
Abstract
This narrative review critically evaluates the evidence for risk of anemia and red blood cell (RBC) transfusion. For this purpose, it assesses large prospective randomized-controlled trials (RCTs) in medical, surgical, and critical care patient populations in which the impact of specific hemoglobin transfusion thresholds are compared. In these trials, the risks of anemia relative to those of RBC transfusion are assessed. The results of published systematic reviews and meta-analyses are also discussed. Lastly, recommendations for patient blood management and treatment of anemia are explored. The main conclusion of this review emphasizes that the decision to transfuse RBCs is complex and depends on the interaction between multiple factors including the balance between the risk of anemia and the risk of RBC transfusion, existing patient comorbidities, and medical and surgical exposures. The transfusion thresholds recommended by current guidelines vary for medical and surgical patient populations. Guidelines suggesting specific transfusion thresholds for different patient populations should be viewed as a starting point for making an informed decision about RBC transfusion. Alternatives to transfusion (i.e., patient blood management), biomarkers of anemia-induced tissue hypoxia, and transfusion alternatives should continue to be evaluated in large RCTs, with the goal of improving event-free survival in critically ill and perioperative patients.
Résumé
Ce compte rendu narratif évalue de façon critique les données probantes concernant le risque de l’anémie et de la transfusion d’érythrocytes. Pour ce faire, nous avons évalué des études randomisées contrôlées (ERC) prospectives de grande envergure réalisées auprès de populations de patients médicaux, chirurgicaux et de soins intensifs dans lesquelles l’impact de seuils spécifiques de transfusion d’hémoglobine est comparé. Dans ces études, les risques de l’anémie sont comparés aux risques de la transfusion d’érythrocytes. Les résultats des comptes rendus systématiques et méta-analyses publiés sont également présentés. Enfin, les recommandations concernant la gestion du sang des patients et le traitement de l’anémie sont explorées. La conclusion principale de ce compte rendu souligne que la décision de transfuser des érythrocytes est complexe et dépend de l’interaction de plusieurs facteurs, notamment de l’équilibre entre le risque de l’anémie et le risque de la transfusion d’érythrocytes, les comorbidités existantes du patient, et les risques médicaux et chirurgicaux. Les seuils de transfusion recommandés par les directives actuelles sont différents pour les populations de patients médicaux et chirurgicaux. Les directives proposant des seuils de transfusion spécifiques en fonction des différentes populations de patients devraient être considérées comme point de départ pour prendre une décision informée concernant la transfusion d’érythrocytes. Les alternatives à la transfusion (c.-à-d. la gestion du sang des patients), les biomarqueurs d’une hypoxie tissulaire induite par l’anémie et les alternatives à la transfusion devraient continuer à être évalués dans des ERC d’envergure, avec pour but l’amélioration de la survie sans complication des patients en état critique et périopératoires.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
This narrative review assesses the balance of risks associated with anemia and acute blood loss vs those of red blood cell (RBC) transfusion and other treatments for anemia (Fig. 1). Both anemia and transfusion are associated with adverse clinical outcomes including increased mortality.1,2,3,4,5,6,7,8,9,10 Nevertheless, the potential direct causal links between anemia, RBC transfusion, adverse outcomes, and the potential interaction between anemia and transfusion are incompletely understood. Firstly, this review will assess the adverse effects of anemia by summarizing the reported risk of anemia in major clinical trials, meta-analyses, and translational studies. Important outcomes will include organ injury and mortality associated with acute and chronic anemia. As RBC transfusion remains one of the main treatments of acute and chronic anemia in critical care and perioperative settings, the potential risk of RBC transfusion will be assessed utilizing retrospective analyses and prospective randomized-controlled trials (RCTs). The rationale for proposed restrictive and liberal transfusion approaches will be reviewed within the context to determine the optimal transfusion thresholds in different patient populations. We then look at options for ameliorating the risk associated with both anemia and transfusion including patient blood management and anemia treatment algorithms, and assess the potential for treatment of anemia to avoid the adverse outcomes associated with anemia and RBC transfusion11,12,13 (Fig. 2).

Modified with permission from Nalla et al.12
A model to describe the risks of anemia and its treatment at varying hemoglobin concentrations. These risks are low at hemoglobin concentrations >100 g·L−1, and with decreasing hemoglobin levels, there is an increased risk of dysfunction and organ injury. The point at which the risk of anemia is balanced with the risks associated with red blood cell transfusion remains undefined, as outlined in the manuscript.

Anemia-induced tissue hypoxia may be a common unifying mechanism for organ injury and mortality. It remains undefined whether treatment of anemia restores tissue oxygen delivery, maintains cellular oxygen homeostasis, and prevents organ injury and mortality. There is evidence supporting inadequate physiologic adaptations to anemia leading to anemia-induced tissue hypoxia. Nevertheless, the causality between anemia-induced tissue hypoxia and organ injury and subsequent mortality has yet to be established.
The over-arching objective of this review is to understand that recommendations for hemoglobin (Hb) transfusion thresholds remain generally restrictive; however, the degree of restriction varies depending on the patient comorbidities and critical care or surgical exposure. Current RCTs are exploring the potential benefit or harm of more liberal transfusion thresholds in specific patient populations. Recommendations for Hb thresholds are a starting point for transfusion decisions, which should incorporate additional patient-specific factors to optimize patient care.
Defining anemia
An estimated 80% of our body’s cells are RBCs14 and Hb comprises the main component of RBC content. This emphasizes the importance of RBCs as the vehicle for Hb to carry oxygen and facilitate its effective delivery to peripheral tissues. Anemia is defined as a decreased number of RBCs and a reduced Hb concentration in the blood. Chlorosis (Greek for “green”) was an early term used to describe patients with anemia based on the patient’s appearance and skin colour.15 The recent evolution of the diagnosis and treatment of anemia was started by early western physicians such as Thomas Sydenham (England 1624–1689). Sydenham recognized the nutritional basis of anemia and was known to prescribe iron supplementation to treat it (e.g., “iron filings steeped in cold Rhenish wine”).15 Yet, despite decades of attention from the modern medical community, our knowledge of the pathophysiology and treatment of anemia remain incomplete. Anemia is defined by the World Health Organization as a Hb < 130 g·L−1 in men and < 120 g·L−1 in women.16 Anemia is a major global health burden, affecting approximately one third of the world’s population.17,18 While beyond the scope of this review, anemia is a leading cause of global years lived with a disability in young adults19 and has been associated with morbidity and mortality in patients of all ages (including neonates and children,20 pregnant women,21 adults, and the elderly.17,18,–19,22
What are the risks associated with perioperative anemia?
Within this section, we will review the risk to patients with pre-existing (i.e., chronic) anemia (largely due to iron deficiency or iron restriction), and the impact of acute anemia associated with acute surgical bleeding and fluid resuscitation. It is clear that both types of anemia may interact to contribute to adverse outcomes.
The risk of preoperative anemia
The adverse impact of anemia on perioperative outcomes has been previously reviewed.1,5,10,23 Recently published outcome data from the International Surgical Outcomes Study (ISOS) trial and other databases show that the prevalence of perioperative anemia remains high (approximately 30–40%) in patients undergoing surgery.17,24,25 The incidence of anemia is comparable (approximately 30%) in patients undergoing cardiac surgery.26 In both types of surgery, anemia is an independent risk factor for increased short- and long-term mortality.17,24,25,27,28 In these retrospective clinical studies, the presence of perioperative anemia has been associated with adverse outcomes including acute renal failure,5,6,24,25,28 myocardial infarction (MI),4,29 stroke,5,6,28 and increased mortality.1,17,24,25,27,28,30 In a recent meta-analysis by Fowler et al.,24 an association was found between pre-surgical anemia, postoperative acute kidney injury (AKI), stroke, death, and infection. In addition, Fowler et al.17 found that the risk of mortality and complications increased with worsening anemia in patients admitted for elective inpatient surgery, especially postoperative infection.
