
Abstract
Urban areas with rapid industrial development have major impacts on environmental soil quality. This study was carried out to determine contamination assessment of heavy metal concentration of urban soil from Klang district (Malaysia). Health risk assessment was used to determine potential health risks (carcinogenic and non-carcinogenic risks) in both adults and children. Moreover, this study was also used to identify the most significant contaminant and exposure pathway with regard to Klang urban soil. Mean bioavailability of heavy metal concentrations were found in the order of Fe (6.65 mg/kg) > Zn (5.61 mg/kg) > Cu (2.96 mg/kg) > Co (0.22 mg/kg) > Cd (0.14 mg/kg) > Pb (0.11 mg/kg) > Cr (0.10 mg/kg). Maximum values of Cd (0.64 mg/kg), Cu (52.14 mg/kg) and Pb (9.18 mg/kg) have exceeded some guidelines and standard values. Study findings showed that total carcinogenic risks values of Cd, Cr and Pb are more than incremental lifetime (1.0E-05). This indicates the likehood of having cancer threat for adults and children. While for total non-carcinogenic risk, none of the heavy metals (Co, Cr, Cu, Pb and Zn) showed Hazard Index values more than one indicating there is no any potential non-carcinogenic risks for adults and children in study area. From this study, Cd is the most significant contaminant as maximum concentration value has exceeded soil guidelines and potential to have carcinogenic risks to adults and children. Pathway order for both carcinogenic and non-carcinogenic risks is ingestion > dermal > inhalation where ingestion pathway contributed the most to potential health risks involving urban soil of Klang.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rapid urbanization is one of the most fundamental demographics taking place globally (United Nation Millennium Development Goals 2013). According to the World Economic and Social Survey (2013), rapid growth of economic activities is much more focused in urban areas. World Health Organization (2013) estimated that urban population growth of developing countries will increase to 5.2 billion in 2050. United Nation-Habitat (2004) reported that urban population increases proportionately with urbanization growth. Thus, urban areas have become a geographic focus of resource consumption and chemical emissions as well as critical influence on the environment and human health (Cachada et al. 2012). Major anthropogenic pollutant sources in urban area are industrial discharge, vehicle emissions, waste from municipal activities, fossil fuel combustion and non-combustion processes, open burning and building structure erosion (Karim and Qureshi 2013; Potsiou 2010). As one of the important component in urban ecosystem, urban soil is subjected to various pollutant accumulation, especially heavy metals. Heavy metal accumulation can remain for a long time and act as a sink and source of urban soil pollution. Studies done by Praveena et al. (2014) in Seri Kembangan (Malaysia), Olawoyin et al. (2012) in Niger Delta Area (Nigeria), Luo et al. (2012) in Xiamen Island (China) and Luo et al. (2011) in Hong Kong have showed that heavy metal accumulation in urban soil may result in further contamination in vegetation, surface and ground water, resulting in potential human health risk to local population.
In comparison with agricultural soil, urban soil especially in parks, residential and industrial areas may have direct influence on public health as it can be transferred into human bodies (Chen et al. 1997). Heavy metal accumulation in urban soil can be transferred into human bodies through inhalation of soil dust, soil ingestion and dermal contact (Guo et al. 2012; Chen et al. 1997). Heavy metals in urban soil can be transported into human body through soil dermal and oral ingestion, especially in young children during outdoor activities (Luo et al. 2011). Outdoor activities may results in oral soil ingestion from hand to mouth, while soil dermal adheres more easily to the skin especially for young children. Soil ingestion due to mouthing behavior of young children is an important potential pathway of exposure to estimate the amount of soil inadvertently ingested and may constitute a health risk. Additionally, soil can be easily resuspended in air by wind erosion or by human feet. Heavy metals in the soils can also generate airborne particles and dusts which can pose potential human health risk through inhalation (Chen et al. 1997).
