
Abstract
Introduction
Lip and oral cavity cancer remains the most common cancer among Indian males and third most common cause of cancer-related deaths in India. Cervical lymph node metastasis is one of the most important prognostic factors in oral cavity cancer. The aim of present study was to estimate the prevalence of nodal involvement and analyse patterns of nodal metastasis in oral cavity cancer patients.
Methods
This prospective observational study was conducted between January 2019 and June 2020. Patients of oral cavity squamous cell carcinoma undergoing surgery with simultaneous neck dissection were included. Data pertaining to the clinical profile, treatment and histology details were collected and analysed.
Results
A total of 63 patients were included in present study. Out of 63 patients, unilateral neck dissection was performed in 47 (75%), while 16 (25%) underwent bilateral neck dissection. Overall clinical and pathological nodal positivity rates were 75% and 52%, respectively. Level I (48%) followed by IIa (20%) were most commonly involved stations. Combined involvement of level IV and V was seen in only 5%, and no skip metastasis was reported in level IV and V.
Conclusion
Level I and II are the most commonly involved stations in oral cavity squamous cell carcinoma (SCC). Oral SCC has a predictable nodal spread pattern with no skip metastasis to level IV/V noted in present study. There is a need for good quality randomised control trials to optimise the treatment protocols in clinically node-positive patients with respect to level IIB and V dissection.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
As per the GLOBOCAN 2020 data, a total of 3, 77, 713 new cases of lip and oral cavity cancer were diagnosed in 2020, out of which approximately one-third (1,35,929) were from India. Oral cavity cancer remains the most common cancer among Indian males (16.2%) and overall second most common cancer in India (10.3%). While globally it shares a very low fraction of annual cancer-related deaths (1.8%), it is the third most common cause (8.8%) of cancer-related deaths in India and contributed approximately 75,000 deaths in 2020 [1, 2]. Surgery remains the standard treatment for oral cancer and includes a margin-negative resection with addressal of regional nodes in the same sitting [3, 4]. Cervical lymph node metastasis is one of the most important prognostic factors in oral cavity cancer [5]. Appropriate neck node management is essential for an improved loco-regional control and overall survival [3, 4, 6]. Clinically N0 neck may harbour occult nodal metastases in 10–40% cases and an elective nodal dissection is the standard of care [3, 7,8,9]. Over years, neck dissection has evolved from radical to functional/selective neck dissection to minimise morbidity and improve the quality of life without compromising oncological outcomes [10, 11].
In comparison with the western world, advanced presentation of the primary and high clinical node positivity rate are common in Indian scenario [12, 13]. Still no reliable way (clinical or radiological) is available to identify cervical nodal metastasis preoperatively and only 40% of the clinically suspected nodes are actually found metastatic on final histology [7, 12]. Despite years of clinical experience and advances with the many ever-evolving guidelines, a clear guideline that ensures low failure rates without overtreatment is still desirable. The aim of present study was to estimate the prevalence of nodal involvement and analyse patterns of nodal metastasis in oral cavity cancer patients. We further tried to identify skip metastasis rate in levels IIb, IV and V to help generate optimal neck management guidelines in the oral cavity SCC.
Methods
After obtaining approval from the Institutional research ethics committee, the study was conducted in the department of surgical oncology and general surgery from January 2019 to June 2020. Patients in the age group 18–70 years, presenting with primary tumour of oral cavity with histological confirmation of squamous cell carcinoma (SCC) undergoing surgery with simultaneous neck dissection were included in present study. Patients with previous history of treatment for the primary cancer (surgery/chemotherapy/radiotherapy), those with clinical node larger than 3 cm or those with distant metastases were excluded from the study. A written, informed consent was obtained from all the participants before enrolment.
