
Abstract
Background
Current gold standard for the diagnosis of gastroesophageal reflux disease (GERD) is 24-hour pH metry though it fails to detect non-acidic reflux. The sensitivity of 24-hour pH metry alone (both catheter-based and Bravo capsule) is questionable, especially if gastric acid secretion is low due to reduced parietal cell mass, Helicobacter pylori–induced gastric atrophy and antisecretory therapy. Accordingly, we analyzed the diagnostic ability of 24-hour pH metry as compared to impedance monitoring in relation to the gastric pH without antisecretory therapy.
Methods
A retrospective analysis of prospectively collected data from 150 patients with suspected GERD undergoing a 24-hour pH impedance study was done.
Results
Among 150 patients with symptoms suggestive of GERD, 106 (70.6%) had confirmed GERD diagnosed either by 24-hour pH metry alone (10 [9.4%]), impedance monitoring alone (49 [46.2%]) or both (47 [44.3%]). Abnormal reflux of acidic and non-acidic gastric contents was detected by 24-hour pH metry and 24-hour impedance monitoring in 57/106 (53.7%) and 96/106 (90.5%) of patients, respectively (p < .00001). Patients with GERD diagnosed by 24-hour impedance monitoring had a higher mean gastric pH (2.9 [median 1.3, IQR 5.3]) than those diagnosed by 24-hour pH metry (2.1 [median 1.4, IQR 2.6]) or both (1.6 [median 1.2, IQR 2.1]) (p = 0.001).
Conclusion
Twenty-four-hour impedance monitoring detects GERD more often than 24-hour pH metry. Patients with higher mean gastric pH leading to non-acidic reflux were more often diagnosed by 24-hour impedance monitoring than 24-hour pH metry. Thus, 24-hour pH metry alone is inferior to additional impedance monitoring in the diagnosis of GERD, particularly in presence of reduced gastric acid secretion.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The current gold standard for the diagnosis of gastroesophageal reflux disease (GERD) is 24-hour-pH monitoring, which measures pH in the distal esophagus [1,2,3]. Esophageal pH monitoring may be done using either a catheter-based system or a wireless pH monitoring capsule (Bravo capsule) [1, 4]. In the catheter-based system, a catheter with pH electrodes, connected to an external recorder, is introduced trans-nasally into the esophagus [5, 6]. The proximal electrode is placed 5 cm above the lower esophageal sphincter (LES), determined by manometry and the distal electrode is placed in the stomach to record gastric pH. Based on esophageal pH monitoring, GERD is diagnosed based on acid exposure time (AET, percentage of time with an esophageal pH < 4) of the total time [7,8,9]. However, an ambulatory 24-hour esophageal pH monitoring neither detects non-acidic reflux episodes, nor characterizes the nature of the refluxed contents (liquid, gaseous or mixed) [10].
In 1996, a novel method of esophageal function assessment was described by Skopnik and Silny, based on the principle of impedance [11]. This technique involves measuring the electrical conductivity of esophageal contents with a probes inserted transnasally. The results are interpreted based on differences in electrical conductivity and impedance between liquids, gas and solids. Electrical impedance (expressed in Ohms) around the catheter in an area between a pair of electrodes is inversely proportional to the electrical conductivity [12]. Liquid contents flowing from the stomach back into the esophagus cause increased electrical flow or decreased impedance due to its high ion concentration, whereas in the case of gaseous esophageal contents (belching), the impedance value is high, as there is no electrical flow between the electrodes. Incorporation of impedance and pH measuring channels in a single catheter system (multichannel intraluminal impedance monitoring combined with pH metry; MII-pH) has greatly improved the accuracy in the diagnosis of GERD [10, 13]. The distribution of impedance electrodes along a catheter also allows differentiation between antegrade propagation of esophageal contents (swallow) and retrograde bolus movements (reflux episodes). Combined esophageal pH impedance monitoring enables detection and characterization of all types of reflux episodes (acid, weakly acid, liquid, gaseous or mixed) [14,15,16,17]. This technique, thus, most importantly, can detect non-acid (pH > 4) reflux episodes, which are undetectable by pH monitoring alone.
