
Abstract
The present study aimed to extend the existing literature of mindfulness as a stress protective factor by (1) exploring the role of mindfulness state, not only in response to but also in anticipation of acute pain and (2) investigating an explanatory pathway, decreased rumination, between anticipation of acute pain and cognitive performance, with mindfulness moderating this indirect effect. One-hundred-and-four undergraduates were assessed for state mindfulness and then underwent an acute pain induction using the cold pressor task (CPT). Pain measures included pain threshold, pain tolerance, pain intensity, short-form McGill Pain questionnaire, and pain catastrophizing. Next, half of the participants were told that they would be repeating the CPT after some intervening tasks; half were not told to expect a second CPT. Participants completed a Cognitive Estimation Task (CET) that involved problem-solving, followed by a measure of rumination during CET. Results showed no meaningful associations between mindfulness state and sensory measures of pain (e.g., pain tolerance, pain threshold), but higher mindfulness state was related to lower pain catastrophizing and lower McGill affective subscale scores. There was also evidence of a moderated indirect effect: the indirect effect of condition through rumination on CET performance was moderated by mindfulness. That is, those in the anticipation condition with higher mindfulness state later reported ruminating less during CET and performed better at CET. Mindfulness thus appeared to have a protective role in maladaptive emotional responses when one anticipates acute pain, shielding self-regulatory resources needed to think flexibly when expecting a stressor.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Stressful situations are part of daily living, yet there are significant differences in how people respond to and anticipate such events that bear important consequences for well-being (Larsen 2000; Weinstein et al. 2009). Mindfulness, an open present-awareness (Brown and Ryan 2003), has been increasingly recognized as a protective factor in coping with not only difficult life events, such as a cancer diagnosis (e.g., Campbell et al. 2012), but also daily stressors and hassles (e.g., Donald et al. 2016; Schultz et al. 2015). Put simply, to be mindful is to pay attention to and be aware of what is happening in the present moment in a non-judgmental manner (Brown et al. 2007; Ryan and Rigby 2015). Over the last three decades, research on both mindfulness trait and mindfulness state has demonstrated the benefits of this attribute of consciousness for a wide array of psychological and physical health outcomes in clinical and non-clinical populations (see for reviews Brown et al. 2007; Chiesa and Serretti 2011; Khoury et al. 2015).
While mindfulness trait pertains to stable individual differences, Brown and Ryan (2003) theorized that mindfulness is inherently a state of consciousness; thus, it varies from moment to moment within a person. Therefore, mindfulness state can be defined as momentary present-awareness. Other scholars also argue that mindfulness may be closer to a state than a trait, dependent on context and time (Bishop et al. 2004). Indeed, studies showed that although those who are dispositionally more mindful were more likely to report mindful states, mindfulness state was predictive of benefits above and beyond mindfulness trait (Brown and Ryan 2003; Weinstein et al. 2009). Mindfulness trait can be measured by validated self-report questionnaires, such as The Mindful Awareness and Attention Scale (MAAS) (Brown and Ryan 2003) and The Five Facet Mindfulness Questionnaire (FFMQ) (Baer et al. 2006). Mindfulness state can be measured by validated self-report questionnaires, such as the MAAS state (Brown and Ryan 2003) and the Toronto Mindfulness Scale (TMS) (Lau et al. 2006).
Prior research on mindfulness state has generally used brief mindfulness interventions (8 to 15 min) to induce a mindful state in controlled settings (e.g., Erisman and Roemer 2010; Kiken and Shook 2011; Ortner et al. 2007). Brief mindfulness inductions have been shown to predict reduced emotional reactivity, distress, and dysphoric mood to potentially threatening stimuli (e.g., Arch and Craske 2006; Brown et al. 2012; Molet et al. 2013). Few studies have examined the role of naturally occurring mindfulness state (Brown and Ryan 2003; Donald et al. 2016; Weinstein et al. 2009). This is relevant because most studies on mindfulness state involve mindfulness induction or training compared to other conditions; the predictor is usually group membership, not mindfulness state (Keng et al. 2011).
In addition, most mindfulness research focuses on mindfulness as a protective factor in response to a stressor; there are fewer studies exploring how it may affect anticipation of a potentially unpleasant situation (Hoge et al. 2018; Laurent et al. 2016; Weinstein et al. 2009). Theoretically, mindfulness may act as a protective factor before, during, and after the stressor. With regard to before a stressor, although only a handful of studies have assessed the role of mindfulness in anticipation of an unpleasant situation; findings are promising. Weinstein et al. (2009, study 4) demonstrated that more mindful individuals appraised the same potentially stressful event (an upcoming exam) more benignly (less threatening) than less mindful individuals, resulting in higher well-being. Similarly, Laurent et al. (2016) had couples engage in two laboratory sessions involving a conflict resolution task. They reported that those with high mindfulness state displayed higher positive affect and lower negative affect before the second conflict task (see also Barnes et al. 2007; Hoge et al. 2018). In terms of after a stressor, studies using self-report and physiological measures have evidenced the benefits of mindfulness in facilitating faster and more adaptive recovery. For example, Brown et al. (2012) showed that higher trait mindfulness was associated with lower cortisol responses and self-reported stress and anxiety following a laboratory stressor (see for similar results, Bergeron et al. 2016).
Fewer are the investigations on the role of mindfulness in reactivity during or immediately after the stressor. In fact, Davidson and colleagues have shown that, in general, there is less variability in emotional reactivity during exposure to a negative affect-producing stimulus than after exposure to the stimulus is terminated (Davidson 2003; Davidson et al. 2000; Jackson et al. 2003). This would suggest that mindfulness may exert its benefits mostly during the recovery phase rather than blunting the intensity or directly altering the subjective experience of those stressors (Collins et al. 2017; Farb et al. 2010; Fogarty et al. 2015). It is important to note, however, that some studies do report benefits of mindfulness during the stressor (e.g., Arch and Craske 2010; Kadziolka et al. 2016).
Several cognitive, emotional, and neural mechanisms through which mindfulness confers its benefits have been theoretically proposed or empirically identified (see for reviews, Bishop et al. 2004; Brown and Ryan 2003; Brown et al. 2007; Schultz and Ryan 2015). Mindfulness is thought to facilitate focus and regulation of thoughts and emotions, thus reducing distraction, mind-wandering, maladaptive amplification of affective cues and ruminative thoughts (Bishop et al. 2004; Moore and Malinowski 2009; Teper et al. 2013). Mindfulness, then, may facilitate the availability of cognitive resources enhancing self-regulation (Short et al. 2016). To be sure, very recent studies have begun to identify the specific cognitive processes mindfulness may benefit. Early evidence suggests that mindfulness may facilitate inhibition of irrelevant information, such as intrusive thoughts, mind-wandering, and automatic responses that are irrelevant to the task at hand (Gallant 2016; Noone et al. 2016). Indeed, mindfulness has been shown to be oppositely related to rumination and associated with inverse adaptive outcomes (e.g., Fresco et al. 2007).
In contrast, rumination, which is an uncontrollable, repetitive, unconstructive thinking about one’s negative emotions and the events that caused them (Nolen-Hoeksema 1991), has been empirically shown to relate to deficits in inhibitory processes of content that is not currently relevant (Brinker et al. 2013; Carson et al. 2003; Martin and Tesser 1996). In fact, theories propose that inhibitory deficits are causal in the overactivation of emotional content that characterizes rumination (Joormann 2006; Koster et al. 2011). When people ruminate, they dwell on negative thoughts, precluding access to more neutral thoughts in working memory (Bernblum and Mor 2010; Donaldson et al. 2007).