A detailed clinical evaluation of the patients was performed to know the status and extent of the index lesion and neck nodes. Clinical finding were supplemented with appropriate radiological imaging whenever required. Eighth edition of the AJCC/UICC manual was followed for staging. Composite resection or wide excision with three-dimensional one cm margins was performed in all patients with an en bloc skin or mandibular resection whenever required. All patients underwent comprehensive neck dissection (level I–V). Bilateral neck dissection was performed for patients with bilateral/contralateral nodal enlargement or when the disease was crossing the midline. All neck dissections were either performed directly or under supervision of the authors (AJ and AP) and same surgical principles were followed in all the surgeries. For proper histological assessment, pathological orientation of the specimen and margins were standardised. In the operating room nodal levels were marked as per anatomical location into levels—Ia, Ib, IIa, IIb, III, IV and V—and the specimens were sent in separate containers. All nodal stations were evaluated for total number of dissected nodes and total number of microscopically positive nodes. In total, 63 patients were enrolled in the present study. Data pertaining to the clinical profile, treatment and histology details were collected and analysed. Further, overall prevalence of nodal involvement and different patterns of lymphatic spread according to the various primary sub-sites were identified and analysed. Skip metastasis were defined as the presence of metastasis at lower levels in the absence of metastasis at all the levels above it. Rates of skip metastasis were analysed at level IV and V.
All the statistical analysis was performed using SPSS software (version 23.0, Chicago, IL). The categorical data were presented as frequency and percentage in contingency tables. The continuous variables were defined as mean (standard deviation) and/or median (range). Different qualitative variables were evaluated using Chi-square test. A p-value of less than 0.05 was considered significant.
Results
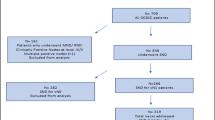
In the one and half year study period from January 2019 to June 2020, a total of 63 patients were included in present study.
Clinical Presentation and Demography
Mean age of the patients was 47.59 (SD ± 12.16) years with a male-to-female ratio of 3.84:1. Young patients of age group 20–40 years constituted 36% of the study population. Majority of the patients (54%) presented with ulcer in oral cavity and it was associated with pain in 46%. Mean duration of symptoms before presentation was 3.05 (SD ± 1.57) months and median duration from the first presentation to hospitalisation was 10 days. Alveolobuccal complex (30%), buccal mucosa (30%) and tongue (22%) were the most common sub-sites (Table 1). Clinically, neck nodes were palpable in 47 patients (74.60%). Details regarding clinical and pathological stage are mentioned in Table 2.
Surgical Details
Composite resection with mandibular resection was performed in 37 (58.73%) patients. All patients underwent margin-negative (R0) resection. Out of 63 patients, unilateral neck dissection was performed in 47 (75%), while 16 (25%) underwent bilateral neck dissection. Thus, results of total 79 neck dissections have been reported in the present study. Modified radical neck dissection type II (MND II) was performed most commonly, in 51 patients (64.5%), followed by MND III (34%). No intraoperative spinal accessory nerve injury was reported, however in one case nerve was sacrificed. Moderately differentiated histology was seen in 68.25% followed by well-differentiated tumours in 20 patients (31.75%). The mean duration of post-operative hospital stay (from the date of surgery to date of discharge) was 9.94 days with a median of 8 days.
Clinicopathological Correlation of Nodal Involvement
Overall pathological nodal positivity was seen in 33 patients (52.38%). Out of the 16 clinically node-negative patients, only two showed occult metastasis on final pathology. The sensitivity of clinical examination for nodal involvement was almost 94%, however specificity remained low at 46% (Table 3). Correlation between clinical T stage and pathological nodal status is shown in Table 4 (not significant p = 0.94) and sub-site-specific correlation between the clinical and pathological nodal positivity rates is shown in Fig. 1.

Correlation among clinical and pathological nodal station according to sub-site
Patterns of Nodal Involvement
Pathological nodal positivity was most commonly seen in level I (48%) followed by IIa (20%) (Table 5). The median number of dissected nodes was 38 (range 17–93) and median number of positive nodes in pN + was 2 (range 1–23). Numbers of nodes dissected at each level are summarised in Table 6. Extranodal spread was seen in 10 patients (12.65%). Pathological nodal positivity in level IV was seen in 3 patients (3.8%) and in level V in only 1 (1.27%) patient. In all three cases, level IV/V involvement was seen in ipsilateral neck with no contralateral involvement of level IV/V seen. There was no isolated metastasis to level IV/V in the present study and in all three cases, upper levels (level I–III) were also involved.