For heavy metal determination in soil, total heavy metal concentration is commonly measured and assessed by comparison with soil quality standards (Scancar et al. 2000). However, total heavy metal concentration will overestimate pollution level and impacts of heavy metals on soil and water (Lee et al. 2006). Moreover, according to Karim and Qureshi (2013), total heavy metal concentration is insufficient for exposure and health risks assessment as well as inadequate for toxic effect determination. Therefore, a better appropriate method in soil analysis is crucial to determine its bioavailability. Heavy metals are present in various chemical forms with different solubility or bioavailability in soils. Using bioavailability of heavy metal concentration via in vitro digestion model provides more realistic exposure and health risk assessment. Using in vitro digestion model, bioavailability of heavy metals from soil to human in gastrointestinal tract can be investigated as an aspect of internal exposure. Among all in vitro digestion models, PBET is one of the most widely used models today that simulate contaminant mobilization in acidic conditions within stomach (Yuswir et al. 2013; Environment Agency 2002). By examining the bioavailability concentration of ingested heavy metals, exposure assessment from different exposure pathways can be determined (Luo et al. 2011; Imperato et al. 2003). Potential health risk involves Health Risk Assessment (HRA) with four main components, namely hazard identification, exposure assessment, dose–response and risk characterization (Lee et al. 2006). Hazard identification is achieved by examination of contaminant properties in terms of mobility and point of exposure. Exposure assessment requires possible exposures such as on air, water, and soil monitoring to avoid underestimating actual human exposure. Dose–response analysis evaluates information obtained during the hazard identification and estimates amount of a chemical likely to result in a particular health effect to human. Risk characterization brings together information developed in previous three steps to estimate health effects in an exposed population. Risk characterization represented quantitatively by carcinogenic and non-carcinogenic risks values to adults and children. Carcinogenic risk is often expressed as the maximum number of new cases of cancer projected to occur in a population of one million people due to exposure to the cancer-causing substance over a 70-year lifetime. Non-carcinogenic risk is usually determined by comparing the actual level of exposure to a chemical to the level of exposure that is not expected to cause any adverse effects, even in the most susceptible people (Man et al. 2010; Lee et al. 2006; Versantvoort et al. 2005; Alaska Department of Environmental Conservation 2000).
So far, many studies have examined the quality of urban soil (Guo et al. 2012; Olawoyin et al. 2012; Manta et al. 2002; Li et al. 2004). However, most of these studies applied total heavy metal concentration and performed in small urban areas (Cachada et al. 2012; Gallego et al. 2002). It is difficult to compare these with other studies due to methodology, contaminants studied and extraction differences. Past aspects of environmental research focusing on urban soils have involved total concentration, pollution extent and source identification of heavy metals. However, studies on bioavailability heavy metals concentration incorporation with HRA are still limited. So far, limited studies on bioavailability heavy metals concentration incorporation with HRA using urban soil were done in Karachi Pakistan (Karim and Qureshi 2013), Xiamen China (Luo et al. 2012), São Paulo city Brazil (Figueiredo et al. 2011). Incorporation of bioavailability of heavy metals in urban soil with health risk assessment is considered to be the most reliable and accurate method to estimate potential human health risk (Ruiz-Cortes et al. 2005). There are also little studies on heavy metals of urban soil in Malaysia, especially in main cities. A few studies associated with heavy metals contamination in urban soil in Malaysia have focused on total heavy metals concentration, contamination levels, spatial distribution, and sources (Najib et al. 2012; Engelsman et al. 2002). Knowledge of the total concentration of heavy metals is not enough to fully assess the human health risks and environmental impacts of urban soils. However, heavy metals of urban soils related to human health impacts, especially in rapidly growing urban areas surrounded by industrial activities, are still sparse in Malaysia. Earliest study to date on bioavailability of heavy metals in urban soils related to human health impacts is done by Praveena et al. (2014) in Seri Kembangan (Malaysia). Klang district is a rapid developing urban area with high population density in Malaysia. Although Klang district (Malaysia) is one of the busiest urban areas surrounded by various land and sea activities, studies of urban soil have been limited and comparative contributions of anthropogenic sources to heavy metals pollution in soil are also unclear.
Specific objectives of this study were to (1) examine bioavailability and contamination of heavy metal concentration of urban soil from Klang district (Malaysia) using soil guidelines and (2) characterize potential health risks on both adults and children and (3) evaluate the most significant contaminant and exposure pathway with regard to human health. Furthermore, output of this study will also help the state and federal government to plan their policy related to urban planning.