There have been concerns about the sensitivity of 24-hour esophageal pH monitoring alone (both catheter-based and Bravo capsule) compared to 24-hour impedance monitoring in the detection of GERD, especially, if gastric acid secretion is low due to reduced parietal cell mass, Helicobacter pylori-induced gastric atrophy and in subjects on antisecretory therapy. Accordingly, we aimed at analyzing the diagnostic ability of 24-hour esophageal pH monitoring as compared to 24-hour impedance monitoring in relation to the gastric pH value in patients off-antisecretory therapy.
Methods
A retrospective analysis of prospectively collected data of 150 patients with suspected GERD referred to the GI Pathophysiology and Motility Laboratory for 24-hour pH impedance monitoring was done.
Patients
Consecutive patients with heartburn and regurgitation attending the gastroenterology outpatient service of a multi-level teaching institution were screened for GERD during four years (between December 2017 and November 2021) (Fig. 1). GERD was diagnosed clinically by the presence of typical symptoms of heartburn and/or regurgitation, which were bothersome to the patient, impairing quality of life and requiring consultation with a physician. Patients with large hiatus hernia, esophageal stricture or diverticula, gastric outlet obstruction, gastrointestinal (GI) neoplasms, peptic ulcer and previous history of GI surgery were excluded from the study. Those who met the inclusion criteria underwent 24-hour pH impedance monitoring while remaining off proton pump inhibitors (PPIs) and prokinetics for at least two weeks before the study and after obtaining informed consent. None of the patients enrolled in the study had history of intake of nitrates, calcium channel blockers or any other drug known to alter lower esophageal sphincter pressure or GI motility.

Study flow diagram. GERD gastroesophageal reflux disease
24-hour pH impedance monitoring
Combined 24-hour pH impedance monitoring was performed after an overnight fast using MII-pH monitoring system (Zephyr; Sandhill Scientific Inc., Highlands Ranch, CO, USA). The MII-pH probe had six impedance channels (four channels located in the distal esophagus at 3 cm, 5 cm, 7 cm, and 9 cm above the LES, while two channels were placed in the proximal esophagus at 15 cm and 17 cm above the LES) and two pH sensors placed 15 cm apart at the distal end of the probe. The pH probes were calibrated using standard buffers of pH 4.0 and pH 7.0 before each procedure. Before the start of impedance-pH metry, all patients had to undergo high-resolution esophageal manometry using a 32-pressure-channel solid-state system (Sandhill Scientific, Inc., Highlands Ranch, CO, USA) to localize and measure LES pressure. After localizing the LES, the proximal pH probe was placed 5 cm above it, while the distal probe was placed in the stomach. The former recorded the esophageal pH, while the latter recorded the gastric pH during the 24-hour study period. Patients were allowed to carry out regular activities and take regular meals but were advised against the intake of sour foods during the study period. Each patient was provided with a diary to record changes in posture, intake of meals and symptoms experienced during the study period. After the 24-hour study, data were transferred from the data logger to a computer for analysis of esophageal acid exposure (mean esophageal pH, percent total time pH less than 4 and per cent time pH less than 4 during upright and supine postures), gastric acid profile (mean gastric pH and per cent time gastric pH less than 4) and bolus exposure using impedance measurement.
24-hour pH and impedance analysis
Abnormal 24-hour esophageal acid exposure was considered when the per cent time esophageal pH was less than 4 for more than 4.2% of the total time on 24-hour pH metry based on the manufacturer’s instruction and earlier studies [8, 9, 18,19,20,21]. Patients were classified as having combined esophageal acid reflux if the per cent time esophageal pH was less than 4 during upright and supine postures were more than 6.3% and 1.2%, respectively, during the 24-hour study period.