Discussion
Oral cavity cancer is a heterogeneous group of loco-regionally aggressive neoplasms. Oral cancer is one of the most common cancers in Indian subcontinent and squamous cell carcinoma is the most common histological sub-type [1, 13]. Disparity exists in the spectrum of distribution, and as opposed to the Global patterns, alveolobuccal cancer, instead of tongue, is the most common sub-site in India probably due to the peculiar and widespread use of the chewing tobacco [8, 13]. In the present study, alveolobuccal complex and buccal mucosa were the most common sub-sites and together contributed to 60% of the study population.
Main treatment of oral cavity SCC remains surgery, often followed by adjuvant radiotherapy depending upon the final stage and prognostic variables [3, 13]. Neck dissection is an integral part of the oral cancer surgery and also helps in deciding the need for adjuvant treatment [5, 12]. The management of neck has undergone a paradigm shift from the initial radical to a selective neck dissection approach to minimise the morbidity while maintaining the oncological safety [6, 10]. Selective neck dissection (SND) for clinically node-negative patients and comprehensive neck dissection for the node-positive patient are the current standard recommendations [4, 9]. The specificity of clinical neck examination is low and still remains a cause of major concern in decision-making [4, 7]. Overtreatment of neck is common in the Indian scenario because of advanced disease at presentation and significant nodal enlargement (clinical or radiological) preoperatively [12]. In the present study, 55 patients (87%) presented with advanced stage (clinical III/IV), and 47 patients (75%) had clinical nodal enlargement.
Incidence of occult nodal metastasis varies from 10 to 40%. Shah et al. reported incidence of occult metastasis in cN0 neck at 34% [9]. The incidence of occult neck metastasis was only 12.5% in our study. Major retrospective and prospective series have reported final pathological nodal positivity in the range of 20–50% irrespective of the clinical nodal status (cN0 or cN +). In a retrospective analysis of 945 oral cavity cancer patients, Deo et al. documented a 39.8% pathological nodal positivity rate [7]. Pathological nodal positivity rate was higher (52%) in our study probably because of advanced presentation of disease.
Various studies have shown that cervical nodal metastasis follows a predictable pattern and neck dissection can be tailored based on that knowledge [7, 10, 14, 15]. Level I and II are the most commonly involved groups irrespective of the oral cavity sub-site of origin. In study by Deo et al., level I (62.54%) was the most commonly involved level, followed by level II in 57.33% [7]. Pantvaidya et al. showed that combined positivity of level I–III was 91% [8]. In the present study, combined level I–III involvement reaches 94%. And, if we add level IV dissection nodal positivity reaches approximately 98% without adding much morbidity of level V LN dissection.
The rate of combined level IV and V involvement was only 6%. Among the three patients showing level IV involvement, two had alveolobuccal complex disease while the third one had carcinoma tongue. This patient with the tongue primary also had level V involvement, with metastases to all upper four levels of neck and extranodal extension of disease. The upper neck-level involvement (level I–III) and extranodal extension were predictors for involvement of level IV and V.
The concept of skip metastasis in oral cancer was first given by Rouviere in 1938 in carcinoma tongue [16]. Incidence of skip metastasis to level IV or V varies from 0–5% in oral cavity SCC [7, 17]. This idea of metastasis to lower levels (III–V) without involvement of upper levels (I/II) was properly described by Bayers et al. in a retrospective analysis of 277 carcinoma tongue patients. He reported that frequency of skip metastasis to level III or IV was 15.8% in SCC tongue. However, most patients in this analysis underwent level I–III dissection and level IV relapse was also considered as skip metastasis [14].
In retrospective analysis of 637 patients of oral cavity SCC, Feng et al. did not find any skip metastasis to level IV or V [18]. A prospective study of 583 lymph node dissections by Pantvaidya et al. showed the rate of skip metastasis to level III to be 17.5%, but no skip metastases were found in level IV or V [8]. Similarly, we did not discover any skip metastasis to level IV or V in our study despite having advanced presentation and higher overall nodal positivity rate in comparison with other studies. Incidence of level IV involvement varies from 3–15% [4, 7, 8]. A recent meta-analysis by Warshavsky et al. showed a level IV skip metastasis incidence rate of 0–5.5% [17]. In our study, level IV involvement was seen in only 3 (3.8%) patients with no skip metastasis. Despite having a low incidence of involvement, considering the low morbidity, level IV dissection can be performed routinely in clinically node-positive patients.
