Teachers (CMT-T), as well as to preliminary explore possible mechanisms of change.
Methods
Participants were 31 teachers from one public school in the centre region of Portugal, who underwent the CMT-T, a six-module Compassionate Mind Training group intervention for teachers. Feasibility was assessed in six domains (acceptability, implementation, practicality, adaptation, integration, and preliminary effectiveness), using self-reports, overall programme assessment, attrition, attendance, and home practice. Using a pre-post within-subject design, changes were assessed in self-reported psychological distress, burnout, well-being, compassion, and self-criticism. Mediation analysis for repeated measures designs was used to explore mechanisms of change.
Results
The CMT-T was feasible in all the six domains. Participants revealed significant decreases in depression, stress, and fears of compassion to others, as well as significant increases in compassion to others, self-compassion, and compassion to others’ motivations and actions after the CMT-T intervention. When self-criticism was controlled, decreases in burnout and increases in satisfaction with professional life, and self-compassion, were also found. Fears of compassion for others mediated the impact of CMT-T on teachers’ burnout, and self-compassion mediated the intervention effect on psychological well-being.
Conclusions
This pilot study provides evidence that CMT-T is feasible and may be effective in promoting teachers’ compassionate motivations, attributes, and actions towards others and themselves and improving their mental health and well-being. These promising findings warrant further investigation within a randomized controlled trial.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Teaching is a demanding job. Teachers must respond to students’ diverse and fluctuating needs, integrate innovative professional learning into their practices, and interact with colleagues and families. These activities require the capacity to regulate thoughts, feelings, and behaviours. Growing evidence indicates that schools are becoming increasingly stressful environments for both teachers and pupils (ESP, 2018; NASUWT, 2016). In fact, teachers’ stress has been described as an international challenge (Hakanen et al., 2006; Liu & Onwuegbuzie, 2012) with reports of stress in teaching professionals being a world-wide phenomenon (e.g. McCallum et al., 2017; Travers, 2017). Recently, OFSTED (2019) reported that 76% of teachers reported their job negatively impacted their mental health, with more than 50% of teachers disappointed with their profession. In Portugal, a recent report about teachers’ work conditions (Varela et al., 2018) documented that 75% of teachers present high burnout levels, with 25% reporting extreme burnout. More than 60% of teachers experience high levels of stress and emotional exhaustion. Furthermore, 84% of these teachers declare that they intend to leave the profession. The high levels of teachers’ stress are detrimental to their well-being (McCallum et al., 2017) and physical (Katz et al., 2016) and mental health (Schonfeld et al., 2017). Moreover, teachers’ stress and burnout are related to an array of negative outcomes in students. A study showed that students’ cortisol levels were much higher in classrooms led by teachers who reported feeling overwhelmed (Oberle & Schonert-Reichl, 2016). Longitudinal studies have revealed that teachers who report higher levels of burnout early in the school year have classes with more behavioural problems across the year (McLean & Connor, 2015). Furthermore, when teachers are highly stressed, children show lower social adjustment levels and academic performance (Hoglund et al., 2015).
Given the high prevalence of mental health problems in the school context, it is crucial to promote adaptive cognitive and emotional processes. Providing teachers with better resources to deal with the school environment’s challenges, resulting from stressful uncertainty, and accelerated social, economic, and technological changes, is essential. In applying Gilbert’s (2009) evolutionary model of compassion and compassion-focused therapy framework, and findings from a therapeutic background (e.g. Leaviss & Uttley, 2015) to a number of compassion-based approaches in education, Welford and Langmead (2015) argued that “compassion-based approaches within education settings offer a potential means of generating greater psychological well-being for students, staff, parents and the wider community whilst also protecting and enhancing the priorities of the settings in which they are applied. Thus, they represent an intervention which is systemic and universal” (p. 71). In fact, making compassion a focus for education is critically important nowadays, as it may provide teachers and pupils with emotional coping skills; address bullying and other behavioural problems; develop ethical behaviour; promote prosociality; and thus contribute to building safe, collaborative, encouraging, and supportive learning environments (Lavelle, 2017; Peterson, 2017; Roeser et al., 2018).
In fact, modern societies’ competitive dynamics, often patent in schools, are major sources of stress, affecting both teachers (e.g. heavy workloads, achievement focus, performance evaluation) and pupils (e.g. focus on academic achievement, self-interest). Self- and other-focused competitive pressures have been highlighted as a major source for teacher and pupil mental health problems (Rodway et al., 2016; Wetherall et al., 2019), and may underlie feelings of shame, unfavourable social comparisons, fear of failure, loneliness, self-criticism, and fears of compassion (e.g. Basran et al., 2019; Cunha et al., 2012). Whilst schools can foster competitive motives and related activation of threat-defensive responses (e.g. in the form of self-criticism), they can also be facilitators of the development of prosociality and compassion motives (Coles, 2015; Gilbert et al., 2020). Contrarily to competitive motives, the enactment of compassion motives, for example through caring and sharing, stimulate particular physiological systems linked to affiliation and social connectedness (e.g. parasympathetic nervous system (Petrocchi & Cheli, 2019), oxytocinergic system (Colonnello et al., 2017)), which contribute to well-being, stress management, and emotion regulation (Carter et al., 2017; Gilbert, 2020).
In evolutionary-focused models (Gilbert, 2014, 2020), compassion has been conceptualized as a prosocial motivation that involves “the sensitivity to suffering in self and others, with a commitment to try to alleviate and prevent it” (Gilbert, 2014, p. 19). In light of this approach, compassion is multidimensional and can be seen as a dynamic intra- and interpersonal process that occurs in a social interactional context. Compassion can hence have different flows: it can be directed inwards, in the form of self-compassion and compassion received from others, and outwards, in the form of or compassion given to others (Gilbert et al., 2011). These flows of compassion (for self, from others, and for others) are highly interactive but can also be independent (Gilbert, 2014; Gilbert et al., 2017), in the sense that one might find it difficult to be self-compassionate but be able to be compassionate towards others (Lopez et al., 2018).
Compassion-based interventions have received increasing empirical support regarding their beneficial impact on developing adaptive emotional regulation skills central to stress regulation and promoting well-being (Kirby, 2017). These interventions have shown numerous benefits in diverse populations and contexts, in mental health indicators (e.g. lower depression, stress, anxiety), physical health (e.g. regulation of neurochemical processes associated with the stress response), and at an interpersonal level (e.g. greater empathy and compassion, improved interpersonal and social relations) (Kirby, 2017; Kirby et al., 2017; Leaviss & Uttley, 2015, for reviews). One of these approaches is Compassion-Focused Therapy (CFT; Gilbert, 2009, 2014), rooted in evolutionary psychology, attachment theory, psychological science, and an understanding of motivational systems, and originally developed as a transdiagnostic treatment for people struggling with shame and self-criticism. CFT aims to help cultivate a person’s compassion/caring motives, emotions, attention, thinking, and behaviour, in order to downregulate competitive and threat-focused ones and alleviate persistent patterns of distress. CFT has gathered mounting evidence for its effectiveness in diverse clinical conditions and symptoms (Craig et al., 2020; Kirby et al., 2017 for reviews).
CFT incorporates Compassionate Mind Training (CMT), which is an evolutionary and biopsychosocial evidence-based approach developed as a psychoeducation and set of core compassion and mindfulness practices within CFT (Gilbert, 2009, 2014, 2020). CMT encompasses psychoeducation about compassion and fears of compassion, the evolved nature of mind and body, emotion regulation systems, and self-criticism, and introduces a variety of physiological and psychological practices to target these aspects (e.g. attention training, mindfulness, soothing rhythm breathing, and compassionate imagery). CMT practices aim to promote mind-awareness, slowing down, and grounding in the body (e.g. via the parasympathetic vagal system), and ultimately cultivate a compassionate self-identity (i.e. the compassionate self), linked to qualities of wisdom, strength and caring motivation, and commitment, which is then embodied to deal with common difficulties and daily struggles (e.g. self-criticism) (Gilbert, 2009, 2014; Irons & Beaumont, 2017). CMT has been broadly applied to a wide range of different populations with promising results, such as the general public (Irons & Heriot-Maitland, 2020; Matos et al., 2017), nurses (Beaumont & Martin, 2016), firefighters (Beaumont et al., 2016a), psychotherapy students (Beaumont et al., 2017), or health care educators and providers (Beaumont et al., 2016b), being an adequate approach to target larger groups and specific problems, using different formats (e.g. regarding number of sessions or practices used). Furthermore, research has established the efficacy of CMT in enhancing compassion skills, mindfulness skills, and well-being; in decreasing psychopathological symptoms, such as depression, anxiety, and stress, and vulnerability factors such as self-criticism (Irons & Heriot-Maitland, 2020; for a meta-analysis, see Kirby et al., 2017); and in improving physiological responses to stress (e.g. HRV; Matos et al., 2017).
Nevertheless, evidence suggests that individual differences in self-criticism may impact how individuals respond to compassion-focused interventions. Self-criticism is a transdiagnostic process and shared difficulty in clinical and non-clinical populations and a major vulnerability and maintenance factor for mental health problems (Gilbert et al., 2004; Werner et al., 2019). For example, previous studies have found that individuals high in self-criticism demonstrate threat-like physiological responses to single/brief interventions of compassion-focused imagery, revealing increased amygdala activation (Longe et al., 2010), decreased HRV (Rockliff et al., 2008), higher alpha-amylase (Duarte et al., 2015), and increased resistance to engage in CFI when given oxytocin (Rockliff et al., 2011). This suggests that self-critical individuals might be fearful of compassion, and that may influence the effects of compassion-focused interventions.
