
Abstract
Background
Gallstones (GS) are formed as a result of impaired metabolic regulation and can be reflected in serum parameters. This study was focused on classifying GS based on spectral microanalysis and identifying the possible role of serum hepatic parameters on GS of different compositions.
Methods
The study included a total of 126 GS from 80 consecutive patients who underwent cholecystectomy for GS diseases in a single center. The composition and microstructure of GS were analyzed using Fourier-transform infrared (FTIR) spectroscopy, field emission scanning electron microscopy (FESEM), and energy dispersive X-ray spectroscopy (EDS). The serum hepatic parameters were studied in order to establish a possible etiologic relationship with GS composition.
Results
In the study group, the incidence of GS was higher in females 62 (77.5%) compared with males 18 (22.5%). The mean age was 42.81 ± 13.01 and 43.78 ± 14.4 years for female and male patients, respectively. Based on composition, the GS were assigned to four major groups: cholesterol, pigment, phosphate, and mixed stones. Mixed composition stones totally represented the majority 53 (66.3%), followed by pure cholesterol 23 (28.8%), pigment stones 2 (2.5%), and phosphate stones 2 (2.5%), respectively. Elemental composition revealed the presence of carbon (C), oxygen (O), calcium (Ca), and phosphorus (P) to be major elements along with traces of sodium (Na), magnesium (Mg), aluminum (Al), iron (Fe), copper (Cu), bromine (Br), manganese (Mn), and zinc (Zn). Among serum parameters, total bilirubin, direct bilirubin, indirect bilirubin, serum glutamic-oxaloacetic transaminase, and total protein were higher in patients with pigment GS than cholesterol GS.
Conclusions
Characterization of GS indicates that different types of stones have different characteristics in terms of microstructure, elemental composition, and distribution. Serum hepatic function test profiles showed an association with the compositions of GS.

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gallstone (GS) disease is one of the major health problems in developed societies, affecting 10% to 15% of the adult population [1]. The incidence of GS is 15% in USA, 5.9% to 21.9% in Europe, 3% to 11% in China, and 4% to 15% in Asia [2, 3]. The estimated prevalence of GS in India is reported as 2% to 29% [4,5,6]. Regional differences in the GS composition are also observed among the Indian patients [7]. Geography, ethnicity, diet, rapid weight loss, and obesity play important role in the development of GS [1, 8].
Information on the chemical composition and elemental distribution of GS is essential for understanding its etiopathogenesis. Generally, GS are mainly composed of cholesterol, bilirubin, calcium carbonate, calcium phosphate, and traces of proteins [9,10,11,12]. In addition, trace elements such as chlorine (Cl), potassium (K), manganese (Mn), iron (Fe), aluminum (Al), and copper (Cu) are also present [13,14,15]. Knowledge on exact pathogenesis of GS is incomplete, possibly because of the complex interaction of various physiological, environmental, and genetic risk factors [16]. GS with cholesterol are generally formed due to high cholesterol concentration exceeding the normal levels in bile [17]. On the other hand, pigment stones occur when there is destruction of red blood cells leading to excess bilirubin in the bile. High lipid concentrations and biliary protein levels are important risk factors for the GS formation [18].
Lack of documentation on the characterization of surgically removed GS is a limitation for understanding the chemical nature of the stones. However, with some recent research based on the composition and microanalysis, more classes of GS have been identified [19]. The present study was carried out to understand the diversity in the composition of GS in patients with cholelithiasis who underwent cholecystectomy. In addition, liver function tests were compared in patients with cholesterol and pigment GS to find relationship correlate between hepatic parameters and development of GS of varying composition.
Methods
The study was approved by the Institutional Ethics Committee (Ref No. YUEC/52/2015) and written informed consent was obtained from all participants. All the patients had symptomatic GS. The diagnosis was done using ultrasound imaging. A total 126 GS from 80 patients who underwent laparoscopic cholecystectomy fulfilling the inclusion criteria were included. Patients with liver cirrhosis and biliary tract parasitic infection were excluded. Liver function test (LFT) was performed in all the patients. Total bilirubin was quantified by diphylline, diazonium salt method, direct bilirubin using spectrophotometric assay, serum glutamic oxaloacetic transaminase (SGOT) by enzymatic colorimetric method, serum glutamic pyruvic transaminase (SGPT) test was performed by the UV spectrometric method with B5P, total protein was quantified by Biuret endpoint method, and serum albumin was estimated by bromocresol green method. All the tests were performed at the clinical laboratory.
