
Abstract
Objectives
Anterior alpha asymmetry is an EEG measure of relative left- or right-sided prefrontal cortical activity that has been associated with affective style, such that greater relative left-sided activity is associated with positive affect and approach-related behaviours. While mindfulness has been shown to enhance attention and affect, here we investigate the underlying neurobiological changes supporting these outcomes by assessing anterior alpha asymmetry.
Methods
A longitudinal RCT was conducted to investigate the effect of an 8-week mindfulness training (MT) intervention on anterior alpha asymmetry and affect in a group of healthy adults aged over 60 years (n = 41). An active control computer-based attention training (CT) program (n = 26) designed to activate similar attentional components to mindfulness was used to determine if outcomes resulted from attention training or mindfulness-specific factors. The Sustained Attention to Response Task was used to assess attentional performance, while a breath counting task was used to classify mindfulness participants into high (MT-HIGH; n = 19) and low (MT-LOW; n = 22) proficiency groups.
Results
While all groups displayed improved attentional performance, only the MT-HIGH and MT-LOW groups showed significant increases in positive affect as measured by the Positive and Negative Affect Schedule. The MT-HIGH group showed significantly increased relative left-sided activity at both Fp1/Fp2 and F3/F4 electrode pairs, while no significant changes were observed in the MT-LOW and CT groups.
Conclusions
These results suggest that 8 weeks of mindfulness training is capable of inducing changes in resting anterior alpha asymmetry, but these results are dependent upon the level of proficiency achieved.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
A growing body of evidence suggests that mindfulness-based practices are capable of inducing both structural and functional brain changes, and these changes have been associated with enhanced cognitive and affective outcomes (Fox et al. 2014; Gotink et al. 2016). Notwithstanding critiques regarding some of the methodological shortcomings present in the field of mindfulness research (Coronado-Montoya et al. 2016; Van Dam et al. 2017), findings to date suggest that mindfulness is capable of enhancing attention and executive function (Lutz et al. 2009; Van den Hurk et al. 2009), increasing positive affect (Garland et al. 2015), and reducing negative affect (Brown and Ryan 2003; Davidson et al. 2003). While the mechanisms underlying these outcomes currently remain unclear, an intriguing possibility is the use of anterior EEG alpha asymmetry to assess patterns of neural activation associated with dispositional changes in affect resulting from mindfulness training.
Anterior alpha asymmetry provides a measure of relative left- or right-sided cortical activity by calculating the difference between EEG alpha power at homologous left and right frontal scalp electrodes. Oscillations in the alpha range have long been assumed to exert an inhibitory influence on cortical network activity, leading to the convention of inversely associating alpha power with cortical activity (Klimesch 1999; Pfurtscheller et al. 1996). Accordingly, when calculated as a measure of right minus left alpha power, higher asymmetry scores reflect greater relative left-sided cortical activity, while lower scores reflect greater relative right-sided activity (Allen et al. 2004). When recorded during a resting state, anterior alpha asymmetry has demonstrated high test-retest reliability and internal consistency (Tomarken et al. 1992b; Towers and Allen 2009).
Greater relative left-sided anterior activity has been associated with approach-related or behaviourally activating trait styles of motivation, including positive dispositional affect, whereas greater relative right-sided anterior activity is associated with withdrawal-related or behaviourally inhibiting styles of motivation, including negative dispositional affect (Coan and Allen 2004; Davidson 1992, 2004; Harmon-Jones and Gable 2017; Reznik and Allen 2018; Smith et al. 2017). Two models have been proposed to describe the lateralisation of anterior cortical activity and its association with affect and behaviour. Tomarken et al. (1992a) have described an affective valence model of anterior asymmetry, where greater relative left-sided anterior cortical activity is associated with positive affect, and greater relative right-sided activity with negative affect. Harmon-Jones (2003) proposed a motivational model, where greater relative left-sided anterior cortical activity is associated with approach motivations, and greater relative right-sided activity with withdrawal motivations. While both of these models are largely descriptive, they offer little specificity as to which neurobiological processes are differentially lateralised, and how these processes impact affect and motivation. Recent evidences from both electrophysiological and brain imaging studies suggest that inhibitory control functions may be differentially lateralised in the prefrontal cortex (Vallesi 2012), such that enhanced inhibitory control has been associated with greater left-sided anterior cortical activity (Allen et al. 2012; Ambrosini and Vallesi 2016; Taren et al. 2017). Grimshaw and Carmel (2014) have integrated these findings with existing models of anterior asymmetry to propose that the lateralisation of attentional inhibitory control processing in anterior cortical regions underlies the observed difference in affective and motivational outcomes.
To date, few studies have investigated the effect of mindfulness training on anterior alpha asymmetry and affect. Studies examining clinical samples (Barnhofer et al. 2007; Keune et al. 2011) report no change toward relative left-sided activity (at Fp1/Fp2, F3/F4, and F7/F8 homologous electrode pairs) after 8 weeks of mindfulness-based cognitive therapy (MBCT; Segal et al. 2002). Two studies examined pre-post mindfulness changes in resting anterior alpha asymmetry in healthy non-clinical samples. Both Moynihan et al. (2013) and Davidson et al. (2003) utilised an 8-week mindfulness-based stress reduction program (MBSR; Kabat-Zinn 1990) together with wait-list control conditions, reporting no significant change anterior alpha asymmetry (at Fp1/Fp2, F3/F4, and F7/F8 homologous electrode pairs) as a result of mindfulness training. Davidson et al. reported evidence of increased relative left-sided cortical activity at central sites (C3/C4 electrode pair), but not at anterior sites. Therefore, while mindfulness has been shown to enhance affect, there is little evidence to date of mindfulness’s ability to produce changes in anterior alpha asymmetry.
The practice of mindfulness primarily involves the cultivation of two components: (1) an attentional component, involving inhibitory control, which continuously attends to an object without its loss from awareness; and (2) equanimity, which is an unbiased and non-reactive orientation toward the contents of experience (Bishop et al. 2004). Each of the studies described above utilised a therapeutic mindfulness-based intervention (either MBCT or MBSR) which cultivate mindfulness together with a range of additional factors, such as cognitive behaviour therapy, psychoeducation, and an array of goal-oriented practices (Chiesa and Malinowski 2011). The heterogeneity of these interventions eliminates the possibility of making clear causal inferences regarding observed outcomes, including affective outcomes. For this reason, studies seeking to clearly investigate the mechanisms underlying mindfulness practice must use an intervention that generates mindfulness without confounding additional components. Isbel and Summers (2017) have introduced such a cognitive model of mindfulness together with a standardised mindfulness technique for use in longitudinal randomised control trials (RCTs). The standardised technique is not a therapeutic mindfulness intervention, but rather permits the study of mindfulness without introducing confounding components, thereby facilitating clearer inferential assessment of observed outcomes.
Attention training as a core feature of mindfulness practice may provide benefits for those at risk of cognitive decline. Normal ageing is associated with a decline in cognitive performance known as age-related cognitive decline (ARCD), which is a non-pathological decline in cognitive performance becoming increasingly evident beyond the age of 60 years (Hedden and Gabrieli 2004; Salthouse 2009), and can be accompanied by a decline in subjective well-being, mood, and affect (Blazer 2003; Gates et al. 2014). The previously reported benefits of mindfulness to attention and cognitive performance may indicate a role for mindfulness interventions in combating ARCD.