Liquid bolus exposure was defined as a retrograde drop in impedance by 50% of the baseline. Abnormal 24-hour esophageal bolus exposure by impedance was defined as the percent time bolus exposure of more than 1.4% of total time. Combined GERD was defined when the per cent time bolus exposure during upright and supine postures was observed to be more than 2.1% and 0.7%, respectively, during the 24-hour study period. Reflux episodes detected by impedance were classified as “acidic” if the pH sensor recorded a decline in pH below 4 or “non-acidic” if the pH remained above 4 during the presence of bolus in the esophagus.
Statistical analysis
Data were checked for normal distribution using the Shapiro–Wilk test. Categorical variables were presented as proportion and inter-group comparisons of these data were performed by Chi-squared test with Yates’ correction, as applicable, or Fisher’s exact test. Continuous parametric and non-parametric data were presented as mean (standard deviation [SD]), median (inter-quartile range [IQR]). Comparison of parametric and non-parametric data of the two groups was done by unpaired t and Mann–Whitney U tests, respectively. Such data of more than two groups were compared using one-way analysis of variance and post-hoc Schiffe test or Kruskal–Wallis H test based on the distribution. Correlation between two continuous variables was performed using Pearson’s correlation method. P values of less than 0.05 were considered significant in all types of analysis. Statistical analysis was performed by R, EpiCalc and R Studio software (R Development Core Team, Vienna, Austria), MedCalc version 14 (Warandeberg 3, 1000 Brussels, Belgium) and Orange (Bioinformatics Lab at the University of Ljubljana, Slovenia).
Results
Among 150 patients with symptoms suggestive of GERD who underwent 24-hour pH impedance monitoring, 106 (70.6%) had confirmed GERD diagnosed either by 24-hour pH metry alone (10 [9.4%]), 24-hour impedance monitoring alone (49 [46.2%]) or both (47 [44.3%]) (Fig. 2). Both 24-hour pH and impedance monitoring were within the normal range in the remaining 44 patients (Fig. 3). Abnormal reflux of acidic and non-acidic gastric contents were detected by 24-hour pH metry and 24-hour impedance monitoring in 57 (53.7%) and 96 (90.5%) patients, respectively (p < 0.00001). Sixteen patients had small hiatus hernia on esophagogastroduodenoscopy, five had esophagitis (Los Angeles grade A in one and B and C each in two patients), and three had Barrett’s esophagus.

Venn diagram showing gastroesophageal reflux disease (GERD) diagnosed either by 24-hour pH metry alone, 24-hour impedance monitoring alone or both

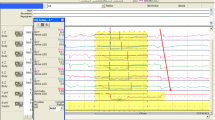
Figure showing that patients with gastroesophageal reflux disease (GERD) who had less acid secretion in the stomach (high pH, pH > 4) were more often diagnosed as GERD by 24-hour impedance monitoring than 24-hour pH metry alone
Demographic characteristics (Table 1)
Subjects diagnosed as GERD (either by 24-hour pH metry, 24-hour impedance monitoring or both) were more often males (70%, 71.4%, and 70.2%, respectively) as compared to those who had a normal study (45.5% males) (p = 0.035). GERD patients, positive by 24-hour pH metry were younger at presentation (31.8 ± 10.8) compared to those diagnosed by impedance monitoring (40.5 ± 12.4) or both (44.1 ± 15.6) (p = 0.049).