Fourier-transform infrared (FTIR), field emission scanning electron microscopy (FESEM), and energy dispersive X-ray spectroscopy (EDS) analysis
For FTIR spectra, surgically removed GS were washed with distilled water and air dried. Approximately 20 mg of stones was powdered and analyzed using Shimadzu IR Prestige 21 instrument [20,21,22,23]. The FTIR spectra were recorded at the range of 4000–400 cm−1 at 4 cm−1 resolution. Based on the IR spectra, the GS composition was determined [24]. Scanning electron microscopy was performed using 10 mg of the samples that were sputter coated with gold using a field emission scanning electron microscope (Carl Zeiss, Cambridge, Germany). The compositions and distribution of elements in GS were analyzed by EDS (Oxford Instruments, England). The microstructure was analyzed at × 1000–20000 magnification [25].
Statistical analysis
Statistical analysis was performed using SPSS software (Version 22; SPSS Inc.; Chicago, IL, USA). Continuous variables were reported as means ± standard deviations. Results for categorical data were summarized using frequencies and percentages. Independent t and Mann-Whitney U tests were used to compare the liver parameters among patients with cholesterol and pigment GS. The value of p < 0.05 was considered statistically significant.
Results
Patient demographics
The study included 80 patients, and among them, 62 (77.5%) were females and 18 (22.5%) were males (female to male ratio of 3.4:1). The mean age of the study group was 43.03 ± 13.24 years (range 17 to 76 years). Peak age group was 35–55 years followed by 15–35 years and above 55 years, respectively. Mean ages of presentation showed no significant difference between females and males (p > 0.05).
Characterization, FTIR spectral analysis, and composition of GS
Based on the composition analyzed by FTIR, the GS were classified into four major types as cholesterol, pigment, phosphate, and mixed stones (Table 1). The mixed stones were highly predominant (66.3%) and composed of two or more than two types of components. The main subtypes of mixed stones were cholesterol-phosphate, bilirubinate-phosphate, bilirubinate-calcium carbonate, cholesterol-bilirubinate-phosphate, cholesterol-bilirubinate, cholesterol-calcium carbonate, cholesterol-calcium carbonate-phosphate, cholesterol-calcium stearate, and bilirubin-calcium stearate.
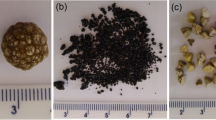
Cholesterol-containing stones were bigger in size and heavier compared with pigment stones (Table 2). Cholesterol stones appeared brownish yellow, gray, or black and mainly spherical in shape. Cross section showed radiating glistening crystals of different sizes (Fig. 1a). On the other hand, pigment stones were mostly amorphous, brittle, black, grayish brown, or charcoal gray and were harder than cholesterol stones (Fig. 1b). Phosphate stones were mainly soft and black in color (Fig. 1c) Most mixed stones were multifaceted, varying in size, appearing mainly black, light green, grayish black, brownish yellow, and spherical in shape (Fig. 1d-f).