Materials and method
Study area and soil sampling
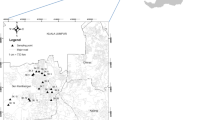
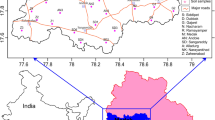
Klang district is a central urban area with a long history as royal city and former capital of the state of Selangor, Malaysia. Klang District comprises two sub-districts, namely Klang and Kapar, located 34 km away from Malaysia’s capital, Kuala Lumpur. Klang district is also one of the main gateways to Malaysia via sea where Port Klang is the 13th busiest transhipment port and the 16th busiest container port in the world. Rapid development including residential, industrial and other intensive commercial activates took place between 2000 and 2008. Since then, rapid development and increasing population have led to various environmental pollution problems. A total of 76 urban surface soil samples (at 0–10 cm in depth) were sampled randomly in September 2013. Global positioning system (GPS) was used to identify the locations (Fig. 1). The sampling was done based on the accessibility of the sampling locations. Surface soil was chosen for this study as this layer controls the exchange of metals between sediments and water. Surface soil samples were taken randomly using stainless steel scoops, placed in a polyethylene bag and labeled. Surface soil samples were kept cool in an icebox during transportation to laboratory. Surface soil samples were air-dried, homogenized, sieved through 2 mm mesh screen and stored in polyethylene bags.

Map showing the location of Klang district and urban soil sampling locations (n = 76)
Bioavailability of heavy metal determination
For determination of bioavailability of heavy metal, in vitro digestion model described by Man et al. (2010) was adapted in this study. This PBET in vitro digestion model is a static model where heavy metals in urban soil were extracted in acid conditions to simulate human stomach and intestinal conditions.
For bioavailability of heavy metals determination, physiologically based extraction test in vitro digestion model described by Man et al. (2010) was adapted in this study. This type of in vitro digestion model has been developed as simple, inexpensive tool to investigate the bioaccessibility of soil contaminants (Oomen et al. 2003). Simulations of both stomach and intestine conditions in human are the most important part in this study. Gastric solution for this model was prepared by adding 3 mL of NaCl, 0.5 g of malate, 0.430 mL of lactic acid, 0.5 mL of acetic acid and 1.25 g of pepsin (Sigma Chemical Co.) into 1 L of deionized water. This gastric solution has a pH of about pH of 1.5 adjusted using 12 M HCl. One gram of soil was added into 50 mL plastic centrifuge tube and 30 mL of prepared gastric solution was added and shaken with shaker using 55 rpm for 1 h at 37 °C. Simulation of gastric condition was changed to intestinal condition by adjusting pH to 7.0 using 1 M NaOH and 0.06 g of porcine bile extract and 0.018 g of porcine pancreatin (Sigma Chemical Co.) was added. During the intestinal condition simulation, the soil samples were shaken with same shaker used previously at 3300 rpm for 10 min at 37 °C. Then, the supernatant was filtered through a 0.45-µm Millipore filter to reduce any effects from microbial activity. The filtered supernatant was analyzed for heavy metal determination (Al, Cd, Co, Cr, Cu, Fe, Pb, Zn) using inductively coupled plasma atomic emission spectroscopy (ICP-AES) Pelkin Elmer Optima 8300. Bioavailability of heavy metal concentrations is defined as fractions which are bioavailable and mobilizable to human.
All the laboratory apparatuses were cleaned with 5 % (v/v) HNO3 and then rinsed with deionized water. The soil samples were digested in an airtight environment with closed digestion system to avoid volatilization and cross-contamination among samples. The operational condition was a cost-effective acid digestion method using closed polypropylene tubes as showed by Wheal et al. (2011). Screw-cap polypropylene (PP) tubes provide an alternative closed digestion vessel with several advantages over open digestion method. These PP tubes can tolerate temperatures of up to 130 °C without deforming and becoming translucent. Moreover, PP tubes are not re-usable, are inexpensive and costs of disposal are offset against time spent cleaning vessels. Significant disadvantages of microwave digestion are labor intensive cleaning, limited lifetime and replacement cost of vessels, need of additional decanting to correctly make to volume, with risks of sample loss and contamination (Sun et al. 2000). All reagents used were of analytical grade or equivalent and free from any contaminants that may have interfered with the analysis. Stock standard solution (Multi-element Calibration Standard 1, Perkin Elmer) was used to obtain calibration curves. Soil samples were analyzed in triplicates to assess the precision and accuracy of the analysis process. A method blank and a spiked blank were processed with each batch of 10 samples during sample analysis. Standard Reference Material (SRM) Montana II Soil (2711) obtained from National Institute of Standards and Technology (NIST) was included with every 10 samples to validate the accuracy of heavy metal analysis.