In the context of educational settings, applying an evolution and biopsychosocial-based approach to compassion for informing, educating, and nurturing teachers and young minds, such as CMT, is particularly pertinent. One of this approach’s central features is that compassion is contextualized within an evolutionary and physiological framework that acknowledges that motives to be caring can be inhibited or in conflict with other motives, such as self-focused competitiveness and threat-defensiveness (Gilbert, 2014, 2020). This type of approach may help societal and educational leaders reframe the focus and context of education from a westernized self-interest and competition-driven philosophy, to a more compassionate, caring, and nurturing philosophy. This would provide a secure basis for learning and hold the prospect of enhancing well-being across individual and societal relations (Gilbert et al., 2020).
Recently, a CMT programme for teachers was applied in schools in Derby in the UK (Maratos et al., 2019). This feasibility study, conducted in a sample of 70 teachers and support staff, showed that the programme was well-received. Participants (N = 34) evaluated the curriculum and the practices positively, considering its usefulness for dealing with emotional difficulties. Moreover, data from a subsample of 20 teachers (who completed pre- and post-self-report assessments), revealed that self-criticism significantly decreased, and self-compassion significantly increased following the programme. No significant changes were found in burnout and psychopathological symptoms (Maratos et al., 2019).
Based on the version of CMT used in Maratos et al. (2019) and considering some of the authors’ recommendations, the Compassionate Mind Training programme for Teachers (CMT-T) was refined by the UK and Portuguese research teams introducing some adjustments (cf. the “Procedures” section for a detailed description; Gilbert et al., 2020). A recent study investigated the international utility and implementation efficacy of this revised six-module CMT curriculum in Portuguese and UK school settings (Maratos et al., 2020). Results revealed that high-quality implementation was achieved across the UK and Portuguese cohorts, with the majority of staff providing extremely positive ratings regarding all aspects of each module content, delivery, and interest/relevance. These findings highlight the international appeal and utility of CMT in school settings in helping teachers manage work-related stress in schools.
Even though the cross-cultural implementation effectiveness and acceptability of the CMT-T has been previously addressed for each single session in Maratos et al. (2020), the feasibility of the overall CMT-T according to a formal feasibility framework as proposed by Bowen et al. (2009) merits further examination. In addition, the impact of CMT-T on a wider range of well-being indicators (e.g. psychological well-being, satisfaction with professional life) and compassion-related variables (e.g. the three flows of compassion, fears of compassion) warrants further investigation. Furthermore, the role of individual differences in self-criticism on the impact of the CMT-T and the processes of change of the CMT-T are yet to be examined.
The current pilot study aims to further assess the feasibility of the CMT-T according to six of the feasibility domains presented by Bowen et al. (2009), specifically its acceptability, implementation, practicality, adaptation, and integration and its preliminary effectiveness on teachers’ psychological distress, burnout, well-being, compassion, and self-criticism. Based on Gilbert’s biopsychosocial-based approach to compassion and the CFT/CMT framework (Gilbert, 2009, 2014, 2020), we hypothesized that CMT-T would reduce symptoms of depression, stress, and burnout, and would increase satisfaction with professional life and psychological well-being (outcome variables), by increasing the flows of compassion (for self, for others, and from others), compassion (to self and others) motivations, and actions, and by diminishing fears of compassion (for self, for others, and from others) and self-criticism (process variables, directly targeted by the intervention). Moreover, we also explored whether baseline self-criticism was associated with the outcome variables at post-intervention and whether controlling for baseline self-criticism would affect the impact of the CMT-T. Given previous research on the impact of self-criticism on individuals’ responses to compassion-focused interventions (Duarte et al., 2015; Longe et al., 2010; Rockliff et al., 2011), we hypothesized that baseline self-criticism would be positively related to psychological distress, burnout, and fears of compassion, and negatively associated with well-being and compassion, at post-intervention. Also, we expected that controlling for self-criticism would influence the impact of the CMT-T intervention on the outcome and process variables. Finally, we examined whether CMT-T-induced increases in the compassion flows and decreases in fears of compassion (processes directly targeted by the CMT-T) would mediate the changes found in the outcome variables between baseline and post-intervention.
Methods
Participants
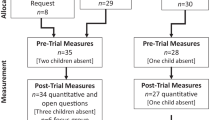
This study was conducted in a sample of public school teachers recruited in a cluster of schools in a small city from Portugal’s centre region. From the initial 40 teachers who registered for the study, 31 enrolled in the CMT-T intervention. This sample is identical to the Portuguese sample used in Maratos et al. (2020). Nine participants dropped out from the study before the start of the intervention due to scheduling incompatibilities (study drop-out rate of 22.5%). All of the 31 participants attended the minimum number of 4 sessions and completed pre- and post-assessments. The final sample was composed of 8 (27%) men and 23 (74.2%) women, with a mean age of 51.33 (SD = 5.27), age ranging between 40 and 62 years old. Most participants held a bachelor degree (N = 20; 64.5%) and the remaining had completed a master degree (N = 8; 25.8%) or a postgraduate specialization degree (N = 3; 9.7%). The majority of the participants were married (N = 23; 74.2%), 22.6% were single (N = 7), and 3.2% were divorced (N = 1).
Regarding teaching-related characteristics, the number of years participants worked as teachers ranged between 17 and 35 (M = 27.53, SD = 4.51). Participants taught in several grade levels and subject areas, with 16.1% (N = 5) being preschool teachers and 6.5% (N = 2) elementary school teachers. The majority of participants qualified as middle or high school grade level teachers in the following content areas: 22.5% (N = 7) languages, 9.7%. (N = 3) social and human sciences, 32.3% (N = 10) mathematics and experimental sciences, and 3.2% (N = 1) artistic expressions. Three teachers did not provide information about this aspect.
In terms of the school setting, the cluster of schools where participants were recruited included large urban schools and small schools in the rural areas. Overall, this cluster encompassed 106 teachers, 64 non-teaching staff, and 1121 students distributed by 59 classes of all grade levels (with a mean of 19 students per class). Around 64% of students had low socioeconomic status.
Procedures
The Ethics Committee of the Faculty of Psychology and Educational Sciences of the University of Coimbra approved the study (CEDI22.03.2018). The project was presented to several Heads of public schools of Coimbra and Viseu districts (the centre region of Portugal). One school was randomly chosen to implement the pilot study of the CMT-T. In a meeting with the Board of the school enrolled in the project, the research team presented the aims of intervention, as well as the programme structure and its implementation. The school provided further ethical approval and invited teachers to take part. A leaflet with information about the CMT-T intervention and conditions for participation in the study was designed for the teachers by the research team and distributed among staff by the school’s Board. Teachers interested in participating in the study contacted the research team via email. Information concerning the study’s voluntary and confidential nature and a brief overview of the intervention was further provided to all teachers. Also, teachers who registered to participate signed an informed consent. A unique and numerical code was assigned to each participant to ensure confidentiality. Baseline assessment occurred during the week previous to the first session; post-treatment assessment was obtained during the first week post-intervention. Participants attended the 6-week CMT-T and were instructed to practise the CMT exercises daily or in moments of stress. They completed a set of self-report measures at pre- and post-intervention and filled out weekly Practice Diaries and Session Evaluation forms.
The Compassionate Mind Training Programme for Teachers
The Compassionate Mind Training programme for Teachers (CMT-T) is a six-module compassion mind training group programme delivered across six sessions, each lasting approximately 2 h. The CMT-T was conducted with one group of teachers (N = 31) during 6 weeks over one school term. Part of this programme was derived from research with community populations that showed significant beneficial effects on a range of psychological and physiological well-being indicators of just 2 weeks of practising a set of core Compassionate Mind Training practices (Matos et al., 2017, 2018). The CMT-T curriculum was developed based on an earlier version of the programme for school staff designed and tested by Maratos et al. (2019) and on a brief CMT programme for the general public (Matos et al., 2017). Please see Table 1 for an overview of the CMT-T. A brief description of the teachers’ Compassionate Mind Training programme session content is presented below (a more detailed description of each CMT-T session content is provided as a Supplementary File).
During the sessions and after each exercise, time was provided for participants to work in small groups to share their experiences, followed by a plenary session. The CMT-T team included four qualified clinical psychologists with a PhD degree and clinical experience in applying CFT-based interventions and one teacher with a PhD degree and a PGCert in CFT. Each session had one lead facilitator, who facilitated the group, presented the content, led experiential exercises, and facilitated the discussion, and one main co-facilitator, who also led some experiential exercises and facilitated the discussion. The other co-facilitators of that session were available if concerns arose and if participants needed one-on-one support, and were responsible for collecting assessment materials. Additionally, participants were informed that the CMT-T team would be available for contact after the sessions if any session’s content or discussions would raise any particular query for them, following the British Psychological Society (BPS, 2018) recommendations.
Measures
Demographic data were gathered in a sociodemographic questionnaire, comprising the following variables: age, years of education, marital status, teaching experience, and teaching-related variables (e.g. teaching subject, professional situation).