Beyond enhanced emotional regulation, more recent studies have suggested that mindfulness may benefit cognitive performance (Eberth and Sedlmeier 2012), such as enhanced academic performance (e.g., Hanley et al. 2015), attention (e.g., Saltzman and Goldin 2008; Semple et al. 2010), episodic memory (Brown et al. 2016), and working memory (Jha et al. 2010; Lao et al. 2016). Mindfulness has also been related to enhanced higher-order cognition activities, such as problem-solving (Ostafin and Kassman 2012), moral reasoning and ethical decision making (Cottone and Javier 2007; Ruedy and Schweitzer 2011), critical thinking (Noone et al. 2016), cognitive flexibility (Heeren et al. 2009; Lao et al. 2016), and performance on GRE (Mrazek et al. 2013). Notably, neuroimaging research supports these findings (e.g., Tang and Posner 2009; Tang et al. 2010; Zeidan et al. 2010).
On a different note, considering mindfulness’ characteristics, this quality of awareness may also support coping with pain, which is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage” (International Association for the Study of Pain 1979, p. 249). Pain experience, then, is a multidimensional construct that has both sensory and emotional qualities (Price et al. 1983; Melzack and Wall 1965). Indeed, it is well known that the experience of pain concerns not only the extent of tissue damage but also how one deals with the pain (Boothby et al. 1999; Turk 1996). Characteristics of pain such as location, tolerance, and intensity comprise the sensory dimension. The affective dimension reflects the emotional reaction to the pain experience (Melzack and Katz 2013).
Although mindfulness-based interventions have shown promising results for the treatment of chronic pain (Chiesa and Serretti 2011), it is less clear whether brief mindfulness inductions may help with coping with an acute pain stimulus. In the context of experimental acute pain, studies usually use interventions ranging from single brief mindfulness induction to a few mindfulness-training sessions and compare them to control or other intervention groups (e.g., hypnosis, distraction). Whereas some studies found that mindfulness intervention increased pain tolerance (e.g., Kingston et al. 2007; Liu et al. 2013; Swain and Trevena 2014), others reported no such benefit (e.g., Petter et al. 2014; Prins et al. 2014; Sharpe et al. 2013). In addition, whereas some investigations have found that mindfulness decrease subjective ratings of pain intensity and increase pain threshold (e.g., Zeidan et al. 2010, 2015), others did not find such results (e.g., Liu et al. 2013; Petter et al. 2014; Prins et al. 2014; Swain and Trevena 2014).
The pattern is somewhat more consistent when it comes to ratings of pain-related distress (i.e., affective dimension of pain), such that brief mindfulness interventions have been shown to reduce self-reported distress to acute pain inductions (Liu et al. 2013; Prins et al. 2014; Zeidan et al. 2015; but see McMullen et al. 2008 for contrasting findings). Studies comparing pain reaction of experienced meditators with matched controls seem to corroborate the view of attenuated affective responding to acute pain induction (Brown and Jones 2010; Perlman et al. 2010). Mindfulness has also been shown to be negatively related to pain catastrophizing (Petter et al. 2014; Prins et al. 2014; Schutze et al. 2010), defined as the tendency to ruminate, magnify, or feel helpless about pain (Sullivan et al. 1995). Therefore, it appears that a state of non-judgmental present-moment awareness may buffer against secondary evaluations of physical sensations that increase pain severity, such as pain catastrophizing, but may not reduce sensory aspects of pain, such as pain intensity (Campbell et al. 2010). In our literature review (English language articles only), we found that most pain studies are in the context of mindfulness interventions, except for one study that investigated naturally occurring state mindfulness with regard to acute pain (Petter et al. 2014).
The present study examined the role of non-induced mindfulness state in response to, and in anticipation of, an unpleasant sensory stimulus. We further investigated an explanatory pathway, namely, decreased rumination, between anticipation of acute pain and cognitive performance, with mindfulness moderating this indirect effect. Presumably, those with higher mindfulness state would later report to ruminate less as they anticipated undergoing a second acute pain induction, leaving them with more self-regulatory resources for a cognitive task. Specifically, we predicted that those higher in mindfulness state would show a more adaptive reaction to pain in the affective dimension (e.g., use less-threatening words to describe the pain, decreased pain catastrophizing), but, given mixed prior findings, we did not make specific hypotheses regarding pain response in the sensory dimension (e.g., pain tolerance, pain threshold, pain intensity). In the present study, we proposed a conditional process model (moderated mediation) of mindfulness as a stressor buffer (see Fig. 1).

Hypothesized conditional process model illustrates the conceptual model to test the indirect effect of anticipating acute pain through ruminative thinking on students’ cognitive performance, with mindfulness state as moderator
We hypothesized that those in the anticipation condition would show worse performance in the estimation task (Fig. 1, labeled A) and that that those in the anticipation condition would later report higher ruminative thinking (Fig. 1, labeled B). Rumination was predicted to relate negatively to performance in the estimation task (Fig. 1, labeled C) and that the association between anticipation and rumination would be moderated by mindfulness, such that participants who were high in mindfulness state would later report lower rumination when anticipating acute pain compared to students low in mindfulness state (Fig. 1, labeled D). Mindfulness would thus act as a buffer to those anticipating an unpleasant experience and was hypothesized to only moderate the condition rumination path (Fig. 1, labeled B), but not the rumination performance in the estimation task path (Fig. 1, labeled C). That is because we expected that once one is ruminating, there is no space for mindfulness to have an effect. In other words, given rumination is the dwelling of negative thoughts and emotions, the open and non-judgmental attention that characterizes mindfulness would already be compromised.
Method
Participants
Participants were 117 undergraduate students. Students were recruited through an online registration system, and received extra credit that could be applied to psychology courses. Thirteen participants were deleted: six due to experimenter error and seven due to survey software malfunction. The final sample included 104 participants (35 males) with a mean age of 20.07 (SD = 1.26) and a range from 18 to 25 years old. Fifty percent identified as Caucasian, 34.6% as Asian, 8.7% as black, 1.9% as mixed, and 4.8% as “other.” Of these, 5.8% further indicated their ethnicity as Hispanic/Latino. Power analyses (Cohen et al. 2003) revealed that significant effects, expecting a medium effect size and power of 0.90, required a minimum sample size of 88 participants. All advertisements and procedures for this study were approved by the University’s Research Subject Review Board (RSRB).
Procedure
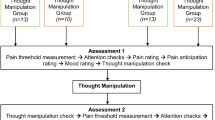
This study was part of a larger study exploring personality characteristics and pain. All participants signed up for two sessions with 1 week apart between the sessions. Participants underwent an initial lab session that lasted approximately 30 min. Upon arrival to the laboratory, participants were screened for exclusion criteria and those who qualified were asked to provide informed consent. Following the procedures of other studies using the Cold Pressor Task (CPT) (e.g., George et al. 2006; Lee et al. 2010; Mitchell et al. 2004), the exclusion criteria selected only participants free from medical conditions that contraindicated exposure to extreme cold temperatures (e.g., Raynaud’s syndrome), those not taking any medication, and those who had no current or history of chronic pain. Participants then completed a questionnaire assessing their demographic information and a series of exploratory measures not reported in this study. Next, the experimenter explained to participants some preparation requirements for the second session to prevent potential effects on pain measures (e.g., no smoking, no intake of pain medication). Finally, participants were asked to re-schedule if they were in any kind of pain.