The current study sought to examine whether affective outcomes following mindfulness result from attention training or from mindfulness-specific factors, and whether or not affective outcomes are accompanied by changes in anterior alpha asymmetry. In line with previous research, it was hypothesised that 8 weeks of mindfulness training (MT) would result in increases in positive affect and reductions in negative affect, and that these changes would be accompanied by increased relative left-sided anterior alpha activity. Furthermore, it was hypothesised that participants who gained high proficiency in mindfulness (MT-HIGH) would demonstrate greater increases in anterior asymmetry scores and greater affective outcomes than those who gain low proficiency (MT-LOW). A computer-based attention training (CT) program designed to activate similar attentional processes to mindfulness was utilised as an active control condition.
Method
Participants
Participants were healthy older adults (≥ 60 years age) recruited from the general community to participate in an attention training program. Respondents underwent telephone screening to ensure those recruited met eligibility criteria (see Supplementary Material 1 for eligibility criteria) and had no prior exposure to either mindfulness or computerised brain training (see Fig. 1 for flowchart of participant retention and reason for dropout). As seen in Fig. 1, the most common exclusion criteria were inability to attend all sessions over the study period, followed by health reasons. As the study sought to recruit healthy older adults, it was expected that exclusion rates would be high given the age group targeted and the stringent eligibility criteria adopted to ensure the integrity of any findings. Information sessions were held for eligible participants, from which 120 participants were allocated by random number generator to the interventions (MT, n = 77; CT, n = 43). Participants were randomly allocated at a rate of 2:1 to MT to enable this group to be divided into high and low proficiency groups following MT training. As shown in Fig. 1, data from 67 participants (MT, n = 41; CT, n = 26) was eligible for analysis. Participant demographic information for the reported data is presented in Table 1.

CONSORT flowchart of participant retention through study with reason for dropout
Procedures
Participants were assessed on all measures at both pre-intervention (T1) and post-intervention (T2), with the exception of the Wechsler Test of Adult Reading which was administered only at baseline. The Positive and Negative Affect Schedule (PANAS; Watson et al. 1988) was completed at a group questionnaire session approximately 1 week prior to the EEG testing session. At the commencement of the EEG testing session, participants were required to report their sleep length and quality over the preceding week on a 5-point Likert-type scale (1 = increased to 5 = greatly reduced), as marked reduction in sleep is known to affect cognitive performance (Dinges and Kribbs 1991). The Hospital Anxiety and Depression Scale (HADS; Zigmond and Snaith 1983) was also completed at the commencement of the EEG test to assess for anxiety and depression as a potential confound. No participant reported markedly reduced sleep length or quality (all scores < 4) or elevated anxiety or depression (all scores < 11) immediately prior to the EEG session, and thus no participants were excluded from analysis due to sleep disturbance or significant psychological states of anxiety or depression.
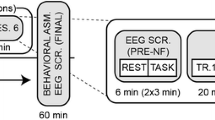
Participants were fitted with the EEG equipment before being given a demonstration of eye and muscle movement effects on EEG recording in order to minimise artefacts during the session. Resting EEG was then collected continuously for 4 min in an eyes open condition. Participants were instructed to “just rest” without intentionally performing any particular task for 4 min. In order to minimise eye movements during the EEG recording, participants were instructed to rest with their eyes fixed in a relaxed manner upon a yellow cross situated in the centre of a grey background presented on a monitor screen placed at a distance of 65 cm. Instructions were presented on the monitor screen prior to the task and participants proceeded at their own pace. An audible tone signalled the commencement of the resting period, which was followed 10 s later by the start of the continuous 4-min EEG recording. Participants then completed the breath counting task followed by the Sustained Attention to Response Task. Stimuli for all tasks were presented using E-Prime 2.0.10 software (Psychology Software Tools, Pittsburgh, PA, USA).
Interventions
The interventions were described to participants as attention training programs, differing only in delivery format. In this way, participants were blinded to experimental and control conditions. The CT program was designed to activate similar attentional components to those trained in mindfulness, but without the inclusion of mindfulness practice. Both programs were structurally equivalent, consisting of weekly 2-h group training sessions for 8 weeks, with topics covering the cognitive processes involved in attention training (see Supplementary Material 2 for weekly structure of the programs). A personal daily home practice requirement was included for both groups, which began at 20 min per day in week 1 and progressed to 45 min per day by week 8. Participants were required to keep a diary record of the amount of time spent engaged in the training intervention. Participants who did not meet the minimum amount of practice assigned during the intervention were excluded from analysis (MT, n = 8; CT, n = 2). All training sessions were conducted by the same trainer in the same room at the same time of day. Participants in both groups were instructed to perform the home training in a quiet environment where the training exercise could be carried out uninterruptedly.
Mindfulness-Based Attention Training Program
The MT program utilised the standardised mindfulness technique developed by Isbel and Summers (2017) for use in longitudinal RCTs. The primary task trained in this technique requires participants to direct and sustain their attention upon a localised set of sensations accompanying the breath at the abdomen in a manner that is nonjudgmental and non-reactive. Participants are required to notice when attention wanders from the primary task to secondary objects, such as mind wandering or distraction. When such an attentional shift occurs, participants were instructed to inhibit and disengage secondary processes, and redirect attention back to the primary task. Working memory is thought to be central to this training, as participants were required to retain the task instructions and continually update and monitor ongoing attentional performance. Thus, the core attentional processes trained in the standardised mindfulness technique include selective attention, task switching, inhibitory control, and working memory. Importantly, the standardised mindfulness technique does not contain non-specific additional components such as relaxation, psychoeducation, or yoga, which are found in MBCT and MBSR.
Computer-Based Attention Training Program
The CT program consisted of a series of targeted attention training exercises presented in game format designed to activate similar attentional processes to those activated in mindfulness practice. Each game emphasised a specific aspect of attention, such as sustained attention, selective attention, inhibitory control, or executive function to replicate the attention training occurring in the MT program (see Supplementary Material 3 for a description of the primary attentional components trained in each task). Difficulty increased on some tasks with successful performance to replicate the changing nature of attentional demands that occurs in mindfulness practice with increasing proficiency. Furthermore, participants were required to play an assigned game continuously each day during their home training sessions rather than switching between games in order to replicate the continuous application to a single task that occurs in MT. Assigned tasks were changed each week. The CT program was available to access online on any device to enable the training to be done in a way most suitable for each participant.
Measures
Wechsler Test of Adult Reading
The Wechsler Test of Adult Reading is a widely used word reading list used to estimate full scale intelligence quotient in adults. The WTAR is co-normed against the Wechsler Adult Intelligence Scale, 3rd edition, and is a reliable and valid estimate of intellectual capacity.
Positive and Negative Affect Schedule
Dispositional positive and negative mood was measured using the PANAS which consists of two 10-item subscales that assess positive affect (PA) and negative affect (NA). Participants respond on a Likert-type scale to indicate the frequency with which they experience particular emotions. The PANAS has demonstrated validity and high reliability (PA, Cronbach’s α .89; NA, Cronbach’s α .85) as a measure of affect in non-clinical samples (Crawford and Henry 2004).
Hospital Anxiety and Depression Scale
Symptoms of anxiety and depression were measured using the HADS. The HADS consists of two 7-item subscales for anxiety (HADS-A) and depression (HADS-D) on which participants indicate the frequency with which they experience symptoms on a Likert-type scale. The HADS is a cut-off criterion instrument designed to detect clinically significant states of anxiety and depression, where subscale scores greater than 11 indicate clinical significance. The HADS was utilised to screen for psychological states which may confound EEG findings such that participants with subscale scores greater than 11 would be excluded. The HADS has been shown to have high validity and reliability (HADS-A, Cronbach’s α .83; HADS-D, Cronbach’s α .82).