Feasibility
Feasibility was assessed according to six criteria of Bowen et al.’s (2009) framework:
Acceptability: defined as importance, relevance, and perceived helpfulness of sessions and practices, as well as motivation and willingness to recommend the CMT-T to peers. Acceptability was assessed using the CMT qualitative assessment questionnaire. In the last session of the CMT, participants were provided with a brief questionnaire to enable an overall qualitative evaluation of the programme. The first part of this form included six questions assessing the importance of the training, the relevance of sessions, helpfulness of sessions, adequacy of practices, attendance motivation, and whether they would recommend the training to other colleagues. Participants were asked to rate each question using a 5-point categorical scale: nothing (1), a little (2), moderately (3), very (4), extremely (5). Teachers were asked to “please mark the response that best reflects your experience of this training”. The second part of the questionnaire assessed which session participants found the most helpful. Among the list of the six sessions, participants were invited to choose the session they found the most helpful. The last part of the evaluation form entailed a question about which practice they considered more helpful. Participants were presented with a list of all the practices introduced in the CMT-T and asked to choose the one(s) they found helpful. Finally, participants were invited to respond to an open-question where they could express any positive or negative comments and suggestions about the CMT-T.
Implementation: operationalized as the extent to which the programme could be fully delivered, specifically number of cancelled or postponed sessions and conditions provided by the enrolled schools.
Practicality: assessed by programme attendance and drop-out.
Adaptation: operationalized as adjustments made to the CMT-T curriculum from its earlier version (Maratos et al., 2019) and from the brief CMT programme (Matos et al., 2017).
Integration: defined as the extent to which participants used the practices and knowledge and were able to embody these in their everyday life. It was assessed through a CMT Practice Diary (Matos et al., 2018) retrospectively filled at the completion of the programme, measuring Practice Frequency (How often did you practise the exercises during the programme?, rated on a 5-point scale: never, 1–2, 3–4, 5–6, and 7 or more times per week) and Embodiment of the compassionate self (i.e. ability to act and feel as their compassionate self) in everyday life and in moments of difficulty (composite index formed by the dimensions of frequency, easiness, power, duration, soothing effect, and impact, each rated on a 10-point scale, cf. Matos et al., 2018 for further detail).
Preliminary effectiveness: operationalized as effect size estimations in well-being, burnout psychological distress, compassion, and self-criticism as measured by the self-report questionnaires described below.
Satisfaction with Teachers’ Professional Life (STPL; Diener et al., 1985; Portuguese Version by Albuquerque et al., 2021a, b)
This is a single-factor scale comprising 5 items assessing global satisfaction with teachers’ professional life. Teachers are asked to rate each item using a 5-point Likert-type scale scored between 1 (I completely disagree) and 5 (I completely agree). The psychometric properties of this scale in the present study showed a Cronbach alpha of 0.90.
Psychological Well-Being Scales (Ryff & Essex, 1992; PWBS-24, Shortened Portuguese Version by Albuquerque et al., 2021a, b)
The Psychological Well-Being (PWB) scales are composed of six dimensions: self-acceptance, positive relationships with others, environmental mastery, autonomy, purpose in life, and personal growth. A Likert scale ranging from 1 (I completely disagree) to 6 (I completely agree) was used to rate the items. In the original study, the PWB presented a Cronbach’s alpha of 0.91 calculated by the total 24 items’ composite index. In the present study, Cronbach’s alpha was also 0.91.
Shirom-Melamed Burnout Measure (Armon et al., 2012; Portuguese Version by Gomes, 2012)
Shirom-Melamed Burnout Measure (SMBM) is a 14-item self-reported instrument that assesses work-related burnout. It comprises three dimensions, namely: physical exhaustion, cognitive weariness, and emotional exhaustion related to work. Participants are asked to rate items using a 7-point scale (1 = never; 7 = always) with higher scores reflecting more burnout symptoms. Previous studies with this scale showed excellent reliability scores (e.g. α = 0.96 to the total score; Baganha et al., 2016). In the current study, only the total score was used to assess burnout levels, and an excellent internal consistency (Cronbach’s alpha of 0.94) was found.
Depression Anxiety and Stress Scales-21 (Lovibond & Lovibond, 1995; Portuguese Version by Pais-Ribeiro et al., 2004)
The Depression Anxiety and Stress Scales-21 (DASS-21) is a self-report instrument that encompasses three subscales measuring depressive, anxiety, and stress symptoms. Participants are asked to use a 4-point scale ranging from 0 (did not apply to me at all) to 3 (applied to me very much, or most of the time) considering the frequency of symptoms during the previous week. In the current study, only the Depression and Stress subscales were used, given that this was a pilot study and these were the two psychopathological symptoms chosen to explore psychological distress in teachers. The original study reported Cronbach’s alphas of 0.94 for Depression and 0.91 for Stress. In the present study, the Cronbach alpha values were 0.94 and 0.92 for the Depression and Stress subscales, respectively.
Compassionate Engagement and Action Scales (Gilbert et al., 2017; Portuguese Version by Matos et al., 2015)
The Compassionate Engagement and Action Scales (CEAS) encompass three scales that assess the flows of compassion according to Gilbert’s evolutionary multidimensional model of compassion and the CFT framework: (1) self-compassion, (2) compassion for others, (3) compassion from others. Each of these scales assesses (a) Compassionate Engagement (i.e. sensitivity to and motivation to engage with suffering) with items tapping into the competencies of sensitivity, sympathy, empathy, distress tolerance, non-judgement, and care for well-being; and (b) Compassionate Action (i.e. committed actions to try to alleviate and prevent suffering), with items focused on domains of helpful (1) attending, (2) thinking/reasoning, (3) behaving, and (4) emotion/feeling. The instructions for each scale present a definition of compassion. Using a 10-point Likert point scale, ranging from never (1) to always (10), participants are asked to answer how they respond when confronted by their own suffering, others’ suffering, or the experience of receiving compassion from others. In Gilbert et al. (2017), all subscales were found with acceptable-to-high reliabilities (range of 0.72 to 0.94). In this study, a Cronbach alpha of 0.90 was found for the self-compassion subscale, of 0.93 for the compassion for others subscale, and 0.96 for the receiving compassion from others subscale.
Compassion Motivation and Action Scales (Steindl et al., 2021; Portuguese Version by Matos et al., 2021)
The Compassion Motivation and Action Scales (CMAS) is a 30-item self-report measure specifically designed to assess self-compassion and compassion to others’ motivations and actions. The CMAS was developed based on a motivational interviewing approach to compassion and explores one’s desire, ability, reasons, and need for compassion for others and for oneself, as well as the commitment to compassionate and self-compassionate action and offers a measure of change in compassionate motivation and action over time. The CMAS Compassion to Others Scale encompasses 12 items addressing (1) compassion intention, (2) compassion distress tolerance, and (3) compassionate action. The CMAS Self-Compassion Scale comprises 18 items and three subscales, (1) self-compassion intention, (2) self-compassion distress tolerance, and (3) self-compassionate action. Items are rated using a 7-point scale ranging from completely disagree (1) to completely agree (7). In the original study, the Compassion to Others Scale showed a Cronbach alpha of 0.88 and the Self-Compassion Scale of 0.94. In the current study, the Compassion to Others Scale showed a Cronbach alpha of 0.87, and the Self-Compassion Scale presented a Cronbach alpha of 0.93.
Fears of Compassion Scale (Gilbert et al., 2011; Portuguese Version by Matos et al., 2016)
The Fears of Compassion Scale (FoC) has been widely used in research and clinical practice, measuring one’s fears, blocks, and resistances to compassion. It identifies barriers to giving compassion to others (10 items) and receiving compassion from others (13 items) or oneself (15 items). The items are rated on a 5-point Likert scale (0 = don’t agree at all, 4 = completely agree). The Cronbach alphas in the original study were 0.85 for fear of compassion for self, 0.87 for fear of compassion from others, and 0.78 for fear of compassion for others. In the present study, reliability values for fears of giving compassion to others, fear of receiving compassion from others, and fear of being self-compassionate were 0.92. 0.95, and 0.94, respectively.
Forms of Self-Criticism and Self-Reassurance Scale (Gilbert et al., 2004; Portuguese Version by Castilho et al., 2015)
The Forms of Self-Criticism and Self-Reassurance Scale (FSCRS) is a 22-item measure addressing the way people think and react when facing failures or setbacks. It comprises two forms of self-criticism: (1) inadequate-self and (2) hated-self and also assesses the ability to self-reassure. Respondents are asked to answer each item following the statement “When things go wrong for me…”, choosing in 5-point scale (0 = not at all like me to 4 = extremely like me) the extent to which each item relates to their experience. The original study showed a Cronbach alpha of 0.87 for self-criticism. In this study, self-criticism was calculated by summing the inadequate-self and hated-self subscales (SC-FSCRS; Halamová et al., 2018), and presented a Cronbach alpha of 0.85.
Data Analyses
Repeated measures ANOVA were performed to test differences in the outcome (teachers’ burnout, stress, depression, well-being, and satisfaction with professional life) and process (flows of compassion, compassion, self-compassion and compassion motivations and actions, self-criticism and fears of compassion) variables between pre- and post-intervention assessments. Additionally, to explore the role of self-criticism on the effects of the CMT-T intervention, repeated measures ANOVAs were also performed controlling for baseline self-criticism (as a covariate). ANOVAS’ effect sizes were calculated using partial eta square (ƞ2) and were interpreted as follows: partial ƞ2 values of 0.01 small, 0.06 medium, and 0.14 large effect sizes (Tabachnick & Fidell, 2007).