A careful decision regarding dissection of level IIB and V is important in view of the proximity with spinal accessory nerve. Various studies have shown that dissection at these two levels can be safely omitted in cN0 neck [7, 10, 19,20,21]. Omitting these two levels, however, remains controversial in clinically node-positive cases. Overall incidence of level V involvement varies from 0–5% and skip metastasis to level V varies from 0–4% [7, 8, 19]. Level V dissection carries a possible additional morbidity of shoulder dysfunction because of spinal accessory nerve handling [20, 21]. The incidence of level V involvement was only 1.25% and none had skip metastasis in the present study. So level V dissection can be safely omitted and in doubtful cases frozen of upper levels can be a useful adjunct. In a recent meta-analysis by Lea et al., the overall incidence of level IIB LN involvement in oral cavity SCC was 6% (95 CI 3.45–8.59) and incidence of skip metastasis was only 0.9% [22]. Studies have shown that level IIB sparing dissections are oncologically safe and avoid shoulder morbidity [23, 24]. In our study, level IIB involvement was seen in three patients (3.8%), out of which level IB was involved in all three and IIA was involved in two of them. So no skip metastasis was seen in level IIB group. Though we did not perform frozen section of above mentioned nodes in our study, but as shown by Gouri et al. and our results as well, frozen section study can be a useful tool for decision-making regarding level IIB dissection [8].
Limitations
In view of advanced presentation and high clinical nodal positivity, and to avoid treating surgeon’s bias, we decided to perform comprehensive neck dissection in all the patients which may have been an overtreatment in a few cases. Single-centre study with a small sample size, mainly due to the short study duration, was another limitation. No formal post-operative assessment of shoulder dysfunction and quality of life was performed which can be an important parameter with respect to level IIb and V dissection. Because of the short duration of study, recurrence patterns were not analysed.
Conclusion
Despite having a small sample size, this study generates a high quality prospectively collected data for nodal mapping. In the era of precision medicine the need for individualised treatment decisions is the key to success. In view of the low specificity of clinical examination, this cannot be relied upon. We did not find any skip metastasis to level IV or V and overall involvement of level IV/V was low in both clinically node-positive and node-negative patients. Selective neck dissection of level I–IV may be considered adequate in most of the oral cavity SCC both clinically N0 and N1. A careful individualised approach by including frozen section analysis for decision-making regarding level IIB and V can be adapted in clinical practice. There is a need for good quality randomised control trials to optimise the treatment protocols in clinically node-positive patients with respect to level IIB and V dissection.
References
356-india-fact-sheets.pdf. [cited 2021 May 1]. https://gco.iarc.fr/today/data/factsheets/populations/356-india-fact-sheets.pdf
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A et al (2021) Global cancer statistics 2020 GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71(3):209–249
D’Cruz AK, Vaish R, Kapre N, Dandekar M, Gupta S, Hawaldar R et al (2015) Elective versus therapeutic neck dissection in node-negative oral cancer. N Engl J Med 373(6):521–529
Shah JP, Candela FC, Poddar AK (1990) The patterns of cervical lymph node metastases from squamous carcinoma of the oral cavity. Cancer 66(1):109–113
Ferlito A, Silver CE, Rinaldo A (2007) Neck dissection in the new era. J Am Coll Surg 204(3):466–468
Byers RM, Wolf PF, Ballantyne AJ (1988) Rationale for elective modified neck dissection. Head Neck Surg 10(3):160–167
Deo S, Singh V, Mokkapati PR, Shukla NK, Dwivedi SN, Sharma A et al (2020) Clinical spectrum, pattern, and level-wise nodal involvement among oral squamous cell carcinoma patients - audit of 945 oral cancer patient data. Indian J Surg Oncol 11(1):86–91