Upon arrival to session two, participants were screened for medication, coffee, and alcohol intake, as well as smoking and current pain. If they did not meet the requirements, they were re-scheduled. Participants were quasi-randomized by gender into the two conditions making an effort to have an equal number of males and females in each condition. They then completed a brief questionnaire assessing mindfulness state, along with filler items. Next, they were asked to undergo the CPT, followed by pain measures. After completing pain measures, half were told they would be repeating the entire CPT after an estimation exercise, while half did not receive this information, and thus were not anticipating further acute pain. At this point, all participants completed an Estimation Task on the computer, followed by a questionnaire assessing rumination during the Estimation Task. Before leaving, participants were thanked and debriefed.
Cold Pressor Task
This task has been shown to reliably elicit a stress response by increasing sympathetic nervous system and HPA axis activity (e.g., Edelson and Robertson 1986; Kelly and Cooper 1998; McRae et al. 2006). Participants were asked to immerse their non-dominant hand to the wrist for 5 min in a container with water at 32 °C (± 1 °C). This procedure was meant to normalize the starting hand temperature. A red mark (with felt tipped pen) on the wrist indicated to participants how deep they had to submerse their hands (to keep the hand at a constant immersion depth). Next, participants immersed their non-dominant hand to the wrist in the cold water bath (water was constantly maintained at 7 ± 0.01 °C). Usually, the temperature in the Cold Pressor Task is between 0 and 2 °C (Mitchell et al. 2004), but because we were interested in leaving more room for subjective interpretation of pain, we had the water slightly warmer (see Helsen et al. 2011). The apparatus used was a circulating and cooling water bath, Lauda Brinkmann (RM6-RMS Refrigerating Circulating Bath). This model of water bath has a 6-L water capacity and maintains temperature within the 0.1 °C level. Immersion time was measured on a stopwatch held outside of the participants’ view, with an uninformed maximum immersion time of 5 min for safety (Lee et al. 2010; Mitchell et al. 2004). Participants were instructed to say “pain” when the sensation first became uncomfortable (i.e., pain threshold) and to remove their hand whenever the pain became intolerable (i.e., pain tolerance).
Measures
Mindfulness State (Brown and Ryan 2003)
To assess mindfulness state, defined as receptive attentiveness to present at a given moment in time, a validated adaptation of the Mindful Attention Awareness Scale (MAAS; Brown and Ryan 2003) was used. The MAAS is well validated and extensively used measure of mindfulness trait. The adapted and validated mindfulness state measure has been used in several previous studies (e.g., Brown et al. 2012, 2016; Weinstein et al. 2009). The measure has five items and uses a 0–6 (not at all to very much) Likert scale. Samples items include “I’m finding it difficult to stay focused on what’s happening in the present moment” and “I’m doing jobs or tasks automatically, without being aware of what I’m doing” (both reverse scored). Reliability for this scale in the present study was α = 0.82.
Pain Threshold
Pain threshold is time in seconds from hand immersion to when participants first experienced discomfort (level one in the Pain Visual Analog Scale (VAS)).
Pain Tolerance
Pain tolerance is total time in seconds of hand immersion.
Peak Pain Intensity
Immediately after the CPT, participants verbally rated their peak pain intensity using a 10-cm Pain VAS (marked from zero to ten, with the following anchors: “0” no pain, “5” moderate pain, and “10” worst possible pain).
Short-Form McGill Pain Questionnaire (Melzack 1987)
This measure has three components. The first assesses quality of pain using 15 adjective-verbal descriptors, 11 items indicating sensory pain dimensions (e.g., throbbing, sharp), and four items indicating affective pain dimensions (e.g., sickening, cruel). The descriptors were rated on a 4-point scale (none, mild, moderate, severe) and yield three scores: sensory, affective, and total. Two additional components assess overall intensity of pain. Participants rated overall pain intensity using a 10-cm horizontal VAS anchored from “no pain” to “worst possible pain” and a 6-point scale (Present Pain Index (PPI)) ranging from no pain to “excruciating.” This measure is reported to be both reliable (Zalon 1999) and valid (Dudgeon et al. 1993; Melzack 1987). Reliabilities for the scale in the present study were as follows: McGill total, α = 0.84; McGill sensory, α = 0.81; and McGill affective, α = 0.79.
Pain Catastrophizing Scale (Sullivan et al. 1995)
This instrument comprises 13 items assessing the extent to which individuals experience negative thoughts and feelings when in pain. It typically uses the frame of “past pain experiences,” but was adapted in the present study to refer to the pain just experienced in the CPT (Lee et al. 2010; Thorn et al. 2004) using a 7-point scale (“0” not at all to “6” very much). The Pain Catastrophizing Scale (PCS) total score is the sum of its three subscales: rumination, magnification, and helplessness. Reliability for this scale in the present study was α = 0.92.
The Biber Cognitive Estimation Test (Bullard et al. 2004; Shallice and Evans 1978)
This 20-item test contains five estimation questions in four different categories (time/duration, quantity, weight, and distance). There are no clear answers to the questions (e.g., “How many seeds are there in a watermelon?”), as participants are required to extrapolate from existing knowledge and use logical thinking to arrive at plausible estimates. The Cognitive Estimation Test (CET) is an open-ended task, as such participants must generate novel responses for each item. It is considered a measure of fluid cognitive functioning (i.e., problem solving), and it is believed to involve the central executive of the work memory system. Moreover, it has been shown that ego depletion impairs performance on this task, given that self-regulatory resources are necessary to generate appropriate answers to ambiguous questions (Schmeichel et al. 2003; Vohs et al. 2012).
Participants’ answers to each item were scored on a 0–2 point scale, with higher scores reflecting better performance. The scoring criteria were based on answers given by a large sample of normal adults (Bullard et al. 2004). Estimates between the 25th and 75th percentile of the normal adult distribution were considered acceptable and received a score of 2. Estimates within the response range of 95% of the normal adult sample but not within the 25th to 75th percentile were considered mildly inappropriate and received a score of 1. Finally, estimates not within the response range of 95% of the normal adult sample were considered inappropriate and received a score of 0. In the present study, the mean score was 28.35 (SD = 4.33), with a range from 6 to 35. Reliability for this scale in the present study was α = 0.60. This value is consistent with reports of reliability for this scale in previous studies (e.g., Bullard et al. 2004).
Rumination During CET
This measure was adapted from the Perseverative Thinking Questionnaire, a content independent measure of rumination (Ehring et al. 2011). It comprised six items (e.g., “I kept “re-hashing” my experience in the cold water) assessing participants’ level of repetitive negative thinking (repetitiveness, intrusiveness, unproductiveness, and difficulties disengaging), using a 7-point Likert scale (“0” not at all to “6” very much). Reliability for this scale in the present study was α = 0.82.
Data Analyses
Preliminary analyses included ANOVAs and chi-squared tests to determine whether the two conditions (control, anticipation) differed at baseline and any potential sex differences. We also conducted hierarchical regressions to explore how mindfulness related to the different measures of pain. Main analyses tested the proposed moderated mediation model. Such models aim to clarify both how and when a specific effect occurs (Preacher et al. 2007). A conditional effect is said to exist “when the strength of an indirect effect depends on the level of some variable, or in other words, when mediation relations are contingent on the level of a moderator” (Preacher et al. 2007, p. 193). We aimed to test whether the indirect effect of anticipating acute pain through ruminative thinking on students’ cognitive performance depended on students’ mindfulness state. To test the proposed model, we used PROCESS, a versatile computational tool for path analysis involving moderation and mediation that can be used in SPSS (Hayes 2012).