MEMORE (Mediation and Moderation analysis for Repeated measures designs) was used (Montoya & Hayes, 2017) to explore whether changes in compassion (for self, to others, and from others) and fears of compassion (for self, for others, and from others) mediated the impact of the intervention on teachers’ burnout, stress, depression, and well-being. MEMORE allows for the estimation of total, direct, and indirect effects of an independent variable (X) on a dependent variable (Y) through one or more mediators (M) simultaneously in a two-occasion within-subject design. MEMORE conceptualizes mediation analysis as a path analytic framework and not a set of discrete hypothesis tests reducing the number of tests needed to test indirect effects, which reduces the chances of inferential errors. MEMORE computes the difference between the two mediator measurements and the difference between the two dependent variable measurements (see Montoya & Hayes, 2017, for a more detailed description). In this study, all participants experienced the same CMT-T intervention and hypothesized mediators and primary outcomes were measured at baseline and post-intervention. Therefore, the independent variable “X” is the passage of time corresponding to the intervention period. Moreover, MEMORE also produces 95% confidence intervals for indirect effect(s) using bootstrapping resampling. The effect is considered statistically significant (p < 0.05) if zero is not included in the interval between the lower and the upper bound of the confidence interval (Montoya & Hayes, 2017).
Results
Acceptability
Results pertaining to the acceptability of overall assessment of the programme are presented in Table 2. The majority of teachers assessed the CMT-T as very/extremely important (91%) and found the sessions very/extremely relevant (97%) and helpful (100%), and the practices from moderately to extremely adequate (97%). Most teachers were highly motivated to attend the training (75%) and would recommend it to others (100%). The most helpful sessions were modules 4 (Working with emotions: the role of compassionate self; 31%) and 3 (Building a compassionate self; 25%). The practices rated as most helpful were soothing rhythm breathing (69%), compassion for the self (69%), safe place imagery (50%), and mindfulness (i.e. mindfulness of the senses and mindful breathing) (50%).
Implementation
No session was cancelled, and the CMT-T curriculum was fully delivered. The enrolled schools provided the necessary conditions (e.g. room for the group sessions, IT resources, after working hours schedule) for the implementation of the programme.
Practicality
The CMT-T was well-received by teachers, with no drop-outs from the intervention. The majority of the participants (77.4%; N = 24) attended ≥ five sessions. More specifically, 7 attended four sessions, 16 attended five sessions, and 8 all six sessions.
Adaptation
An earlier version of a CMT programme for teachers, comprising six sessions delivered across 12 weeks (circa 2.5 h each), was implemented with UK teachers and support staff as part of their continued professional development (Maratos et al., 2019). The CMT-T evaluated in the current study also encompassed six sessions which correspond to six distinct modules, delivered weekly (circa 2 h each) to teachers who volunteered to take part in the study. The CMT-T was developed by the UK and the Portuguese teams from the earlier version of the CMT curriculum for school staff (Maratos et al., 2019) and the brief CMT programme for the general public (Matos et al., 2017), with several adaptations introduced in the structure and content of the sessions and the practices introduced in each session (cf. the “Procedures” section for a detailed description).
Integration
A subset of participants (n = 23) indicated to use the learned practices in their everyday life: 48.4% (n = 15) reported to engage with the practices 1 to 2 times a week, 16.1% (n = 5) 3 to 4 times a week, and 9.7% (n = 3) 5 to 6 times a week. The same participants revealed that they were able to use the learned knowledge and techniques by embodying their compassionate selves in everyday life and in moments of difficulty (M = 6.76, SD = 1.70), scoring above the mean in a 1 to 10 response rate.
Preliminary Effectiveness
Repeated measures ANOVAs were performed to test differences in all variables from baseline to post-intervention. At post-intervention, participants presented increased compassion to others, compassion to others’ motivation and action, and self-compassion motivation and action. The increase in self-compassion from pre- to post-intervention approached statistical significance. Additionally, participants showed a decrease in depression and stress levels and fears of compassion for others (Table 3). All significant differences reflected large effect sizes.
Significant correlations were found between self-criticism levels at baseline and the outcome and process variables at post-intervention. Namely, self-criticism was positively correlated with burnout (r = 0.51, p = 0.005), depression (r = 0.56, p = 0.002), stress (r = 0.61, p ≤ 0.001), fears of self-compassion (r = 0.39, p = 0.030), and fears of compassion to others (r = 0.47, p = 0.009); and inversely associated with psychological well-being (r = − 0.71, p ≤ 0.005), satisfaction with teachers’ life (r = − 0.40, p = 0.030), and self-compassion (r = − 0.59, p = 0.001) and marginally correlated with compassion to others (r = − 0.35, p = 0.057). Thus, additional repeated measures ANOVAs were also conducted controlling for baseline self-criticism (Table 4). Results revealed significant time × self-criticism effects for burnout and satisfaction with teachers’ life, depressive and stress symptoms, self-compassion, and compassion to others. These results showed that when controlling for self-criticism, significant decreases in burnout, depression, and stress levels were found from baseline to post-treatment. Moreover, significant increases in satisfaction with teachers’ life, self-compassion, and compassion for others were also found.
Processes of Change Mediation Analysis
To explore the mechanisms of change on primary outcomes, two condition within-subjects’ mediation analyses were performed using the MEMORE. Changes from baseline to post-intervention in compassion (for self, to others, and from others) and fears of compassion (for self, for others, and from others) were hypothesized as possible mediators of changes in primary outcomes, namely: burnout, stress, depression, well-being, and satisfaction with teachers’ life. Changes in all outcomes were assessed from baseline to post-intervention. As we were interested in exploring each mediator process’s unique and specific contribution, all analyses were performed separately. Compassion to others and from others and fears of compassion for self and from others were not significant mediators of the intervention’s impact on teachers’ burnout, stress, depression, and well-being.
As can be seen in Table 5, only fears of compassion for others mediated the changes from baseline to post-intervention in burnout levels. Results showed that participants had lower levels of burnout post-intervention relative to baseline, through the process of the intervention’s effect on reducing their levels of fears of compassion for others. Conversely, self-compassion, and not fears of compassion, emerged as a significant mediator of the impact of the intervention on psychological well-being. This result indicated that the increase in psychological well-being after the intervention occurred through the process of the intervention’s influence on increasing participants’ self-compassion levels from baseline to post-intervention. Finally, the direct effects were both non-significant. Self-compassion and fears of self-compassion did not mediate changes found in teachers’ stress, depressive symptoms, and satisfaction with teachers’ lives.
Discussion
This pilot study aimed to test the feasibility and impact of the Compassionate Mind Training programme for Teachers (CMT-T) on symptoms of depression, stress, burnout, satisfaction with professional life, and psychological well-being, and on compassion, fears of compassion, and self-criticism. The results on all six dimensions demonstrate a high feasibility and a successful tailoring of the CMT-T. In regard to acceptability, the CMT-T was well-received and teachers evaluated the CMT-T as very/extremely important and relevant to their professional and personal lives, and all of them considered it very helpful, were highly motivated to attend, and would highly recommend it to other colleagues. These results suggest that CMT-T had positive acceptability and are in line with the ones of the earlier version of the CMT in school settings by Maratos et al. (2019). Furthermore, these feasibility results of the acceptability domain regarding the overall CMT-T evaluation mirror the findings reported in Maratos et al. (2020) pertaining to the positive ratings regarding the distinct modules’ content, delivery, and interest/relevance across the Portuguese and UK staff. It is worth noting the rating scale used in overall acceptability of the programme reported in this study had 5 response categories (from nothing to extremely), whereas in the single session evaluation, only 3 response categories were used (which varied depending on the topic being assessed, e.g. Relevant: not, somewhat, very). It is possible that this change in referenced object of judgment (single sessions versus whole intervention) and in the response category option may have led to different acceptability evaluations. In addition, the overall acceptability evaluation of the CMT-T also included the helpfulness of the sessions and the practices. Interestingly, teachers rated sessions 4 and 3 as the most helpful sessions of CMT-T. Session 4 addressed the multiple selves, how to work with different and conflicting emotions, and the compassionate self’s role. Session 3 targeted the soothing system’s cultivation and the development of the compassionate mind/self through a range of imagery practices (e.g. Safe Place, Ideal Compassionate Other or Building the Compassionate Self). The session that was rated last in terms of helpfulness was session 2, which was a more psychoeducation-based module, focused on the function of emotions and three affect regulation systems. The practices rated as the most helpful by the teachers were the soothing rhythm breathing and compassion for the self, followed by the safe place imagery and mindfulness. The practice rated by fewer participants as most helpful was the Ideal Compassionate Other. These findings extend Maratos et al.’s (2019) work in the evaluation of the earlier version of the CMT in school settings by adding relevant information about the overall assessment of modules and practices’ helpfulness. Moreover, these data expand the current knowledge regarding the assessment of CMT interventions with community samples (e.g. Irons & Heriot-Maitland, 2020; Matos et al., 2017, 2018). Importantly, these results offer pertinent acceptability feedback that should be incorporated towards the CMT-T refinement to better implement and further evaluate the programme in future studies. The CMT-T revealed adequate implementation, practicality, and adaptation. Furthermore, participants were able to use and integrate the knowledge and techniques learned during the programme in their everyday life, suggesting a positive integration of the CMT-T.