Breath Counting Task
Breath counting has previously been validated as a behavioural measure capable of distinguishing proficient from non-proficient mindfulness practitioners and has shown good test-retest reliability (Levinson et al. 2014; Wong et al. 2018). The task requires participants to observe their breathing while reporting a count of their in-and-out breath cycles for 15 min. Participants were instructed to breathe naturally while being attentive to the sensations accompanying the rising and falling of the abdomen as they mentally counted the in-out cycles of their breath from one to 21. Participants reported each in-out cycle with a down-arrow key press on counts one to 20, while on count 21 participants were instructed to press the right-arrow key to indicate successful count cycle. Self-caught counting errors were indicated by a left-arrow key press. Breath counting accuracy was physiologically confirmed using a piezo-electric crystal effort sensor placed around the chest to record respiration movement. A breath counting accuracy score was calculated as a percentage of correct count cycles to total cycles completed during the task (correct count ∕ total cycles × 100). Each self-caught error was recorded as an incorrect count cycle.
Sustained Attention to Response Task
The Sustained Attention to Response Task (SART; Robertson et al. 1997) consisted of a serial presentation of digits (1–9) to which participants to were instructed to respond via keypress to all go stimuli (digits 1–2, and 4–9) while withholding a response to each no-go stimuli (digit 3). For each block of nine trials, a single digit (1–9) was randomly chosen without replacement. Prior to the commencement of the experimental block, participants completed a practice block consisting of 45 trials (containing 5 no-go stimuli) with performance feedback to ensure the task was correctly understood. The experimental block consisted of 540 trials (60 blocks of 9 trials) containing 60 no-go stimuli (11% of total trials). Digits were black in colour and appeared in randomly allocated font sizes (100, 120, 140, 160, or 180 points) in the centre of a grey background for 200 ms. After stimulus offset, a yellow fixation cross was presented in the middle of the grey background for a variable inter-stimulus interval ranging from 1000 to 2000 ms (see Supplementary Material 4). Participants were instructed to respond as quickly and accurately as possible during the task.
Performance measures for the SART included errors of commission (percentage of errors on no-go), reaction time (RT), and reaction time coefficient of variation (RT CV). Errors of commission index failures of inhibitory control while variability in RT indexes sustained attention, wherein greater fluctuations in sustained attention are observed as increasing variability (CV) of responding (RT) to stimuli (Mrazek et al. 2012; Robertson et al. 1997).
EEG Measures
Continuous EEG data was recorded from 128 Ag/AgCl active electrodes mounted in an elastic head cap using a Biosemi ActiveTwo amplifier system (Biosemi, Amsterdam, Netherlands). To monitor eye movements, horizontal electrooculogram (EOG) was recorded using electrodes placed 1 cm lateral to the outer canthus of each eye, while vertical EOG was recorded using supra- and infraorbital electrodes on the left eye. During acquisition data was hardware filtered using a fixed first order analogue anti-aliasing filter (− 3 dB at 208 Hz) and digitised at 1024 Hz with a 24-bit analogue-to-digital converter. Further, offline processing was conducted using Brain Vision Analyzer2 software (Brain Products, GmbH, Gilching, Germany).
Continuous EEG data was referenced offline to an average reference in accord with the recommendations of Davidson (1998) and Allen et al. (2004). A zero-phase shift Butterworth infinite response filter (slope 12 dB/octave) was used to low pass (30-Hz cut-off) and high pass (0.5-Hz cut-off) filter the data, while a 50-Hz notch filter was applied to remove electrical line noise. All EEG data was visually inspected to detect noisy electrodes, and electrodes with consistent artefact were interpolated using spherical spines from surrounding sites (0.17% of all electrodes analysed). Ocular artefact correction was then performed to remove eye blink artefacts using the linear regression technique of Gratton et al. (1983). Artefact detection was then performed using a semiautomatic procedure to detect activity that (i) exceeded an absolute change of 50 μV/ms, or (ii) exceeded an absolute min-max difference of 100 μV/200 ms. When artefact was detected in any channel, data 200 ms prior to 200-ms post-event was marked as bad for all channels.
Each 4-min continuous recording was then segmented into overlapping 2-s epochs (50% overlap), with epochs containing artefact excluded from analysis. An a priori decision to reject participants with fewer than 50% artefact-free epochs at both time points from further analysis resulted in 19 participants being excluded due to insufficient artefact-free data (MT, n = 13; CT, n = 6). Spectral power (μV2) was calculated on artefact-free epochs using a fast Fourier transform (FFT) with a Hanning window at a resolution of 0.5 Hz. Epochs were averaged to provide the average power spectrum at each electrode for T1 and T2. Absolute power in the alpha frequency band (8–13 Hz) was then calculated and natural log-transformed to normalise the data distribution (Allen et al. 2004). In accord with previous studies examining anterior alpha asymmetry and mindfulness, an asymmetry score was calculated for homologous anterior electrode pairs Fp1/Fp2, F3/F4, and F7/F8 by subtracting log-transformed power at left location from log-transformed power at right location (i.e., ln[right] − ln[left]). Higher scores calculated in this way indicate increased relative left-sided cortical activity.
Data Analyses
Independent groups t tests were performed to examine pre-intervention between-group differences in age, FSIQ, and anterior alpha asymmetry, between-group difference in amount of training undertaken during the intervention, and between-group difference in artefact-free epochs available for analysis at each time point. Gender balance and handedness differences between the groups were examined using chi-square analysis.
To test the effect of the attention training programs on attention and inhibitory control, a mixed design analysis of variation (ANOVA) of SART commission errors, RT, and RT CV, with group (MT, CT) as a between-subjects factor and time (T1, T2) as a within-subjects factor, was performed.
Change in mindfulness across the intervention was assessed using the breath counting task. Breath counting accuracy scores were entered into a mixed design ANOVA performed with group (MT, CT) as a between-subjects factor and time (T1, T2) as a within-subjects factor. Breath counting scores at T2 were also used to provide a median split of the MT group into top and bottom 50th percentile groups, corresponding to mindfulness high performers (MT-HIGH) and mindfulness low performers (MT-LOW). This enables exploratory analysis of the differential effects of mindfulness proficiency on anterior alpha asymmetry and affect. Differences in reported and physiologically confirmed breath counting scores were assessed using mixed design ANOVA with group (MT, CT) as a between-subjects factor and time (T1, T2) as a within-subjects factor.
To determine the effect of the interventions on affect, a mixed design ANOVA with PANAS (PA, NA) and time (T1, T2) as within-subjects factors and group (MT, CT) as a between-subjects factor was performed. To examine the effect of mindfulness proficiency on affective outcomes, a second mixed design ANOVA with PANAS (PA, NA) and time (T1, T2) as within-subjects factors with group (MT-HIGH, MT-LOW, CT) as a between-subjects factor was performed. A single PANAS factor with two levels was used in order to reduce the risk of spurious type I errors resulting from multiple statistical analyses. Significant main effects were investigated with follow-up pairwise comparisons.
To test the effect of the attention training programs on resting anterior alpha asymmetry, a mixed design ANOVA of electrode (Fp1/Fp2, F3/F4, F7/F8) and time (T1, T2) as within-subjects factors with group (MT, CT) as a between-subjects factor was performed. To examine the effect of mindfulness proficiency on resting anterior alpha asymmetry, a second mixed design ANOVA with electrode (Fp1/Fp2, F3/F4, F7/F8) and time (T1, T2) as within-subjects factors with group (MT-HIGH, MT-LOW, CT) as a between-subjects factor was performed. A single electrode factor with three levels was used in order to reduce the risk of spurious type I errors resulting from multiple electrode analyses. Significant main effects were investigated with follow-up pairwise comparisons.