Physical appearance of surgically removed gallstones. (a) Pure cholesterol stone; inset—cross section showing radiating glistening cholesterol crystals. (b) Pigment stone showing homogenously distributed pigment material. (c) Phosphate stone. (d) Bilirubinate-calcium carbonate mixed stone. (e) Cholesterol-bilirubinate-phosphate mixed stone. (f) Bilirubinate-phosphate mixed stone; inset—cross section showing pigment and phosphate layers
The FTIR spectra of the cholesterol and pigment GS are shown in Fig. 2 (a,b). The GS with phosphate content showed characteristic vibration frequency arising from PO43− at 1036 cm−1, 605 cm−1, and 564 cm−1 (Fig. 2c). Cholesterol-bilirubinate mixed stones showed peaks at 1663.71 cm−1, 1571.9 cm−1, and 1247.2 cm−1 due to absorption peaks of bilirubin and bilirubinate; 1466 cm−1, 1377 cm−1, and 1057 cm−1 were indicative of cholesterol. Bilirubinate-phosphate mixed stones similarly showed vibrational frequencies representing the absorption peaks of bilirubin/bilirubinate, and of phosphate. Bilirubinate-calcium carbonate mixed stones showed vibrational frequencies at 1454.3 cm−1, 854 cm−1, 700 cm−1, and 688 cm−1 of calcium carbonate in addition to bilirubin and bilirubinate peaks. Similarly, cholesterol-phosphate mixed stone showed peaks corresponding to phosphate at 1031 cm−1, 602 cm−1, and 551.64 cm−1 in addition to cholesterol peaks (Fig. 2d).

Fourier-transform infrared spectra of five gallstone types with characteristic peaks marked. (a) Pure cholesterol stone. (b) Pigment stone. (c) Phosphate stone. (d) Cholesterol-phosphate mixed stone: 2872 cm−1, 1466 cm−1, 1377 cm−1, and 1057 cm−1 characteristic absorption peaks of cholesterol and 1036 cm−1 and 605 cm−1 are the characteristic absorption peaks of phosphate. (e) Cholesterol-bilirubinate-phosphate mixed stone: 2872 cm−1, 1466 cm−1, 1377 cm−1, and 1057 cm−1 are the characteristic absorption peaks of cholesterol, 1663 cm−1 and 1629 cm−1 are of bilirubin and bilirubinate, and 1036 cm−1 and 605 cm−1 are of phosphate
Microstructure and elemental composition
The microstructure of all types of GS is presented as representative micrographs in Fig. 3. FESEM analysis revealed that cholesterol stones were mainly composed of plate-like or lamellar, cholesterol crystals with an irregular arrangement (Fig. 3a). Pigment stones showed different sizes, clumped sphere-like or irregular bilirubinate particles (Fig. 3b). The shape and the microstructure of mixed stones varied depending on the components.

Scanning electron microphotographs showing microstructure of different types of gallstones. (a) Cholesterol stone, showing plate- and lamella-shaped cholesterol crystals. (b) Pigment stone, showing irregularly arranged, clumped bilirubinate particle. (c) Cholesterol-bilirubinate mixed stone, showing plate-like cholesterol crystals with scattered bilirubinate particle. (d) Bilirubinate-calcium carbonate mixed stone, showing irregular bilirubinate particles and calcium carbonate crystals. (e) Bilirubinate-phosphate mixed stone, showing irregularly arranged bilirubinate particles and clumped phosphate crystals. (f) Cholesterol-calcium carbonate mixed stone, showing lamellar cholesterol and calcium carbonate crystals
The elemental composition of the GS obtained from EDS analysis is presented in S1 Fig. Cholesterol stones contained carbon (C), oxygen (O), calcium (Ca), sodium (Na), and magnesium (Mg) as major elements, with traces of Al, Cl, Fe, and silicon (Si). Pigment stones contained carbon, oxygen, iron, sodium, magnesium, aluminum, chlorine, and copper. The elemental composition of mixed stones was complex; cholesterol-phosphate mixed stone contained major elements such as Ca, O, C, and P, and boron (B), fluorine (F), Na, Al, sulfur (S), Cl, Mn, Cu, and zinc (Zn) as minor elements. Bilirubinate-phosphate mixed stones had similar elements as in cholesterol-phosphate mixed, in addition to Mg and Fe. Cholesterol-calcium carbonate mixed stones consisted of C, Ca, and O as major elements, whereas B, Fe, nitrogen (N), Na, Mg, Al, P, S, and Cl were also found in trace quantities.