The CMT-T focuses on the cultivation of the compassionate mind to help teachers deal with life’s adversities, improve their capacities to regulate distressing/conflicting emotions, work with their self-criticism, promote positive interpersonal relationships, and ultimately foster their well-being and physical and mental health (Gilbert et al., 2020; Maratos et al., 2020). It encompasses psychoeducation and a set of experiential exercises adapted from CFT (Gilbert, 2010). The development of a compassionate mind encompasses the development of the three flows of compassion: self-compassion, compassion to others, and one’s openness to receive compassion from others. Regarding the CMT-T’s impact on self-compassion, when comparing baseline to post-intervention, significant increases in self-compassion motivations and actions (as measured by the CMAS) were found with large effect sizes. This indicates that, after the CMT-T, teachers improved their motivation to engage with life’s hardships and suffering with an accepting and caring attitude towards the self, instead of denying, withdrawing, or avoiding them. They also showed a greater ability to tolerate distress concerning oneself and be kind and supportive when facing difficulties.
Moreover, teachers revealed an increased capacity to act compassionately towards themselves and to be caring, gentle, and forgiving to themselves in the face of distress. Interestingly, this expands the results of an earlier version of this training (Maratos et al., 2019) where self-compassion changes, as measured by a different questionnaire (Self-Compassion Scale (SCS); Neff, 2003), were only significant when associated with increased practice. Therefore, these findings support the beneficial effects of this novel CMT-T (developed based on this earlier version) in promoting compassionate motivations and behaviours towards the self. It is worth noting that these results are in line with previous studies that show the positive impacts of CMT on self-compassion engagement and action in community samples (Irons & Heriot-Maitland, 2020; Matos et al., 2017). However, in these studies, these significant changes were found in the CEAS self-compassion scale, whereas in the current study, changes in this measure did not reach statistical significance. It is possible that the development of self-compassion attributes and competencies (as measured by the CEAS) might take longer to manifest than the motivation to be accepting and caring and take concrete compassionate actions towards oneself (as assessed by the CMAS). Our results are also in support of studies that found significant improvements in self-compassion (as measured by the SCS) post-CMT training in other professions, such as health care educators and providers (Beaumont et al., 2016b), psychotherapy students (Beaumont et al., 2017), and firefighters (Beaumont et al., 2016a).
The CMT-T also focuses on the development of compassion to others (Gilbert, 2014, 2020). In the current study, teachers revealed significant increases in compassion to others (as measured by the CEAS), and in compassion motivation and action towards others (as assessed by the CMAS), as well as significant reductions in fears of compassion to others, from pre- to post-intervention, with large effect sizes. This suggests that the CMT-T seems to be effective, not only in diminishing teachers’ fears, blocks, and resistances of being compassionate to others, but also in fostering their willingness and competencies to engage with other people’s suffering through the development of motivation to care, sensitivity to distress, sympathy, distress tolerance, empathy, and non-judgement (Gilbert, 2014, 2020). In addition, teachers were able to work with others’ distress skillfully and to take action in helpful ways to prevent or alleviate their suffering.
The current findings extend the results from studies using CMT with teachers (Maratos et al., 2019), and with other professions (e.g. health care educators and providers, Beaumont et al., 2016b; fire service personnel, Beaumont et al., 2016a), where this flow of compassion was not assessed, and go beyond previous research that did not find significant changes in compassion to others when using CMT with psychotherapy students (Beaumont et al., 2017), and after an 8-week CMT (Irons & Heriot-Maitland, 2020) and a brief CMT (Matos et al., 2017) with community samples, possibly due to ceiling effects. Nevertheless, in our study, albeit participants’ scores in compassion to others (as measured by the CEAS) were higher than the other flows, there were still significant increases. Additionally, although previous research has indicated that the relationship between self-compassion and compassion to others is not straightforward, and one might be able to be compassionate towards others but struggle to be self-compassionate (Lopez et al., 2018), in our study, these two flows of compassion concurrently improved post-CMT-T. One may hypothesize that the specificity of the target population and the context in which the CMT-T was implemented may facilitate teachers’ conditions to develop the attributes and practise the competencies of compassion towards other people, as well as for themselves. The CMT-T may thus contribute to the weakening of the barriers to compassion and the building of more compassionate relationships, particularly in the school setting (e.g. colleagues, pupils, staff), which was also reflected in the acceptability feedback provided by the participants in the sessions.
In terms of receiving compassion from others, and contrarily to what was reported in previous studies in community samples (Matos et al., 2017), no significant changes were found from pre- to post-CMT-T. It is important to note that compassion from others, as measured by the CEAS, evaluates how one perceives other people’s motivation and ability to engage with one’s suffering and to take action to alleviate one’s distress, and not one’s ability to be open and willing to receive compassion from others. Even though CMT-T does not directly target the former, one would expect an increase in the later, that is, in one’s openness to be the recipient of compassion from others, which could be reflected in a decrease in the fears of compassion from others. However, although we can see an increase in how participants felt others being compassionate towards them and a decrease in their fear of compassion from others, from before to after the CMT-T, these changes did not reach statistical significance. These results are in line with what Irons and Heriot-Maitland (2020) found in a community sample, and might be related to the limited sample size of this study. Our findings expand upon previous studies using CMT with teachers (Maratos et al., 2019) and other professionals (Beaumont et al., 2016a, b, 2017), where this flow of compassion was not evaluated. Nonetheless, this is a relevant finding for the CFT model and should be considered in future developments and the CMT-T implementation. It seems one may remain relatively blocked from other people’s caring minds even if they are able to develop greater compassion for themselves and others. Given that the three flows of compassion remain relatively unexplored in current CMT research, and considering the emerging evidence supporting the relevance of compassion from others to mental health (e.g. Kirby et al., 2019), future studies should examine the impact of CMT on this particular flow of compassion, both in larger teachers’ samples and in samples from the general community and other professions.
Regarding the impact of the CMT-T on the outcome measures, specifically on psychological distress, when comparing baseline to post-intervention, significant decreases were found in teachers’ depression and stress levels with large effect sizes. These findings are in line with previous CMT and CFT studies, which found similar results for these psychopathological indicators, namely with community samples (Irons & Heriot-Maitland, 2020; Matos et al., 2017) and other professionals (i.e. firefighters, Beaumont et al., 2016a). Besides, these results extend Maratos et al.’s (2019) feasibility study, where thematic analyses revealed benefits of CMT for dealing with emotional difficulties. Still, quantitative data did not reach criteria for statistical significance. Other outcome measures of the current study were burnout, psychological well-being, and satisfaction with teachers’ professional life, but no significant changes were found on these indicators.
Similar to the current study, in the earlier version of CMT for school staff (Maratos et al., 2019), no significant changes were found from pre- to post-intervention in burnout dimensions of emotional exhaustion and personal accomplishment. Concerning well-being, previous studies have indeed reported significant increases in positive affect after a CMT intervention, particularly in feelings of safeness, contentment, and relaxation (Irons & Heriot-Maitland, 2020; Matos et al., 2017). However, the impact of CMT on these specific burnout and well-being indicators was not evaluated in these studies.
In fact, other psychological processes might be influencing and explaining these results, and thus require further exploration. One of these processes is self-criticism, which may play a key role in shaping the potential effects of compassion and self-compassion on well-being (Duarte et al., 2019; Matos et al., 2017). Self-criticism has been found to be associated with a range of negative intrapersonal (e.g. shame, rumination, worry, poor emotion regulation skills) and interpersonal (e.g. submissive behaviour, aggression) factors in non-clinical populations, as well as with lower levels of well-being, life satisfaction, and greater mental distress (e.g. Pinto-Gouveia et al., 2013; Werner et al., 2019). However, in the current study and contrarily to our predictions and results from previous studies using CMT interventions in community samples (Irons & Heriot-Maitland, 2020; Matos et al., 2017; Sommers-Spikerman et al., 2018), and other professional groups (e.g. psychotherapy students, Beaumont et al., 2017; health care educators and providers, Beaumont et al., 2016b), changes in self-criticism from pre- to post-intervention were not significant. Comparably, Maratos et al. (2019) reported that self-criticism changes were also not significant after the CMT for school staff, but were positively linked to practice. A possible explanation for this non-significant finding might be that self-criticism was only directly addressed in the CMT-T later in the programme, in session 5, and a substantial number of participants did not attend this session (25.8%, N = 8). Hence, this might have influenced a lack of systematic integration by the teachers of knowledge on the functional analysis of self-criticism and strategies to use the compassionate self to work with self-criticism when things go wrong, or they make mistakes.