Esophageal acid exposure
Among 10 patients diagnosed with GERD by pH metry alone, six (60%) had reflux in the supine posture, four (40%) had reflux in both upright and supine positions and none had reflux in the upright posture alone. Among 47 patients diagnosed with GERD, both by pH and by impedance monitoring, nine (19.1%) had reflux in the supine posture, six (12.8%) had reflux in an upright posture and 32 (68.1%) had reflux in both positions. Abnormal esophageal acid reflux was absent in 48 (98%) patients with GERD diagnosed by 24-hour impedance monitoring. The total percentage time of esophageal acid reflux was observed to be higher in patients with GERD diagnosed by 24-hour pH metry (5.8% [median 4.9, IQR 17.4]) and combined 24-hour pH impedance monitoring (13% [median 7.9, IQR 26.2]) as compared to those diagnosed by impedance monitoring alone (0.7% [median 0.1, IQR 2.1]; p < 0.001). The number of episodes of acid reflux over five minutes was noted to be significantly higher in patients with GERD diagnosed by combined 24-hour pH impedance monitoring (7.3 [median 4, IQR 13.2]) and 24-hour pH metry (2.6 [median 1.4, IQR 6]) as compared to those diagnosed by 24-hour impedance monitoring alone, which recorded none (p < 0.001). Further, it was observed, GERD diagnosed by 24-hour pH metry and combined 24-hour pH impedance monitoring had significantly longer episodes of reflux (48.3 minutes [median 41.1, IQR 77.1]) and (38.5 minutes [median 19.6, IQR 94.1]), respectively, as compared to those diagnosed by 24-hour impedance monitoring alone (2.9 min [median 0.8, IQR 4.1]). The composite DeMeester scores were significantly higher in patients with GERD diagnosed by combined 24-hour pH impedance monitoring (44.6 [median 27, IQR 85.2]) and 24-hour pH metry (22.4 [median 19.8, IQR 56.6]) in comparison to those diagnosed by 24-hour impedance monitoring alone (3.3 [median 1, IQR 7.4]; p < 0.001).
Esophageal bolus exposure
Among 49 patients diagnosed with GERD by 24-hour impedance monitoring, two (4.1%) had bolus reflux in the supine posture, 14 (28.6%) had bolus reflux in an upright posture, while 33 (67.3%) had bolus reflux in both positions. Among 47 patients diagnosed with GERD by combined 24-hour pH impedance monitoring, seven (14.9%) had bolus reflux in the supine posture, six (12.8%) had bolus reflux in an upright posture, while 34 (72.3%) had bolus reflux in both positions. Esophageal bolus exposure was undetectable in nine (90%) patients with GERD diagnosed by 24-hour pH metry alone.
Trends of mean gastric pH and mean esophageal pH in patients with GERD
Patients diagnosed with GERD by 24-hour impedance monitoring had a higher mean gastric pH (2.9 [median 1.3, IQR 5.3]) as compared to those diagnosed by 24-hour pH metry (2.1 [median 1.4, IQR 2.6]) or both (1.6 [median 1.2, IQR 2.1]; p = 0.001). It was also observed that those diagnosed with GERD by impedance monitoring had a higher mean esophageal pH (6.3 [median 5.9, IQR 6.6]) as compared to those diagnosed by 24-hour pH metry (4.9 [median 3.6, IQR 5.2]) or both (5.1 [median 3.4, IQR 5.7]; p < 0.001). As seen in Fig. 3, most patients with GERD diagnosed either by 24-hour pH metry alone or both by pH-impedance monitoring had mean gastric pH less than 4 than those diagnosed either by impedance monitoring alone or not having GERD.
Discussion
The current study showed that (i) 24-hour pH metry alone missed the diagnosis of GERD in more than 90% of our study population and 24-hour impedance monitoring was far more superior to pick up the diagnosis of GERD and (ii) patients with GERD diagnosed by 24-hour impedance monitoring had a higher mean gastric pH than those diagnosed by 24-hour pH metry suggesting that the diagnosis of GERD was missed in a large proportion of patients with high gastric pH leading to non-acidic or weakly acidic reflux. Both these findings have considerable clinical implications in the management of patients with GERD.