Hepatic parameters and their association with GS
Results of LFT among patients with cholesterol and pigment GS are shown in Table 3. Comparison of hepatic parameters such as total bilirubin, direct bilirubin, indirect bilirubin, SGOT, SGPT, serum alkaline phosphatase (SAP), total protein, and serum globulin showed higher levels in patients with pigment GS than cholesterol GS. But serum albumin and albumin globulin ratio was higher in patients with cholesterol GS than pigment GS. The cholesterol mixed stones showed higher total bilirubin and SAP when compared with pure cholesterol, pure pigment, or other mixed types. Other parameters did not show differences in different stone types. None of the LFT parameters was significantly different between cholesterol and pigmented GS (p > 0.05).
Discussion
Among the stones analyzed, GS was more frequent in among the age group between 35 and 55 years. These observations are in conformity with earlier studies [26, 27]. GS patients included in the present study were more commonly females. Among the factors that contribute to a higher incidence of GS in females, female sex hormones, parity, oral contraceptive use, and estrogen replacement therapy are some of the important ones [28,29,30]. It has been also reported that females with obesity have an increased risk of GS formation [1].
Some of the studies reporting the biochemical compositions of GS among Indians are from the northern parts of India and studied mostly the cholesterol stones [31, 32]. However, a retrospective study from northern India (n = 1100) reported more than 62% of GS to be mixed in composition followed by pigment and cholesterol [33]. Similar results are found in our study; 69% of GS were of mixed composition followed by pure cholesterol, pigment, and phosphate stones. Higher frequency of cholesterol GS is generally observed in patients from developed countries [3].
Gallstone classification based on chemical analysis has gradually been recognized and widely used with the application of infrared spectroscopy [12, 34]. In this study, we could identify nine subtypes of GS by FTIR spectroscopy. The non-spectroscopic method is also used to determine the chemical composition of GS, and lack of specificity, sensitivity, and inaccuracy are common with such methods. Further, FESEM and EDS results provided strong evidence for the occurrence of multiple constituents in the cholesterol and pigment GS. Advanced technologies have made the identification of the microstructure and elemental compositions of GS easy [35].
Pathogenesis of GS is multifactorial and affected by a complex interaction of lifestyle, environmental, and genetic factors [36]. Cholesterol supersaturation, nucleation, precipitation, and gallbladder hypomotility are mainly associated with cholesterol stone formation in addition to the abnormal expression of the related genes [37]. Pigment GS are also associated with increased serum unconjugated bilirubin levels because the supersaturation of pigment stones occurs in presence of increased concentration of unconjugated bilirubin or free ionized Ca2+ in the bile [38]. This may be the reason for the increase in total, direct, and indirect bilirubin in patients with pigmented GS compared with cholesterol GS. The deconjugation of bilirubin by bacterial beta-glucuronidase results in precipitation of calcium bilirubinate, which contributes to pigment stone formation [38]. Knowledge about the color, appearance, and composition of GS is necessary as there are evidences which state black pigmented stones form only in the gallbladder as a result of hemolysis or abnormal erythropoiesis, whereas, the brown pigment stones can form at any part of the biliary duct or gallbladder caused by anaerobic bacterial infections [39]. Serum total protein was comparatively higher in female patients, most likely indicating an increase in gammaglobulin production resulting from the stimulation of the inflammatory response by the presence of the GS [40]. However, there was no significant association between the biochemical parameters among the GS with different compositions. The pigment stone can also form in patients with hemolytic disease [39]. The hepatic parameters highly vary in each patient of similar stone types. The GS composition may depend strongly on the other comorbidities, hepatobiliary conditions, lifestyle, and dietary habits. Careful investigations are needed to identify biomarkers for preventing the progression of the GS.
In conclusion, the study findings indicate that different types of stones have diversity in terms of the microstructure, elemental composition, and distribution. As GS may impair the normal digestive process, exploring into further role of hepatic parameters in different types of GS formation will be helpful in understanding the etiopathogenesis.
References
Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut Liver. 2012;6:172–87.
Everhart JE, Khare M, Hill M, Maurer KR. Prevalence and ethnic differences in gallbladder disease in the United States. Gastroenterology. 1999;117:632–9.
Stinton LM, Myers RP, Shaffer EA. Epidemiology of gallstones. Gastroenterol Clin N Am. 2010;39:157–69.
Sharma MP, Duphare HV, Nijhawan S, Dasarathy S. Gallstone disease in North India: clinical and ultrasound profile in a referral hospital. J Clin Gastroenterol. 1990;12:547–9.
