
Abstract
Background
Analgesia might be evaluated with simple changes in vital signs, a non-specific and non-sensitive method. Heart rate variability (HRV) correlates with autonomous nervous system activity and can be used to evaluate painful stimuli. Heart rate variability is then transformed into a numeric scale called the analgesia nociception index (ANI), where higher values represent predominant parasympathetic tone, thus low nociception. Under general anesthesia, the ANI decreases following painful stimuli and increases after administration of analgesia, but significant interindividual variability is present. The goal of the present study was to evaluate the ANI as a pain index in healthy awake volunteers.
Methods
Following research ethics board approval, participants were positioned supine in a calm operating room. The participants’ vital signs and ANI were monitored. After evaluation of all parameters without any stimulation, 23 volunteers received a 2 Hz electrical stimulus at the wrist with increasing current intensity from 0–30 mA (5 mA increments). The current was kept constant for three minutes at each level, and the volunteers rated their pain on a numeric rating scale (NRS) every minute. The Pearson correlation coefficient and linear regression were used to analyze the relationship between the ANI and the NRS score. The ANI absolute values and the variations from baseline were both analyzed.
Results
There was a very weak negative correlation between the NRS score and ANImean (Pearson, -0.089; 95% confidence interval [CI], −0.192 to −0.014; P = 0.045) and between the NRS score and ∆ANImean (Pearson, −0.174; 95% CI, −0.272 to −0.072; P < 0.001; regression slope, −0.586; 95% CI, −0.930 to −0.243; P < 0.001). Heart rate, blood pressure, and respiratory rate did not vary significantly throughout the study.
Conclusions
These findings provide little evidence to support use of the ANI in awake subjects or in awake patients such as those in the emergency room or in the intensive care unit. Nevertheless, based on an important difference between the expected correlation and the real correlation between the ANI and the NRS scores found in our results, the present study might be underpowered. Studies with a larger sample size would be required to enable firm conclusions about the clinical utility of the ANI in this population of awake volunteers as well as in awake patients. This study was registered with ClinicalTrials.gov (NCT02589093).
Résumé
Contexte
L’analgésie peut être évaluée en observant de simples changements des signes vitaux, via une méthode non spécifique et non sensible. La variabilité de la fréquence cardiaque (HRV) est corrélée à l’activité du système nerveux autonome et peut être utilisée pour évaluer les stimuli douloureux. La variabilité de la fréquence cardiaque est ensuite transformée en une échelle numérique, l’indice ANI (pour analgesia nociception index), sur laquelle les valeurs plus élevées représentent un tonus parasympathique prédominant, soit une nociception moindre. Sous anesthésie générale, l’ANI diminue après des stimuli douloureux et augmente après l’administration d’une analgésie, mais il existe une importante variabilité interpersonnelle. L’objectif de cette étude était d’évaluer l’ANI en tant qu’indice de la douleur chez des volontaires sains éveillés.
Méthode
Après avoir reçu l’approbation du Comité d’éthique de la recherche, les participants ont été placés en décubitus dorsal dans une salle d’opération calme. Les signes vitaux et l’ANI des participants ont été monitorés. Après l’évaluation de tous les paramètres sans aucune stimulation, 23 volontaires ont reçu un stimulus électrique de 2 Hz au poignet avec une intensité de courant augmentant de 0 à 30 mA (en incréments de 5 mA). Le courant a été maintenu pendant trois minutes à chaque niveau, et les volontaires ont évalué leur douleur sur une échelle d’évaluation numérique (EEN) chaque minute. Le coefficient de corrélation de Pearson et la régression linéaire ont été utilisés pour analyser la relation entre l’ANI et le score sur l’EEN. Les valeurs absolues de l’ANI et les variations par rapport aux valeurs de base ont toutes deux été analysées.
Résultats
Il y a eu une très faible corrélation négative entre le score sur l’EEN et l’ANImean (Pearson, −0,089; intervalle de confiance [IC] 95%, −0,192 à −0,014; P = 0,045) et entre le score sur l’EEN et ∆ANImean (Pearson, −0,174; IC 95%, −0,272 à −0,072; P < 0,001; courbe de régression, −0,586; IC 95%, −0,930 à −0,243; P < 0,001). Il n’y a pas eu de variation significative de la fréquence cardiaque, de la tension artérielle et de la fréquence respiratoire tout au long de l’étude.