Results
Table 1 presents reliabilities (Cronbach’s alpha), means, standard deviations, and intercorrelations for the study measures. At the zero-order level, mindfulness did not significantly correlate with more sensory measures of pain: pain threshold, pain tolerance, and pain intensities. However, mindfulness did significantly correlate with more affective measures of pain: McGill affective and pain catastrophizing, as well as with rumination during CET. That is, higher levels of mindfulness were associated with lower levels of affective pain and rumination. In addition, higher levels of pain catastrophizing were related to lower pain threshold, pain tolerance, and CET scores, but higher levels of pain intensities, McGill descriptors (especially McGill affective), and rumination during CET. Surprisingly, mindfulness state was not correlated with CET scores.
ANOVAs and chi-squared tests were computed to determine whether the two conditions (control, anticipation) differed at baseline. No significant differences were found between the groups at baseline in terms of gender, age, race, and ethnicity, indicating that the quasi-randomization procedure was successful (see Table 2). In the subsequent analyses, we included sex as covariate given that other studies have shown it to influence some variables of interest. For example, males typically have higher pain tolerance than females and females typically have higher pain catastrophizing scores than males (Dixon et al. 2004; Lee et al. 2010; Thorn et al. 2004). In the current study, although there were no significant sex differences in terms of pain tolerance (p > 0.18), females showed higher levels of McGill total, B = − 3.22, F(1, 101) = 4.05, p < 0.05, and pain catastrophizing, B = − 0.51, F (1, 101) = 4.10, p < 0.05. In addition, there was a non-significant trend such that females were associated with higher McGill affective ratings, B = − 0.495, F (1, 101) = 3.43, p = 0.07, and higher reported McGill sensory ratings, B = − 2.27, F (1, 101) = 3.06, p = 0.08.
Hierarchical regressions were performed to explore the role of mindfulness in the different pain measures. In the first step, we included the covariate sex. In the second step, we entered mindfulness. The results were null for the following variables: pain threshold, pain tolerance, peak pain, McGill total, McGill sensory, McGill pain intensity, and McGill PPI. However, higher levels of mindfulness were associated with lower pain catastrophizing, B = − 0.31, F (1, 101) = 8.6, p < 0.01, and lower McGill affective scores, B = − 0.43, F (1, 101) = 3.84, p = 0.05.
Next, the conditional process model tested whether rumination during the cognitive estimation task mediates the relationship between the condition (i.e., anticipation of pain or not) and performance on the cognitive task differently at different levels of mindfulness (see Fig. 1). In other words, the question was do those high in mindfulness when anticipating pain report to ruminate less and therefore perform better in the cognitive task than those low in mindfulness? In a preliminary step, to visualize the interaction of interest, we performed a hierarchical regression with the covariate sex entered in the first step, the main effects (condition and mindfulness) entered simultaneously in the second step, and the two-way interaction included in the third step (condition × mindfulness). The interaction of mindfulness and condition predicted rumination during CET, ΔR2 = 0.03, F (1, 99) = 4.01, p < 0.05.
To examine the interaction between mindfulness and condition on rumination during CET, a simple slope analysis was conducted. Using the control condition as the reference group, the effect of mindfulness on rumination during CET was not significant (p > 0.78). Using the anticipation condition as the reference, higher levels of mindfulness were associated with lower rumination during CET, B = − 0.32, F (1, 99) = 12.66, p < 0.01. Thus, when participants were not anticipating pain, mindfulness had no effect on how much they later reported ruminating during the CET, whereas when pain was anticipated, then those higher in mindfulness later reported ruminating less (see Fig. 2).

Moderation effect of mindfulness on the relation between condition (anticipation of pain vs. control) and rumination during Cognitive Estimation Task (CET)
Next, we used methods discussed in Preacher et al. (2007) to examine moderation of the indirect effect of condition (anticipation vs. control) on CET performance through rumination during CET, which generated two regression models (see Fig. 3 and Table 3). The first is called the mediator variable model, which specified rumination during CET as the dependent variable. The second regression model is called the dependent variable model, which specified CET score as the dependent variable. We calculated bootstrap confidence intervals at different levels of mindfulness to determine how the strength of the conditional indirect effect changed. To do that, we examined the effect at one standard deviation below the mean, at the mean, and at one standard deviation above the mean. Indirect effect results are reported using 95% bias corrected confidence interval with 10,000 resamples (95% BC CI).

Statistical conditional process model illustrates paths to test the indirect effect of condition (anticipating acute pain vs. control) through ruminative thinking on students’ cognitive performance, with mindfulness state as moderator. Sex variable was added as a covariate
In the mediator variable model, condition uniquely predicted rumination during CET (b = 0.47, p < 0.01), mindfulness did not uniquely predict rumination during CET (p > 0.05), and the interaction of condition with mindfulness uniquely predicted rumination during CET (b = − 0.29, p < 0.05). In the dependent variable model, rumination during CET uniquely predicted CET performance (b = − 1.6, p < 0.01), but condition did not uniquely predict CET score (p > 0.05). The conditional indirect effect was significant at 1 SD below the mindfulness mean (95% BC CI{ − 3.57, − 0.12}), at the mindfulness mean (95% BC CI { − 2.38, − 0.06}), but non-significant at 1 SD above the mindfulness mean (95% BC CI {− 1.82, 0.24}) (see Table 3). Results then indicate that those with high levels of mindfulness state later report to ruminate less when anticipating acute pain and perform better at the estimation task when compared to those low in mindfulness state when anticipating acute pain.
Discussion
We examined the role of non-induced state mindfulness in response to and in anticipation of acute pain. Further, we investigated an explanatory pathway, decreased rumination, between anticipation of acute pain, and performance in a higher-order cognitive task, with mindfulness moderating this indirect effect. This study is unique in exploring the role of naturally occurring mindfulness state (as opposed to mindfulness training), how mindfulness may be protective not only in response to but also in anticipation of a stressor, and extends the pain literature in providing further evidence with regard to the relations between mindfulness state and acute pain.
As predicted, mindfulness state was related to more adaptive acute pain response in the affective dimension, as indicated by lower pain catastrophizing and lower McGill affective scores. This finding extends and is consistent with pain distress research on mindfulness training and experienced meditators (Brown and Jones 2010; Liu et al. 2013; Prins et al. 2014; Zeidan et al. 2015; but see McMullen et al. 2008 for contrasting findings). Given mixed findings of previous studies, there were no specific predictions with regard to the sensory dimension of pain. The null findings between mindfulness state and pain tolerance, pain threshold, pain intensity, and McGill sensory scores are aligned with some past studies (e.g., Petter et al. 2014; Prins et al. 2014; Sharpe et al. 2013), but oppose others (e.g., Kingston et al. 2007; Zeidan et al. 2010). This highlights the importance of including both affective and sensory dimensions when studying mindfulness and pain (Lee et al. 2010) and appears to suggest that those who are high in mindfulness may feel similar levels of pain (i.e., no blunting of intensity), but have more benign secondary evaluations of pain. Considering the evolutionary function of accurate perception of acute pain for survival, it seems adaptive for mindful individuals to not blunt or minimize pain experience (Riva et al. 2014). It is equally adaptive not to amplify it in threatening/unpleasant affect words, possibly excessively escalating the situation, leading to prolonged ill-being, activation of the stress system, and preventing one to attend to the present moment (Britton et al. 2012; Hoge et al. 2018).