Notably, previous studies have documented the role of individual differences in self-criticism on individuals’ responses to compassion-based interventions (e.g. Duarte et al., 2015; Longe et al., 2010). Moreover, a pathway through which compassion might operate to promote well-being and reduce mental distress is via reducing self-criticism (Duarte et al., 2019; Matos et al., 2017). Taken together our findings and these considerations, we examined how baseline self-criticism was associated with the other variables at post-intervention. The results revealed that levels of self-criticism at baseline were indeed positively linked to post-intervention levels of burnout, depression, stress, fears of self-compassion, and fears of compassion to others; and negatively associated with psychological well-being, satisfaction with teachers’ life, and self-compassion, and marginally with compassion to others. Furthermore, when baseline self-criticism was controlled for, significant interaction effects were found for burnout and depressive symptoms, satisfaction with teachers’ life, self-compassion, and compassion for others (as measures by the CEAS). Thus, aside from the overall effects of the CMT-T reported above, when self-criticism was controlled for, teachers revealed further decreases in burnout and increases in their satisfaction with their professional lives, and they showed greater self-compassion (as measured by the CEAS) from baseline to post-intervention. This points to the key role self-criticism may play in how CMT-T operates in developing teachers’ abilities to be compassionate towards themselves, thus fostering their well-being and diminishing mental distress. These data also provide further support to previous research that has already documented that individuals high on self-criticism tend to respond to CMT practices with threat-based physiological responses (Duarte et al., 2015; Longe et al., 2010; Rockliff et al., 2011). Therefore, these results suggest that it may be critical to address and work with self-criticism throughout a CMT intervention in order for changes in self-compassion and well-being indicators to be facilitated. Importantly, this emphasizes the need to incorporate these findings in future refinements of the CMT-T (and other CMT interventions), particularly in terms of assessing and working with self-criticism earlier in the programme and address it throughout the sessions.
Overall, these results support the preliminary effectiveness of the CMT-T and, together with findings regarding the other five feasibility criteria discussed above, provide evidence that the CMT-T is a feasible intervention for teachers. Taken together, our findings highlight that using a compassion-focused intervention, like CMT-T, in educational settings, might be particularly relevant to address teachers’ psychological distress, burnout, and low occupational well-being (OFSTED, 2019; Varela et al., 2018) arising from the many challenges they face on a daily bases, such as self- and other-focused competitive pressures, heavy workloads, achievement focus, performance evaluation, and pupils’ behavioural problems (Gilbert et al., 2020). The CMT-T seems to mitigate the resistances to compassion and facilitate the cultivation of teachers’ self-compassion competencies, motives and actions, and the enhancement of their compassionate abilities, motives, and actions towards others. Tentatively, this shift to more compassion-focused motives, in relation to oneself and to others, may allow teachers to better regulate their emotions and cope with these sources of psychological distress, which seems to be reflected in the reduced levels of depression, stress, and burnout and increased satisfaction with professional life found at post-CMT-T. Another key goal from the present study was to obtain some knowledge of the processes that mediate intervention changes. Gathering this information is of paramount importance (e.g. McCracken & Gutiérrez-Martínez, 2011) as it will allow to develop further and enhance the effectiveness of the CMT-T intervention. Overall, results showed that the decrease in teachers’ burnout levels after the CMT-T intervention was mediated by decreased levels of fears of compassion for others. Thus, it seems that reducing teachers’ resistances in being caring, tolerant, kind, and compassionate towards others as a result of the CMT-T intervention was an important process to reduce teachers’ burnout levels. On the other hand, the intervention effect on teachers’ psychological well-being was fully mediated by the increase in teachers’ ability to be more self-compassionate. These results suggest that practising the ability to be warm and caring towards oneself throughout the intervention may play a crucial role in increasing well-being among teachers. Taken together, these exploratory findings point to the importance of targeting fears of compassion for others and self-compassion abilities in schools to decrease distress and promote psychological well-being among teachers. By reducing teachers’ resistance towards compassion alongside cultivating their self-compassion and genuinely embodying their compassionate self, teachers may make a unique contribution to foster more compassionate schools.
Limitations and Future Research
Given the exploratory nature of this pilot study, focused on feasibility and preliminary effectiveness of this novel 6-module CMT group intervention for teachers, we did not have a control group to compare the changes here reported. This limits the extrapolation of the causes of these changes and the comparison of our findings to the effects that might arise from attendance of other courses tailored for the same target population (e.g. CARE for teachers, CASEL). The limited sample size and lack of control group could also be considered additional reasons for finding effects that were not found in similar studies and vice versa (e.g. Maratos et al., 2019). Future studies should integrate the findings outlined in this article to refine further and improve the CMT-T programme and conduct a randomized controlled trial comparing the CMT-T with a larger sample and a suitable control group to establish causality and the significance of effects. Previous research has shown that practice frequency (Maratos et al., 2019), practice helpfulness, and the embodiment of the compassionate self in everyday life may be key in promoting changes in a CMT intervention (Matos et al., 2018). In the future, studies should explore the impact of these practice indicators on the effectiveness of the CMT-T. Social desirability may also have impacted participants’ responses on the acceptability questionnaire regarding the overall programme evaluation. Another aspect relates to the length of the programme. Both participants’ qualitative feedback and the facilitators’ experience running the CMT-T hinted that more time might be necessary to allow for slower paced learning and more systematic integration of the knowledge and practices in everyday life. Thus, it might be fitting to consider in future iterations of the CMT-T extending the number of sessions (8 instead of 6, for example) whilst maintaining the same modules and exploring how this might affect the feasibility and impact of the intervention. It would also be pertinent for future research to investigate the stability of the changes after the CMT-T by including a follow-up assessment moment.
Moreover, future studies should employ a mixed-methods approach to test the efficacy of the CMT-T, encompassing self-report psychological measures, as well as physiological indicators, such as heart rate variability, which has been proposed as a crucial outcome measure for compassion-based interventions in general (due to its connection to vagal regulatory activity, and its link to overall health and well-being), and for CMT in particular (Kim et al., 2020; Matos et al., 2017). Another relevant assessment methodology that could be employed to explore the appropriateness of the intervention is focus groups. In the future, this element could be included in CMT-T-related research to supplement the in-depth understanding of the impact of the intervention and of possible moments and mechanisms of change. Finally, because we aimed to specifically track the impact of the six CMT-T sessions, unlike other similar courses (e.g. Mindful Self-Compassion, MBSR), we did not have a half-day/day-long retreat. In the future, it may be helpful to incorporate a half-day/day-long retreat in the programme.
The current pilot study presents promising data demonstrating the possible benefits of the CMT-T in school settings in promoting teachers’ compassion-focused motivations, attitudes, and actions, and possibly fostering the creation of safe, collaborative, and encouraging educational environments. The CMT-T seems to be a feasible and useful intervention to promote teachers’ professional satisfaction and compassionate motivations, attributes, and actions (towards others and oneself) and reduce burnout, depression, and stress symptoms. Our findings further suggest the importance of targeting teachers’ self-criticism across the programme to improve its beneficial impact on teachers’ well-being.
Data Availability
The data that support the findings of this study are available upon reasonable request from the authors.
Change history
05 February 2022
A Correction to this paper has been published: https://doi.org/10.1007/s12671-022-01833-7
11 December 2021
A Correction to this paper has been published: https://doi.org/10.1007/s12671-021-01796-1
References
Albuquerque, I., Matos, M., Figueiredo, C. & Lima, M.C. (2021). Pursuing a better understanding of psychological well-being: Confirmatory factor analyses in a Portuguese sample. [Manuscript in preparation]. Center for Research in Neuropsychology and Cognitive and Behavioural Intervention (CINEICC), University of Coimbra.
Albuquerque, I., Palmeira, L., Lima, M.P., Cunha, M., Galhardo, A. & Matos, M., (2021). Measuring the satisfaction with professional life of teachers: Psychometric validation in a Portuguese sample. [Manuscript in preparation]. Center for Research in Neuropsychology and Cognitive and Behavioural Intervention (CINEICC), University of Coimbra.
Armon, G., Shirom, A., & Melamed, S. (2012). The Big Five personality factors as predictors of changes across time in burnout and its facets. Journal of Personality, 80(2), 403–427. https://doi.org/10.1111/j.1467-6494.2011.00731.x
Baganha, C., Gomes, A. R., & Esteves, A. (2016). Stresse ocupacional, avaliação cognitiva, burnout e comprometimento laboral na aviação civil. Psicologia, Saúde & Doenças, 17(2), 164–179. https://doi.org/10.15309/16psd170212
Basran, J., Pires, C., Matos, M., McEwan, K., & Gilbert, P. (2019). Styles of leadership, fears of compassion, and competing to avoid inferiority. Frontiers in Psychology, 9, 2460. https://doi.org/10.3389/fpsyg.2018.02460
Beaumont, E., Irons, C., Rayner, G., & , Dagnall, N. . (2016b). Does compassion-focused therapy training for health care educators and providers increase self-compassion and reduce self-persecution and self-criticism? Journal of Continuing Education in the Health Professions, 36(1), 4–10. https://doi.org/10.1097/CEH.0000000000000023
Beaumont, E., Rayner, G., Durkin, M., & Bowling, G. (2017). The effects of Compassionate Mind Training on student psychotherapists. The Journal of Mental Health Training, Education and Practice, 12(5), 300–312. https://doi.org/10.1108/JMHTEP-06-2016-0030
Beaumont, E., & Martin, C. J. H. (2016). Heightening levels of compassion towards self and others through use of compassionate mind training. British Journal of Midwifery 24(11), 777–786. https://doi.org/10.12968/bjom.2016.24.11.777
Beaumont, E., Durkin, M., McAndrew, S., & Martin, C. (2016a). Using compassion focused therapy as an adjunct to trauma-focused CBT for fire service personnel suffering with trauma-related symptoms. The Cognitive Behaviour Therapist, 9.https://doi.org/10.1017/S1754470X16000209
Bowen, D. J., Kreuter, M., Spring, B., Cofta-Woerpel, L., Linnan, L., Weiner, D., et al. (2009). How we design feasibility studies. American Journal of Preventive Medicine, 36(5), 452–457. https://doi.org/10.1016/j.amepre.2009.02.002
British Psychological Society (2018). Code of ethics and conduct. The British Psychological Society
Carter, S., Bartal, I. B., & Porges, E. (2017). The roots of compassion: An evolutionary and neurobiological perspective. In E. M. Seppälä, E. Simon-Thomas, S. L. Brown, M. C. Worline, C. D. Cameron, & J. R. Doty (Eds.), The Oxford handbook of compassion science (pp. 178–188). Oxford University Press.