Potential human health risk assessment
HRA is a model developed to estimate the risk posed to human caused by contaminants. Risk assessment is a multi-step procedure comprising data collection and evaluation, exposure assessment, toxicity assessment, and risk characterization (Luo et al. 2012). Exposure of humans to heavy metals in urban soils can occur via three main pathways: direct oral ingestion of substrate particles, inhalation of resuspended particulates emitted from soil through the mouth and nose and dermal absorption of heavy metals in particles adhering to exposed skin (Luo et al. 2012). As a step of exposure assessment, a specific approach characteristic of human exposure to urban soil was applied to the non-carcinogenic hazard exposure for both children and adult. The carcinogenic risk was calculated for the lifetime exposure, estimated as the incremental probability of an individual developing cancer over a lifetime as a result of total exposure to the potential carcinogen. In order to evaluate health risk assessment through ingestion, inhalation and dermal exposure pathways on children and adults, the chronic daily intake (CDI) (mg/kg/day) of a contaminant was applied and Eqs. 1, 2 and 3 were used in the estimation of CDI via the three routes of exposure pathways. Exposure Factors Handbook (USEPA 2002), US Department of Environment (2011) and Department of Statistic Malaysia (2014) were used as a main guide to obtain the IngR, InhR, EF, ED, SA, AF, ABS and AT values in CDI calculation for soil (Table 1). Meanwhile, the RfD and cancer slope factor (CSF) values were taken from Integrated Risk Information System (USEPA 2012), and World Health Organization (2010) as shown in Table 2. For carcinogenic health risks, International Agency for Research on Cancer (IARC 2012) has classified heavy metals (Cd, Cr and Pb) as can induce carcinogenesis. According to IARC, Cobalt (Co), Chromium (Cr), Copper (Cu), iron (Fe), Plumbum (Pb) and Zinc (Zn) are classified as non-carcinogenic to humans.
where C soil is the concentration of the contaminant in soil (mg/kg), IngR is the ingestion rate of soil (mg/kg), EF is the exposure frequency (days/year), ED is the exposure duration (years), BW is the average body weight (kg), AT is the averaging time (days), CF is the conversion factor (1 × 10−6 kg/mg), SA is the surface area of the skin that contacts the soil (cm2), AFsoil is the skin adherence factor for soil (mg/cm2), ABS is the dermal absorption factor (chemical specific), InhR is the inhalation rate (m3/day) and PEF is the particle emission factor = 1.36 × 109 m3/kg.
Cumulative non- carcinogenic risk, expressed as the hazard index (HI) is equal to the sum of hazard quotient (HQ) as expressed in Eqs. 4 and 5. If the value of HI is less than one, it is believed that there is no significant risk of non-carcinogenic effects. If HI exceeds one, then there is a chance that non-carcinogenic risks effects may occur, with a probability which tends to increase as the value of HI increases (USEPA 2002).
The total lifetime cancer risk (LCR) is expressed as the sum of the carcinogenic risk from each exposure pathway (Eqs. 6 and 7). The acceptable or tolerable LCR for regulatory purposes is in the range of 1 × 10−6–1 × 10−4 (USEPA 2002).