In fact, these findings parallel Davidson and colleagues’ findings of mindfulness having greater impact in emotional reactivity after the exposure to a negative stimulus (faster recovery) than during it (e.g., Davidson 2003; Jackson et al. 2003). In other words, in general, results have shown less variability in emotional reactivity during exposure to a negative affect-producing stimulus than after exposure to the stimulus is terminated (see also Davidson et al. 2000). This would suggest that mindfulness may exert its benefits mostly during the recovery phase rather than blunting the intensity or directly altering the subjective experience of those stressors (Farb et al. 2010; Williams and Swales 2004). Corroborating this argument, Fogarty et al. (2015) showed equal reactivity during a lab stress task in low- and high-mindfulness individuals, but superior recovery indicated by heart rate for those high in mindfulness. Other studies also did not find differences in the magnitude of immediate emotional response to lab-based stressors after mindfulness training, but did demonstrate more adaptive recovery patterns (e.g., Britton et al. 2012; Collins et al. 2017; Farb et al. 2010, but see for opposing findings, Kadziolka et al. 2016). Our results support the above literature demonstrating that mindfulness state may regulate chronicity and escalation of negative reactions rather than blunt the intensity of responses (Britton et al. 2012; Collins et al. 2017).
Related to the above, growing evidence indicates that mindfulness facilitates not only self-reported affective recovery but also effective HPA axis activation termination after stress, returning the stress system to baseline levels faster. For example, Brown et al. (2012) showed that higher trait mindfulness was associated with lower cortisol responses and self-reported stress and anxiety following a laboratory stressor. Similarly, Bergeron et al. (2016) reported that priming mindfulness had beneficial psychological and physiological effects after a stressful speech task, indicated by lower perceived stress and negative affect, in addition to faster cortisol recovery (see for similar findings, Hoge et al. 2018).
Unexpectedly, given the growing literature showing a relation between enhanced cognitive performance and mindfulness (e.g., Brown et al. 2016; Eberth and Sedlmeier 2012), mindfulness state did not significantly correlate with performance in the estimation task. This may indicate that the relation between mindfulness and cognition is more complex when responding to or anticipating a stressor.
With regard to the conditional process model, hypotheses were partially confirmed. In contrast to what was proposed, those in the anticipation condition did not show a worse performance in the estimation task than those in the control condition. Yet, as hypothesized, those in the anticipation condition later reported ruminating more during the estimation task than those who were not expecting a second acute pain induction. In addition, holding condition constant, those who later reported ruminating more performed worse in the estimation task. Also, consistent with hypotheses, we found that mindfulness moderated the relationship between condition and rumination such that those high in mindfulness state later reported ruminating less when anticipating acute pain, compared to students low in mindfulness state in the same group. The indirect effect of condition on the estimation task through rumination was significant at low and mean levels of mindfulness, but not at higher levels of mindfulness. In other words, high-mindfulness state acted as a shield for those anticipating pain, such that they later reported ruminating less during the estimation task, and consequently performed better at it.
The high-quality present-moment attention seemed to facilitate focus and reduce intrusive thoughts about the acute pain induction for those expecting it (Bishop et al. 2004; Moore and Malinowski 2009; Teper et al. 2013). In turn, this adaptive inhibition of irrelevant information presumably resulted in high availability of cognitive resources for completing a task that requires self-regulation, as participants must use existing knowledge and logical thinking to problem-solve and generate novel answers. Being more mindful appears to have shielded self-regulatory resources needed to think flexibly when expecting a stressor. Such results are consistent with literature linking mindfulness with lower rumination and associated mal-adaptive outcomes (e.g., Fresco et al. 2007). For example, studies have shown that individuals with higher dispositional mindfulness displayed lower rumination after an emotional challenge (Eisenlohr-Moul et al. 2016; Kaiser et al. 2015). Moreover, mindfulness training has been shown to decrease ruminative behavior (Chambers et al. 2009; Kaiser et al. 2015), and to allow for better inhibition of irrelevant information (e.g., Gallant 2016; Mrazek et al. 2013; Noone et al. 2016; Short et al. 2016). Finally, the lack of a direct relationship between condition and performance in the cognitive task in the presence of a significant indirect effect through rumination may suggest the presence of unmodeled mediators of opposite effect of rumination (Hayes and Preacher 2013; O’Rourke and MacKinnon 2015). That is, the lack of effect of condition on cognitive performance may be non-significant due to the presence of unidentified mediators competing with rumination during the task.
Limitations and Future Directions
There are several limitations to this research that should be acknowledged and addressed in future work. The conclusions made in the present paper are based on a single study and future studies are needed to replicate and expand on them. The sample was comprised of undergraduates who were largely women, and although sample size was adequate based on power analyses, it is relatively small. Such limitations impact the potential generalizability and implication of results. Moreover, rumination during CET was assessed retrospectively, after students had already completed the Estimation Task, but was tested as the mediator, preceding the Estimation Task, in the moderated mediation model. This is also a limitation because retrospective self-report may include time-related bias and may be influenced by how one thinks one performed in the Estimation Task.
Furthermore, it is important for future studies to explore alternative mediators, particularly given the lack of a direct effect between condition and cognitive performance in the presence of a significant indirect effect through rumination. Potential promising mediators include coping style (Weinstein et al. 2009), cognitive flexibility (Lao et al. 2016; Heeren et al. 2009), and experiential avoidance (Hayes et al. 2006). Finally, future studies exploring the relationship between pain and mindfulness should include both affective and sensory dimensions of pain, given that current results show distinguished effects of mindfulness for each dimension. This would help clarify the pattern of mixed findings in the pain literature (Lee et al. 2010).
References
Arch, J. J., & Craske, M. G. (2006). Mechanisms of mindfulness: emotion regulation following a focused breathing induction. Behaviour Research and Therapy, 44(12), 1849–1858.
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13, 27–45.
Barnes, S., Brown, K. W., Krusemark, E., Campbell, W. K., & Rogge, R. D. (2007). The role of mindfulness in romantic relationship satisfaction and responses to relationship stress. Journal of Marital and Family Therapy, 33(4), 482–500.
Bergeron, C. M., AlmgrenDore, I., & Dandeneau, S. (2016). “Letting go” (implicitly): priming mindfulness mitigates the effects of a moderate social stressor. Frontiers in Psychology, 7, Art 872-8.
Bernblum, R., & Mor, N. (2010). Rumination and emotion-related biases in refreshing information. Emotion, 10(3), 423–432.
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., et al. (2004). Mindfulness: a proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230–241.
Boothby, J. L., Thorn, B. E., Stroud, M. W., & Jensen, M. P. (1999). Chapter: coping with pain. In R. J. Gatchel & D. C. Turk (Eds.), Psychosocial factors in pain: Critical perspectives (pp. 343–359). New York: Guilford Press.
Brinker, J. K., Campisi, M., Gibbs, L., & Izzard, R. (2013). Rumination, mood and cognitive performance. Psychology, 4(3A), 224–231.