Castilho, P., Pinto-Gouveia, J., & Duarte, J. (2015). Exploring self-criticism: Confirmatory factor analysis of the FSCRS in clinical and non-clinical samples. Clinical Psychology & Psychotherapy, 22(2), 153–164. https://doi.org/10.1002/cpp.1881
Coles, M. I. (2015). Towards the compassionate school. Trentham Books.
Colonnello, V., Petrocchi, N., Farinelli, M., & Ottaviani, C. (2017). Positive social interactions in a lifespan perspective with a focus on opioidergic and oxytocinergic systems: Implications for neuroprotection. Current Neuropharmacology, 15(4), 543–561. https://doi.org/10.2174/1570159X14666160816120209
Craig, C., Hiskey, S., & Spector, A. (2020). Compassion focused therapy: A systematic review of its effectiveness and acceptability in clinical populations. Expert Review Neurotherapeutics, 385-400.https://doi.org/10.1080/14737175.2020.1746184
Cunha, M., Matos, M., Faria, D., & Zagalo, S. (2012). Shame memories and psychopathology in adolescence: The mediator effect of shame. International Journal of Psychology and Psychological Therapy, 12(2), 203–218.
Diener, E. D., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49(1), 71–75. https://doi.org/10.1207/s15327752jpa4901_13
Duarte, J., McEwan, K., Barnes, C., Gilbert, P., & Maratos, F. A. (2015). Do therapeutic imagery practices affect physiological and emotional indicators of threat in high self-critics? Psychology and Psychotherapy: Theory, Research and Practice, 88(3), 270–284. https://doi.org/10.1111/papt.12043
Duarte, C., Gilbert, P., Stalker, C., Catarino, F., Basran, J., Scott, S., ..., Stubbs, R. J. (2019). Effect of adding a compassion focused intervention on emotion, eating and weight outcomes in a commercial weight management programme. Journal of Health Psychology, 33(3). https://doi.org/10.1177/2F1359105319890019
ESP (2018) Teacher well-being index. Retrieved from: https://www.educationsupportpartnership.org.uk/sites/default/files/resources/teacher_wellbeing_index_2018.pdf [Last accessed 05.03.2020].
Gilbert, P. (2014). The origins and nature of compassion focused therapy. British Journal of Clinical Psychology, 53(1), 6–41. https://doi.org/10.1111/bjc.12043
Gilbert, P. (2020). Compassion: From its evolution to a psychotherapy. Frontiers in Psychology, 11, 3123.
Gilbert, P., Clarke, M., Hempel, S., Miles, J. N., & Irons, C. (2004). Criticising and reassuring oneself: An exploration of forms, styles and reasons in female students. British Journal of Clinical Psychology, 43, 31–50. https://doi.org/10.1348/014466504772812959
Gilbert, P., McEwan, K., Matos, M., & Rivis, A. (2011). Fears of compassion: Development of three self-report measures. Psychology and Psychotherapy: Theory, Research and Practice, 84, 239–255. https://doi.org/10.1348/147608310X526511
Gilbert, P., Matos, M., Wood, W., & Maratos, F. (2020). The compassionate mind and the conflicts between competing and caring: Implications for educating young minds. In M. I. Coles & B. Gent (Eds.), Education for survival: The pedagogy of compassion (pp. 44–76). Trentham Books.
Gilbert, P., Catarino, F., Duarte, C., Matos, M., Kolts, R., Stubbs, J., ..., & Basran, J. (2017). The development of compassionate engagement and action scales for self and others. Journal of Compassionate Health Care, 4(1), 4. https://doi.org/10.1186/s40639-017-0033-3
Gilbert, P. (2009). The compassionate mind: A new approach to facing the challenges of life. Constable Robinson.
Gilbert, P. (2010). Compassion focused therapy: Distinctive features. Routledge.
Gomes, A. R. (2012). Medida de “Burnout” de Shirom-Melamed (MBSM). Relatório técnico não publicado.
Hakanen, J. J., Bakker, A. B., & Schaufeli, W. B. (2006). Burnout and work engagement among teachers. Journal of School Psychology, 43(6), 495–513. https://doi.org/10.1016/j.jsp.2005.11.001
Halamová, J., Kanovský, M., Kupeli, N., Gilbert, P., Troop, N., Zuroff, D., Hermanto, N., Petrocchi, N., Sommers-Spijkerman, M., Kirby, J., Shahar, B., Krieger, T., Matos, M., Asano, K., Yu, F., & Basran, J. (2018). The factor structure of the forms of self-criticising, attacking & self-reassuring scale in thirteen distinct populations. Journal of Psychopathology and Behavioral Assessment., 40(4), 736–751. https://doi.org/10.1007/s10862-018-9686-2
Hoglund, W. L. G., Klingle, K. E., & Hosan, N. E. (2015). Classroom risks and resources: Teacher burnout, classroom quality and children’s adjustment in high needs elementary schools. Journal of School Psychology, 53(5), 337–357. https://doi.org/10.1016/j.jsp.2015.06.002
Irons, C., & Beaumont, E. (2017). The compassionate mind workbook: A step-by-step guide to developing your compassionate self. Robinson.
Irons, C., & Heriot-Maitland, C. (2020). Compassionate Mind Training: An 8-week group for the general public. Psychology and Psychotherapy: Theory, Research and Practice. https://doi.org/10.1111/papt.12320
Katz, D. A., Greenberg, M. T., Klein, L. C., & Jennings, P. A. (2016). Associations between salivary α-amylase, cortisol and self-report indicators of health and well-being among educators. Teacher and Teacher Education, 54, 98–106. https://doi.org/10.1016/j.tate.2015.11.012
Kim, J. J., Parker, S. L., Doty, J. R., Cunnington, R., Gilbert, P., & Kirby, J. N. (2020). Neurophysiological and behavioural markers of compassion. Scientific Reports, 10(1), 1–9. https://doi.org/10.1038/s41598-020-63846-3
Kirby, J. N. (2017). Compassion interventions: The programmes, the evidence, and implications for research and practice. Psychology and Psychotherapy: Theory, Research and Practice, 90, 432–455. https://doi.org/10.1111/papt
Kirby, J. N., Tellegen, C. L., & Steindl, S. R. (2017). A meta-analysis of compassion-based interventions: Current state of knowledge and future directions. Behavior Therapy, 48, 778–792. https://doi.org/10.1016/j.beth.2017.06.003
Kirby, J. N., Day, J., & Sagar, V. (2019). The ‘Flow’ of compassion: A meta-analysis of the fears of compassion scales and psychological functioning. Clinical Psychology Review, 70, 26–39. https://doi.org/10.1016/j.cpr.2019.03.001
Lavelle, B.D (2017). Compassion in schools. In Seppälä, E. M., Simon-Thomas, E., Brown, S. L., Worline, M. C., Cameron, C. D., & Doty, J. R. (Eds.). (2017). The Oxford handbook of compassion science. Oxford University Press.
Leaviss, J., & Uttley, L. (2015). Psychotherapeutic benefits of compassion-focused therapy: An early systematic review. Psychological Medicine, 45, 927–945. https://doi.org/10.1017/S0033291714002141
Liu, S., & Onwuegbuzie, A. J. (2012). Chinese teachers’ work stress and their turnover intention. International Journal of Educational Research, 53, 160–170. https://doi.org/10.1016/j.neuroimage.2009.09.019
Longe, O., Maratos, F. A., Gilbert, P., Evans, G., Volker, F., Rockliff, H., & Rippon, G. (2010). Having a word with yourself: Neural correlates of self-criticism and self-reassurance. NeuroImage, 49(2), 1849–1856. https://doi.org/10.1016/j.neuroimage.2009.09.019
Lopez, A., Sanderman, R., Ranchor, A. V., & Schroevers, M. J. (2018). Compassion for others and self-compassion: Levels, correlates, and relationship with psychological well-being. Mindfulness, 9, 325–331. https://doi.org/10.1007/s12671-017-0777-z
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335–343. https://doi.org/10.1016/0005-7967(94)00075-U
Maratos, F. A., Montague, J., Ashra, H., Welford, M., Wood, W., Barnes, C., Sheffield, D., & Gilbert, P. (2019). Evaluation of a Compassionate Mind Training intervention with school teachers and support staff. Mindfulness, 10, 2245–2258. https://doi.org/10.1007/s12671-019-01185-9
Maratos, F., Matos, M., Albuquerque, I., Wood, W., Palmeira, L., Cunha, M., Lima, M. P., & Gilbert, P. (2020). Exploring the international utility of progressing Compassionate Mind Training in school settings: A comparison of implementation effectiveness of the same curricula in the UK and Portugal. Psychology of Education Review, 44(2), 73–82. http://hdl.handle.net/10545/625433
Matos, M., Duarte, C., Duarte, J., Pinto-Gouveia, J., Petrocchi, N., Basran, J., & Gilbert, P. (2017). Psychological and physiological effects of compassionate mind training: A pilot randomised controlled study. Mindfulness, 8(6), 1699–1712. https://doi.org/10.1007/s12671-017-0745-7
Matos, M., Duarte, C., Duarte, J., Gilbert, P., & Pinto-Gouveia, J. (2018). How one experiences and embodies compassionate mind training influences its effectiveness. Mindfulness, 9(4), 1224–1235. https://doi.org/10.1007/s12671-017-0864-1
Matos, M., Pinto-Gouveia, J., Duarte, C., & Duarte, J. (2015). Portuguese translation of the compassionate engagement and action scales for self and others. [Unpublished manuscript]. Center for Research in Neuropsychology and Cognitive and Behavioural Intervention (CINEICC), University of Coimbra.