Anemic patients, when compared with non-anemic patients, were more likely to require treatment in the intensive care unit (ICU) and have a longer in-hospital stay.17 Lastly, investigators found that high income countries experienced fewer complications in their anemic patients than low to medium income countries, suggesting that anemia may be of greater concern in the latter.17 The mechanism by which anemia in surgical patients increases morbidity and mortality has not been established but the take home message is simple—anemia is associated with an increase in morbidity and mortality in patients undergoing surgery or with critical illnesses.
The risk of acute intraoperative anemia and hemodilution
Intraoperative acute anemia is a common event most often related to acute blood loss and/or concurrent hemodilution with intravenous fluids. This disruption of physiologic hemodynamics has been extensively modeled and studied in animal experiments.31,32,33,34,35 In surgical patients, the two patient populations who commonly suffer from moderate to severe acute hemodilution in the perioperative context are those who refuse transfusions for religious reasons1,2,4 and those undergoing cardiopulmonary bypass (CPB) for cardiac surgery.3,6,36,37 In these and other populations, acute hemodilutional anemia has been associated with worsened patient morbidity and mortality.1,2,3,4,5,6,36 In translational animal models, acute and subacute anemia increased expression of markers for tissue hypoxia, thus providing a possible causal link between anemia, tissue hypoxia, organ injury, and death (Fig. 2).
Animal models of acute and subacute anemia have identified several important concepts for understanding anemia. These include the finding that acute anemia leads to tissue hypoxia in vital organs including the brain, kidney, and liver.32,34,35,38 In addition, inhibition of active cardiovascular response to acute anemia by preventing the increase in cardiac output and cerebral vasodilation with β1 and β2 specific antagonists accentuated anemia-induced cerebral-tissue hypoxia.31,39,40,41 Further support for the importance of adaptive hypoxic cellular responses during anemia are provided by studies in which genetic deletion of neuronal nitric oxide synthase (nNOS) inhibited the molecular response of hypoxia signalling to anemia.34 Mice deficient in nNOS exhibited a severely attenuated hypoxic cellular response to acute anemia, and did not show the characteristic real-time increase in hypoxia-inducible factor-α normally observed in living transgenic hypoxia-inducible factor (HIF)-luciferase mice.34 These nNOS deficient mice also lacked the cardiac output response to acute anemia. Absence of these adaptive cellular and cardiovascular responses may have contributed to the observed increase in acute mortality in acutely anemic rodents.34 Thus, animal models of acute and subacute anemia show that anemia leads to tissue hypoxia despite the simultaneous activation of adaptive integrative physiologic responses to maintain tissue oxygen delivery. Inhibiting these responses increased the severity of tissue hypoxia31,40,41 and increased mortality.34
The impact of acute surgical blood loss resulting in anemia in patients who decline RBC transfusion has been extensively reviewed. These studies showed a direct relationship between decreasing Hb and mortality.1,2,4 An acute reduction in Hb to 30 g·L−1 leads to about a 50% mortality rate with an increase towards 100% mortality as Hb decreases further (Fig. 1).1,2,4,10 The mechanisms of death likely include the loss of blood oxygen-carrying capacity to a level that cannot support sufficient tissue oxygen delivery to maintain cellular energetics and biological function.
In addition, acute hemodilution during cardiac surgery involving CPB, as well as lowest hematocrit (Hct) on CPB, have been associated with worsened perioperative morbidity, including stroke,36,42 AKI,36,43,44 and MI,36 and to increased mortality.3,5,6,36 The relationship between nadir Hct and perioperative stroke was clearly shown by Karkouti et al. who found an increased incidence of stroke with a declining nadir Hct on CPB.42 This correlation was possibly related to the increase in cerebral blood flow associated with acute anemia on CPB,45 which may have increased the number of emboli directed to the brain, and/or anemia-induced brain tissue hypoxia32 may have accentuated the negative impact of any single embolic event.46 With respect to AKI associated with CPB, retrospective studies have shown a relationship between intraoperative hemodilutional anemia while on CPB and postoperative renal dysfunction (Fig. 3).36,37,43,44 Karkouti et al. also showed that AKI is associated with an increase in mortality in patients who experience a significant reduction in estimated glomerular filtration rate or a need for dialysis within one week of cardiac surgery.44 Modifiable risk factors for AKI include both preoperative anemia and perioperative transfusion. The importance of the impact of AKI on patients undergoing CPB was emphasized by a recent meta-analysis that showed a correlation between AKI, duration of CPB, and increased mortality.47

Anemia-induced renal hypoxia as a potential mechanism for acute kidney injury (AKI). A) Experimental models of moderate anemia have been associated with a high magnitude of renal hypoxia as evidenced by increased hypoxia-inducible factor luciferase radiance (a) and erythropoietin mRNA levels (b). B) Observational studies have associated acute early anemia on cardiopulmonary bypass with renal hypoxia as evidenced by delayed increase in erythropoietin expression upon intensive care unit admission (c) and (d). C) Prospective studies have shown a reduction in urinary oxygen tension with cardiopulmonary bypass (e). The duration and magnitude of urinary hypoxia has been associated with a greater risk of postoperative acute kidney injury (f).
A possible explanation for this relationship between anemia, CPB, and renal injury could relate to the kidney’s susceptibility to low tissue oxygen delivery, and the impact of acute hemodilution on reducing renal tissue partial pressure of oxygen (PO2) during conditions of non-physiologic perfusion on CPB.48,49,50,51 Tissues in the region of the medulla of the kidney have lower partial pressures of oxygen relative to the renal cortex, both at baseline and following acute anemia,49 likely because of a lower oxygen supply relative to the higher metabolic demand in the medulla. The impact of anemia on renal medullary hypoxia is accentuated in rats undergoing CPB50 and has been associated with an increase in endothelial nitric oxide synthase expression within the renal medulla (not renal cortex) of anemic rats following CPB.51 A more pronounced decrease in oxygen delivery associated with hemodilution, and non-physiologic perfusion on CPB could further disrupt the oxygen delivery-consumption balance, resulting in renal hypoxia and tissue injury.52,53 A recent clinical trial showed an association between acute anemia, metabolic acidosis, and increased systemic erythropoietin (EPO) levels (response to renal hypoxia),54 further supporting a potential causal link between anemia-induced tissue hypoxia and organ injury.
The previous relationships between acute anemia and adverse outcomes including AKI do not provide evidence of causality. It is reasonable to believe that multiple factors associated with hemodilution in both the above-mentioned populations could be involved in increased perioperative morbidity and mortality, such as hypotension, hypoperfusion, effect of anesthesia,55 and the artificial circulation associated with CPB.56 In the case of CPB,37 circulatory dynamics directly related to the CPB apparatus, and changes in rheology during acute hemodilution may negatively affect renal tissue PO2.50 In addition, translational studies that have assessed hypoxia signalling mechanisms in the kidney during acute anemia support the hypothesis that inadequate oxygen delivery to tissues could contribute to organ failure and mortality during acute anemia.31,35,38,53,57
As seen in murine models, moderate anemia is associated with renal hypoxia as shown by an increase in HIF in the kidney.31,34,35,38 Such molecular hypoxia signalling is a primary function of the kidney under physiologic conditions. Increased production of the HIF-dependent molecule EPO in the kidney as well other organs is a physiologic responses to correct anemia.58,59 The physiologic EPO response to anemia-induced tissue hypoxia occurs in greatest magnitude in the kidney (approximate 20-fold increase in RNA level) relative to other tissues such as the brain (approximate two-fold increase in RNA level).38 In addition, EPO is more sensitive in terms of magnitude of response to tissue hypoxia relative to other HIF-dependent molecules.38,48 Nevertheless, if the anemia-induced renal hypoxia is severe and prolonged, this exposure may lead to much higher expression and release of renal EPO and eventually lead to renal tissue injury.53 A recent study in humans undergoing CPB supports this hypothesis by showing that low Hb was associated with increased lactic acid and a subsequent increase in EPO levels in the ICU. Patients who developed AKI (KDIGO criteria; increase in serum creatinine > 26.5 umol·L−1 within 48 hr of surgery or > 1.5 times the baseline value within seven days of surgery) showed a numerical trend towards higher EPO levels in the ICU (P = 0.08) compared with non-AKI counterparts, indicating possible worse renal hypoxia.54 Additional evidence that renal hypoxia is associated with kidney injury is provided by a human study showing that prolonged reductions in renal/urinary PO2 is associated with kidney injury53 (Fig. 3). Nonetheless, further study will be required to prove causality and to determine if treatment of anemia can avert this outcome.