Intraclass correlation coefficients (ICC) were calculated for each group on breath counting scores over time to assess the test-retest reliability of this measure. To assess the correlation between change in resting anterior alpha asymmetry and change in affect, change scores for each variable were calculated by subtracting T1 scores from T2 scores. Bivariate correlations between change scores were then assessed. All statistical analysis was performed using SPSS version 24 (SPSS Inc., Chicago, IL, USA).
Results
Pre-Intervention Between-Group Comparisons
There were no significant pre-intervention differences between the MT and CT groups in age, gender balance, handedness, FSIQ, or anterior alpha asymmetry at Fp1/Fp2, F3/F4, or F7/F8 homologous electrode sites (see Table 1). Pre-intervention differences between post hoc identified groups are presented in Table 2.
Intervention Training Time
Inspection of mean daily practice time showed that the CT group (M = 36.0 min/day (SD = 6.3)) spent approximately 3 min longer per day engaged in the training program than the MT group (MT, M = 33.4 min/day (SD = 4.0)). An independent groups t test confirmed that the CT group engaged in a significantly greater amount of daily practice than the MT group during the 8-week program (t(65) = 2.07, p = .04).
Sustained Attention to Response Task
Table 3 shows the descriptive statistics and ANOVA results for each SART measure. Both groups showed significant reductions in errors of commission (F(1,65) = 12.84, p = .001, partial η2 = .165) and RT CV (F(1,65) = 18.33, p < .001, partial η2 = .200) from pre- to post-intervention, with no change in RT (F(1,65) = .051, p = .822, partial η2 = .001). No significant group × time interactions were observed. These results demonstrate that both attention training programs were effective in improving sustained attention and executive inhibitory control, and confirm that the CT group was not a sham control, but rather a true active control that effectively trained the attentional components targeted.
Breath Counting Task
Mean breath counting accuracy scores for each group at pre- and post-intervention are shown in Fig. 2. Repeated measures ANOVA revealed a significant group × time interaction (F(1,65) = 4.311, p = .042, partial η2 = .062). Follow-up Bonferroni-corrected pairwise comparisons indicated that the MT group showed significant pre- to post-intervention improvement on the breath counting task (MI-J = 14.01, SE = 5.06, p = .007), while the CT group showed no significant change (MI-J = − 2.87, SE = 6.36, p = .653). These results indicate that the MT intervention was effective in improving both attention and mindfulness, while the CT intervention was effective in training attention without improving mindfulness.

Mean breath counting accuracy at pre- (T1) and post-intervention (T2). MT mindfulness training group, CT computer training group. Error bars show standard error of the mean. *Change is significant (p < .01)
In the MT group, the median score on the breath counting task at T2 was 75%. Using this score, we were able to median split the MT group into top (> 75% accuracy = MT-HIGH; n = 19) and bottom (≤ 75% accuracy = MT-LOW; n = 22) 50th percentile groups based on T2 breath counting accuracy scores.
No significant change between reported and physiologically confirmed breath counting scores was observed over time (F(1,65) = 2.091, p = .158, partial η2 = .060) or within groups (F(1,65) = 0.036, p = .850, partial η2 = .001).
Positive and Negative Affect
Mixed design ANOVA (between-subjects: MT, CT) revealed a significant main effect of time (F(1,65) = 9.140, p = .004, partial η2 = .123), together with a significant group × time interaction (F(1,65) = 4.909, p = .030, partial η2 = .070). Follow-up pairwise comparisons confirmed PA significantly increased over time in the MT group (MI-J = 3.24, SE = 0.771, p < .001) but not in the CT group (MI-J = 0.500, SE = 0.969, p = .608). These results indicate that the MT program was effective at increasing positive affect, while no change in positive affect was observed in the CT group.
Exploratory mixed ANOVA with three-level between-groups factor (MT-LOW, MT-HIGH, CT) revealed a significant main effect of time (F(1,64) = 15.575, p < .001, partial η2 = .196), together with a significant main effect of PANAS (F(1,64) = 592.355, p < .001, partial η2 = .902) and a marginally significant time × group × PANAS interaction (F(1,64) = 3.026, p = .050, partial η2 = .086). Follow-up pairwise comparisons revealed that both the MT-LOW (MI-J = 3.14, SE = 1.09, p = .005) and MT-HIGH (MI-J = 3.35, SE = 1.11, p = .004) groups showed significant increases in PA from pre- to post-intervention, while the CT group (MI-J = 0.500, SE = 0.976, p = .610) showed no significant change in PA. Mean positive affect scores for these groups at pre- and post-intervention are shown in Fig. 3a. Negative affect scores showed no significant change from pre- to post-intervention in the MT-LOW (MI-J = 0.455, SE = 1.150, p = .694) and MT-HIGH (MI-J = − 1.053, SE = 1.237, p = .398) groups, while the CT groups displayed a marginally significant increase in NA (MI-J = 2.115, SE = 1.058, p = .050), as seen in Fig. 3b.

a Positive affect scores and b Negative affect scores at pre- (T1) and post-intervention (T2). Error bars show standard error of the mean. *Change is significant (p < .01)
Anterior Alpha Asymmetry Scores
Mixed design ANOVA with two-level between-groups factor (MT, CT) revealed a significant main effect of time (F(1,65) = 4.392, p = .040, partial η2 = .063) without any group or electrode interaction effects, indicating that there was a change in asymmetry scores over time disregarding group and electrode location. Exploratory mixed design ANOVA with three-level between-groups factor (MT-LOW, MT-HIGH, CT) showed a significant main effect of time (F(1,64) = 8.632, p = .005, partial η2 = .119) qualified by a significant time × group interaction (F(1,64) = 5.009, p = .010, partial η2 = .135) and a significant 3-way time × electrode × group interaction (F(1,64) = 2.715, p = .033, partial η2 = .1078). Follow-up Bonferroni-corrected pairwise comparisons revealed that the MT-HIGH group showed significant pre- to post-intervention increases in anterior alpha asymmetry scores at both the Fp1/Fp2 (MI-J = 0.178, SE = 0.06, p = .007) and F3/F4 (MI-J = 0.280, SE = 0.07, p < .001) homologous electrode pairs (see Fig. 4a and b respectively). The MT-HIGH group showed no significant change in alpha asymmetry at the F7/F8 electrode pair (see Fig. 4c). No significant change in anterior alpha asymmetry at any electrode pair was observed for the MT-LOW or CT group.

Mean alpha asymmetry scores at a Fp1/Fp2, b F3/F4, and c F7/F8 electrode pairs at pre- (T1) and post-intervention (T2). Higher scores indicate increased relative left-sided cortical activity. MT-LOW low proficiency in mindfulness, MT-HIGH high proficiency in mindfulness, CT computer training group. Error bars show standard error of the mean. *Change is significant (p < .01)
These results indicate that participants who gained high proficiency in mindfulness showed significant increases in relative left-sided anterior cortical activity as recorded at Fp1/Fp2 and F3/F4 homologous electrode sites, while those who gained low proficiency in mindfulness or who undertook CT did not demonstrate a change in anterior alpha asymmetry.
Correlations
Breath counting accuracy scores in the MT group demonstrated an 8-week test-retest reliability of ICC = .62, and for the CT group ICC = .68, which were very similar to the ICC = .60 reported by Levinson et al. (2014) in their original validation studies of this task as a measure of mindfulness proficiency.