Pantvaidya GH, Pal P, Vaidya AD, Pai PS, D’Cruz AK (2014) Prospective study of 583 neck dissections in oral cancers: implications for clinical practice. Head Neck 36(10):1503–1507
Shah JP (1990) Patterns of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. Am J Surg 160(4):405–409
Pantvaidya G, Rao K, D’Cruz A (2020) Management of the neck in oral cancers. Oral Oncol 100:104476
Harish K (2005) Neck dissections: radical to conservative. World J Surgical Oncol 3(1):1–13
Deo SVS, Shukla NK, Jha D, Khanna P, Pandit A, Thulkar S (2012) Are we over-treating neck in buccal & alveolo-buccal cancers: experience from a tertiary cancer care center. Indian J Surg Oncol 3(4):272–275
Deo SV, Jakhetiya A, NML M, Sreenivas V, Thulkar S, Bhasker S, &, Sharma A (2018) Clinical spectrum, treatment and relapse patterns in 353 patients with squamous cell carcinoma of the alveobuccal complex treated with a curative intent: a retrospective study. J Maxillofac Oral Surg 17(1):24–31
Byers RM, Weber RS, Andrews T, McGill D, Kare R, Wolf P (1997) Frequency and therapeutic implications of “skip metastases” in the neck from squamous carcinoma of the oral tongue. Head Neck 19(1):14–19
Woolgar JA (2007) The topography of cervical lymph node metastases revisited: the histological findings in 526 sides of neck dissection from 439 previously untreated patients. Int J Oral Maxillofac Surg 36(3):219–225
Kapoor C, Vaidya S, Wadhwan V, Malik S (2015) Lymph node metastasis: a bearing on prognosis in squamous cell carcinoma. Indian J Cancer 52(3):417
Warshavsky A, Rosen R, Nard-Carmel N, Abu-Ghanem S, Oestreicher-Kedem Y, Abergel A, Horowitz G (2019) Assessment of the rate of skip metastasis to neck level iv in patients with clinically node-negative neck oral cavity squamous cell carcinoma: a systematic review and meta-analysis. JAMA Otolaryngol-Head Neck Surg 145(6):542–548
Feng Z, Li JN, Niu LX, Guo CB (2014) Supraomohyoid neck dissection in the management of oral squamous cell carcinoma: special consideration for skip metastases at level IV or V. J Oral Maxillofac Surg 72(6):1203–1211
Lim YC, Koo BS, Lee JS, Choi EC (2006) Level V lymph node dissection in oral and oropharyngeal carcinoma patients with clinically node-positive neck: Is it absolutely necessary? Laryngoscope 116(7):1232–1235
Bradley PJ, Ferlito A, Silver CE, Takes RP, Woolgar JA, Strojan P et al (2011) Neck treatment and shoulder morbidity: still a challenge. Head Neck 33(7):1060–1067
Cappiello J, Piazza C, Giudice M, De Maria G, Nicolai P (2005) Shoulder disability after different selective neck dissections (levels II-IV versus levels II-V): a comparative study. Laryngoscope 115(2):259–263
Lea J, Bachar G, Sawka AM, Lakra DC, Gilbert RW, Irish JC et al (2010) Metastases to level IIb in squamous cell carcinoma of the oral cavity: a systematic review and meta-analysis. Head Neck 32(2):184–190
Bhattacharya A, Adwani D, Adwani N, Sharma V (2015) Is it worthy? removal of level IIB nodes during selective neck dissection (I-III) for oral carcinomas. Ann Maxillofac Surg 5(1):20–25
Pandey M, Karthikeyan S, Joshi D, Kumar M, Shukla M (2018) Results of a randomized controlled trial of level IIb preserving neck dissection in clinically node-negative squamous carcinoma of the oral cavity. World J Surg Oncol 16(1):219
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
They authors declare no conflict of interest.
Ethical standards
Institutional ethical committee clearance was obtained before enrollement.
Human and animals rights
This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed written consent was obtained from all the participants. Complete anonymity is maintained for all included participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mehta, N., Jakhetiya, A., Patel, D. et al. Prevalence and Patterns of Nodal Metastasis Among Oral Cavity Cancer Patients: A Prospective Observational Study. J. Maxillofac. Oral Surg. 22, 245–251 (2023). https://doi.org/10.1007/s12663-022-01739-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12663-022-01739-w