What is the risk associated with RBC transfusion?
While the actuarial risk of immediate mortality associated with RBC transfusion is of the same order of magnitude as being struck by lightning,60,61,62 real concerns about morbidity and mortality exist. Transfusion risks are routinely reported by established reporting agencies including the US Food and Drug Association (FDA),63 the National Healthcare Safety Network Hemovigilance Module in the US,64 the UK’s Serious Hazards of Transfusion (SHOT) program,62 and the Canadian Transfusion Transmitted Injuries Surveillance System (TTISS).65
According to the UK National Health Service SHOT annual report on transfusion-related adverse events,62 human error is an important factor for a high proportion (87.3%) of transfusion-related adverse outcomes. These include ABO incompatibility events, incorrect blood component transfusions, handling and storage errors, delayed transfusion, avoidable transfusion, over- and under-transfusion, “right blood type (wrong blood) to right patient-type” errors (a circumstance when the patient was transfused with the right blood type despite errors in identifying the correct patient or blood unit), and near misses. The near-misses category accounted for 43.6% of reported adverse events.62 A large proportion of major adverse reactions include transfusion-associated circulatory overload (TACO), febrile responses, and allergic and hypotensive reactions. With regard to transfusion-related deaths, over the past nine years, the leading causes of death were pulmonary complications including transfusion-related lung injury (TRALI) and respiratory complications secondary to TACO. Transfusion-associated circulatory overload is reported as one of the leading cause of transfusion-related mortality and major morbidity in the UK.62
According to FDA reports in 2017 and 2018, TACO remains one of the most common causes for transfusion-related mortality in the United States. Consistent with this, in Canada’s TTISS 2006–2012 report, up to 42% of adverse reactions related to blood component transfusion were classified as TACO. While severe allergic anaphylactic/anaphylactoid reactions accounted for 14% of transfusion-related reactions. During this same period, TACO was also associated with 32% of deaths related to transfusion. Interestingly, the incidence/risk of TACO and TRALI are often not specifically reported in RCTs assessing the impact of liberal vs restrictive transfusion thresholds.66,67,68
Finally, ongoing data published by the ONTraC network in Ontario have shown that a reduction of RBC transfusion through patient blood management programs has significantly reduced transfusion-related adverse events.11,13,69 As shown by Yanagawa et al. in patients presenting for cardiac surgery,13 increasing severity of anemia is associated with an increase in the number of RBC transfusions. This increase in RBC transfusion in more anemic patients shows a possible confounding—i.e., “sicker” and more anemic patients receive more transfusions and therefore are exposed to the increased risks of transfusion. Thus, adverse outcomes associated with anemia and RBC transfusion are linked.10 Retrospective data have shown that the risk of adverse outcomes, including death, increases as a function of the number of units transfused.8,9,70 If the risks associated with transfusion make clinicians reticent to transfuse RBCs in acute clinical situations, then the risks associated with untreated acute blood loss and anemia must be considered. For example, the 2018 SHOT report states 112 reports of delayed transfusion (3.3% of total reports) were associated with adverse outcomes including death, marking the importance of the timely and effective treatment of acute anemia.62 Thus, hesitancy to transfuse based on the belief that all patients should have a restrictive transfusion threshold may cause harm in conditions associated with acute or active blood loss.
What is the risk of transfusion specifically in critically ill and surgical patients?
Much of the concern about adverse outcomes associated with RBC transfusion is informed from observational (retrospective) data8,9 as opposed to prospective RCTs.70 Observational data often report a high odds ratio (OR) for adverse clinical outcomes associated with transfusion including mortality, MI, stroke, AKI, pulmonary morbidity, and infection (Fig. 4).8,9,70 For example, in a retrospective study, Koch et al. found that, in patients undergoing coronary artery bypass grafting, each unit of RBC transfused was associated with incremental risks of postoperative morbidity and mortality. These risks had notably high ORs for mortality, renal failure, prolonged ventilatory support, serious infection, cardiac complications, and neurologic events.9 Also favouring transfusion avoidance are two large multicentre observational studies in critical care—the anemia and blood transfusion in the critically ill-current clinical practice in the United States (CRIT) study in North America,71 and the Anemia and Blood transfusion in the Critically ill (ABC) study in Europe72—which both suggested that RBC transfusion was independently associated with mortality after adjusting for confounders. It is unclear, though, whether the increased mortality can be explained by residual (i.e., unaccounted for) confounding. Again, there is discrepancy between the high ORs for risk of transfusion in observational studies, which are associated with possible confounding factors, vs prospective RCTs, where such confounding can be minimized. In one analysis, the risk of transfusion in liberal vs restrictive transfusion strategies are much closer to unity, emphasizing the importance of assessing the outcomes of prospective RCTs (Fig. 4).

Adapted with permission from Patel et al.70
Discrepancy between evidence from randomized-controlled trials vs observational trials assessing adverse outcomes in transfusion threshold trials. Odds ratios compare the liberal strategy with the restrictive strategy.
The reason for the discrepancy in risk of transfusion reported by retrospective vs prospective studies may derive from confounding associated with clinical practice for acutely ill patients. In this setting, patients who are assessed as doing poorly clinically may receive a blood transfusion as part of their care plan. Nevertheless, the blood transfusion may be unrelated to the disease pathophysiology responsible for adverse outcomes. In this setting, adverse outcomes may occur because of the disease, and be independent to RBC transfusion. Nevertheless, the outcomes become statistically linked to the RBC transfusion even though the transfusion may not have impacted outcome, thus inappropriately attributing risk to the transfusion.
What do the current RCTs tell us?
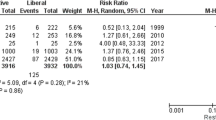
With an expanding number of large well-conducted transfusion RCTs, systematic reviews and clinical guidelines that confirm the relative benefits of restrictive and liberal transfusion strategies seem to be highly dependent on the patient population, study design, and surgical risk.23,73,74 The synthesis of these trial results suggest that all critically ill patients should be transfused using a restrictive transfusion threshold of 70 g·L−1.75 The original findings of the Transfusion Requirements in Critical Care (TRICC) trial did not show a significant difference between liberal and restrictive transfusion in terms of 30-day mortality (the primary outcome) (P = 0.11). Interestingly, the secondary outcomes supported the hypothesis that restrictive transfusion may be superior in specific subpopulations, such as younger, less ill patients, as mortality was lower in the restrictive transfusion group in patients < 55 years old (P = 0.02) and with an Acute Physiology And Chronic Health Evaluation II score ≤ 20 (P = 0.02).76 Furthermore, additional sub-analyses of this trial revealed that patients with cardiovascular disease or traumatic brain injury tended to have better outcomes with a more liberal transfusion threshold.77,78 Thus, this landmark study suggests that different patient subpopulations may benefit from a more liberal or a more restrictive transfusion strategy, depending on patient comorbidities and clinical conditions. Additionally, data sets from the Transfusion Requirements in Cardiac Surgery III (TRICS III) study support an interesting hypothesis regarding liberal vs restrictive transfusion.66,73 In this study assessing restrictive vs liberal transfusion strategies in cardiac surgical patients, most subgroup analyses showed no interaction of demographic factors with the primary outcome. Nevertheless, stratification of subjects by age suggested that older patients may benefit from a restrictive transfusion strategy, while younger patients may benefit from a more liberal transfusion strategy66,73 (Fig. 5). This has led to the proposed TRICS IV study (ClinicalTrials.gov; NCT02042898), which will test the hypothesis that a liberal transfusion strategy is superior to a restrictive strategy in younger patients undergoing cardiac surgery.