Conclusion
Ces résultats ne sont pas suffisamment probants pour appuyer l’utilisation de l’ANI chez des sujets éveillés ou des patients éveillés tels que ceux de l’urgence ou de l’unité des soins intensifs. Toutefois, étant donné l’importante différence entre la corrélation anticipée et la corrélation véritable entre l’ANI et les scores sur l’EEN dans nos résultats, il est possible que notre étude manque de puissance. Des études portant sur un échantillon plus vaste seraient nécessaires pour parvenir à des conclusions définitives concernant l’utilité clinique de l’ANI chez cette population de volontaires éveillés ainsi qu’auprès de patients éveillés. Cette étude a été enregistrée au ClinicalTrials.gov, numéro NCT02589093.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Contrary to “immobility” and, to a lesser extent, to the “hypnosis/unconsciousness” component of general anesthesia, the monitoring of intraoperative “analgesia” is poorly described. It is assessed mainly through insensitive and potentially undesirable changes in a patient’s vital signs. This has led to the development of various devices and indices for specific monitoring of analgesia.
Heart rate variability (HRV) is a parameter related to the activity of the autonomic nervous system,1,2,3 which has a tone greatly influenced by factors such as pain and stress, including those associated with surgery. Although HRV does not predict anesthesia depth,4 it seems to point towards the balance between nociceptive input and antinociception.5 Heart rate variability is calculated from the electrocardiogram (ECG) and is based on an algorithmic analysis of the R-R interval. During stable general anesthesia and without surgical stimuli, parasympathetic tone predominates and HRV is high.6 When autonomic tone is altered by a painful stimulus, the R-R interval varies and HRV decreases. In patients undergoing surgery with total intravenous anesthesia,7 HRV decreases in a reproducible manner following painful stimulus but remains unchanged with prior administration of adequate analgesia.
The analgesia nociception index (ANI) is based on HRV,8 which rates the autonomic nervous system tone on a scale of 0–100. A high ANI value represents high HRV and thus prevalent parasympathetic tone. A low ANI value represents low HRV and thus prevalent sympathetic tone and diminished parasympathetic tone. The PhysioDoloris™ analgesia monitor (MetroDoloris Medical Systems SAS, Lille, France) was developed to measure the ANI continuously in patients under anesthesia.9 When tested on patients whose ANI remained stable during the maintenance of anesthesia, the monitor showed a decrease in the ANI when the surgical incision occurred and an increase back to basal values when analgesics were administered. The ANI values are also influenced by other surgical stimuli such as the induction of a pneumoperitoneum.10 A study has found significant interindividual variability in ANI changes despite similar stimuli,11 thus limiting its use in guiding the administration of adequate analgesia. In fact, intraoperative opioid administration guided by the ANI during laparoscopic cholecystectomies did not decrease drug consumption or postoperative pain scores.12
The ANI was studied in awake patients, including in women in labour, in the postanesthesia care unit (PACU), and in stressful situations.13 In the first study, 45 parturient women were monitored and asked to rate their pain at five-minute intervals as they were in active labour.14 Their ANI decreased during contractions, and a negative linear correlation was established between pain scores and the ANI. In two studies conducted in the PACU, patients who had undergone surgery under general anesthesia had their ANI monitored prior to extubation.15,16 It was determined that their ANI correlated negatively with the pain scores on a numeric rating scale (NRS, 0-10 scale) in the PACU. An Australian study17 monitored the ANI and the NRS pain scores in 120 patients in the PACU after elective surgery and found a weak negative correlation between these two parameters.
In this prospective observational study, we sought to evaluate the performance of the ANI in awake subjects and in a context free of confounding factors, such as movement, visual stimuli, or loud noises. We hypothesized that the ANI and the NRS pain scores would be negatively correlated in healthy awake volunteers subjected to stepwise increasingly painful standard experimental and electrical stimuli.