Matos, M., Pinto-Gouveia, J., Duarte, J., & Simões, D. (2016). Portuguese translation of the fears of compassion scales. [Unpublished manuscript]. Center for Research in Neuropsychology and Cognitive and Behavioural Intervention (CINEICC), University of Coimbra.
Matos, M., Gonçalves, E., Palmeira. L., Melo, I., Steindl, S., & Gomes, A. (2021). Advancing the Assessment of Compassion: Psychometric Study of the Compassion Motivation and Action Scales in a Portuguese Sample. Current Psychology. https://doi.org/10.1007/s12144-021-02311-4
McCallum, F., Price, D., Graham, A., & Morrison, A. (2017). Teacher well-being: A review of the literature. The Association of Independent Schools of New South Wales Limited.
McCracken, L. M., & Gutiérrez-Martínez, O. (2011). Processes of change in psychological flexibility in an interdisciplinary group-based treatment for chronic pain based on Acceptance and Commitment Therapy. Behaviour Research and Therapy, 49(4), 267–274. https://doi.org/10.1016/j.brat.2011.02.004
McLean, L., & Connor, C. M. (2015). Depressive symptoms in third-grade teachers: Relations to classroom quality and student achievement. Child Development, 86(3), 945–954. https://doi.org/10.1111/cdev.12344
Montoya, A. K. & Hayes, A. F. (2017). Two conditions within-participant statistical mediation analysis: A path-analytic framework. Psychological Methods, 22(1). https://doi.org/10.1037/met0000086
NASUWT. (2016). The Big Question 2016: An opinion survey of teachers and school leaders. https://www.nasuwt.org.uk/uploads/assets/uploaded/7649b810-30c7-4e93-986b363487926b1d.pdf
Neff, K. D. (2003). The development and validation of a scale to measure self-compassion. Self and Identity, 2(3), 223–250. https://doi.org/10.1080/15298860309027
Oberle, E., & Schonert-Reichl, K. A. (2016). Stress contagion in the classroom? The link between classroom teacher burnout and morning cortisol in elementary school students. Social Science & Medicine, 159, 30–37. https://doi.org/10.1016/j.socscimed.2016.04.031
OFSTED (2019). Teacher well-being at work in schools and further education providers. Retrieved from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/819314/Teacher_well-being_report_110719F.pdf
Pais-Ribeiro, J. L., Honrado, A., & Leal, I. (2004). Contribuição para o estudo da adaptação portuguesa das escalas de ansiedade, depressão e stress (EADS) de 21 itens de Lovibond e Lovibond. Psicologia, Saúde & Doenças, 5(2), 229–239.
Peterson, A. (2017). Compassion and education: Cultivating compassionate children, schools and communities. Palgrave.
Petrocchi, N., & Cheli, S. (2019). The social brain and heart rate variability: Implications for psychotherapy. Psychology and Psychotherapy, 92, 208–223. https://doi.org/10.1111/papt.12224
Pinto-Gouveia, J., Castilho, P., Matos, M., & Xavier, A. (2013). Centrality of shame memories and psychopathology: The mediation effect of self-criticism. Clinical Psychology: Science and Practice, 20, 323–334. https://doi.org/10.1111/cpsp.12044
Rockliff, H., Karl, A., McEwan, K., Gilbert, J., Matos, M., & Gilbert, P. (2011). Effects of intranasal oxytocin on compassion focused imagery. Emotion, 11(6), 1388–1396. https://doi.org/10.1037/a0023861
Rockliff, H., Gilbert, P., McEwan, K., Lightman, S., & Glover, D. (2008). A pilot exploration of heart rate variability and salivary cortisol responses to compassion-focused imagery. Journal of Clinical Neuropsychiatry, 5, 132–139. http://hdl.handle.net/10545/622861
Rodway, C., Tham, S. G., Ibrahim, S., Turnbull, P., Windfuhr, K., Shaw, J., & Appleby, L. (2016). Suicide in children and young people in England: A consecutive case series. The Lancet Psychiatry, 3(8), 751–759.
Roeser, R. W., Collaianne, B. A., & Greenberg, M. A. (2018). Compassion and human development: Current approaches and future directions. Research in Human Development. https://doi.org/10.1080/15427609.2018.1495002
Ryff, C. D., & Essex, M. J. (1992). The interpretation of life experience and well-being: The sample case of relocation. Psychology and Aging, 7(4), 507. https://doi.org/10.1037/0882-7974.7.4.507
Schonfeld, I., Bianchi, R., & Luehring-Jones, P. (2017). Consequences of job stress for the mental health of teachers. In M. McIntyre et al. (Eds.), Educator stress, aligning perspectives on health, safety and well-being. Springer. https://doi.org/10.1007/978-3-319-53053-6_3
Sommers-Spijkerman, M. P. J., Trompetter, H. R., Schreurs, K. M. G., & Bohlmeijer, E. T. (2018). Compassionfocused therapy as guided self-help for enhancing public mental health: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 86(2), 101–115. https://doi.org/10.1037/ccp0000268
Steindl, S. R., Tellegen, C. L., Filus, A., Seppala, E., Doty, J. R., & Kirby, J. N. (2021). The Compassion Motivation and Action Scales: A self-report measure of compassionate and self-compassionate behaviours. Australian Psychologist. https://doi.org/10.1080/00050067.2021.1893110
Tabachnick, B., & Fidell, L. (2007). Using multivariate statistics. Pearson Education Inc.
Travers, C. (2017). Current knowledge on the nature, prevalence, sources and potential impact of teacher stress. Educator Stress, 23-54.https://doi.org/10.1007/978-3-319-53053-6_2
Varela, R. C., della Santa, R., Silveira, H., Coimbra de Matos, A., Rolo, D., Areosa, J., & Leher, R. (2018). Inquérito nacional sobre as condições de vida e trabalho na educação em Portugal (INCVTE). Jornal da FENPROF. Retrieved from https://www.fenprof.pt/?aba=39&cat=667
Welford, M., & Langmead, K. (2015). Compassion-based initiatives in educational settings. Educational and Child Psychology, 32(1), 71–80.
Werner, A. M., Tibubos, A. N., Rohrmann, S., & Reiss, N. (2019). The clinical trait self-criticism and its relation to psychopathology: A systematic review - Update. Journal of Affective Disorders, 246, 530–547. https://doi.org/10.1016/j.jad.2018.12.069
Wetherall, K., Robb, K. A., & O’Connor, R. C. (2019). Social rank theory of depression: A systematic review of self-perceptions of social rank and their relationship with depressive symptoms and suicide risk. Journal of Affective Disorders, 246, 30–39. https://doi.org/10.1016/j.jad.2018.12.045
Acknowledgements
The authors would like to thank the educational institution that collaborated with this project and the teachers for their kind participation.
Funding
This work has received funding and support from Sarah and John Rockliff and the Reed Foundation (UK) and supported by the Compassionate Mind Foundation (UK).
Author information
Authors and Affiliations
Contributions
MM, LP, IA, MC, MPL, FM, and PG designed the study. MM, LP, IA, MC, and MPL executed the study and conducted the data analyses. MM, LP, IA, MC, MPL, and AG wrote the original and final draft of the manuscript. PG collaborated with the review and editing of the final draft. All authors approved the final version of the manuscript. MM, FM, and PG were responsible for the funding acquisition that supported the current study. MM, LP, IA, FM, and PG developed the resources and materials used in the current study. The study was supervised by MM, FM, and PG.
Corresponding author
Ethics declarations
Ethics Approval
The authors declare that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975 and its later amendments. The Ethics Committee of the Faculty of Psychology and Educational Sciences of the University of Coimbra approved the study (CEDI22.03.2018).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised to update the author name of Marcela A. Matos to Marcela Matos.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Matos, M., Palmeira, L., Albuquerque, I. et al. Building Compassionate Schools: Pilot Study of a Compassionate Mind Training Intervention to Promote Teachers’ Well-being. Mindfulness 13, 145–161 (2022). https://doi.org/10.1007/s12671-021-01778-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-021-01778-3