Results and discussion
Contamination assessment
Bioavailability of heavy metal concentration found in urban soil of Klang (Malaysia) is presented in Table 3. Mean bioavailability concentrations of these heavy metals were found in the order of Fe > Zn > Cu > Co > Cd > Pb > Cr. Land use types influenced the heavy metal exposure corresponding to human health. Thus, comparison with soil guideline values is crucial to understand contamination of heavy metals in urban soil. However, according to Najib et al. (2012) and Ghazali (2010), no soil standards and protocols have been developed in Malaysia to evaluate contamination level in soil using bioavailability of heavy metal concentration. This situation is different for countries such as Canada, United Kingdom and United States of America in which soil guideline values of pollutants have been proposed based on bioavailability of heavy metal concentration and different land use types. Soil guidelines used based on different land use types are namely California Human Health SSLs (Cal/EPA 2005), Dutch Soil Guidelines (VROM 2000), Tolerable Daily Intake (TDI, Baars et al. 2001) and Maximum Permissible Level (MPL, USEPA 2008). From all the heavy metals, maximum values of Cd (0.64 mg/kg) and Cu (52.14 mg/kg) have exceeded the TDI and target values (Dutch Soil Guideline), respectively, while maximum values of Cu, Pb and Zn have exceeded California Human Health SSLs (Cal/EPA 2005) for residential and industrial areas.
According to Naji and Ismail (2011), surface sediments close to industrial and urban areas were more metal-enriched than those in other areas in Klang. Similarly, findings by Naji and Ismail (2011) showed that Cd enrichment in surface sediment of Klang river indicated high anthropogenic discharge and should be of major concern. Moreover, Klang district experienced rapid commercial and industrial development, which caused an increase in population, leading to contamination and deterioration of the environment (Sany et al. 2013). Cd is highly toxic and exposure to this metal is known to cause carcinogenic effects. On the other hand, Cu is considered to be probable cause of non-carcinogenic risks to children and adults. However, these is insufficient to elaborate carcinogenic and non-carcinogenic risks without a proper potential health risk assessment HRA. Moreover, there are also countries such as China and India which still use single soil guideline which may lead to misleading interpretation in human health risks. Thus, a proper interpretation of human health risk is a crucial step to enhance understanding of health risk or urban soil in Klang.
Potential human health risks of heavy metal in urban soil to adults and children
Some elements such as Cu and Zn are essential nutrients; however, in higher levels they have serious impacts on human health. Risk characterization was used to calculate carcinogenic and non-carcinogenic risks to heavy metals from soil through ingestion, inhalation and dermal pathways. Carcinogenic risk corresponds to an incremental lifetime of 1.0E-05. Non-carcinogenic risks with combined pathways (ingestion, inhalation and dermal pathways) correspond to hazard quotient of 1. Tables 4 and 5 show both carcinogenic and non carcinogenic risks of each heavy metals, cumulative HI and total risk values of combined heavy metals.
Heavy metals (Cd, Cr and Pb) have possibilities of inducing carcinogenic risks in adults and children. Carcinogenic risks of Cd, Cr and Pb are expected to be potential total cancer risk in Klang. Mean total carcinogenic risk values of Cd, Cr and Pb have exceeded incremental lifetime of 1.0E-05; thus the likehood of having cancer is evident for adults and children (Table 4). Suzana et al. (2008) and Shahar et al. (2010) showed that breast cancer remains the most common cancer among women in Malaysia, which accounted for 29.9 % of newly diagnosed cancer cases in Malaysian women registered in the national cancer registry. As shown in Figs. 2 and 3, children are more likely to have adverse effects of carcinogenic risks due to higher HI compared to adults. For the combined exposure pathways, total carcinogenic risk for children is nine times higher than that for adults for Cd, Cr and Pb (Figs. 2 and 3). For Cd, cumulative HI ingestion children to adult ratio is 9 to 1, while cumulative HI ingestion children to adult ratio is 9 for Cr and Pb. The study findings are similar to those of the study done by Luo et al. (2010), where ingestion pathway contributed most to the overall carcinogenic risk where probable toxicological risks are expected. Dermal and ingestion pathways have lower influence compared to ingestion pathway. Carcinogenic risks are disturbing and still need further toxicological study as these values suggest high risk to children health in this study area.