Britton, W. B., Shahar, B., Szepsenwol, O., & Jacobs, W. J. (2012). Mindfulness-based cognitive therapy improves emotional reactivity to social stress: results from a randomized controlled trial. Behavior Therapy, 43(2), 365–380.
Brown, C. A., & Jones, A. K. P. (2010). Meditation experience predicts less negative appraisal of pain: electrophysiological evidence for the involvement of anticipatory neural responses. Pain, 150(3), 428–438.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: the role of mindfulness in psychological well-being. Journal of Personality and Social Psychology, 84, 822–848.
Brown, K. W., Ryan, R. M., & Creswell, J. D. (2007). Mindfulness: theoretical foundations and evidence for its salutary effects. Psychological Inquiry, 18, 1–26 2007-17560-001.
Brown, K. W., Weinstein, N., & Creswell, J. D. (2012). Trait mindfulness modulates neuroendocrine and affective responses to social evaluative threat. Psychoneuroendocrinology, 37(12), 2037–2041.
Brown, K. W., Goodman, R. J., Ryan, R. M., & Analayo, B. (2016). Mindfulness enhances episodic memory performance: evidence from a multimethod investigation. PLoS One, 11(4), Art e0153309.
Bullard, S. E., Fein, D., Gleeson, M. K., Tischer, N., Mapou, R. L., & Kaplan, E. (2004). The biber cognitive estimation test. Archives of Clinical Neuropsychology, 19(6), 835–846.
Campbell, C. M., Kronfli, T., Buenaver, L. F., Smith, M. T., Berna, C., Haythornthwaite, J. A., & Edwards, R. R. (2010). Situational versus dispositional measurement of catastrophizing: associations with pain responses in multiple samples. The Journal of Pain, 11(5), 443–453.
Campbell, T. S., Labelle, L. E., Bacon, S. L., Faris, P., & Carlson, L. E. (2012). Impact of mindfulness-based stress reduction (MBSR) on attention, rumination and resting blood pressure in women with cancer: a waitlist-controlled study. Journal of Behavioral Medicine, 35(3), 262–271.
Carson, S. H., Peterson, J. B., & Higgins, D. M. (2003). Decreased latent inhibition is associated with increased creative achievement in high-functioning individuals. Journal of Personality and Social Psychology, 85(3), 499–506.
Chambers, R., Gullone, E., & Allen, N. B. (2009). Mindful emotion regulation: an integrative review. Clinical Psychology Review, 29(6), 560–572.
Chiesa, A., & Serretti, A. (2011). Mindfulness-based interventions for chronic pain: a systematic review of the evidence. The Journal of Alternative and Complementary Medicine, 17(1), 83–93.
Cohen, J., Cohen, P., West, S. G., & Aiken, L. S. (2003). Applied multiple regression/correlation analysis for the behavioral sciences. Mahwah: Lawrence Erlbaum Associates Publishers.
Collins, K. R. L., Stebbing, C., Stritzke, W. G. K., & Page, A. C. (2017). A brief mindfulness intervention attenuates desire to escape following experimental induction of the interpersonal adversity implicated in suicide risk. Mindfulness, 8(4), 1096–1105.
Cottone, J., & Javier, R. A. (2007). Predictors of moral reasoning: components of executive functioning and aspects of religiosity. Journal for the Scientific Study of Religion, 46, 37–53.
Davidson, R. J. (2003). Affective neuroscience and psychophysiology: toward a synthesis. Psychophysiology, 40(5), 655–665.
Davidson, R. J., Jackson, D. C., & Kalin, N. H. (2000). Emotion, plasticity, context, and regulation: perspectives from affective neuroscience. Psychological Bulletin, 126(6), 890–909.
Dixon, K. E., Thorn, B. E., & Ward, L. C. (2004). An evaluation of sex differences in psychological and physiological responses to experimentally-induced pain: a path analytic description. Pain, 112(1–2), 188–196.
Donald, J. N., Atkins, P. W. B., Parker, P. D., Christie, A. M., & Ryan, R. M. (2016). Daily stress and the benefits of mindfulness: examining the daily and longitudinal relations between present-moment awareness and stress responses. Journal of Research in Personality, 65, 30–37.
Donaldson, C., Lam, D., & Mathews, A. (2007). Rumination and attention in major depression. Behaviour Research and Therapy, 45(11), 2664–2678.
Dudgeon, D., Raubertas, R. F., & Rosenthal, S. N. (1993). The short-form McGill pain questionnaire in chronic cancer pain. Journal of Pain and Symptom Management, 8(4), 191–195.
Eberth, J., & Sedlmeier, P. (2012). The effects of mindfulness meditation: a meta-analysis. Mindfulness, 3(3), 174–189.
Edelson, J. T., & Robertson, G. L. (1986). The effect of the cold pressor test on vasopressin secretion in men. Psychoneuroendocrinology, 11, 07–316.
Ehring, T., Zetsche, U., Weidacker, K., Wahl, K., Schonfeld, S., & Ehlers, A. (2011). The perseverative thinking questionnaire (PTQ): validation of a content-independent measure of repetitive negative thinking. Journal of Behavior Therapy and Experimental Psychiatry, 42(2), 225–232.
Eisenlohr-Moul, T. A., Peters, J. R., Pond, R. S. J., & DeWall, C. N. (2016). Both trait and state mindfulness predict lower aggressiveness via anger rumination: a multilevel mediation analysis. Mindfulness, 7(3), 713–726.
Erisman, S. M., & Roemer, L. (2010). A preliminary investigation of the effects of experimentally induced mindfulness on emotional responding to film clips. Emotion, 10(1), 72–82.
Farb, N. A. S., Anderson, A. K., Mayberg, H., Bean, J., McKeon, D., & Segal, Z. V. (2010). Minding one’s emotions: mindfulness training alters the neural expression of sadness. Emotion, 10(1), 25–33.
Fogarty, F. A., Lu, L. M., Sollers, J. J., Krivoschekov, S. G., Booth, R. J., & Consedine, N. S. (2015). Why it pays to be mindful: trait mindfulness predicts physiological recovery from emotional stress and greater differentiation among negative emotions. Mindfulness, 6(2), 175–185.
Fresco, D. M., Rytwinski, N. K., & Craighead, L. W. (2007). Explanatory flexibility and negative life events interact to predict depression symptoms. Journal of Social and Clinical Psychology, 26(5), 595–608.
Gallant, S. N. (2016). Mindfulness meditation practice and executive functioning: breaking down the benefit. Consciousness and Cognition: An International Journal, 40, 116–130.
George, S. Z., Dannecker, E. A., & Robinson, M. E. (2006). Fear of pain, not pain catastrophizing, predicts acute pain intensity, but neither factor predicts tolerance or blood pressure reactivity: an experimental investigation in pain-free individuals. European Journal of Pain, 10(5), 457–465.
Hanley, A. W., Palejwala, M. H., Hanley, R. T., Canto, A. I., & Garland, E. L. (2015). A failure in mind: dispositional mindfulness and positive reappraisal as predictors of academic self-efficacy following failure. Personality and Individual Differences, 86, 332–337.
Hayes, A. F. (2012). PROCESS: a versatile computational tool for observed variable mediation, moderation, and conditional process modeling. Retrieved from http://www.afhayes.com/public/process2012.pdf.
Hayes, A. F., & Preacher, K. J. (2013). Conditional process modeling: using structural equation modeling to examine contingent causal processes. In G. R. Hancock & R. O. Mueller (Eds.), Structural equation modeling: a second course (2nd ed.). Greenwich: Information Age Publishing.