Methods
Recruitment
The Scientific and Ethics Committees of our institution reviewed and approved this prospective study on healthy awake volunteers (REB # 14074, Maisonneuve-Rosemont Hospital, Montreal, QC, Canada, approved November 2014). The protocol was registered with ClinicalTrials.gov (NCT02589093).
The PhysioDoloris analgesia monitor was not approved for commercial use in Canada at the time of this study. A no objection letter was obtained from Health Canada for use of the PhysioDoloris for this study. Potential participants were informed of the study via posters displayed throughout the hospital and were invited to contact one of the investigators if they were interested in participating. The study was explained to potential participants and informed consent was obtained. We included healthy volunteers 18–80 years of age. We chose not to include subjects with cardiac (including arrhythmias) or neurologic diseases, chronic pain or regular consumption of analgesics, medications that interfere with autonomous nervous system tone, and any incapacity to understand an NRS for pain.
Study design
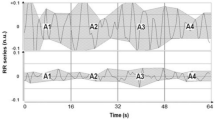
Each subject was positioned supine on a surgical table in a quiet and empty operating room. They were covered with warm blankets and blindfolded in order to minimize contact with the surroundings and unwanted stimuli. Vital signs were monitored continuously, including heart rate through ECG, respiratory rate through thoracic impedance, and oxygen saturation through pulse oximetry, and a noninvasive blood pressure measurement was obtained every minute. The PhysioDoloris device was connected and set to record both instantaneous ANI (ANI i) and two-minute average ANI values. Nerve stimulator electrodes were placed on the subject’s skin over the ulnar nerve of the left forearm and connected to a Life-Tech EZstim II analogue nerve stimulator. We assumed that electrode impedance variability was minimal. After evaluation of all parameters without any stimulation, the volunteers received a 2 Hz electrical stimulus (each lasting 0.2 msec) with stepwise increasing current intensity from 0-30 mA in intervals of 5 mA. Each intensity step lasted three minutes, and every minute, the volunteers were asked to rate their pain on a NRS (from 0-10), as illustrated in Fig. 1. Before the study protocol began, all volunteers were informed that they could ask for the painful stimuli to cease at any time. If they made that request, they were to remain supine, as a final data collection step was continued for three minutes without any electrical stimulation. Stimulation intensity of 0 mA was considered equivalent to an absence of stimulus.

Study design. ANI m = Analgesia Nociception Index (two-minute average measured at end of each step)
Statistical analysis
For each step, the two-minute average ANI value (out of three-minute duration for each step) and the average of the three NRS pain scores were calculated. The relationship between these paired data points were analyzed using both the Pearson correlation coefficient and linear regression and constituted the primary outcome. The ANI data were analyzed both as absolute values and as variations from the baseline measurements. The baseline values were those recorded prior to electrical stimulation during the first step at a current intensity of 0 mA. As a secondary outcome, the correlation between the two-minute average ANI and the current intensity at the end of each step was also calculated. The relationship between vital signs (heart rate, blood pressure, and respiratory rate) and the NRS pain scores was also analyzed (see Fig. 1 for study design).
A P value < 0.05 was considered statistically significant. We used GraphPad Prism version 5.03 (La Jolla, CA, USA) for all statistical analyses. A power analysis determined that we needed 23 volunteers to show a Pearson correlation coefficient of −0.5 between the ANI and NRS pain scores, with α = 0.05 and 1 − β = 0.8 (http://www.sample-size.net/).
Results
Twenty-three volunteers gave informed consent and were recruited to participate in this study from October–December 2014. Volunteer characteristics are shown in Table 1. Four of the 23 volunteers requested that the painful stimuli be stopped before reaching the final and highest step of current intensity. They nonetheless remained cooperative for the final three-minute step (at 0 mA, no stimulus) of data collection and their results were included in the overall analysis. None of the volunteers had any adverse effects resulting from their participation in our study.