Potential carcinogenic risks induced by heavy metals (Cd, Cr and Pb) in urban soil of Klang for adults

Potential carcinogenic risks induced by heavy metals (Cd, Cr and Pb) in urban soil of Klang for children
Table 5 shows that HI values are lower than one indicating that there is no potential non-carcinogenic risks associated with exposure of Co, Cr, Cu, Pb and Zn expected in study area. For average non-carcinogenic risks in adults, heavy metals’ order of HI is Cu (0.0028) > Cr (0.0012) > Pb (0.0011) > Zn (0.00065) > Co (0.00058) > Fe (0.00033). For average non-carcinogenic risks in children, it is Cu (0.03) > Cr, Pb and Zn (0.01) > Co (0.0004) > Fe (0.003). The HI values lower than one incorporating three pathways suggested that there are no non-carcinogenic risks from exposure to these heavy metals for children and adults in study area. The pathway order for these heavy metals is ingestion > dermal > inhalation. Similarly to findings by Luo et al. (2012), for the three exposure pathways, obviously, ingestion was the dominant pathway contributing to HQ values although it is lower than one.
Conclusion
Bioavailability of heavy metal concentrations of Klang urban soil is generally in the order of Fe, Zn, Cu, Co, Cd, Pb. Among these heavy metals, Cd and Cu concentrations have exceeded soil guidelines and values. Potential health risks (carcinogenic and non-carcinogenic risks) in both adults and children were calculated using USEPA human health risk assessment. This study found that there is potential health risk from cumulative carcinogenic risks (Cd, Cr and Pb) on lifelong adults and children of Klang district. For non-carcinogenic risks, there is no potential non-carcinogenic health effects for both adults and children. This study has identified Cd as the most significant pollutant as its concentration has exceeded soil guidelines and potentially can cause carcinogenic effects on adults and children. Ingestion pathway was found as a major route with high HI and carcinogenic risk values in urban soil of Klang district. Moreover, these findings are capable of providing a direction to Klang district urban planning and policy. This study output also opens a wide direction on clinical toxicological research, especially on heavy metals which can cause carcinogenic risks (Cd, Cr and Pb) on children and adults living in Klang district.
References
Alaska Department of Environmental Conservation (2000) Human health risk assessment. Environmental cleanup educational tools series. Alaska Department of Environmental Conservation, Alaska
Baars AJ, Theelen RMC, Janssen PJCM, Hesse JM, van Apeldoorn ME, Meijerink MCM, Verdam L, Zeilmaker MJ (2001) Re-evaluation of human toxicological maximum permissible risk levels. RIVM Report 71170102. National Institute of Public Health and the Environment, Netherlands
Cachada A, Pereira ME, da Silva EF, Duarte AA (2012) Sources of potentially toxic elements and organic pollutants in an urban area subjected to an industrial impacts. Environ Monit Assess 184:15–32. doi:10.1007/s10661-011-1943-8
California Environmental Protection Agency (2005) Use of California human health screening levels (CHHSLs) in evaluation of contaminated properties. California Department of Environmental Protection, Calfornia
Chen TB, Wong JW, Zhou HY (1997) Assessment of trace metal distribution and contamination in surface soils of Hong Kong. Environ Pollut 96:61–68. doi:10.1016/S0269-7491(97)00003-1
Department of Statistic Malaysia (2014) Life expectancy for Malaysian. http://www.statistics.gov.my/portal/index. Accessed 24 February 2014
Engelsman W, Verburg P, Velkamp T, Sharifah Mastura SA (2002) Simulating land use changes in an urbanising area in Malaysia. Wageningen University, Netherlands
Figueiredo AMG, Tocchini M, dos Santos TFS (2011) Metals in playground soils of Sao Paulo city, Brazil. Procedia Environ Sci 4:303–309. doi:10.1016/j.proenv.2011.03.035