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). Acceptance and commitment therapy: model, processes and outcomes. Behavior Research and Therapy, 44, 1–25.
Heeren, A., Van Broeck, N., & Philippot, P. (2009). The effects of mindfulness on executive processes and autobiographical memory specificity. Behaviour Research and Therapy, 47(5), 403–409.
Helsen, K., Goubert, L., Peters, M. L., & Vlaeyen, J. W. S. (2011). Observational learning and pain-related fear: an experimental study with colored cold pressor tasks. The Journal of Pain, 12(12), 1230–1239.
Hoge, E. A., Bui, E., Palitz, S. A., Schwarz, N. R., Owens, M. E., Johnston, J. M., … Simon, N. M. (2018). The effect of mindfulness meditation training on biological acute stress responses in generalized anxiety disorder. Psychiatry Research.
IASP. (1979). Pain terms: a list with definitions and notes on usage. Recommended by the IASP subcommittee on taxonomy. Pain, 6, 249.
Jackson, D. C., Mueller, C. J., Dolski, I., Dalton, K. M., Nitschke, J. B., Urry, H. L., et al. (2003). Now you feel it, now you don’t: frontal brain electrical asymmetry and individual differences in emotion regulation. Psychological Science, 14(6), 612–617.
Jha, A. P., Stanley, E. A., Kiyonaga, A., Wong, L., & Gelfand, L. (2010). Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion, 10(1), 54–64.
Joormann, J. (2006). The relation of rumination and inhibition: evidence from a negative priming task. Cognitive Therapy and Research, 30, 149–160.
Kadziolka, M. J., Di Pierdomenico, E., & Miller, C. J. (2016). Trait-like mindfulness promotes healthy self-regulation of stress. Mindfulness, 7(1), 236–245.
Kaiser, R. H., AndrewsHanna, J. R., Metcalf, C. A., & Dimidjian, S. (2015). Dwell or decenter? Rumination and decentering predict working memory updating after interpersonal criticism. Cognitive Therapy and Research, 39(6), 744–753.
Kelly, C. B., & Cooper, S. J. (1998). Plasma norepinephrine response to a cold pressor test in subtypes of depressive illness. Psychiatry Research, 81(1), 39–50.
Keng, S., Smoski, M. J., & Robins, C. J. (2011). Effects of mindfulness on psychological health: a review of empirical studies. Clinical Psychology Review, 31(6), 1041–1056.
Khoury, B., Sharma, M., Rush, S. E., & Fournier, C. (2015). Mindfulness-based stress reduction for healthy individuals: a meta-analysis. Journal of Psychosomatic Research, 78(6), 519–528.
Kiken, L. G., & Shook, N. J. (2011). Looking up: mindfulness increases positive judgments and reduces negativity bias. Social Psychological and Personality Science, 2(4), 425–431.
Kingston, J., Chadwick, P., Meron, D., & Skinner, T. C. (2007). A pilot randomized control trial investigating the effect of mindfulness practice on pain tolerance, psychological well-being, and physiological activity. Journal of Psychosomatic Research, 62(3), 297–300.
Koster, E. H. W., De Lissnyder, E., Derakshan, N., & De Raedt, R. (2011). Understanding depressive rumination from a cognitive science perspective: the impaired disengagement hypothesis. Clinical Psychology Review, 31(1), 138–145.
Lao, S., Kissane, D., & Meadows, G. (2016). Cognitive effects of MBSR/MBCT: a systematic review of neuropsychological outcomes. Consciousness and Cognition: An International Journal, 45, 109–123.
Larsen, R. J. (2000). Toward a science of mood regulation. Psychological Inquiry, 11, 129–141.
Lau, M. A., Bishop, S. R., Segal, Z. V., Buis, T., Anderson, N. D., Carlson, L., et al. (2006). The Toronto Mindfulness Scale: development and validation. Journal of Clinical Psychology, 62, 1445–1467.
Laurent, H. K., Laurent, S. M., Lightcap, A., & Nelson, B. W. (2016). How situational mindfulness during conflict stress relates to well-being. Mindfulness, 7(4), 909–915.
Lee, J. E., Watson, D., & Law, L. A. F. (2010). Lower-order pain-related constructs are more predictive of cold pressor pain ratings than higher-order personality traits. The Journal of Pain, 11(7), 681–691.
Liu, X., Wang, S., Chang, S., Chen, W., & Si, M. (2013). Effect of brief mindfulness intervention on tolerance and distress of pain induced by cold-pressor task. Stress and Health: Journal of the International Society for the Investigation of Stress, 29(3), 199–204.
Martin, L. L., & Tesser, A. (1996). Some ruminative thoughts. In R. S. J. Wyer (Ed.), Ruminative thoughts (pp. 1–47). Hillsdale: Lawrence Erlbaum Associates.
McMullen, J., Barnes-Holmes, D., Barnes-Holmes, Y., Stewart, I., Luciano, C., & Cochrane, A. (2008). Acceptance versus distraction: Brief instructions, metaphors and exercises in increasing tolerance for self-delivered electric shocks. Behaviour Research and Therapy, 46(1), 122–129.
McRae, A. L., Saladin, M. E., Brady, K. T., Upadhyaya, H., Back, S. E., & Timmerman, M. A. (2006). Stress reactivity: Biological and subjective responses to the cold pressor and trier social stressors. Human Psychopharmacology: Clinical and Experimental, 21(6), 377–385.
Melzack, R. (1987). The short-form McGill pain questionnaire. Pain, 30(2), 191–197.
Melzack, R., & Katz, J. (2013). Pain. WIREs Cognitive Science, 4(1), 1–15.
Melzack, R., & Wall, P. D. (1965). Pain mechanisms: a new theory. Science, 150, 971–979.
Mitchell, L. A., MacDonald, R. A. R., & Brodie, E. E. (2004). Temperature and the cold pressor test. The Journal of Pain, 5(4), 233–238.
Molet, M., Macquet, B., Lefebvre, O., & Williams, K. D. (2013). A focused attention intervention for coping with ostracism. Consciousness and Cognition: An International Journal, 22(4), 1262–1270.
Moore, A., & Malinowski, P. (2009). Meditation, mindfulness and cognitive flexibility. Consciousness and Cognition: An International Journal, 18(1), 176–186.
Mrazek, M. D., Franklin, M. S., Phillips, D. T., Baird, B., & Schooler, J. W. (2013). Mindfulness training improves working memory capacity and GRE performance while reducing mind wandering. Psychological Science, 24(5), 776–781.
Nolen-Hoeksema, S. (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100(4), 569–582.
Noone, C., Bunting, B., & Hogan, M. J. (2016). Does mindfulness enhance critical thinking? Evidence for the mediating effects of executive functioning in the relationship between mindfulness and critical thinking. Frontiers in Psychology, 6, Art 2043-16.
O'Rourke, H. P., & MacKinnon, D. P. (2015). When the test of mediation is more powerful than the test of the total effect. Behavior Research Methods, 47(2), 424–442.
Ortner, C. N. M., Kilner, S. J., & Zelazo, P. D. (2007). Mindfulness meditation and reduced emotional interference on a cognitive task. Motivation and Emotion, 31(4), 271–283.
Ostafin, B. D., & Kassman, K. T. (2012). Stepping out of history: mindfulness improves insight problem solving. Consciousness and Cognition: An International Journal, 21(2), 1031–1036.