Adapted with permission from Mazer et al.73
Unadjusted subgroup analyses of primary outcome. Odds ratios compare the restrictive strategy with the liberal strategy. The solid and dashed grey lines represent the odds ratio and 95% confidence interval for the primary composite outcome of death, stroke, myocardial infarction, and renal failure requiring dialysis at six months from index surgery.
Should we consider a universal transfusion threshold or a spectrum of transfusion thresholds for different patient populations and clinical conditions?
In considering the statement: “A transfusion threshold of 70 g·L−1 should be the new norm […] for all critically ill patients. […] We recommend upgrading the evidence base […] to class 1A (strong recommendation and evidence)75”, written by Drs Hébert and Carson in a 2014 editorial in the New England Journal of Medicine, we need to explore the relative importance of the stated protocol transfusion threshold vs the Hb range to which the randomized patients are actually exposed to during the study (the average/or lowest daily Hb). Many physicians withhold transfusion until a threshold of 70 g·L−1 is “triggered”, leaving patients at a Hb value near 70 g·L−1 without transfusion. As shown in the summary Figs 6–8, on average, patients in the restrictive arms have Hb levels that are often well above the stated trigger per se. In these Figures, trials have been selected based on their sample size and prospective randomized design and grouped based on similar procedures and patient populations.74 Exclusion criteria for these include small sample size (n ≤ 100), lack of Hb results, or stratification of transfusion triggers. The most recent transfusion guidelines for the recommended thresholds have been based on the largest current trials as they carry the most weight in current scientific knowledge.23 While the trial design does not differentiate between transfusion and no transfusion, the paradigm set forth since the original TRICC trial involves comparing a restrictive transfusion strategy to a more liberal strategy in an attempt to define best practice in transfusion. To assess the impact of restrictive vs liberal transfusion strategies on clinical outcomes, data were extracted from well-conducted large RCTs in three patient populations including: 1) medical patients with critical illness,76,79,80,81,82,83 2) patients with cardiovascular risk undergoing orthopedic surgical procedures,67,84,85 and 3) patients undergoing cardiac surgery.66,68,86,87,88 Data for Hb concentration, at or near discharge (representing the clinical exposure), were extracted and compared with the listed primary outcomes reported most frequently at 28–90 days postoperatively (Table 1).

Restrictive transfusion thresholds and restrictive hemoglobin range (range of last measured hemoglobin before discharge in the restrictive arm) for trials assessing critically ill patients. Black bars indicate the protocol specific restrictive transfusion trigger for each representative trial. The mean and standard deviation (SD) represents the last or pre-discharge hemoglobin level for each representative trial. Red indicates liberal treatment group, and blue indicates restrictive treatment group. The restrictive hemoglobin range (in grey) is represented by the lowest bound of the SD of the lowest restrictive treatment group, and the highest bound of the SD of the highest restrictive treatment group. The guideline recommended restrictive red blood cell transfusion threshold suggests transfusion at a threshold in the critically ill is of 70 g·L−1 (red line).23 Data extracted from published trials.76,79,80,81,82,83
Transfusion threshold in the critically ill patient
The concept of comparing restrictive and liberal transfusion strategies originated with the critical care trial led by Hébert et al. assessing whether it was safe to restrict transfusion in critically ill patients to 70 g·L−1. The trial results showed no difference in the primary outcome of mortality between the two groups, suggesting that restrictive transfusion can be safely applied to the sickest patients.76 The Transfusion Requirements in Septic Shock (TRISS) trial in 2014 supported this finding and led to a fundamental paradigm shift in clinical care—i.e., that a restrictive transfusion threshold is the new norm.81 Nevertheless, apart from the original TRISS trials in which the average Hb level in the restrictive arm actually approaches the administrative trial threshold of 70 g·L−1, in all other medical trials, randomization to the restrictive arm resulted in an average Hb concentration above 80 g·L−1 (Fig. 6). In addition, a growing number of well-conducted trials in diverse surgical patient populations suggest that a one threshold fits all approach may not be optimal.
Transfusion threshold in the orthopedic surgical patient with cardiovascular risk
Review of three large trials showed that the mean daily Hb in the restrictive arms in patients undergoing orthopedic procedures were all above 90 g·L−1 (Fig. 7). In the 2011 Transfusion Trigger Trial for Functional Outcomes in Cardiovascular Patients Undergoing Surgical Hip Fracture Repair (FOCUS) trial, liberal vs restrictive transfusion practices were assessed in high risk patients (i.e., patients with cardiovascular disease or cardiovascular risk factors) after hip surgery, where the primary outcome was death or the ability to walk across a room without assistance after 60 days. The conclusion of this trial was that the restrictive threshold of 80 g·L−1, (not 70 g·L−1) was non-inferior to 100 g·L−1. Nevertheless, when reviewing outcome data, 156 vs 53 patients (P < 0.001) in the restrictive vs liberal group respectively received blood transfusion for clinical indications such as for treatment of hypotension, tachycardia, congestive heart failure, chest pain, or rapid bleeding. Thus, a difference of 103 patients in the restrictive arm vs liberal arm (approximately 10% of the group sample size) received more liberal transfusions than they would have based solely on the Hb threshold. Had these patients not received these transfusions, the outcome data analysis may have been different.67 This trial supports the addition of physiologic or functional variables as a component of the outcome analysis.

Restrictive transfusion threshold and restrictive hemoglobin range (range of last measured hemoglobin before discharge in the restrictive arm) for trials assessing orthopedic surgical patients with cardiovascular risk. Black bars indicate the protocol specific restrictive transfusion trigger for each representative trial. The mean and standard deviation (SD) represents the last or pre-discharge hemoglobin level for each representative trial. Red indicates liberal treatment group, and blue indicates restrictive treatment group. The restrictive hemoglobin range (in grey) is represented by the lowest bound of the SD of the lowest restrictive treatment group, and the highest bound of the SD of the highest restrictive treatment group. The guideline recommended restrictive red blood cell transfusion threshold in orthopedic surgery patients suggests transfusion at a threshold of 80 g·L−1 (red line).23 Data extracted from published trials.67,84,85
Transfusion threshold in the cardiac surgical patient
For patients undergoing cardiac surgery, clinicians have long held strong opinions about the Hb threshold or trigger used to optimally manage their patients. Murphy et al. provided data that maintained equipoise between restrictive and liberal transfusion strategies following publication of the Transfusion Indication Threshold Reduction (TITRe2) trial (Fig. 8). In that study, patients undergoing cardiac surgery were randomized to restrictive or liberal protocols after cardiac surgery. While there was no difference in the primary outcome (a composite of mortality, ischemic event, and serious infection or ischemic event within three months after surgery), an important secondary outcome was observed—i.e., a significant difference in 90-day mortality that favoured liberal transfusion.68 The TRICS III trial again showed non-inferiority of restrictive vs liberal strategy at 90 days and six months.66,73 While the primary outcome data and subsequent six-month outcome data showed non-inferiority of a restrictive transfusion strategy in all patients, some interesting observations were made. A sub-analysis did not show any interaction of transfusion strategy with important comorbidities, including preoperative Hb, left ventricular function, type of surgery, pulmonary disease, diabetes, or sex. Nevertheless, the analyses did show a significant age interaction (Fig. 5). The primary outcome, when stratified by age, showed an interaction where a restrictive transfusion strategy was favoured in patients ≥ 75 yr (OR, 0.77; 95% confidence interval [CI], 0.62 to 0.96) and a liberal transfusion strategy was favoured in younger patients (< 75 yr) (OR, 1.32; 95% CI, 1.07 to 1.64) with respect to the primary composite outcome. This interaction was consistent with deciles of age. This hypothesis-generating data suggested a possible effect by age grouping and has led to a successful Canadian Institutes of Health Research application for the TRICS IV study, which will assess the potential superiority of a liberal transfusion strategy in younger patients undergoing cardiac surgery. Thus, within the data set of the largest transfusion trial completed to date, patient variability may determine whether restrictive or liberal transfusion is optimal and in which patient population.