Twenty-four-hour pH metry has been considered the gold standard for diagnosis of GERD in the recent past though currently, it has been largely replaced by combined pH-impedance monitoring [1,2,3]. However, even now some centers do perform 24-hour pH metry alone to diagnose GERD. Moreover, Bravo Calibration-free Reflux Capsule (Medtronic, Houston, TX, USA) and Alphaone (Chong Qing Jinshan Science and Technology Group Co. Ltd., Chongqing, China) pH metry, in which pH-sensitive capsules are placed in the distal esophagus endoscopically to record pH for more than 24 hours, have been also popularized for diagnosis of GERD. A few studies compared the diagnostic utility of 24-hour catheter-based pH metry with a prolonged recording of distal esophageal pH by Bravo capsule to diagnose GERD [22, 23]. Some of these studies showed the superiority of a prolonged recording of distal esophageal pH by Bravo capsule compared to the 24-hour recording by catheter-based pH metry [23,24,25]. Since we missed the diagnosis of GERD in more than 90% of patients on 24-hour pH metry alone, our data raise considerable doubt on the diagnostic ability of prolonged pH metry by Bravo capsule or similar technologies. Moreover, since Bravo capsule pH metry records only the distal esophageal and not gastric pH, the investigators do not have the opportunity to be particularly careful while interpreting the results in patients with less acidic stomach. A comparative study on catheter-based 24-hour pH-impedance monitoring and longer recording of esophageal pH by Bravo capsule is urgently needed.
The diagnostic utility of impedance monitoring is expected to be particularly high in patients with non-acidic reflux [16]. Non-acidic reflux is expected to be higher among Indian patients with GERD due to multiple reasons. Parietal cell mass is known to be less in Indian subjects [26]. Pangastritis and gastric atrophy due to H. pylori infection are associated with reduced gastric acid secretion [27]. We earlier found gastric acid secretion and degree of esophagitis among patients with GERD with H. pylori infection to be lesser than those without the infection [28]. Moreover, over-the-counter availability and widespread use of PPIs are further expected to reduce gastric acid secretion among Indian subjects due to their misuse. Though for the diagnosis of GERD, 24-hour pH metry is performed without anti-secretary agents such as PPI for two to three weeks, patients may not comply with this advice as troublesome symptoms may recur following the withdrawal of drugs. Multichannel intra-luminal impedance monitoring combined with pH metry (MII-pH) enables detection and characterization of all types of reflux episodes (acid, weakly acid, liquid, gaseous or mixed) [15,16,17]. It is particularly useful in diagnosing reflux events, while on treatment with acid-lowering agents regardless of the pH value of the refluxate [29]. It also aids in investigating patients with atypical symptoms of GERD [30,31,32,33]. The Indian consensus on GERD by Indian Society of Gastroenterology states that 24-hour impedance pH monitoring off PPI is currently the gold standard for the diagnosis of GERD [34].
We further noted that patients with GERD diagnosed by 24-hour pH metry were younger compared to those diagnosed by 24-hour impedance monitoring or a combined method. This observation probably reflects the fact that, with higher age and longer duration of GERD, prolonged and frequent use of antisecretory therapy (PPI) leads to higher gastric pH due to gastric atrophy, particularly in the presence of H. pylori infection; this may be associated with increased non-acidic reflux, which is more often detected by 24-hour impedance monitoring. A few studies suggested that patients with H. pylori infection treated with PPI over a prolonged period may develop gastric atrophy [35]. Moreover, we have previously demonstrated that genetic factors, especially IL-1B-511*T/IL-1RN*1 haplotype, is associated with reduced risk of GERD, particularly among patients with H. pylori infection, probably because of higher gastric mucosal IL-1beta levels [36,37,38,39].
Data from our study may also have therapeutic implications. In patients with refractory GERD symptoms with low gastric secretion, as shown by the pre-treatment 24-hour pH metry study, but persistent non-acidic reflux on impedance monitoring, instead of increasing the dose of PPIs or addition of potassium competitive acid blockers, measures to reduce non-acidic or weakly acidic volume reflux with pharmacotherapy (e.g. prokinetics, baclofen, sodium alginate), surgical or endoscopic anti-reflux therapies may be tried.