Gallego JLR, Ordóñez A, Loredo J (2002) Investigation of trace element sources from an industrialized area (Avilés, northern Spain) using multivariate statistical methods. Environ Int 27:589–596. doi:10.1016/S0160-4120(01)00115-5
Ghazali H (2010) Malaysia’s experience in developing the framework and guidelines for managing contaminated land. Department of Environment, Malaysia
Guo G, Wu F, Xie F, Zhang R (2012) Spatial distribution and pollution assessment of heavy metals in urban soils from southwest China. J Enviro Sci 24:410–418. doi:10.1016/S1001-0742(11)60762-6
Imperato M, Adamo P, Naimo D (2003) Spatial distribution of heavy metals in urban soils of Naples city (Italy). Environ Pollut 124:247–256. doi:10.1016/S0269-7491(02)00478-5
International Agency for Research on Cancer (IARC) (2012) Monograph on Cadmium, Chromium, Copper, Iron, Plumbum and Zinc. International Agency for Research on Cancer, Lyon
IRIS USEPA (2012) Integrated risk information system of the US Environmental Protection Agency. http://www.epa.gov/iris/. Accessed 24 February 2014
Karim Z, Qureshi BA (2013) Health risk assessment of heavy metals in urban soil of Karachi. Human and Ecological Risk Assessment, Pakistan. doi:10.1080/10807039.2013.791535
Lee SW, Lee BT, Kim JY, Kim KW, Lee JS (2006) Human risk assessment for heavy metals and As concentration in the abandoned metal mine areas, Korea. Environ Monit Assess 119:233–244. doi:10.1007/s10661-005-9024-5
Li X, Lee SL, Wong SC, Shi W, Thornton I (2004) The study of metal contamination in urban soils of Hong Kong using a GIS-based approach. Environ Pollut 129:113–124. doi:10.1016/j.envpol.2003.09.030
Luo XS, Yu S, Li XD (2011) Distribution, availability, and sources of trace metals in different particle size fractions of urban soils in Hong Kong: implications for assessing the risk to human health. Environ Pollut 159:1317–1326. doi:10.1016/j.envpol.2011.01.013
Luo XS, Ding J, Xu B, Wang YJ, Li HB, Yu S (2012) Incorporating bioaccessibility into human health risk assessments of heavy metals in urban park soils. Sci Total Environ 424:88–96. doi:10.1016/j.scitotenv.2012.02.053
Man YB, Sun XL, Zhao YG, Lopez BN, Chung SS, Wu SC, Cheung KC, Wong MH (2010) Health risk assessment of abandoned agricultural soils based on heavy metal contents in Hong Kong, the world’s most populated city. Environ Int 36:570–576. doi:10.1016/j.envint.2010.04.014
Manta DS, Angelone M, Bellanca A (2002) Heavy metals in urban soils: a case study from the city of Palermo (Sicily), Italy. Sci Total Environ 300:229–243. doi:10.1016/S0048-9697(02)00273-5
Naji A, Ismail A (2011) Metals fractionation and evaluation of their risk connected with urban and industrial influx in the Klang River surface sediments, Malaysia. Environment Asia 5:17–25
Najib NWAZ, Mohammed SA, Ismail SH (2012) Assessment of heavy metal in soil due to human activities in Kangar, Perlis, Malaysia. Int J Civil Environ Eng 12:28–33
Olawoyin R, Oyewole SA, Grayson RL (2012) Potential risk effect from elevated levels of soil heavy metals on human health in the Niger delta. Ecotox Environ Safety 85:120–130. doi:10.1016/j.ecoenv.2012.08.004
Oomen AG, Rompelberg CJM, Bruil MA, Dobbe CJG, Pereboom DPKH, Sips AJAM (2003) Development of an in vitro digestion model for estimation the bioaccessibility of soil contaminants. Arch Environ Contam Toxicol 44:281–287. doi:10.1007/s00244-002-1278-0
Potsiou C (2010) Rapid urbanization and mega cities: the need for spatial information management. The International Federation of Surveyors (FIG), Copenhagen
Praveena SM, Yuswir NS, Aris AZ, Hashim Z (2014) Potential health risk assessment of urban soil on heavy metal content in Seri Kembangan. In: Proceedings of the international conference on environmental forensics, Kuala Lumpur, Malaysia
Ruiz-Cortes E, Reinoso R, Diaz-Barrientos E, Madrid L (2005) Concentrations of potentially toxic metals in urban soils of Seville: relationship with different land uses. Environ Geochem Health 27:465–474