Jayanthi V, Palanivelu C, Prasanthi R, Mathew S, Srinivasan V. Composition of gallstones in Coimbatore District of Tamil Nadu state. Indian J Gastroenterol. 1998;17:134–5.
Singh V, Trikha B, Nain C, Singh K, Bose S. Epidemiology of gallstone disease in Chandigarh: a community-based study. J Gastroenterol Hepatol. 2001;16:560–3.
Jayanthi V, Sarika S, Varghese J, et al. Composition of gallbladder bile in healthy individuals and patients with gallstone disease from North and South India. Indian J Gastroenterol. 2016;35:347–53.
Shaffer EA. Epidemiology of gallbladder stone disease. Best Pract Res Clin Gastroenterol. 2006;20:981–96.
Ravnborg L, Teilum D, Pedersen LR. Gallbladder stones classified by chemical analysis of cholesterol content. Frederiksberg, 1987-1988. Scand J Gastroenterol. 1990;25:720–4.
Duane WC. Pathogenesis of gallstones: implications for management. Hosp Pract (Off Ed). 1990;25:65–76.
Donovan JM, Carey MC. Physical-chemical basis of gallstone formation. Gastroenterol Clin N Am. 1991;20:47–66.
Zeng F, Hai H, Jin L. Analysis on infrared spectrum of human body gallstone with comparative method. Guang Pu Xue Yu Guang Pu Fen Xi. 2001;21:314–6.
Al-Kinani AT, Harris IA, Watt DE. Analysis of minor and trace elements in gallstones by induction of characteristic ionising radiation. Phys Med Biol. 1984;29:175–84.
Salimi J, Moosavi K, Vatankhah S. The concentration of heavy trace elements in pigment and cholesterol human gallstones: comparative studies by PIXE analysis. Iran J Radiat Res. 2003;1:93–7.
Omer LS. Quantitative analysis in (33) traces metals in human gallstones by ICP-AES. Int J Chem. 2011;3:105–10.
Johnston DE, Kaplan MM. Pathogenesis and treatment of gallstones. N Engl J Med. 1993;328:412–21.
Weerakoon HT, Ranasinghe S, Navaratne A, Sivakanesan R, Galketiya K, Rosairo S. Serum lipid concentrations in patients with cholesterol and pigment gallstones. BMC Res Notes. 2014;7:548.
Njeze GE. Gallstones. Niger J Surg. 2013;19:49–55.
Qiao T, Ma RH, Luo XB, Yang LQ, Luo ZL, Zheng PM. The systematic classification of gallbladder stones. PLoS One. 2013;8:e74887.
Manzoor MAP, Mujeeburahiman M, Rekha PD. Electron probe micro-analysis reveals the complexity of mineral deposition mechanisms in urinary stones. Urolithiasis. 2019;47:137–48.
Manzoor MAP, Mujeeburahiman M, Rekha PD. Association of serum biochemical panel with mineralogical composition of kidney stone in India. Acta Med Int. 2017;4:26–30.
Manzoor MAP, Duwal SR, Mujeeburahiman M, Rekha PD. Vitamin C inhibits crystallization of struvite from artificial urine in the presence of Pseudomonas aeruginosa. International Braz J Uro. 2018;44:1234–42.
Manzoor MAP, Mujeeburahiman M, Duwal SR, Rekha PD. Investigation on growth and morphology of in vitro generated struvite crystals. Biocatal Agric Biotechnol. 2019;17:566–70.
Weerakoon H, Navaratne A, Ranasinghe S, Sivakanesan R, Galketiya KB, Rosairo S. Chemical characterization of gallstones: an approach to explore the aetiopathogenesis of gallstone disease in Sri Lanka. PLoS One. 2015;10:e0121537.
Manzoor MAP, Singh B, Agrawal AK, Arun AB, Mujeeburahiman M, Rekha PD. Morphological and micro-tomographic study on evolution of struvite in synthetic urine infected with bacteria and investigation of its pathological biomineralization. PLoS One. 2018;13:e0202306.