Our study has a few limitations. Though infection with H. pylori, which is common in Indian population, [40] is expected to reduce gastric acid secretion due to gastric atrophy, [34, 36, 41] we did not perform gastric biopsy to look for the presence and degree of gastric atrophy and tests for H. pylori. As per our protocol, all patients had combined pH-impedance monitoring. We only analyzed the data of pH and impedance separately. None of the patients underwent pH metry alone. We did not systematically follow-up the patients for response to PPI treatment. Most of our patients had non-erosive disease. This might have resulted from the fact that those who had symptoms suggestive of GERD, but erosive disease, might not be referred for 24-hour pH-impedance monitoring to investigate for GERD. An unexpectedly large proportion of patients had high gastric pH (Fig. 3) in our study. This might result from multiple factors such as gastric atrophy, H. pylori infection and most importantly prolonged effect of prior PPI treatment and non-adherence to advise to stop PPI. We do not believe that the pH probe was incorrectly placed in such a large proportion of patients. Since our study is a real-life study, it may be of considerable clinical value. In fact, it supports our point on need for impedance monitoring in addition to 24-hour pH metry with greater degree to diagnose GERD in real-life situation.
In conclusion, the present study shows that 24-hour impedance monitoring detects GERD more often than 24-hour pH metry. Patients with higher mean gastric pH leading to non-acidic reflux were more often diagnosed by 24-hour impedance monitoring than 24-hour pH metry. Thus, 24-hour pH metry alone is inferior to additional impedance monitoring in the diagnosis of GERD, particularly in the presence of low gastric acid secretion. We consider that the current “gold standard” for diagnosis of GERD (24-hour pH metry) should be replaced with 24-hour pH impedance monitoring.
References
Wiener GJ, Morgan TM, Copper JB, et al. Ambulatory 24-hour esophageal pH monitoring. Reproducibility and variability of pH parameters. Dig Dis Sci. 1988;33:1127–33.
Fass R, Hell R, Sampliner RE, et al. Effect of ambulatory 24-hour esophageal pH monitoring on reflux-provoking activities. Dig Dis Sci. 1999;44:2263–9.
Bollschweiler E, Feussner H, Holscher AH, Siewert JR. pH monitoring: the gold standard in detection of gastrointestinal reflux disease? Dysphagia. 1993;8:118–21.
Monkemuller K, Neumann H, Fry LC, Kolfenbach S, Malfertheiner P. Catheter-free pH-metry using the Bravo capsule versus standard pH-metry in patients with non-erosive reflux disease (NERD). Z Gastroenterol. 2009;47:351–6.
Forootan M, Zojaji H, Ehsani MJ, Darvishi M. Advances in the diagnosis of GERD using the esophageal pH monitoring, gastro-esophageal impedance-pH monitoring, and pitfalls. Open Access Maced J Med Sci. 2018;6:1934–40.
Sararu ER, Enciu V, Peagu R, Fierbinteanu-Braticevici C. Advances in the diagnosis of GERD. Rom J Intern Med. 2021;59:3–9.
Gyawali CP, Kahrilas PJ, Savarino E, et al. Modern diagnosis of GERD: the Lyon Consensus. Gut. 2018;67:1351–62.
Dhiman RK, Saraswat VA, Naik SR. Ambulatory esophageal pH monitoring: technique, interpretations, and clinical indications. Dig Dis Sci. 2002;47:241–50.
Saraswat VA, Dhiman RK, Mishra A, Naik SR. Correlation of 24-hr esophageal pH patterns with clinical features and endoscopy in gastroesophageal reflux disease. Dig Dis Sci. 1994;39:199–205.
Hila A, Agrawal A, Castell DO. Combined multichannel intraluminal impedance and pH esophageal testing compared to pH alone for diagnosing both acid and weakly acidic gastroesophageal reflux. Clin Gastroenterol Hepatol. 2007;5:172–7.
Skopnik H, Silny J, Heiber O, Schulz J, Rau G, Heimann G. Gastroesophageal reflux in infants: evaluation of a new intraluminal impedance technique. J Pediatr Gastroenterol Nutr. 1996;23:591–8.