To examine the relation between changes in anterior asymmetry and affect, change scores were calculated by subtracting T1 scores from T2 scores for Fp1/Fp2, F3/F4, and F7/F8 asymmetry scores, positive affect, and negative affect. Bivariate correlations identified no significant relationship between alpha asymmetry change scores and positive or negative affect or breath counting accuracy change scores in either the MT-HIGH group or the MT-LOW group, or the MT group as a whole or the CT group (see Supplementary Material 5 for correlation tables). Change in alpha asymmetry at Fp1/Fp2 and F3/F4 was significantly correlated in the MT-HIGH group (r = .678, p = .001), but not in the MT-LOW or CT groups.
Discussion
The present study found increased relative left-sided resting anterior cortical activity as measured at both the Fp1/Fp2 and F3/F4 electrode pairs in participants who achieved a high level of proficiency in mindfulness after an 8-week mindfulness intervention. No such changes were observed in those who gained low proficiency after the intervention, or in those who undertook an 8-week CT program. These results lend partial support to the hypothesis that 8 weeks of MT is capable of inducing changes in resting anterior alpha asymmetry since these changes were observed only in those who gained high proficiency in the practice.
The training of attention is a core feature of the early stages of mindfulness practice, and thus the CT program was designed to train similar attentional components to those activated in mindfulness practice. Both the MT and CT groups demonstrated improved inhibitory control and sustained attention as measured by SART errors of commission and RT CV respectively, indicating that both programs were effective in improving attention. While the CT group engaged in more training time than the MT group, only the MT group demonstrated improved performance on the breath counting task. This is an important finding, since previous studies comparing mindfulness to active control conditions have failed to show that the active control did not also improve mindfulness (Goldberg et al. 2016). In the present study, we have demonstrated that the CT program was a true active control that was effective at improving attention without enhancing mindfulness. In this way, we can be confident that any differences observed between the MT group and the CT group are the result of MT, since the CT program contained similar attention training and was structurally equivalent to the MT program.
It has been proposed that during mindfulness the prefrontal cortex exerts top-down inhibitory control to effect emotion regulation (Chiesa et al. 2013; Davidson et al. 2000). Orbitofrontal cortical (OFC) regions have been implicated in both the assignment of affective value to stimuli based upon a reward or punishment valence (Davidson 2004; Kringelbach 2005), as well as emotion regulation through amygdala-OFC functional connectivity (Banks et al. 2007). In particular, greater OFC/ventromedial PFC activity has been associated with increased ability to regulate negative affect and lower amygdala activity (Urry et al. 2006), while greater relative left-sided cortical activity has been associated with increased ability to regulate emotional responses to adverse emotional events (Jackson et al. 2003). Dorsolateral PFC (dlPFC) regions have been directly implicated in inhibitory control functions during emotion regulation (Ochsner et al. 2012; Pessoa 2008; Tang et al. 2015), with evidence now suggesting that inhibitory control may be differentially lateralised across the dlPFC such that effective inhibitory control is associated with greater left-sided dlPFC activity (Ambrosini and Vallesi 2016; Vallesi 2012). Increased left-sided activation in resting frontoparietal intrinsic networks has been shown following cognitive training in older adults, suggesting that lateralisation of intrinsic central executive network functions is alterable through targeted training interventions (Luo et al. 2016). In relation to MT, increased left dlPFC activity after a 6-week mindfulness intervention has been associated with greater inhibitory control during an affective Stroop task, with increases proportional to the amount of MT undertaken (Allen et al. 2012). Furthermore, Taren et al. (2017) have reported increased resting state functional connectivity between the left dlPFC and multiple distributed neural regions associated with executive control and emotion processing following a short-term mindfulness intervention. While research into emotion regulation is still in its infancy, evidence to date suggests that OFC and dlPFC regions of the PFC cortex may act via differing pathways to enact affective regulation, whereby OFC regions are recruited in the top-down regulation of limbic regions via efferent projections to the amygdala and limbic centres once an emotional response has been generated, whereas the dlPFC acts via inhibitory control and attentional regulation to diminish the initial response itself (Davidson 2004; Nejati et al. 2018; Pessoa 2008; Rule et al. 2002).
Emotion regulation in mindfulness practice does not involve suppression or cognitive reappraisal of affective stimuli, but rather an ability to simply observe with equanimity one’s emotional responses without altering them (Chambers et al. 2009; Vago and Silbersweig 2012). According to the cognitive model proposed by Isbel and Summers (2017), early stages of mindfulness practice involve metacognitive regulation of affective responses without avoidance, allowing them to be experienced without becoming caught up in them. These control influences produce state-like changes in overall affective composition since metacognitive monitoring and control is effective only when active (Teasdale et al. 1995). This corresponds to the regulation of active emotional responses via the recruitment of OFC regions to regulate active limbic centres. The model of Isbel and Summers further predicts that stable dispositional changes to affective composition are enacted through the development of insight which is capable of inhibiting disruptive cognitive and affective responses in a manner that prevents them from becoming manifest emotional disturbances. Importantly, the model predicts that the development of insight unfolds with enhanced executive attentional control, and these changes are expected only in those who achieve a high level of proficiency in mindfulness. In support of this prediction, evidence from fMRI studies suggests that minimising emotional responses via dlPFC regions through effective inhibitory control of aversive affective stimuli may only be achieved with proficiency in mindfulness practice. Allen et al. (2012) demonstrated that greater mindfulness experience is associated with increased left dlPFC activation and enhanced inhibitory control toward adverse affective content. Brefczynski-Lewis et al. (2007) reported increasing levels of activation in left dlPFC regions as practitioners develop from novice to highly experienced practitioners. In the current study, increased relative left-sided anterior cortical activity was observed only in those who gained high proficiency in mindfulness, supporting the hypothesis that these outcomes are dependent upon proficiency in the practice.
Existing models of anterior asymmetry are yet to clarify the underlying neurobiological mechanisms responsible for observable differences in anterior alpha asymmetry. The findings reported here may offer some support to the asymmetric inhibition model of alpha asymmetry proposed by Grimshaw and Carmel (2014). This model suggests that left-lateralised executive control inhibits negative or withdrawal-related stimuli, while right-lateralised control inhibits positive or approach-related stimuli. Here, we report that increased proficiency in mindfulness, and given its central role in mindfulness practice increased proficiency in inhibitory control, is accompanied by increased relative left-sided anterior cortical activity. Based on these findings, further research is warranted to investigate the role of inhibitory control in affective regulation.
Since anterior alpha asymmetry has been associated with dispositional affective style, the absence of change in asymmetry scores in the MT-LOW group suggests that increases in positive affect in this group may not represent dispositional changes. These findings support the predictions of the cognitive model of mindfulness of Isbel and Summers (2017) regarding state vs trait affective outcomes arising from MT. Since no similar increases in positive affect were observed in the active control group, we are able to conclude that the changes in the MT-LOW group were not the result of attention training or non-specific intervention factors (such as attending weekly training sessions, increased social engagement, and the performance of daily training exercises), but rather were the result of MT. Such a conclusion is supported by the wide body of evidence demonstrating improved affective outcomes resulting from mindfulness practice. Furthermore, since the active control condition was used to partial out the attention training component from mindfulness practice, the lack of change in anterior asymmetry in the CT group suggests that the observed increases in the MT-HIGH group resulted from mindfulness-specific factors such as equanimity, rather than attention training. The results reported here indicate that further research is required to investigate the long-term stability of affective outcomes from mindfulness practice, and whether these outcomes are differentially impacted by mindfulness proficiency.
No significant correlation between change in anterior alpha asymmetry and change in affect was identified in the present study. This accords with the majority of previous mindfulness intervention studies which found no significant correlation between measures of affect and anterior alpha asymmetry (Barnhofer et al. 2007; Davidson et al. 2003). Anterior alpha asymmetry generally correlates with a disposition toward affective experience rather than current mood states (Grimshaw and Carmel 2014). This lack of a simple correlation between anterior asymmetry and affect suggests a more complex relationship between these two variables. Further investigation to determine the possibility that lateralised inhibitory control may serve as a mediator between asymmetry and affect is warranted to uncover the relationship between these variables.