We found a very weak negative correlation between the NRS pain scores and the mean of the ANI values (Pearson, −0.089; 95% confidence interval [CI], −0.192 to −0.014; P = 0.045; regression slope, −0.358; 95% CI, −0.770 to 0.055; P = 0.090). A stronger correlation was found between the NRS pain scores and the change in ANI from the baseline values, or ∆ANI (Pearson, −0.174; 95% CI, −0.272 to −0.072; P < 0.001; regression slope, −0.586; 95% CI, −0.930 to −0.243; P < 0.001). Plots of the ANI and ∆ANI values against the NRS pain scores are found in Figs 2 and 3, respectively. The current intensity did not correlate significantly with either the absolute values of the ANI (Pearson, −0.036; 95% CI, −0.139 to 0.067; P = 0.246; regression slope, −0.038; 95% CI, −0.147 to 0.070; P = 0.492) or with the ∆ANI (Pearson, −0.061; 95% CI, −0.163 to 0.043; P = 0.125; regression slope, −0.054; 95% CI, −0.145 to 0.038; P = 0.250). The vital signs recorded during data collection did not vary significantly with the increase in the NRS pain scores: heart rate (regression slope, 0.414; 95% CI, −0.036 to 0.792; P = 0.133), systolic blood pressure (regression slope, 0.537; 95% CI, −0.015 to 1.062; P = 0.115), diastolic blood pressure (regression slope, 0.032; 95% CI, −0.260 to 0.325; P = 0.829), and respiratory rate (regression slope, 0.305; 95% CI, −0.168 to 0.793; P = 0.157). Results for all measures over time are summarized in Table 2.

Analgesia nociception index as a function of numeric rating scale score for pain. ANI = analgesia nociception index

∆ANI (ANI variation) as a function of numeric rating scale score for pain. ANI = analgesia nociception index
Unsurprisingly, NRS pain scores and current intensity had a strong positive correlation (Pearson, 0.860; 95% CI, 0.831 to 0.885; P < 0.001; regression slope, 0.227; 95% CI, 0.212 to 0.240; P < 0.001), as shown in Fig. 4.

Numeric rating scale score for pain as a function of current intensity
Discussion
This study reports a very weak negative correlation between the ANI values and NRS pain scores in healthy awake volunteers. Because of this very weak correlation between the absolute values of ANI and the NRS pain scores, we decided to conduct a post hoc exploratory analysis evaluating the correlation between the ANI variation from baseline values (or delta ANI) and the NRS scores. Compared with absolute values of ANI, change in the ANI from baseline (∆ANI) was modestly more correlated with the NRS score, but the association remained weak. Significant interindividual variability in the measurement of the ANI accounts for the superiority of the ∆ANI. A similar observation was made in a study evaluating the ANI as a predictor of hemodynamic changes in patients under general anesthesia.18
Neither the heart rate nor the blood pressure varied significantly in association with pain scores, at least for non-surgical intensity stimuli, such as those applied to the volunteers in this study, and despite the fact that these stimulations were able to induce pain scores of 6.5 (2.1) at the higher level of stimulation (Table 2).
Investigations of the ANI as a predictor of intraoperative hemodynamic changes have found contradictory results. An earlier study evaluating patients under sevoflurane-fentanyl anesthesia determined that the ANI was unable to predict hemodynamic changes.19 A later project with patients under desflurane-remifentanil concluded that both the ANI and ∆ANI could predict hemodynamic reactivity. Nevertheless, in addition to the differences in the drugs used during the maintenance of anesthesia, the former study relied on a lesser threshold in defining hemodynamic changes.
Our study presents some limitations. The a priori power analysis assumed a correlation coefficient of −0.5 between the ANI and the NRS pain scores. Our results reported a Pearson correlation coefficient of only −0.089 (95% CI, −0.192 to −0.014; P = 0.045; regression slope, −0.358; 95% CI, −0.770 to 0.055; P = 0.090). If we had initially hypothesized such a weak correlation, a much larger number of volunteers (about 1,000) would have been needed. This discrepancy between the expected correlation and the real reported correlation means that our study might have been underpowered to detect such a correlation. Nevertheless, the correlation we found, though indeed very weak, was statistically significant. Furthermore, age and sex are likely to impact autonomic nervous tone and pain perception, but this study was not designed to detect their effects.
The use of an electrical stimulus to generate pain also presents some issues. Anesthesiologists are familiar with the required equipment, and many studies evaluate nociception with electrical stimuli. These have amplitude and duration that are easy to control. On the other hand, they are limited by the fact that they excite all peripheral nerve fibres at once and in a synchronized manner.20 This means that the electrical stimuli we used may not necessarily represent acute surgical pain.