Pundir CS, Chaudhary R, Rani K, Chandran P, Kumari M, Garg P. Chemical analysis of biliary calculi in Haryana. Indian J Surg. 2001;63:370–3.
Chandran P, Kuchhal NK, Garg P, Pundir CS. An extended chemical analysis of gallstone. Indian J Clin Biochem. 2007;22:145–50.
Thijs C, Knipschild P. Oral contraceptives and the risk of gallbladder disease: a meta-analysis. Am J Public Health. 1993;83:1113–20.
Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. JAMA. 1998;280:605–13.
Cirillo DJ, Wallace RB, Rodabough RJ, et al. Effect of estrogen therapy on gallbladder disease. JAMA. 2005;293:330–9.
Sarin SK, Kapur BML, Tandon RK. Cholesterol and pigment gallstones in northern India - a prospective analysis. Dig Dis Sci. 1986;31:1041–5.
Agarwal DK, Choudhuri G, Kumar J. Chemical nature and distribution of calcium compounds in radiolucent gallstones. Scand J Gastroenterol. 1993;28:613–6.
Mohan H, Punia RPS, Dhawan SB, Ahal S, Sekhon MS. Morphological spectrum of gallstone disease in 1100 cholecystectomies in North India. Indian J Surg. 2005;67:140–2.
Malet PF, Dabezies MA, Huang GH, Long WB, Gadacz TR, Soloway RD. Quantitative infrared spectroscopy of common bile duct gallstones. Gastroenterology. 1988;94:1217–21.
Manzoor MAP, Agrawal AK, Singh B, Mujeeburahiman M, Rekha PD. Morphological characteristics and microstructure of kidney stones using synchrotron radiation μCT reveal the mechanism of crystal growth and aggregation in mixed stones. PLoS One. 2019;14:e0214003.
Katsika D, Grjibovski A, Einarsson C, Lammert F, Lichtenstein P, Marschall HU. Genetic and environmental influences on symptomatic gallstone disease: a Swedish study of 43,141 twin pairs. Hepatology. 2005;41:1138–43.
Xiao ZL, Chen Q, Amaral J, Biancani P, Jensen RT, Behar J. CCK receptor dysfunction in muscle membranes from human gallbladders with cholesterol stones. Am J Physiol. 1999;276:G1401–7.
Acalovschi M. Gallstones in patients with liver cirrhosis: incidence, etiology, clinical and therapeutical aspects. World J Gastroenterol. 2014;20:7277–85.
Stewart L, Ponce R, Oesterk AL, Griffiss JM, Way LW. Pigment gallstone pathogenesis: slime production by biliary bacteria is more important than beta-glucuronidase production. J Gastrointest Surg. 2000;4:547–53.
Al-Kassab AS, Malatani TMS. The pattern of serum biochemical abnormalities in patients with gallstones. Eur J Clin Chem Clin Biochem. 1992;30:21–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
MAPM, ASS, SAK, MSM, and P-DR declare that they have no conflict of interests.
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (YUEC/52/2015) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards and the authors followed the policy concerning informed consent as shown on Springer.com.
Informed consent
Written informed consent was obtained from all individual participants included in the study.
Disclaimer
The authors are solely responsible for the findings and the content of the paper. In no way, the Honorary Editor-in-Chief, Editorial Board members, or the printer/publishers are responsible for the results/ findings and content of this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
S1Fig.
Elemental composition of different types of gallstones derived from Energy-dispersive X-ray spectroscopy. (a). Cholesterol stone. (b). Pigment stone. (c). Cholesterol-phosphate mixed stone. (d). Bilirubinate-calcium carbonate mixed stone. (e). Bilirubinate-phosphate mixed stone. (f). Cholesterol-calcium carbonate mixed stone. (PNG 1183 kb)
Rights and permissions
About this article

Cite this article
Manzoor, M.A.P., Sudhakar, A.S., Kadar, S.A. et al. Microstructural diversity of gallstones revealed by spectral microanalyses and their association with hepatic parameters. Indian J Gastroenterol 38, 391–398 (2019). https://doi.org/10.1007/s12664-019-00972-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12664-019-00972-5