The results reported here have implications for the development of interventions to combat age-related cognitive decline. Cognitive performance is considered to decline beyond the age of 60 years, and may be accompanied by declines in affective well-being (Hedden and Gabrieli 2004). The average age of participants in the current study was approximately 71 years. We have demonstrated that 8-week training interventions are capable of enhancing attentional performance in healthy older adults, suggesting that these programs may have an application in combating age-related cognitive decline. Further studies are required to determine if the cognitive benefits arising from these training programs are maintained beyond the intervention.
Limitations and Future Research
While there were no significant pre-intervention differences in anterior alpha asymmetry between the MT and CT groups, proficiency groups identified post hoc using the breath counting task revealed a marginally significant baseline difference between the MT-HIGH group and the CT group at Fp1/Fp2. Although pre-intervention differences between the MT-HIGH group and other groups did not near significance at other sites, it is noted that the post hoc median split did appear to create an MT-HIGH group that differed from the other groups. An intriguing possibility suggested by these results is that future mindfulness proficiency may be predicted by pre-intervention EEG assessment, specifically anterior alpha asymmetry. This finding warrants further investigation into the potential of EEG measures to determine receptiveness to MT.
The absence of follow-up testing for participants after the 8-week program meant that we were unable to assess the stability of these effects beyond the intervention. Ideally, six- or 12-month follow-up assessments would be required to examine if the observed enhancements to attention and affect are maintained. This data would be valuable in determining if the observed improvements to affect in the MT-LOW group represented stable trait-like changes or temporary improvements. This data would be useful in further understanding the relationship between affect and anterior alpha asymmetry. In addition, if the attentional improvements in both the MT and CT groups were maintained over a long period, this would lend support to their use in either slowing age-related cognitive decline.
While two separate studies have provided robust evidence for the use of breath counting tasks as behavioural measures of mindfulness (Levinson et al. 2014; Wong et al. 2018), such tasks remain indirect measures of mindfulness. In the absence of neurobiological markers of mindfulness, the use of breath counting to assess mindfulness is certainly an improvement upon self-report measures. However, as an indirect measure, its sensitivity to discriminate mindfulness proficiency is to some extent confounded by participants’ general cognitive ability which also impacts their ability to successfully control attention during a breath counting task.
Comparison with existing studies of mindfulness and anterior asymmetry are restricted due to the wide range of interventions used, differing study populations, and the heterogeneity of EEG recording and data analysis techniques reported. The adoption of a standardised mindfulness technique would allow accurate cross-study comparisons, rather than the current situation where MBCT, MBSR, and various other MBIs are being utilised. Few studies to date have examined the effects of mindfulness on older adults; however, as the field continues to grow, we expect these numbers to increase, thereby permitting analysis of outcomes in elderly groups compared to younger cohorts. Finally, the field of EEG research has yet to adopt a standardised recording or data analysis procedure, and thus there exists in the literature a wide variety of reported EEG reference choices, electrode sites, and data analysis techniques. The lack of a standardised approach may contribute to the reporting of mixed anterior asymmetry results as evidenced in the field to date.
References
Allen, J. J. B., Coan, J. A., & Nazarian, M. (2004). Issues and assumptions on the road from raw signals to metrics of frontal EEG asymmetry in emotion. Biological Psychology, 67(1–2), 183–218. https://doi.org/10.1016/j.biopsycho.2004.03.007.
Allen, M., Dietz, M., Blair, K. S., van Beek, M., Rees, G., Vestergaard-Poulsen, P., … Roepstorff, A. (2012). Cognitive-affective neural plasticity following active-controlled mindfulness intervention. Journal of Neuroscience, 32(44), 15601–15610. https://doi.org/10.1523/JNEUROSCI.2957-12.2012.
Ambrosini, E., & Vallesi, A. (2016). Asymmetry in prefrontal resting-state EEG spectral power underlies individual differences in phasic and sustained cognitive control. NeuroImage, 124, 843–857. https://doi.org/10.1016/j.neuroimage.2015.09.035.
Banks, S. J., Eddy, K. T., Angstadt, M., Nathan, P. J., & Phan, K. L. (2007). Amygdala–frontal connectivity during emotion regulation. Social Cognitive and Affective Neuroscience, 2(4), 303–312. https://doi.org/10.1093/scan/nsm029.
Barnhofer, T., Duggan, D., Crane, C., Hepburn, S., Fennell, M. J. V., & Williams, J. M. G. (2007). Effects of meditation on frontal α-asymmetry in previously suicidal individuals. NeuroReport, 18(7), 709–712. https://doi.org/10.1097/WNR.0b013e3280d943cd.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., … Devins, G. (2004). Mindfulness: a proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230–241. https://doi.org/10.1093/clipsy.bph077.
Blazer, D. G. (2003). Depression in late life: review and commentary. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences, 58(3), M249–M265. https://doi.org/10.1093/gerona/58.3.M249.
Brefczynski-Lewis, J. A., Lutz, A., Schaefer, H. S., Levinson, D. B., & Davidson, R. J. (2007). Neural correlates of attentional expertise in long-term meditation practitioners. Proceedings of the National Academy of Sciences of the United States of America, 104(27), 11483–11488. https://doi.org/10.1073/pnas.0606552104.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822–848. https://doi.org/10.1037/0022-3514.84.4.822.
Chambers, R., Gullone, E., & Allen, N. B. (2009). Mindful emotion regulation: an integrative review. Clinical Psychology Review, 29(6), 560–572. https://doi.org/10.1016/j.cpr.2009.06.005.
Chiesa, A., & Malinowski, P. (2011). Mindfulness-based approaches: are they all the same? Journal of Clinical Psychology, 67(4), 404–424. https://doi.org/10.1002/jclp.20776.
Chiesa, A., Serretti, A., & Jakobsen, J. C. (2013). Mindfulness: top–down or bottom–up emotion regulation strategy? Clinical Psychology Review, 33(1), 82–96. https://doi.org/10.1016/j.cpr.2012.10.006.
Coan, J. A., & Allen, J. J. B. (2004). Frontal EEG asymmetry as a moderator and mediator of emotion. Biological Psychology, 67(1), 7–50. https://doi.org/10.1016/j.biopsycho.2004.03.002.
Coronado-Montoya, S., Levis, A. W., Kwakkenbos, L., Steele, R. J., Turner, E. H., & Thombs, B. D. (2016). Reporting of positive results in randomized controlled trials of mindfulness-based mental health interventions. PLoS One, 11(4), e0153220. https://doi.org/10.1371/journal.pone.0153220.
Crawford, J. R., & Henry, J. D. (2004). The positive and negative affect schedule (PANAS): construct validity, measurement properties and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 43(3), 245–265. https://doi.org/10.1348/0144665031752934.
Davidson, R. J. (1992). Anterior cerebral asymmetry and the nature of emotion. Brain and Cognition, 20(1), 125–151. https://doi.org/10.1016/0278-2626(92)90065-T.
Davidson, R. J. (1998). Anterior electrophysiological asymmetries, emotion, and depression: conceptual and methodological conundrums. Psychophysiology, 35(5), 607–614. https://doi.org/10.1017/S0048577298000134.
Davidson, R. J. (2004). What does the prefrontal cortex “do” in affect: perspectives on frontal EEG asymmetry research. Biological Psychology, 67(1), 219–234. https://doi.org/10.1016/j.biopsycho.2004.03.008.