Restrictive transfusion threshold and restrictive hemoglobin range (range of last measured hemoglobin before discharge in the restrictive arm) for trials assessing cardiac surgical patients. Black bars indicate the restrictive transfusion threshold for each representative trial. The mean and standard deviation (SD) represents the last or pre-discharge hemoglobin level for each representative trial. Red indicates liberal treatment group, and blue indicates restrictive treatment group. The restrictive hemoglobin range (in grey) is represented by the lowest bound of the SD of the lowest restrictive treatment group, and the highest bound of the SD of the highest restrictive treatment group. The guideline recommended restrictive red blood cell transfusion threshold in cardiac surgery patients suggests transfusion at a threshold of 75 g·L−1 (red line).23 Data extracted from published trials.66,68,86,87,88
Transfusion threshold consensus statement
Based on the collective data from many completed transfusion trials, a 2018 Patient Blood Management Consensus Conference has recommended different transfusion thresholds for a variety of medical and surgical patient populations, with recommendation for thresholds of 70, 75, and 80 g·L−1, depending on the patient population.23 A meta-analysis by Hovaguimian et al. in which they compared restrictive and liberal strategies in patients undergoing cardiac and non-cardiac surgery, suggested that restrictive strategies increased the risk of adverse events related to hypoxia in some patient populations.74 In contrast to the results from the TRICS III trial, the meta-analysis by Simon et al.89 suggested that liberal transfusion may be favourable in geriatric patients, implying that the impact of differing patient comorbidities and patient circumstances may impact outcomes associated with different treatment strategies. This data further supports individualization of transfusion strategies and, again that the transfusion thresholds may vary with clinical context.89 Simon et al. further explain that older adults have a lower tolerance for anemia due to age-related pathophysiology, indicating that optimal patient blood management may require adaptation to individual patient settings.90 Thus, as in other aspects of medical therapy, a one size fits all approach may not lead to the best clinical outcome; instead, a personalized approach may lead to an optimal clinical outcome.91
Management of anemia vs RBC transfusion
As preoperative anemia is one of the most consistently published risk factors for perioperative transfusion,10,11,13 a focus on optimal treatment management of preoperative anemia to minimize the potential risk of both anemia and RBC transfusion requires ongoing attention. Ongoing clinical trials are addressing the importance of treating anemia to improve outcome in perioperative patients. These trials include the Hemoglobin Optimization to Prevent Transfusion and Adverse Events in Perioperative Patients with Iron Restricted Anemia (HOPE-Hb; ClinicalTrials.gov; NCT03528564), Preoperative Intravenous Iron to Treat Anemia in Major Surgery (PREVENTT; ClinicalTrials.gov; NCT01692418), and Intravenous Iron for Treatment of Anemia Before Cardiac Surgery (ITACS; ClinicalTrials.gov; NCT02632760), and have focused on optimal intravenous iron therapy to effectively treat anemia. In addition, two recent meta-analyses suggest that, combined treatment with iron plus erythropoiesis-stimulating agent (ESA) is safe and more effective at reducing RBC transfusion.92,93 Lastly, novel oral medications that prevent HIF breakdown by inhibiting prolyl hydroxylase activity should be studied in the management of perioperative anemia.94
Patient blood management (PBM) programs, such as those in the United States,95,96 Europe,97 and Canada, including the Ontario Nurse Transfusion Coordinators (ONTraC) Program11,13 have led to optimal management of patients while reducing adverse events associated with anemia and transfusions. These approaches have reduced unnecessary transfusion and potentially reduced the incidence of transfusion-related adverse outcomes.96 Based on the results of these PBM programs and clinical and research recommendations presented at the 2018 Frankfurt Consensus Conference,23 it is clear that detecting and treating preoperative anemia early before any major surgery may avoid the risks of anemia and transfusion. The causality of anemia-induced tissue hypoxia, organ injury, and subsequent mortality has not yet been established (Fig. 2). Nevertheless, management of anemia has been continually emphasized as an important and often unmet goal in medical and surgical patients.98 Treatment algorithms have been suggested for preoperative anemia,99 with the use of iron therapy or ESAs based on iron status. Treatment with preoperative EPO is associated with reduced perioperative blood transfusions92,93,100 and theoretically should improve patient outcomes. Nevertheless, further research is needed to confirm optimal administration of these therapies to improve outcomes without an increase in associated adverse events (such as hypersensitivity reactions and thromboembolic events).92
Ongoing trials of liberal vs restrictive transfusion in patients with specific patient populations: traumatic brain injury and acute coronary syndromes
A number of clinical trials continue to assess the impact of liberal vs restrictive transfusion in different patient populations including patients with traumatic brain injury and acute coronary syndromes.
Assessing the impact of acute anemia and cerebral hypoxia on clinical outcomes following traumatic brain injury
Two clinical trials are currently assessing the importance of the interaction between anemia, transfusions and cerebral hypoxia and other clinical outcomes following traumatic brain injury (TBI)— the HEMOglobin Transfusion Threshold in Traumatic Brain Injury OptimizatioN (HEMOTION; ClinicalTrials.gov;NCT03260478) and the Brain Oxygen Optimization in Severe TBI Phase 3 study (BOOST III; ClinicalTrials.gov; NCT03754114). From published studies, we know that systemic hypoxia/hypoxemia is a significant risk factor for secondary brain injury following TBI.101 With the introduction of direct brain tissue PO2 measurements using implanted Clark-type electrodes, low brain PO2 has been identified to be a prognostic indicator of poor outcomes including worsened brain injury and mortality.102,103 Furthermore, an interaction was observed between low Hb and low brain PO2 (< 20 mmHg) such that the combination of these two clinical indicators was associated with an unfavourable outcome (defined as a Glasgow Comma Scale 1–3 at 30 days; OR, 6.24; 95% CI, 1.61 to 24.22; P = 0.008).104 An experimental study has supported a causal role for anemia-induced brain tissue hypoxia as a mediator of increased brain injury by showing that acute anemia reduces brain PO2, and that very small decreases in brain PO2 are associated with up to three-fold increases in cerebral infarction volume.105 Additionally, the type of resuscitation fluid (including blood) has a significant impact on the recovery of brain PO2 and on brain electrical activity in another experimental study.106 Nevertheless, whether active treatments to increase brain tissue PO2, including correction of anemia, can significantly improve outcomes in patients with TBI remains to be determined. A treatment protocol for TBI based on monitoring and maintaining adequate brain PO2 has been suggested.107 Okonkwo et al. have provided data in support of the hypothesis that this treatment protocol, designed to improve brain perfusion and real-time brain tissue PO2, may increase functional outcomes after TBI (BOOST II).108 This hypothesis is being more completely assessed in a multi-national phase III clinical trial (BOOST III).
Retrospective and early randomized prospective studies have assessed the risk-benefit of liberal transfusion strategies in patients who have suffered a TBI.109,110 Despite the evidence suggesting the harmful effects of anemia and low brain PO2 following TBI, a clear benefit from liberal transfusion is not supported by all studies.109,110 As a consequence, some authors are calling for more rigorous non-inferiority RCTs to evaluate liberal vs restrictive transfusion practices following TBI.111 Ongoing trials, such as HEMOTION, have sought to fill a similar knowledge gap by examining the superiority of liberal transfusion strategies (trigger ≤ 100 g·L−1) vs restrictive strategies (trigger ≤ 70 g·L−1) with respect to neurologic functional outcomes. Unfortunately, this study will also simply assess the superiority of one arbitrary transfusion trigger vs another arbitrary trigger. There is also a need for studies which address individualizing transfusion based on clinical and/or physiologic parameters. As an alternative to transfusion, some groups have evaluated administering ESAs to improve outcomes in TBI.109 Therefore, although the decrease in brain PO2 due to anemia has a negative impact on outcomes in TBI patients, the advantage of treating this low PO2 value, through a number of treatments including RBC transfusion, remains to be shown.
Assessing the impact of anemia on acute coronary syndrome
One of the ongoing large RCTs evaluating the effect of anemia and transfusion on outcomes in acute coronary syndrome is the Myocardial Ischemia and Transfusion (MINT) trial (NCT02981407). Hébert et al. suggested that restrictive transfusion strategies might not be safe in patients with acute MIs or unstable angina.78 Carson et al. identified a lack of high quality RCTs to guide transfusion practices in patients with ACS. In a pilot trial, Carson et al. found that liberal transfusion strategies showed a trend of superiority compared with restrictive strategies, with regards to major cardiac events and deaths.80 As a result, they are currently conducting the Phase III MINT trial (NCT02981407), with the purpose of filling this knowledge gap.