Nguyen HN, Domingues GR, Lammert F. Technological insights: combined impedance manometry for esophageal motility testing-current results and further implications. World J Gastroenterol. 2006;12:6266–73.
Shay SS, Bomeli S, Richter J. Multichannel intraluminal impedance accurately detects fasting, recumbent reflux events and their clearing. Am J Physiol Gastrointest Liver Physiol. 2002;283:G376–83.
Sifrim D, Holloway R, Silny J, et al. Acid, nonacid, and gas reflux in patients with gastroesophageal reflux disease during ambulatory 24-hour pH-impedance recordings. Gastroenterology. 2001;120:1588–98.
Roman S, Gyawali CP, Savarino E, et al. Ambulatory reflux monitoring for diagnosis of gastro-esophageal reflux disease: update of the Porto consensus and recommendations from an international consensus group. Neurogastroenterol Motil. 2017;29:1–15.
Bredenoord AJ. Impedance-pH monitoring: new standard for measuring gastro-oesophageal reflux. Neurogastroenterol Motil. 2008;20:434–9.
Tutuian R, Castell DO. Review article: complete gastro-oesophageal reflux monitoring - combined pH and impedance. Aliment Pharmacol Ther. 2006;24 Suppl 2:27–37.
Shay S, Tutuian R, Sifrim D, et al. Twenty-four hour ambulatory simultaneous impedance and pH monitoring: a multicenter report of normal values from 60 healthy volunteers. Am J Gastroenterol. 2004;99:1037–43.
Zentilin P, Iiritano E, Dulbecco P, et al. Normal values of 24-h ambulatory intraluminal impedance combined with pH-metry in subjects eating a Mediterranean diet. Dig Liver Dis. 2006;38:226–32.
Zerbib F, des Varannes SB, Roman S, et al. Normal values and day-to-day variability of 24-h ambulatory oesophageal impedance-pH monitoring in a Belgian-French cohort of healthy subjects. Aliment Pharmacol Ther. 2005;22:1011–21.
Dhiman RK, Saraswat VA, Mishra A, Naik SR. Inclusion of supine period in short-duration pH monitoring is essential in diagnosis of gastroesophageal reflux disease. Dig Dis Sci. 1996;41:764–72.
Hakanson BS, Berggren P, Granqvist S, Ljungqvist O, Thorell A. Comparison of wireless 48-h (Bravo) versus traditional ambulatory 24-h esophageal pH monitoring. Scand J Gastroenterol. 2009;44:276–83.
Gillies RS, Stratford JM, Booth MI, Dehn TC. Oesophageal pH monitoring using the Bravo catheter-free radio capsule. Eur J Gastroenterol Hepatol. 2007;19:57–63.
des Varannes SB, Mion F, Ducrotte P, et al. 2005 Simultaneous recordings of oesophageal acid exposure with conventional pH monitoring and a wireless system (Bravo). Gut. 2005;54:1682–6.
Pandolfino JE, Richter JE, Ours T, Guardino JM, Chapman J, Kahrilas PJ. Ambulatory esophageal pH monitoring using a wireless system. Am J Gastroenterol. 2003;98:740–9.
Naik SR, Bajaj SC, Goyal RK, Gupta DN, Chuttani HK. Parietal cell mass in healthy human stomach. Gastroenterology. 1971;61:682–5.
Smolka AJ, Schubert ML. Helicobacter pylori-induced changes in gastric acid secretion and upper gastrointestinal disease. Curr Top Microbiol Immunol. 2017;400:227–52.
Chourasia D, Misra A, Tripathi S, Krishnani N, Ghoshal UC. Patients with Helicobacter pylori infection have less severe gastroesophageal reflux disease: a study using endoscopy, 24-hour gastric and esophageal pH metry. Indian J Gastroenterol. 2011;30:12–21.
Galmiche JP. Impedance-pH monitoring in proton pump inhibitor resistant patients: ready for clinical application? Gut. 2006;55:1379–81.
Tutuian R. Update in the diagnosis of gastroesophageal reflux disease. J Gastrointestin Liver Dis. 2006;15:243–7.