Davidson, R. J., Jackson, D. C., & Kalin, N. H. (2000). Emotion, plasticity, context, and regulation: perspectives from affective neuroscience. Psychological Bulletin, 126(6), 890–909. https://doi.org/10.1037/0033-2909.126.6.890.
Davidson, R. J., Kabat-Zinn, J., Schumacher, J., Rosenkranz, M. A., Muller, D., Santorelli, S. F., … Sheridan, J. F. (2003). Alterations in brain and immune function produced by mindfulness meditation. Psychosomatic Medicine, 65(4), 564–570. https://doi.org/10.1097/01.PSY.0000077505.67574.E3.
Dinges, D. F., & Kribbs, N. B. (1991). Performing while sleepy: effects of experimentally-induced sleepiness. In T. H. Monk (Ed.), Sleep, sleepiness and performance (pp. 97–128). Oxford: John Wiley & Sons.
Fox, K. C. R., Nijeboer, S., Dixon, M. L., Floman, J. L., Ellamil, M., Rumak, S. P., … Christoff, K. (2014). Is meditation associated with altered brain structure? A systematic review and meta-analysis of morphometric neuroimaging in meditation practitioners. Neuroscience and Biobehavioral Reviews, 43, 48–73. https://doi.org/10.1016/j.neubiorev.2014.03.016.
Garland, E. L., Geschwind, N., Peeters, F., & Wichers, M. (2015). Mindfulness training promotes upward spirals of positive affect and cognition: multilevel and autoregressive latent trajectory modeling analyses. Frontiers in Psychology, 6, 1–13. https://doi.org/10.3389/fpsyg.2015.00015.
Gates, N., Valenzuela, M., Sachdev, P. S., & Fiatarone Singh, M. A. (2014). Psychological well-being in individuals with mild cognitive impairment. Clinical Interventions in Aging, 9, 779–792. https://doi.org/10.2147/CIA.S58866.
Goldberg, S. B., Wielgosz, J., Dahl, C. J., Schuyler, B. S., MacCoon, D. S., Rosenkranz, M. A., … Davidson, R. J. (2016). Does the Five Facet Mindfulness Questionnaire measure what we think it does? Construct validity evidence from an active controlled randomized clinical trial. Psychological Assessment, 28(8), 1009–1014. https://doi.org/10.1037/pas0000233.
Gotink, R. A., Meijboom, R., Vernooij, M. W., Smits, M., & Hunink, M. G. M. (2016). 8-week Mindfulness Based Stress Reduction induces brain changes similar to traditional long-term meditation practice – a systematic review. Brain and Cognition, 108, 32–41. https://doi.org/10.1016/j.bandc.2016.07.001.
Gratton, G., Coles, M. G. H., & Donchin, E. (1983). A new method for off-line removal of ocular artifact. Electroencephalography and Clinical Neurophysiology, 55(4), 468–484. https://doi.org/10.1016/0013-4694(83)90135-9.
Grimshaw, G. M., & Carmel, D. (2014). An asymmetric inhibition model of hemispheric differences in emotional processing. Frontiers in Psychology, 5, 1–7. https://doi.org/10.3389/fpsyg.2014.00489.
Harmon-Jones, E. (2003). Clarifying the emotive functions of asymmetrical frontal cortical activity. Psychophysiology, 40(6), 838–848. https://doi.org/10.1111/1469-8986.00121.
Harmon-Jones, E., & Gable, P. A. (2017). On the role of asymmetric frontal cortical activity in approach and withdrawal motivation: an updated review of the evidence. Psychophysiology, (1), –23. https://doi.org/10.1111/psyp.12879.
Hedden, T., & Gabrieli, J. D. E. (2004). Insights into the ageing mind: a view from cognitive neuroscience. Nature Reviews. Neuroscience, 5(2), 87–96. https://doi.org/10.1038/nrn1323.
Isbel, B., & Summers, M. J. (2017). Distinguishing the cognitive processes of mindfulness: developing a standardised mindfulness technique for use in longitudinal randomised control trials. Consciousness and Cognition, 52(Supplement C), 75–92. https://doi.org/10.1016/j.concog.2017.04.019.
Jackson, D. C., Mueller, C. J., Dolski, I., Dalton, K. M., Nitschke, J. B., Urry, H. L., … Davidson, R. J. (2003). Now you feel it, now you don’t: frontal brain electrical asymmetry and individual differences in emotion regulation. Psychological Science, 14(6), 612–617. https://doi.org/10.1046/j.0956-7976.2003.psci_1473.x.
Kabat-Zinn, J. (1990). Full catastrophe living: using the wisdom of your mind to face stress, pain and illness. New York: Delta.
Keune, P. M., Bostanov, V., Hautzinger, M., & Kotchoubey, B. (2011). Mindfulness-based cognitive therapy (MBCT), cognitive style, and the temporal dynamics of frontal EEG alpha asymmetry in recurrently depressed patients. Biological Psychology, 88(2–3), 243–252. https://doi.org/10.1016/j.biopsycho.2011.08.008.
Klimesch, W. (1999). EEG alpha and theta oscillations reflect cognitive and memory performance: a review and analysis. Brain Research Reviews, 29(2), 169–195. https://doi.org/10.1016/S0165-0173(98)00056-3.
Kringelbach, M. L. (2005). The human orbitofrontal cortex: linking reward to hedonic experience. Nature Reviews Neuroscience, 6, 691–702. https://doi.org/10.1038/nrn1747.
Levinson, D. B., Stoll, E. L., Kindy, S. D., Merry, H. L., & Davidson, R. J. (2014). A mind you can count on: validating breath counting as a behavioral measure of mindfulness. Frontiers in Psychology, 5, 1–10. https://doi.org/10.3389/fpsyg.2014.01202.
Luo, C., Zhang, X., Cao, X., Gan, Y., Li, T., Cheng, Y., … Li, C. (2016). The lateralization of intrinsic networks in the aging brain implicates the effects of cognitive training. Frontiers in Aging Neuroscience, 8(32), 1–9. https://doi.org/10.3389/fnagi.2016.00032.
Lutz, A., Slagter, H. A., Rawlings, N. B., Francis, A. D., Greischar, L. L., & Davidson, R. J. (2009). Mental training enhances attentional stability: neural and behavioral evidence. The Journal of Neuroscience, 29(42), 13418–13427. https://doi.org/10.1523/JNEUROSCI.1614-09.2009.
Moynihan, J. A., Chapman, B. P., Klorman, R., Krasner, M. S., Duberstein, P. R., Brown, K. W., & Talbot, N. L. (2013). Mindfulness-based stress reduction for older adults: effects on executive function, frontal alpha asymmetry and immune function. Neuropsychobiology, 68(1), 1–17. https://doi.org/10.1159/000350949.
Mrazek, M. D., Smallwood, J., & Schooler, J. W. (2012). Mindfulness and mind-wandering: finding convergence through opposing constructs. Emotion, 12(3), 1–7. https://doi.org/10.1037/a0026678.
Nejati, V., Salehinejad, M. A., & Nitsche, M. A. (2018). Interaction of the left dorsolateral prefrontal cortex (l-DLPFC) and right orbitofrontal cortex (OFC) in hot and cold executive functions: evidence from transcranial direct current stimulation (tDCS). Neuroscience, 369, 109–123. https://doi.org/10.1016/j.neuroscience.2017.10.042.
Ochsner, K. N., Silvers, J. A., & Buhle, J. T. (2012). Functional imaging studies of emotion regulation: a synthetic review and evolving model of the cognitive control of emotion. Annals of the New York Academy of Sciences, 1251, E1–E24. https://doi.org/10.1111/j.1749-6632.2012.06751.x.