Sany SBT, Salleh A, Sulaiman AH, Sasekumar A, Rezayi M, Tehrani GM (2013) Heavy metal contamination in water and sediment of the Port Klang coastal area, Selangor, Malaysia. Environ Earth Sci 69:2013–2025. doi:10.1007/s12665-012-2038-8
Scancar J, Milacic R, Stratzar M (2000) Total metal concentrations and partitioning of Cd, Cr, Cu, Fe, Ni and Zn in sewage sludge. Sci Total Environ 250:9–19. http://dx.doi.org/10.1016/S0048-9697(99)00478-7
Shahar S, Salleh RM, Ghazali AR, Koon PB, Wan Mohamud WNW (2010) Roles of adiposity, lifetime physical activity and serum adiponectin in occurrence of breast cancer among Malaysian women in Klang Valley. Asian Pac J Cancer Prev 11:61–66
Sun DH, Waters JK, Mawhinney TP (2000) Determination of thirteen common elements in food samples by inductively coupled plasma atomic emission spectrometry: comparison of five digestion methods. J AOAC Int 5:1218–1224
Suzana S, Cham BG, Ahmad Rohi G, Mohd Rizal R, Fairulnizal MN, Normah H, Fatimah A (2008) Relationship between selenium and breast cancer: a case–control study in the Klang Valley. Singapore Medical J 50:265–269
United Nation Millennium Development Goals (2013) Millennium development goals (MDGs). Department of Economic and Social Affairs of the United Nations Secretariat, United Nations, New York
United Nation-Habitat (2004) The state of the world’s cities: globalization and urban culture. United Nations Human Settlements Programme. Earthscan, London
US Environmental Protection Agency (USEPA) (2002) Supplemental guidance for developing soil screening levels for superfund sites, OSWER 9355. Office of Emergency and Remedial Response, Washingston, DC, pp 4–24
US Environmental Protection Agency (2008) Child-specific exposure factors handbook (final report). US Environmental Protection Agency, Washington, DC (EPA/600/R-06/096F)
US Environmental Protection Agency (USEPA) (2011) Exposure factors handbook, 2011 edn. National Center for Environmental Assessment, Washington, DC (EPA/600/R-09/052F)
USDOE (2011) The risk Assessment information system (RAIS). US Department of Energy’s Oak Ridge Operations Office (ORO), Oak Ridge
Versantvoort CHM, Oomen AG, Kamp EVD, Rompelberg CJM, Sips AJAM (2005) Applicability of an in vitro digestion model in asssesing the bioaccessibility of mycotoxins from food. Food Chemical Toxicol 43:31–40. doi:10.1016/j.fct.2004.08.007
VROM (2000) Circular on target values and intervention values for soil remediation eAnnex A: target values, soil remediation intervention values and indicative levels for serious contamination. Dutch ministry of housing, spatial planning and environment
Wheal MS, Fowles TO, Palmer LT (2011) A cost-effective acid digestion method using closed polypropylene tubes for inductively coupled plasma optical emission spectrometry (ICP-OES) analysis of plant essential elements. Anal Methods 3:2854–2863. doi:10.1039/C1AY05430A
World Economic and Social Survey (2013) Sustainable development challenges. E/2013/50/Rev. 1 ST/ESA/344. United Nation
World Health Organization (1993) Guidelines for drinking-water quality, Volume 1. World Health Organization, Geneva
World Health Organization (2013) World health statistics 2013. WHO Press, World Health Organization, Geneva
Yuswir NS, Praveena SM, Aris AZ, Hashim Z (2013) Bioavailability of heavy metals using in vitro digestion model: a state of present knowledge. Rev Environ Health 128:181–187. doi:10.1515/reveh-2013-0012
Acknowledgments
The authors would like to thank Research University Grant Scheme (RUGS) vote number 9335100 for financial support. Special thanks to Miss Raihanah Binti Chokeli, Miss Nur Aida Binti Aziz and Mr. Fauzudin Bin Mislan for assistance during field sampling.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Praveena, S.M., Yuswir, N.S., Aris, A.Z. et al. Contamination assessment and potential human health risks of heavy metals in Klang urban soils: a preliminary study. Environ Earth Sci 73, 8155–8165 (2015). https://doi.org/10.1007/s12665-014-3974-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12665-014-3974-2