Furthermore, many factors, such as movement and breathing pattern, can interfere with the measurement of the ANI in the awake subject despite optimization of the study settings to reduce stimuli other than pain. We had no control over the volunteers’ respiration, their thoughts, or their possible anxiety, even though we tried to minimize the latter factor by providing ample explanations and reassurance. We also assumed that the painful stimulus of the blood pressure cuff was minimal as volunteers never complained of pain when blood pressure was measured.
We did not randomize the current intensities used for each step, and it might be argued that this allowed the volunteers to prepare or anticipate the increase in pain. Though this is a possibility, we could not proceed with such a design. This approach would have allowed a scenario where a subject could be exposed to maximal stimulation right from the beginning of the study, and it was the Institutional Ethics Committee’s opinion that such occurrence should be avoided in awake volunteers.
Also, although we found a statistically significant correlation between the ∆ANI and NRS score, the magnitude of the correlation suggests questionable clinical significance in the evaluation of pain in awake patients. Given the rather low correlation between the NRS scores and ANI values in the quiet setting of the present trial, it would be challenging to study how the ANI would perform in a regular clinical environment filled with many confounding factors that can influence pain perception, such as emergency departments, intensive care units, and clinical wards.
Moreover, a recent study exploring the effects of both expected and non-expected electrical stimuli on 20 male volunteers found no correlation between the ANI and NRS pain scores.21 The painful stimuli were delivered by a nerve stimulator, but the current intensity of 2 mA was much lower than that used in this study (up to 30 mA). Furthermore, only ANI absolute values were analyzed, rather than their variation from baseline or ∆ANI. These two elements might account for the lack of correlation in that study. Nevertheless, it seems that their study and ours suggest that a correlation between ANI and pain scores in awake volunteers does not exist or is weak and, as a consequence, might have small clinical relevance for pain monitoring in this specific population.
In conclusion, the ANI exhibited a very weak correlation with pain perception, as measured by an NRS of 0-10 in healthy conscious subjects, particularly when we analyzed ANI variations from baseline rather than absolute values. It is doubtful whether the ANI can be used in awake patients, such as those in emergency departments. A higher correlation between the ANI and pain scores should be reported before proposing its use to monitor pain in this clinical context.
References
Latson TW, O’Flaherty D. Effects of surgical stimulation on autonomic reflex function: assessment of changes in heart rate variability. Br J Anaesth 1993; 70: 301-5.
Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology the North American Society of Pacing and Electrophysiology. Circulation 1996; 93: 1043-65.
Pichot V, Gaspoz JM, Molliex S, et al. Wavelet transform to quantify heart rate variability and to assess its instantaneous changes. J Appl Physiol 1985; 1999(86): 1081-91.
Pichot V, Buffiere S, Gaspoz JM, et al. Wavelet transform of heart rate variability to assess autonomic nervous system activity does not predict arousal from general anesthesia. Can J Anesth 2001; 48: 859-63.
Logier R, Jeanne M, Tavernier B, De Jonckheere J. Pain/analgesia evaluation using heart rate variability analysis. Conf Proc IEEE Eng Med Biol Soc 2006; 1: 4303-6.
Jeanne M, Logier R, De Jonckheere J, Tavernier B. Validation of a graphic measurement of heart rate variability to assess analgesia/nociception balance during general anesthesia. Conf Proc IEEE Eng Med Biol Soc 2009; 2009: 1840-3.
Jeanne M, Logier R, De Jonckheere J, Tavernier B. Heart rate variability during total intravenous anesthesia: effects of nociception and analgesia. Auton Neurosci 2009; 147: 91-6.
De Jonckheere J, Logier R, Jounwaz R, Vidal R, Jeanne M. From pain to stress evaluation using heart rate variability analysis: development of an evaluation platform. Conf Proc IEEE Eng Med Biol Soc 2010; 2010: 3852-5.
Logier R, Jeanne M, De Jonckheere J, Dassonneville A, Delecroix M, Tavernier B. PhysioDoloris: a monitoring device for analgesia / nociception balance evaluation using heart rate variability analysis. Conf Proc IEEE Eng Med Biol Soc 2010; 2010: 1194-7.