Conclusions
In summary, based on the evidence provided by high-quality RCTs, associated meta-analyses, and derived guidelines, the determination of an appropriate Hb threshold for RBC transfusion may vary depending on important patient factors and clinical circumstances. The concept of a one size fits all approach to anemia and transfusion based purely on Hb levels should be rigorously re-evaluated.
References
Carson J, Poses RM, Spence RK, Bonavita G. Severity of anaemia and operative mortality and morbidity. Lancet 1988; 1: 727-9.
Carson JL, Duff A, Poses RM, et al. Effect of anaemia and cardiovascular disease on surgical mortality and morbidity. Lancet 1996; 348: 1055-60.
Fang WC, Helm RE, Krieger KH, et al. Impact of minimum hematocrit during cardiopulmonary bypass on mortality in patients undergoing coronary artery surgery. Circulation 1997; 96(9 Suppl): II-194-9.
Guinn NR, Cooter ML, Villalpando C, Weiskopf RB. Severe anemia associated with increased risk of death and myocardial ischemia in patients declining blood transfusion. Transfusion 2018; 58: 2290-6.
Karkouti K, Wijeysundera DN, Beattie WS; Reducing Bleeding in Cardiac Surgery (RBC) Investigators. Risk associated with preoperative anemia in cardiac surgery: a multicenter cohort study. Circulation 2008; 117: 478-84.
Kulier A, Levin J, Moser R, et al. Impact of preoperative anemia on outcome in patients undergoing coronary artery bypass graft surgery. Circulation 2007; 116: 471-9.
Government of Canada, Public Health Agency of Canada. Transfusion Transmitted Injuries Surveillance System, 2006-2012 Summary Results; 2014. Available from URL: www.canada.ca (accessed May 2020).
Karkouti K, Wijeysundera DN, Yau TM, et al. The independent association of massive blood loss with mortality in cardiac surgery. Transfusion 2004; 44: 1453-62.
Koch CG, Li L, Duncan AI, et al. Morbidity and mortality risk associated with red blood cell and blood-component transfusion in isolated coronary artery bypass grafting. Crit Care Med 2006; 34: 1608-16.
Shander A, Javidroozi M, Ozawa S, Hare GM. What is really dangerous: anaemia or transfusion? Br J Anaesth 2011; 107: i41-59.
Hare GM, Freedman J, Mazer CD. Risks of anemia and related management strategies: can perioperative blood management improve patient safety? Can J Anesth 2013; 60: 168-75.
Nalla BP, Freedman J, Hare GM, Mazer CD. Update on blood conservation for cardiac surgery. J Cardiovasc Thorac Anesth 2012; 26: 117-33.
Yanagawa B, Rocha RV, Mazine A, et al. hemoglobin optimization for coronary bypass: a 10-year Canadian multicenter experience. Ann Thorac Surg 2019; 107: 711-7.
Sender R, Fuchs S, Milo R. Revised estimates for the number of human and bacteria cells in the body. PLoS Biol 2016; DOI: https://doi.org/10.1371/journal.pbio.1002533.
Poskitt EM. Early history of iron deficiency. Br J Haematol 2003; 122: 554-62.
World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity 2011. Available from URL: https://www.who.int/vmnis/indicators/haemoglobin/en/ (accessed May 2020).
Fowler AJ, Ahmad T, Abbott TE, et al. Association of preoperative anaemia with postoperative morbidity and mortality: an observational cohort study in low-, middle-, and high-income countries. Br J Anaesth 2018; 121: 1227-35.
Kassebaum NJ, Jasrasaria R, Naghavi M, et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood 2014; 123: 615-24.
Global Burden of Disease Pediatrics Collaboration; Kyu H, Pinho C, Wagner JA, et al. Global and National Burden of Diseases and injuries among children and adolescents between 1990 and 2013: findings from the Global Burden of Disease 2013 study. JAMA Pediatr 2016; 170: 267-87.
Scott SP, Chen-Edinboro LP, Caulfield LE, Murray-Kolb LE. The impact of anemia on child mortality: an updated review. Nutrients 2014; 6: 5915-32.
Daru J, Zamora J, Fernandez-Felix BM, et al. Risk of maternal mortality in women with severe anaemia during pregnancy and post partum: a multilevel analysis. Lancet Glob Health 2018; 6: e548-54.
Penninx BW, Pahor M, Woodman RC, Guralnik JM. Anemia in Old Age Is Associated With Increased Mortality and Hospitalization. J Gerentol A Biol Sci Med Sci 2006; 61: 474-9.
Mueller MM, Van Remoortel H, Meybohm P, et al. Patient blood management: recommendations from the 2018 Frankfurt Consensus Conference. JAMA 2019; 321: 983-97.
Fowler AJ, Ahmad T, Phull MK, Allard S, Gillies MA, Pearse RM. Meta-analysis of the association between preoperative anaemia and mortality after surgery. Br J Surg 2015; 102: 1314-24.
Musallam KM, Tamim HM, Richards T, et al. Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study. Lancet 2011; 378: 1396-407.
Klein AA, Collier TJ, Brar MS, et al. The incidence and importance of anaemia in patients undergoing cardiac surgery in the UK - the first Association of Cardiothoracic Anaesthetists national audit. Anaesthesia 2016; 71: 627-35.
Padmanabhan H, Brookes MJ, Nevill AM, Luckraz H. Association between anemia and blood transfusion with long-term mortality after cardiac surgery. Ann Thorac Surg 2019; 108: 687-92.
Padmanabhan H, Siau K, Curtis J, et al. Preoperative anemia and outcomes in cardiovascular surgery: systematic review and meta-analysis. Ann Thorac Surg 2019; 108: 1840-8.
Beattie WS, Wijeysundera DN, Karkouti K, et al. Acute surgical anemia influences the cardioprotective effects of β-blockade: a single-center, propensity-matched cohort study. Anesthesiology 2010; 112: 25-33.
Beattie WS, Karkouti K, Wijeysundera DN, Tait G. Risk associated with preoperative anemia in noncardiac surgery: a single-center cohort study. Anesthesiology 2009; 110: 574-81.
Ragoonanan TE, Beattie WS, Mazer CD, et al. Metoprolol reduces cerebral tissue oxygen tension after acute hemodilution in rats. Anesthesiology 2009; 111: 988-1000.
McLaren AT, Marsden PA, Mazer CD, et al. Increased expression of HIF-1α, nNOS, and VEGF in the cerebral cortex of anemic rats. Am J Physiol Regul Integr Comp Physiol 2007; 292: R403-14.
Hare GM, Mazer CD, Mak W, et al. Hemodilutional anemia is associated with increased cerebral neuronal nitric oxide synthase gene expression. J Appl Physiol 1985; 2003(94): 2058-67.
Tsui AK, Marsden PA, Mazer CD, et al. Priming of hypoxia-inducible factor by neuronal nitric oxide synthase is essential for adaptive responses to severe anemia. Proc Natl Acasd Sci USA 2011; 108: 17544-9.
Tsui AK, Marsden PA, Mazer CD, et al. Differential HIF and NOS responses to acute anemia: defining organ-specific hemoglobin thresholds for tissue hypoxia. Am J Physiol Regul Integr Comp Physiol. 2014; 307: R13-25.
Loor G, Li L, Sabik JF 3rd, Rajeswaran J, Blackstone EH, Koch CG. Nadir hematocrit during cardiopulmonary bypass: end-organ dysfunction and mortality. J Thorac Cardiovasc Surg 2012; 144(654–62): e4.
Karkouti K, Beattie WS, Wijeysundera DN, et al. Hemodilution during cardiopulmonary bypass is an independent risk factor for acute renal failure in adult cardiac surgery. J Thorac Cardiovasc Surg 2005; 129: 391-400.