Bajbouj M, Becker V, Neuber M, Schmid RM, Meining A. Combined pH-metry/impedance monitoring increases the diagnostic yield in patients with atypical gastroesophageal reflux symptoms. Digestion. 2007;76:223–8.
Blondeau K, Tack J. Pro: impedance testing is useful in the management of GERD. Am J Gastroenterol. 2009;104:2664–6.
Ghoshal UC, Singh R, Misra A. Esophageal function tests in clinical practice: a review. Trop Gastroenterol. 2010;31:145–54.
Bhatia SJ, Makharia GK, Abraham P, et al. Indian consensus on gastroesophageal reflux disease in adults: A position statement of the Indian Society of Gastroenterology. Indian J Gastroenterol. 2019;38:411–40.
Kuipers EJ, Lundell L, Klinkenberg-Knol EC, et al. Atrophic gastritis and Helicobacter pylori infection in patients with reflux esophagitis treated with omeprazole or fundoplication. N Engl J Med. 1996;334:1018–22.
Chourasia D, Achyut BR, Tripathi S, Mittal B, Mittal RD, Ghoshal UC. Genotypic and functional roles of IL-1B and IL-1RN on the risk of gastroesophageal reflux disease: the presence of IL-1B-511*T/IL-1RN*1 (T1) haplotype may protect against the disease. Am J Gastroenterol. 2009;104:2704–13.
Ghoshal UC, Chourasia D. Gastroesophageal reflux disease and Helicobacter pylori: what may be the relationship? J Neurogastroenterol Motil. 2010;16:243–50.
Achyut BR, Moorchung N, Mittal B. Genetic association of interleukin-1 haplotypes with gastritis and precancerous lesions in North Indians. Clin Exp Med. 2008;8:23–9.
Chourasia D, Ghoshal UC. Pathogenesis of gastro-oesophageal reflux disease: what role do Helicobacter pylori and host genetic factors play? Trop Gastroenterol. 2008;29:13–9.
Singh K, Ghoshal UC. Causal role of Helicobacter pylori infection in gastric cancer: an Asian enigma. World J Gastroenterol. 2006;12:1346–51.
Rai S, Kulkarni A, Ghoshal UC. Prevalence and risk factors for gastroesophageal reflux disease in the Indian population: a meta-analysis and meta-regression study. Indian J Gastroenterol. 2021;40:209–19.
Acknowledgements
The authors thank Mr. Raghunath of the GI Pathophysiology and Motility Laboratory in the Department of Gastroenterology for his support for this work.
Author information
Authors and Affiliations
Contributions
UCG: study concept, design, data analysis and writing and editing the paper; SNB, AE: collection of the data, contribution to writing; BF, APA and AM: performing the 24-hour pH and impedance studies and help during data collection. All authors read and approved the final version of the paper.
Corresponding author
Ethics declarations
Conflict of interest
UCG, SNB, AE, BF, APA and AM declare no competing interests.
Ethics approval
The study was performed in a manner to conform with the Helsinki Declaration of 1975, as revised in 2000 and 2008 concerning human and animal rights, and the authors followed the policy concerning informed consent as shown on Springer.com.
Disclaimer
The authors are solely responsible for the data and the content of the paper. In no way, the Honorary Editor-in-Chief, Editorial Board Members, printer/publishers or the Indian Society of Gastroenterology are responsible for the results/ findings and content of this article. The opinions expressed in this paper are the independent opinion of the authors and are not influenced in any way by the funding bodies.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
UCG and SNB contributed equally to the work and are joint first authors of the paper.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ghoshal, U.C., Biswas, S.N., Elhence, A. et al. Twenty-four-hour pH metry alone is inferior to additional impedance monitoring in the diagnosis of gastroesophageal reflux disease, particularly in presence of reduced gastric acid secretion. Indian J Gastroenterol 42, 525–533 (2023). https://doi.org/10.1007/s12664-023-01359-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12664-023-01359-3