Jeanne M, Clement C, De Jonckheere J, Logier R, Tavernier B. Variations of the analgesia nociception index during general anaesthesia for laparoscopic abdominal surgery. J Clin Monit Comput 2012; 26: 289-94.
Gruenewald M, Ilies C, Herz J, et al. Influence of nociceptive stimulation on analgesia nociception index (ANI) during propofol-remifentanil anaesthesia. Br J Anaesth 2013; 110: 1024-30.
Szental JA, Webb A, Weeraratne C, Campbell A, Sivakumar H, Leong S. Postoperative pain after laparoscopic cholecystectomy is not reduced by intraoperative analgesia guided by analgesia nociception index (ANI) monitoring: a randomized clinical trial. Br J Anaesth 2015; 114: 640-5.
De Jonckheere J, Rommel D, Nandrino J, Jeanne M, Logier R. Heart rate variability analysis as an index of emotion regulation processes: interest of the analgesia nociception index (ANI). Conf Proc IEEE Eng Med Biol Soc 2012; 2012: 3432-5.
Le Guen M, Jeanne M, Sievert K, et al. The analgesia nociception index: a pilot study to evaluate of a new pain parameter during labor. Int J Obstet Anesth 2012; 21: 146-51.
Boselli E, Daniela-Ionescu M, Begou G, et al. Prospective observational study of the non-invasive assessment of immediate postoperative pain using the analgesia/nociception index (ANI). Br J Anaesth 2013; 111: 453-9.
Boselli E, Bouvet L, Begou G, et al. Prediction of immediate postoperative pain using the analgesia/nociception index: a prospective observational study. Br J Anaesth 2014; 112: 715-21.
Ledowski T, Tiong WS, Lee C, Wong B, Fiori T, Parker N. Analgesia nociception index: evaluation as a new parameter for acute postoperative pain. Br J Anaesth 2013; 111: 627-9.
Boselli E, Logier R, Bouvet L, Allaouchiche B. Prediction of hemodynamic reactivity using dynamic variations of analgesia/nociception index (∆ANI). J Clin Monit Comput 2016; 30: 977-84.
Ledowski T, Averhoff L, Tiong WS, Lee C. Analgesia nociception index (ANI) to predict intraoperative haemodynamic changes: results of a pilot investigation. Acta Anaesthesiol Scand 2014; 58: 74-9.
Handwerker HO, Kobal G. Psychophysiology of experimentally-induced pain. Physiol Rev 1993; 73: 639-71.
Jess G, Pogatzki-Zahn M, Zahn PK, Meyer-Frießem CH. Monitoring heart rate variability to assess experimentally induced pain using the analgesia nociception index: a randomized volunteer study. Eur J Anaesthesiol 2016; 33: 118-25.
Acknowledgements
The Department of Anesthesiology sincerely thank Nadia Godin, Research Nurse and Coordinator, for her collaboration in this study.
Conflict of interest
Dr. Philippe Richebé is a member of the Scientific Advisory Board of Medasense Biometrics Limited (Ramat Gan, Israel). Both the technology and manufacturer (MetroDoloris Medical Systems SAS, Lille, France) of the PhysioDoloris device used in this study are distinct from pain assessment products marketed by Medasense. The PhysioDoloris device belongs to the Department of Anesthesiology, Hôpital Maisonneuve-Rosemont
Editorial responsibility
This submission was handled by Dr. Gregory L. Bryson, Deputy Editor-in-Chief, Canadian Journal of Anesthesia.
Author contributions
Philippe Richebé and Rami Issa were involved in conducting the study and writing the manuscript. Philippe Richebé, Rami Issa, and Pierre Drolet were involved in the data analysis. All authors were involved in the study design and in planning and revising the manuscript.
Funding
This work was supported by the Department of Anesthesiology of the Maisonneuve-Rosemont Hospital.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Issa, R., Julien, M., Décary, E. et al. Evaluation of the analgesia nociception index (ANI) in healthy awake volunteers. Can J Anesth/J Can Anesth 64, 828–835 (2017). https://doi.org/10.1007/s12630-017-0887-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-017-0887-z