Mistry N, Mazer CD, Sled JG, et al. Red blood cell antibody-induced anemia causes differential degrees of tissue hypoxia in kidney and brain. Am J Physiol Regul Integr Comp Physiol 2018; 314: R611-22.
El Beheiry MH, Heximer SP, Voigtlaender-Bolz J, et al. Metoprolol impairs resistance artery function in mice. J Appl Physiol 1985; 2011(111): 1125-33.
Hu T, Beattie WS, Mazer CD, et al. Treatment with a highly selective beta(1) antagonist causes dose-dependent impairment of cerebral perfusion after hemodilution in rats. Anesth Analg 2013; 116: 649-62.
Hare GM, Worrall JM, Baker AJ, Liu E, Sikich N, Mazer CD. Beta2 adrenergic antagonist inhibits cerebral cortical oxygen delivery after severe haemodilution in rats. Br J Anaesth 2006; 97: 617-23.
Karkouti K, Djaiani G, Borger MA, et al. Low hematocrit during cardiopulmonary bypass is associated with increased risk of perioperative stroke in cardiac surgery. Annal Thorac Surg 2005; 80: 1381-7.
Swaminathan M, Phillips-Bute BG, Conlon PJ, Smith PK, Newman MF, Stafford-Smith M. The association of lowest hematocrit during cardiopulmonary bypass with acute renal injury after coronary artery bypass surgery. Annal Thorac Surg 2003; 76: 784-91.
Karkouti K, Wijeysundera DN, Yau TM, et al. Acute kidney injury after cardiac surgery: focus on modifiable risk factors. Circulation 2009; 119: 495-502.
Cook DJ, Orszulak TA, Daly RC, MacVeigh I. Minimum hematocrit for normothermic cardiopulmonary bypass in dogs. Circulation 1997; 96(Suppl 9): II-200-4.
Homi HM, Yang H, Pearlstein RD, Grocott HP. Hemodilution during cardiopulmonary bypass increases cerebral infarct volume after middle cerebral artery occlusion in rats. Anesth Analg 2004; 99: 974-81.
Kumar AB, Suneja M, Bayman EO, Weide GD, Tarasi M. Association between postoperative acute kidney injury and duration of cardiopulmonary bypass: a meta-analysis. J Cardiovasc Thorac Surg 2012; 26: 64-9.
Abrahamson JR, Read A, Chin K, et al. Renal tissue PO2 sensing during acute hemodilution is dependent on the diluent. Am J Physiol Regul Integr Comp Physiol 2020; DOI: https://doi.org/10.1152/ajpregu.00323.2019.
Johannes T, Mik EG, Nohe B, Unertl KE, Ince C. Acute decrease in renal microvascular PO2 during acute normovolemic hemodilution. Am J Physiol Renal Physiol 2007; 292: F796-803.
Darby PJ, Kim N, Hare GM, et al. Anemia increases the risk of renal cortical and medullary hypoxia during cardiopulmonary bypass. Perfusion 2013; 28: 504-11.
Mazer CD, Briet F, Blight KR, et al. Increased cerebral and renal endothelial nitric oxide synthase gene expression after cardiopulmonary bypass in the rat. J Thorac Cardiovasc Surg 2007; 133: 13-20.
Souma T, Suzuki N, Yamamoto M. Renal erythropoietin-producing cells in health and disease. Front Physiol 2015; DOI: https://doi.org/10.3389/fphys.2015.00167.
Zhu MZ, Martin A, Cochrane AD, et al. Urinary hypoxia: an intraoperative marker of risk of cardiac surgery-associated acute kidney injury. Nephrol Dial Transplant 2018; 33: 2191-201.
Hare GM, Han K, Leshchyshyn Y, et al. Potential biomarkers of tissue hypoxia during acute hemodilutional anemia in cardiac surgery: a prospective study to assess tissue hypoxia as a mechanism of organ injury. Can J Anesth 2018; 65: 901-13.
Iguchi N, Kosaka J, Booth LC, et al. Renal perfusion, oxygenation, and sympathetic nerve activity during volatile or intravenous general anaesthesia in sheep. Br J Anaesth 2019; 122: 342-9.
Lankadeva YR, Cochrane AD, Marino B, et al. Strategies that improve renal medullary oxygenation during experimental cardiopulmonary bypass may mitigate postoperative acute kidney injury. Kidney Int 2019; 95: 1338-46.
Lankadeva YR, Kosaka J, Evans RG, Bellomo R, May CN. Urinary oxygenation as a surrogate measure of medullary oxygenation during angiotensin II therapy in septic acute kidney injury. Crit Care Med 2018; 46: e41-8.
Tan CC, Eckardt KU, Firth JD, Ratcliffe PJ. Feedback modulation of renal and hepatic erythropoietin mRNA in response to graded anemia and hypoxia. Am J Physiol 1992; 263(3 Pt 2): F474-81.
Koury ST, Koury MJ, Bondurant MC, Caro J, Graber SE. Quantitation of erythropoietin-producing cells in kidneys of mice by in situ hybridization: correlation with hematocrit, renal erythropoietin mRNA, and serum erythropoietin concentration. Blood 1989; 74: 645-51.
Friedman MT, Avadhani V, Gilmore S, Madrigal E. Blood transfusion in the 21st century. Discoveries 2014; DOI: https://doi.org/10.15190/d.2014.3.
Elsom DM, Webb J. Deaths and injuries from lightning in the UK, 1988–2012. Weather 2014; DOI: https://doi.org/10.1002/wea.2254.
Working Expert Group (WEG) & Writing Group, on behalf of the SHOT Steering Group. Annual SHOT Report - 2018. Available from URL: https://www.shotuk.org/wp-content/uploads/myimages/SHOT-Report-2018_Web_Version-1.pdf (accessed May 2020).
Food and Drug Association. Transfusion/Donation Fatalities. Available from URL: https://www.fda.gov/vaccines-blood-biologics/report-problem-center-biologics-evaluation-research/transfusiondonation-fatalities (accessed May 2020).
Harvey AR, Basavaraju SV, Chung KW, Kuehnert MJ. Transfusion-related adverse reactions reported to the National Healthcare Safety Network Hemovigilance Module, United States, 2010 to 2012. Transfusion 2015; 55: 709-18.
Ditomasso J, Liu Y, Heddle NM. The Canadian Transfusion Surveillance System: what is it and how can the data be used? Transfus Apher Sci 2012; 46: 329-35.
Mazer CD, Whitlock RP, Fergusson DA, et al. Restrictive or liberal red-cell transfusion for cardiac surgery. N Engl J Med 2017; 377: 2133-44.
Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med 2011; 365: 2453-62.
Murphy GJ, Pike K, Rogers CA, et al. Liberal or restrictive transfusion after cardiac surgery. N Engl J Med 2015; 372: 997-1008.
Callum JL, Pinkerton PH, Lima A, et al. Bloody Easy 4. Blood Transfusions, Blood Alternatives and Transfusion Reactions. A Guide to Transfusion Medicine, Fourth Edition. Ontario Regional Blood Coordinating Network 2016.
Patel NN, Avlonitis VS, Jones HE, Reeves BC, Sterne JA, Murphy GJ. Indications for red blood cell transfusion in cardiac surgery: a systematic review and meta-analysis. Lancet Haematol 2015; 2: e543-53.
Corwin HL, Gettinger A, Pearl RG, et al. The CRIT study: anemia and blood transfusion in the critically ill–current clinical practice in the United States. Crit Care Med 2004; 32: 39-52.
Vincent JL, Baron JF, Reinhart K, et al. Anemia and blood transfusion in critically ill patients. JAMA 2002; 288: 1499-507.
Mazer CD, Whitlock RP, Fergusson DA, et al. Six-month outcomes after restrictive or liberal transfusion for cardiac surgery. N Engl J Med 2018; 379: 1224-33.
Hovaguimian F, Myles PS. Restrictive versus liberal transfusion strategy in the perioperative and acute care settings. A context-specific systematic review and meta-analysis of randomized controlled trials. Anesthesiology 2016; 125: 46-61.