Pessoa, L. (2008). On the relationship between emotion and cognition. Nature Reviews Neuroscience, 9, 148–158. https://doi.org/10.1038/nrn2317.
Pfurtscheller, G., Stancák, A., & Neuper, C. (1996). Event-related synchronization (ERS) in the alpha band — an electrophysiological correlate of cortical idling: a review. International Journal of Psychophysiology, 24(1), 39–46. https://doi.org/10.1016/S0167-8760(96)00066-9.
Reznik, S. J., & Allen, J. J. B. (2018). Frontal asymmetry as a mediator and moderator of emotion: an updated review. Psychophysiology, 55(1), 1–32. https://doi.org/10.1111/psyp.12965.
Robertson, I. H., Manly, T., Andrade, J., Baddeley, B. T., & Yiend, J. (1997). ‘Oops!’: performance correlates of everyday attentional failures in traumatic brain injured and normal subjects. Neuropsychologia, 35(6), 747–758. https://doi.org/10.1016/S0028-3932(97)00015-8.
Rule, R. R., Shimamura, A. P., & Knight, R. T. (2002). Orbitofrontal cortex and dynamic filtering of emotional stimuli. Cognitive, Affective, & Behavioral Neuroscience, 2(3), 264–270. https://doi.org/10.3758/cabn.2.3.264.
Salthouse, T. A. (2009). When does age-related cognitive decline begin? Neurobiology of Aging, 30(4), 507–514. https://doi.org/10.1016/j.neurobiolaging.2008.09.023.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2002). Mindfulness-based cognitive therapy for depression: a new approach to preventing relapse. New York: Guilford Press.
Smith, E. E., Reznik, S. J., Stewart, J. L., & Allen, J. J. B. (2017). Assessing and conceptualizing frontal EEG asymmetry: an updated primer on recording, processing, analyzing, and interpreting frontal alpha asymmetry. International Journal of Psychophysiology, 111(Supplement C), 98–114. https://doi.org/10.1016/j.ijpsycho.2016.11.005.
Tang, Y. Y., Hölzel, B. K., & Posner, M. I. (2015). The neuroscience of mindfulness meditation. Nature Reviews Neuroscience, 16(4), 213–225. https://doi.org/10.1038/nrn3916.
Taren, A. A., Gianaros, P. J., Greco, C. M., Lindsay, E. K., Fairgrieve, A., Brown, K. W., … Marsland, A. L. (2017). Mindfulness meditation training and executive control network resting state functional connectivity: a randomized controlled trial. Psychosomatic Medicine, 79(6), 674–683. https://doi.org/10.1097/PSY.0000000000000466.
Teasdale, J. D., Segal, Z. V., & Williams, J. M. G. (1995). How does cognitive therapy prevent depressive relapse and why should attentional control (mindfulness) training help? Behaviour Research and Therapy, 33(1), 25–39. https://doi.org/10.1016/0005-7967(94)E0011-7.
Tomarken, A. J., Davidson, R. J., Wheeler, R. E., & Doss, R. C. (1992a). Individual differences in anterior brain asymmetry and fundamental dimensions of emotion. Journal of Personality and Social Psychology, 62(4), 676–687. https://doi.org/10.1037/0022-3514.62.4.676.
Tomarken, A. J., Davidson, R. J., Wheeler, R. E., & Kinney, L. (1992b). Psychometric properties of resting anterior EEG asymmetry: temporal stability and internal consistency. Psychophysiology, 29(5), 576–592. https://doi.org/10.1111/j.1469-8986.1992.tb02034.x.
Towers, D. N., & Allen, J. J. B. (2009). A better estimate of the internal consistency reliability of frontal EEG asymmetry scores. Psychophysiology, 46(1), 132–142. https://doi.org/10.1111/j.1469-8986.2008.00759.x.
Urry, H. L., van Reekum, C. M., Johnstone, T., Kalin, N. H., Thurow, M. E., Schaefer, H. S., … Davidson, R. J. (2006). Amygdala and ventromedial prefrontal cortex are inversely coupled during regulation of negative affect and predict the diurnal pattern of cortisol secretion among older adults. The Journal of Neuroscience, 26(16), 4415–4425. https://doi.org/10.1523/JNEUROSCI.3215-05.2006.
Vago, D. R., & Silbersweig, D. A. (2012). Self-awareness, self-regulation, and self-transcendence (S-ART): a framework for understanding the neurobiological mechanisms of mindfulness. Frontiers in Human Neuroscience, 6, 1–30. https://doi.org/10.3389/fnhum.2012.00296.
Vallesi, A. (2012). Organisation of executive functions: hemispheric asymmetries. Journal of Cognitive Psychology, 24(4), 367–386. https://doi.org/10.1080/20445911.2012.678992.
Van Dam, N. T., van Vugt, M. K., Vago, D. R., Schmalzl, L., Saron, C. D., Olendzki, A., … Meyer, D. E. (2017). Mind the hype: a critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspectives on Psychological Science, 13(1), 1–26. https://doi.org/10.1177/1745691617709589.
Van den Hurk, P. A. M., Giommi, F., Gielen, S. C., Speckens, A. E. M., & Barendregt, H. P. (2009). Greater efficiency in attentional processing related to mindfulness meditation. The Quarterly Journal of Experimental Psychology, 63(6), 1168–1180. https://doi.org/10.1080/17470210903249365.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070. https://doi.org/10.1037/0022-3514.54.6.1063.
Wong, K. F., Massar, S. A. A., Chee, M. W. L., & Lim, J. (2018). Towards an objective measure of mindfulness: replicating and extending the features of the breath-counting task. Mindfulness, 9(5), 1402–1410. https://doi.org/10.1007/s12671-017-0880-1.
Zigmond, A. S., & Snaith, R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67(6), 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x.
Funding
BI conducted this work with the support of the Judy Henzell Memorial Scholarship. MS reports personal fees from Eli Lily (Australia) Pty Ltd. and grants from Novotech Pty Ltd., outside the submitted work.
Author information
Authors and Affiliations
Contributions
BI designed and conducted the study, delivered the interventions, performed the data analysis, and wrote the paper. JL collaborated in the data analysis, writing, and editing of the final manuscript. DH collaborated in the data analysis, writing, and editing of the final manuscript. MS collaborated in the design, data analysis, writing, and editing of the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethics Statement
All procedures were performed in accordance with the ethical standards of the University of the Sunshine Coast Human Research Ethics Committee (approval: HREC A-15-748), the Australian National Statement on Ethical Conduct in Human Research, and the Code of Ethics of the World Medical Association (Declaration of Helsinki). In accordance with the latter two ethical statements which proscribe the use of no-treatment or placebo controls when existing effective treatment conditions exist, an active control condition consisting of a program of cognitive training was used as a comparison condition to assess the benefits of mindfulness training.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Supplementary Material 1
Participant acceptance criteria for inclusion into the study (PDF 76 kb)
Supplementary Material 2
Weekly structure of the training interventions. (PDF 47 kb)
Supplementary Material 3
Computer-based attention training tasks utilised in the active control condition. (PDF 54 kb)
Supplementary Material 4
Sustained Attention to Response Task (SART) (PDF 179 kb)
Supplementary Material 5
Correlational results for change in alpha asymmetry, affect, and breath-counting accuracy. (PDF 73 kb)
Rights and permissions
About this article

Cite this article
Isbel, B., Lagopoulos, J., Hermens, D.F. et al. Mindfulness Induces Changes in Anterior Alpha Asymmetry in Healthy Older Adults. Mindfulness 10, 1381–1394 (2019). https://doi.org/10.1007/s12671-019-01106-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-019-01106-w