Perlman, D. M., Salomons, T. V., Davidson, R. J., & Lutz, A. (2010). Differential effects on pain intensity and unpleasantness of two meditation practices. Emotion, 10(1), 65–71.
Petter, M., McGrath, P. J., Chambers, C. T., & Dick, B. D. (2014). The effects of mindful attention and state mindfulness on acute experimental pain among adolescents. Journal of Pediatric Psychology, 39(5), 521–531.
Preacher, K. J., Rucker, D. D., & Hayes, A. F. (2007). Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivariate Behavioral Research, 42(1), 185–227.
Price, D. D., McGrath, P. A., Rafii, A., & Buckingham, B. (1983). The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain, 17(1), 45–56.
Prins, B., Decuypere, A., & Van Damme, S. (2014). Effects of mindfulness and distraction on pain depend upon individual differences in pain catastrophizing: an experimental study. European Journal of Pain, 18(9), 1307–1315.
Riva, P., Wesselmann, E. D., Wirth, J. H., Carter-Sowell, A. R., & Williams, K. D. (2014). When pain does not heal: the common antecedents and consequences of chronic social and physical pain. Basic and Applied Social Psychology, 36(4), 329–346.
Ruedy, N. E., & Schweitzer, M. E. (2011). In the moment: the effect of mindfulness on ethical decision making. Journal of Business Ethics, 95, 73–87.
Ryan, R. M., & Rigby, C. S. (2015). Did the Buddha have a self? No-self, self and mindfulness in Buddhist thought and western psychologies. In K. W. Brown, R. M. Ryan, & J. D. Creswell (Eds.), Handbook of mindfulness (pp. 245–265). New York: Guilford Press.
Saltzman, A., & Goldin, P. (2008). Mindfulness-based stress reduction for school-age children. In L. A. Greco & S. C. Hayes (Eds.), Acceptance and mindfulness treatments for children and adolescents: a practitioner’s guide (pp. 139–161). Oakland: New Harbinger Publications.
Schmeichel, B. J., Vohs, K. D., & Baumeister, R. F. (2003). Intellectual performance and ego depletion: role of the self in logical reasoning and other information processing. Journal of Personality and Social Psychology, 85(1), 33–46.
Schultz, P. P., & Ryan, R. M. (2015). The “why,” “what,” and “how” of healthy self-regulation: mindfulness and well-being from a self-determination theory perspective. In B. D. Ostafin, M. D. Robinson, & B. P. Meier (Eds.), Handbook of mindfulness and self-regulation (pp. 81–94). New York: Springer Science + Business Media.
Schultz, P. P., Ryan, R. M., Niemiec, C. P., Legate, N., & Williams, G. C. (2015). Mindfulness, work climate, and psychological need satisfaction in employee well-being. Mindfulness, 6(5), 971–985.
Schutze, R., Rees, C., Preece, M., & Schutze, M. (2010). Low mindfulness predicts pain catastrophizing in a fear-avoidance model of chronic pain. Pain, 148(1), 120–127.
Semple, R. J., Lee, J., Rosa, D., & Miller, L. F. (2010). A randomized trial of mindfulness-based cognitive therapy for children: promoting mindful attention to enhance social-emotional resiliency in children. Journal of Child and Family Studies, 19(2), 218–229.
Shallice, T., & Evans, M. E. (1978). The involvement of the frontal lobes in cognitive estimation. Cortex, 14, 294–303.
Sharpe, L., Perry, K. N., Rogers, P., Refshauge, K., & Nicholas, M. K. (2013). A comparison of the effect of mindfulness and relaxation on responses to acute experimental pain. European Journal of Pain, 17(5), 742–752.
Short, M. M., Mazmanian, D., Oinonen, K., & Mushquash, C. J. (2016). Executive function and self-regulation mediate dispositional mindfulness and well-being. Personality and Individual Differences, 93, 97–103.
Sullivan, M. J. L., Bishop, S. R., & Pivik, J. (1995). The pain catastrophizing scale: development and validation. Psychological Assessment, 7(4), 524–532.
Swain, N. R., & Trevena, J. (2014). A comparison of therapist-present or therapist-free delivery of very brief mindfulness and hypnosis for acute experimental pain. New Zealand Journal of Psychology, 43(3), 22–28.
Tang, Y., & Posner, M. I. (2009). Attention training and attention state training. Trends in Cognitive Sciences, 13(5), 222–227.
Tang, Y., Lu, Q., Geng, X., Stein, E. A., Yang, Y., & Posner, M. I. (2010). Short-term meditation induces white matter changes in the anterior cingulate. PNAS Proceedings of the National Academy of Sciences of the United States of America, 107(35), 15649–15652.
Teper, R., Segal, Z. V., & Inzlicht, M. (2013). Inside the mindful mind: how mindfulness enhances emotion regulation through improvements in executive control. Current Directions in Psychological Science, 22(6), 449–454.
Thorn, B. E., Clements, K. L., Ward, L. C., Dixon, K. E., Kersh, B. C., Boothby, J. L., & Chaplin, W. F. (2004). Personality factors in the explanation of sex differences in pain catastrophizing and response to experimental pain. The Clinical Journal of Pain, 20(5), 275–282.
Turk, D. C. (1996). Psychological aspects of chronic pain and disability. Journal of Musculoskeletal Pain, 4(4), 145–153.
Vohs, K. D., Baumeister, R. F., & Schmeichel, B. J. (2012). Motivation, personal beliefs, and limited resources all contribute to self-control. Journal of Experimental Social Psychology, 48(4), 943–947.
Weinstein, N., Brown, K. W., & Ryan, R. M. (2009). A multi-method examination of the effects of mindfulness on stress attribution, coping, and emotional well-being. Journal of Research in Personality, 43(3), 374–385.
Williams, J. M. G., & Swales, M. (2004). The use of mindfulness-based approaches for suicidal patients. Archives of Suicide Research, 8(4), 315–329.
Zalon, M. L. (1999). Comparison of pain measures in surgical patients. Journal of Nursing Measurement, 7(2), 135–152.
Zeidan, F., Gordon, N. S., Merchant, J., & Goolkasian, P. (2010). The effects of brief mindfulness meditation training on experimentally induced pain. The Journal of Pain, 11(3), 199–209.
Zeidan, F., Emerson, N. M., Farris, S. R., Ray, J. N., Jung, Y., McHaffie, J. G., & Coghill, R. C. (2015). Mindfulness meditation-based pain relief employs different neural mechanisms than placebo and sham mindfulness meditation-induced analgesia. The Journal of Neuroscience, 35(46), 15307–15325.
Arch, J. J., & Craske, M. G. (2010). Laboratory stressors in clinically anxious and non-anxious individuals: the moderating role of mindfulness. Behaviour Research and Therapy, 48(6), 495–505.
Author information
Authors and Affiliations
Contributions
PPS designed and executed the study, analyzed the data, and wrote the paper. RMR collaborated with the design, execution, writing of the study, and provided guidance with data analyses. All authors approved the final version of the manuscript for submission.
Corresponding author
Ethics declarations
Ethical approval was provided by research subjects review board at the University of Rochester. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Schultz, P.P., Ryan, R.M. Cognitive and Affective Benefits of a Mindful State in Response to and in Anticipation of Pain. Mindfulness 10, 657–669 (2019). https://doi.org/10.1007/s12671-018-1013-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-018-1013-1