Hébert PC, Carson JL. Transfusion threshold of 7 g per deciliter—the new normal. N Engl J Med 2014; 371: 1459-61.
Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999; 340: 409-17.
McIntyre LA, Fergusson DA, Hutchison JS, et al. Effect of a liberal versus restrictive transfusion strategy on mortality in patients with moderate to severe head injury. Neurocrit Care 2006; 5: 4-9.
Hébert PC, Yetisir E, Martin C, et al. Is a low transfusion threshold safe in critically ill patients with cardiovascular diseases? Crit Care Med 2001; 29: 227-34.
Bergamin FS, Almeida JP, Landoni G, et al. Liberal versus restrictive transfusion strategy in critically ill oncologic patients: the transfusion requirements in critically ill oncologic patients randomized controlled trial. Crit Care Med 2017; 45: 766-73.
Carson JL, Brooks MM, Abbott JD, et al. Liberal versus restrictive transfusion thresholds for patients with symptomatic coronary artery disease. Am Heart J 2013; 165(964–71): e1.
Holst LB, Haase N, Wetterslev J, et al. Lower versus higher hemoglobin threshold for transfusion in septic shock. N Engl J Med 2014; 371: 1381-91.
Jairath V, Kahan BC, Gray A, et al. Restrictive versus liberal blood transfusion for acute upper gastrointestinal bleeding (TRIGGER): a pragmatic, open-label, cluster randomised feasibility trial. Lancet 2015; 386: 137-44.
Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med 2013; 368: 11-21.
Gregersen M, Borris LC, Damsgaard EM. Postoperative blood transfusion strategy in frail, anemic elderly patients with hip fracture: the TRIFE randomized controlled trial. Acta Orthop 2015; 86: 363-72.
Grover M, Talwalkar S, Casbard A, et al. Silent myocardial ischaemia and haemoglobin concentration: a randomized controlled trial of transfusion strategy in lower limb arthroplasty. Vox Sang 2006; 90: 105-12.
Bracey AW, Radovancevic R, Riggs SA, et al. Lowering the hemoglobin threshold for transfusion in coronary artery bypass procedures: effect on patient outcome. Transfusion 1999; 39: 1070-7.
Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA 2010; 304: 1559-67.
Koch CG, Sessler DI, Mascha EJ, et al. A randomized clinical trial of red blood cell transfusion triggers in cardiac surgery. Ann Thorac Surg 2017; 104: 1243-50.
Simon GI, Craswell A, Thom O, Fung YL. Outcomes of restrictive versus liberal transfusion strategies in older adults from nine randomised controlled trials: a systematic review and meta-analysis. Lancet Haematol 2017; 4: e465-74.
Simon GI, Craswell A, Thom O, Chew MS, Anstey CM, Fung YL. Impacts of aging on anemia tolerance, transfusion thresholds, and patient blood management. Transfus Med Rev 2019; 33: 154-61.
Kashani HH, Lodewyks C, Kavosh MS, et al. The effect of restrictive versus liberal transfusion strategies on longer-term outcomes after cardiac surgery: a systematic review and meta-analysis with trial sequential analysis. Can J Anesth 2020; 67: 577-87.
Kei T, Mistry N, Curley G, et al. Efficacy and safety of erythropoietin and iron therapy to reduce red blood cell transfusion in surgical patients: a systematic review and meta-analysis. Can J Anesth 2019; 66: 716-31.
Cho BC, Serini J, Zorrilla-Vaca A, et al. Impact of preoperative erythropoietin on allogeneic blood transfusions in surgical patients: results from a systematic review and meta-analysis. Anesth Analg 2019; 128: 981-92.
Chen N, Hao C, Peng X, et al. Roxadustat for anemia in patients with kidney disease not receiving dialysis. N Engl J Med 2019; 381: 1001-10.
Shander A, Bracey AW Jr, Goodnough LT, et al. Patient blood management as standard of care. Anesth Analg 2016; 123: 1051-3.
Anthes E. Evidence-based medicine: save blood, save lives. Nature 2015; 520: 24-6.
Kaserer A, Rossler J, Braun J, et al. Impact of a patient blood management monitoring and feedback programme on allogeneic blood transfusions and related costs. Anaesthesia 2019; 74: 1534-41.
Shander A, Goodnough LT. From tolerating anemia to treating anemia. Ann Intern Med 2019; 170: 125-6.
Goodnough LT, Shander A. Patient blood management. Anesthesiology 2012; 116: 1367-76.
Spahn DR, Schoenrath F, Spahn GH, et al. Effect of ultra-short-term treatment of patients with iron deficiency or anaemia undergoing cardiac surgery: a prospective randomised trial. Lancet 2019; 393: 2201-12.
Chesnut RM, Marshall LF, Klauber MR, et al. The role of secondary brain injury in determining outcome from severe head injury. J Trauma 1993; 34: 216-22.
Van den Brink WA, van Santbrink H, Steyerberg EW, et al. Brain oxygen tension in severe head injury. Neurosurgery 2000; 46: 868-76; discussion 876-8.
Valadka AB, Gopinath SP, Contant CF, Uzura M, Robertson CS. Relationship of brain tissue PO2 to outcome after severe head injury. Crit Care Med 1998; 26: 1576-81.
Oddo M, Levine JM, Kumar M, et al. Anemia and brain oxygen after severe traumatic brain injury. Intensive Care Med 2012; 38: 1497-504.
Hare GM, Mazer CD, Hutchison JS, et al. Severe hemodilutional anemia increases cerebral tissue injury following acute neurotrauma. J Appl Physiol 1985; 2007(103): 1021-9.
Baker AJ, Park E, Hare GM, Liu E, Sikich N, Mazer DC. Effects of resuscitation fluid on neurologic physiology after cerebral trauma and hemorrhage. J Trauma 2008; 64: 348-57.
Chesnut R, Aguilera S, Buki A, et al. A management algorithm for adult patients with both brain oxygen and intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med 2020; DOI: https://doi.org/10.1007/s00134-019-05900-x.
Okonkwo DO, Shutter LA, Moore C, et al. Brain oxygen optimization in severe traumatic brain injury phase-II: a phase II randomized trial. Crit Care Med 2017; 45: 1907-14.
Robertson CS, Hannay HJ, Yamal JM, et al. Effect of erythropoietin and transfusion threshold on neurological recovery after traumatic brain injury: a randomized clinical trial. JAMA 2014; 312: 36-47.
Salim A, Hadjizacharia P, DuBose J, et al. Role of anemia in traumatic brain injury. J Am Coll Surg 2008; 207: 398-406.
Utter GH, Shahlaie K, Zwienenberg-Lee M, Muizelaar JP. Anemia in the setting of traumatic brain injury: the arguments for and against liberal transfusion. J Neurotrauma 2011; 28: 155-65.
Acknowledgements
Drs Baker, Hare and Mazer were supported by Merit Awards from the Department of Anesthesia at the University of Toronto. Supported in part by a grant from CIHR (165808).
Author information
Authors and Affiliations
Contributions
Gregory M.T. Hare, Melina P. Cazorla-Bak, S.F. Michelle Ku, Nikhil Mistry, Kyle Chin, Katerina Pavenski, Andrew J. Baker, and C. David Mazer contributed to all aspects of this manuscript, including study conception and design; acquisition, analysis, and interpretation of data; figure design; and drafting the article. Michael C. Sklar, Ahmad Alli, Adriaan Van Rensburg, and Jan O. Friedrich contributed to study conception and design; analysis and interpretation of data; and drafting the article.
Corresponding author
Ethics declarations
Disclosures
None.
Funding statement
None.
Editorial responsibility
This submission was handled by Dr. Hilary P. Grocott, Editor-in-Chief, Canadian Journal of Anesthesia.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hare, G.M.T., Cazorla-Bak, M.P., Ku, S.F.M. et al. When to transfuse your acute care patient? A narrative review of the risk of anemia and red blood cell transfusion based on clinical trial outcomes. Can J Anesth/J Can Anesth 67, 1576–1594 (2020). https://doi.org/10.1007/s12630-020-01763-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-020-01763-9